
Abstract
Introduction
Trauma is a leading cause of paediatric morbidity and mortality, but is often managed at non-paediatric specialist centres, where limited familiarity with paediatric patient management impacts care quality and outcomes. Telemedicine presents a unique solution to these problems, having the potential to improve patient outcomes by influencing the immediate assessment, management and disposition of injured children. This scoping review aims to detail the use of telemedicine in acute paediatric trauma: when and where it is used, what outcomes have been evaluated and any evidence gaps.
Methodology
We conducted a scoping review to identify primary studies that evaluated the use of telemedicine in paediatric trauma. Five databases were searched for relevant studies published prior to June 2024.
Results
Nine studies were included. Most papers (n = 8) reported on the effect of telehealth on patient treatment decisions and outcomes, including a decrease in mortality (n = 1), impact on patient disposition (n = 1) and change in patient care due to telehealth (n = 1). Clinician satisfaction (n = 3), parent satisfaction (n = 3) and difficulties encountered with telemedicine usage (n = 2) were also explored.
Conclusion
When employed to connect rural mixed emergency departments with paediatric trauma centres, telemedicine has the potential to influence initial management and improve appropriate disposition rates, with demonstrated improvement in care quality and survival rates, as well as improved stakeholder satisfaction. However, there is a need for higher-quality evidence generated through prospective studies to validate the use of telemedicine in paediatric trauma and demonstrate its impact on value-based care provided to children and their support networks.
Introduction
Traumatic injuries are a leading cause of death and disability in the paediatric population. 1 Children, anatomically and physiologically, respond differently to adults, requiring specific age-adjusted management of traumatic injuries. 2 In Australia, the vast majority of paediatric presentations to the emergency department (ED) are to mixed EDs with varying paediatric expertise. 3 Globally, rates of presentation to mixed EDs are significantly higher for lower-income countries and areas of increased rurality, although there is no composite global epidemiological data.4–6 There may be limited familiarity or confidence with paediatric resuscitation equipment and the management of paediatric problems, particularly in rural, remote and low-resource hospitals. 7 Disparities in paediatric resourcing and expertise can have significant impacts on patient outcomes: paediatric trauma mortality risk increases twofold with rurality, 8 and children managed at paediatric trauma centres (PTCs) have approximately 40% lower mortality than those who are not, although this evidence is of low certainty. 9 In Australia, a retrospective review in 2013 of 1138 severely injured children found that children who received treatment at a PTC were between three and six times more likely to survive than if they were treated at a mixed ED. 10
In a trauma setting, effective communication is imperative to optimise the quality, safety and outcomes of care delivered.11–13 With constantly improving technology, accelerated by the recent COVID-19 pandemic, the role of telemedicine in optimising this communication is increasing. Telemedicine is defined by the World Health Organization as the delivery of health-care services, where distance is a key factor, using information and communication technologies, to help diagnose, treat and prevent disease or injury. 14 It may involve various technologies, including real-time audio and visual calls, text messages, systems to store and hold messages or remote monitoring of vitals. 15
Telemedicine presents a unique solution to some of the problems encountered with the presentation of paediatric illness and trauma to mixed EDs. Real-time video and audio conferencing has been found to be superior to telephone communication alone. 16 It allows for timely and efficient access to off-site specialists, improving patient assessment, resuscitation decisions and care, including support with performing procedures.17,18 Telemedicine allows paediatric specialists to make care recommendations based on direct observations unavailable during telephone consultations. For example, an evaluation of paediatric consultations in rural EDs in two US states revealed that specialist paediatric advice via telemedicine prevented unnecessary intubation in 12 critically ill paediatric patients and led to a further seven other patients being intubated who would otherwise have remained without respiratory support, highlighting the benefits of telemedicine for tailoring interventions to improve care outcomes. 16 Such a connection of rural or mixed EDs to PTCs creates collaborative supportive partnerships and improves access, regardless of financial or geographical barriers.7,18,19 The extent of the benefit of access to specialist expertise remains contingent on referral hospitals being adequately supplied with paediatric-specific resources.
Telemedicine can also provide valuable assistance with decisions regarding the transfer of injured children to tertiary paediatric care facilities. Remote telemedicine triage by a paediatric specialist can help better determine the acuity and level of service required for a patient, promote transfer expedition when transfer is warranted, and prevent unnecessary transfer when it is not.18,20,21 The utility of remote expertise has been previously demonstrated, as without specialist paediatric input, children are often unnecessarily admitted to hospital or transferred from general EDs more frequently than adults.16,19,22 Equally, without specialist input, the necessary transfer may be delayed instead of being expedited. Delayed transfer not only poses an economic cost to the health system, 23 but also an emotional and financial cost to the patient and their family, by increasing travel times to distant facilities and limiting social and emotional support structures.7,18,21
Telemedicine has been widely used in a variety of paediatric emergency care settings, including urgent care, 20 orthopaedics,24–26 intensive care, 27 burns,21,22,28,29 maxillofacial 23 and traumatic brain injury.30,31 In a burns setting, one study demonstrated that clinicians utilising telemedicine had similar efficacy to face-to-face consultation in clinical assessment and in decision making. 22 In the ED, it has been shown to improve patient outcomes, diagnostic accuracy, and reduce the number of transfers, 32 whilst also being described as a satisfactory consultation modality by parents.33,34 Telemedicine, when compared with telephone consults, has also been found to be cost and time-saving with potential annual savings of $4662 USD per child per ED and a reduction in interhospital transfers of over 30%. 35
These advantages, however, do not come without limitations. High start-up costs, the need to be connected to high-quality internet, technology learning barriers, 36 potential misdiagnoses and further need for in-person review are all significant barriers to the general use of telemedicine.37,38 Furthermore, despite the increasing availability and use of telemedicine post COVID-19, 39 research surrounding the outcomes of telemedicine is limited, lacking the high-quality evidence associated with long-term randomised control trials (RCTs).34,40 In adults, one systematic review by Nouh et al. has been published, including only four RCTs, 20 cohort studies and one pilot study. 41 In children, the use of telemedicine to assist with imaging decisions and interpretation in acute trauma has been explored systematically. 42 However, despite the growing body of evidence of its use in the holistic acute care of children experiencing acute trauma, the application, impact and acceptability of telemedicine in this population have not been systemically examined. This presents a key barrier to informing resourcing decisions, as well as the design and uptake of telemedicine models across diverse contexts. Indeed, its role is currently not incorporated into published clinical practice guidelines. 43
This scoping review aims to map studies of the use of telemedicine in acute paediatric trauma, including when and where it is used, what outcomes have been evaluated, and evidence of impact. Remaining evidence gaps will be identified. The findings in this review will be used to inform the design of an implementation trial aiming to improve the management of acutely injured children across the trauma system in New South Wales, Australia.
Methodology
Search strategy
A scoping review was undertaken to identify the role of telemedicine in acute paediatric trauma. The review was conducted in accordance with the Preferred Reporting Items for Systematic and Meta-Analyses Statement for Scoping Reviews (PRISMA-ScR) guidelines (Online Supplemental File 1) 44 and the study protocol was registered in PROSPERO (CRD420250568405).
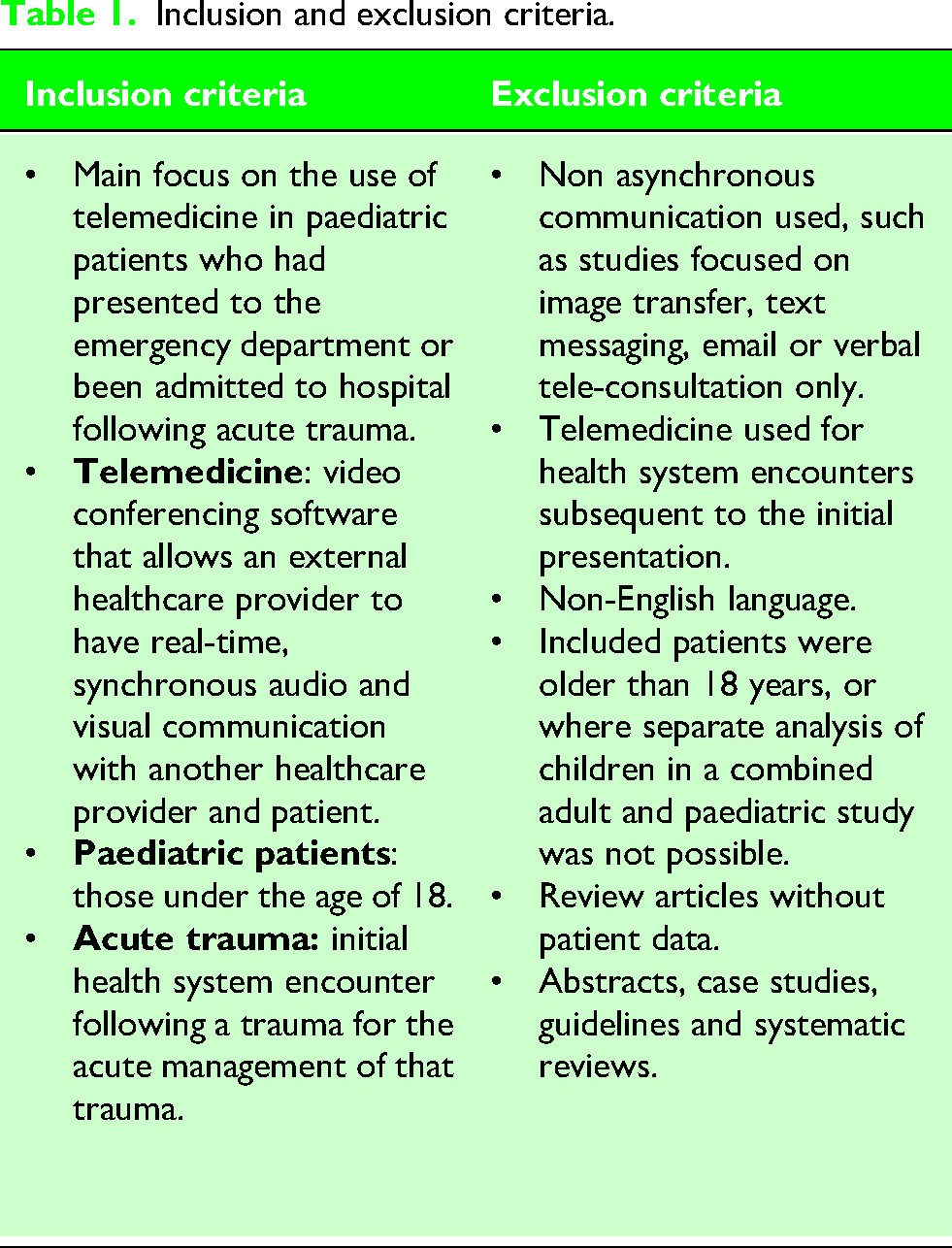
We searched PubMed, MedLine, EMBASE, Web of Science and Cochrane electronic databases for relevant studies published prior to June 2024 using the following keyword terms: [(telemedicine) OR (virtual care) OR (telehealth)] AND [(paediatric trauma) OR (pediatric trauma) OR (injured children)]. Studies that focused on the use of telemedicine in paediatric patients presenting to the ED with acute trauma were included. Reference lists from included articles were also reviewed for relevant studies. Telemedicine was defined as the use of information and communication technologies that allowed for real-time audio and visual communication between two or more healthcare providers. This mode of telemedicine best aligns with the current standard of acute telemedicine care in New South Wales, Australia. Study inclusion and exclusion criteria are presented in Table 1.
Inclusion and exclusion criteria.
Study selection
The results of the individual database searches were combined, and duplicate references were removed. Titles and abstracts of all articles identified by the initial search were independently screened for potential relevance by two authors (CL and ES). Selected articles were retrieved as full texts and independently reviewed against the inclusion and exclusion criteria by the same two authors (Table 1). Studies were stored and screened in Covidence, a web-based collaboration software platform designed to streamline literature reviews. Disagreements were resolved by a third reviewer (AP).
Data extraction and synthesis
Data were extracted independently by two reviewers (JC, CL) into a pre-formatted Word template, and included: study details (publication date, study design, years of data collection); setting (country, health care setting, rurality); study population (number of participants, age, sex and ethnicity); and trauma details (head, orthopaedic, abdominal, wounds, multiple, unspecified and other) (Online Supplemental File 2). Outcome data was extracted for all studies, then thematically organised depending on the nature of the outcomes reported (Online Supplemental File 3).
Once extracted, the data was synthesised using a narrative synthesis approach similar to Arksey and O’Malley, 45 with both reviewers discussing the results and establishing thematic similarities across the studies, then updating the entries. Study quality was not formally assessed.
Results
Study characteristics
A total of nine studies met the full inclusion criteria (Figure 1). Study characteristics are summarised in Table 2. Included studies were published between 2004 and 2023. Five studies were retrospective cohort studies,18,46–49 three were retrospective observational studies7,19,50 and one was an interim mixed methods evaluation of an RCT. 36 The included studies were undertaken in three high-income countries (United States [n = 7]; Australia [n = 1]; and Russia [n = 1]). Five studies looked exclusively at acute trauma.18,36,48–50 Six studies compared cases who had telehealth to those who did not,18,36,46–49 whilst the remaining three had no comparator.7,19,50 Overall sample sizes ranged from 15 48 to 4279 patients 47 ; in studies including a comparator group, the telemedicine cohorts ranged from eight18,48 to 212 patients. 47
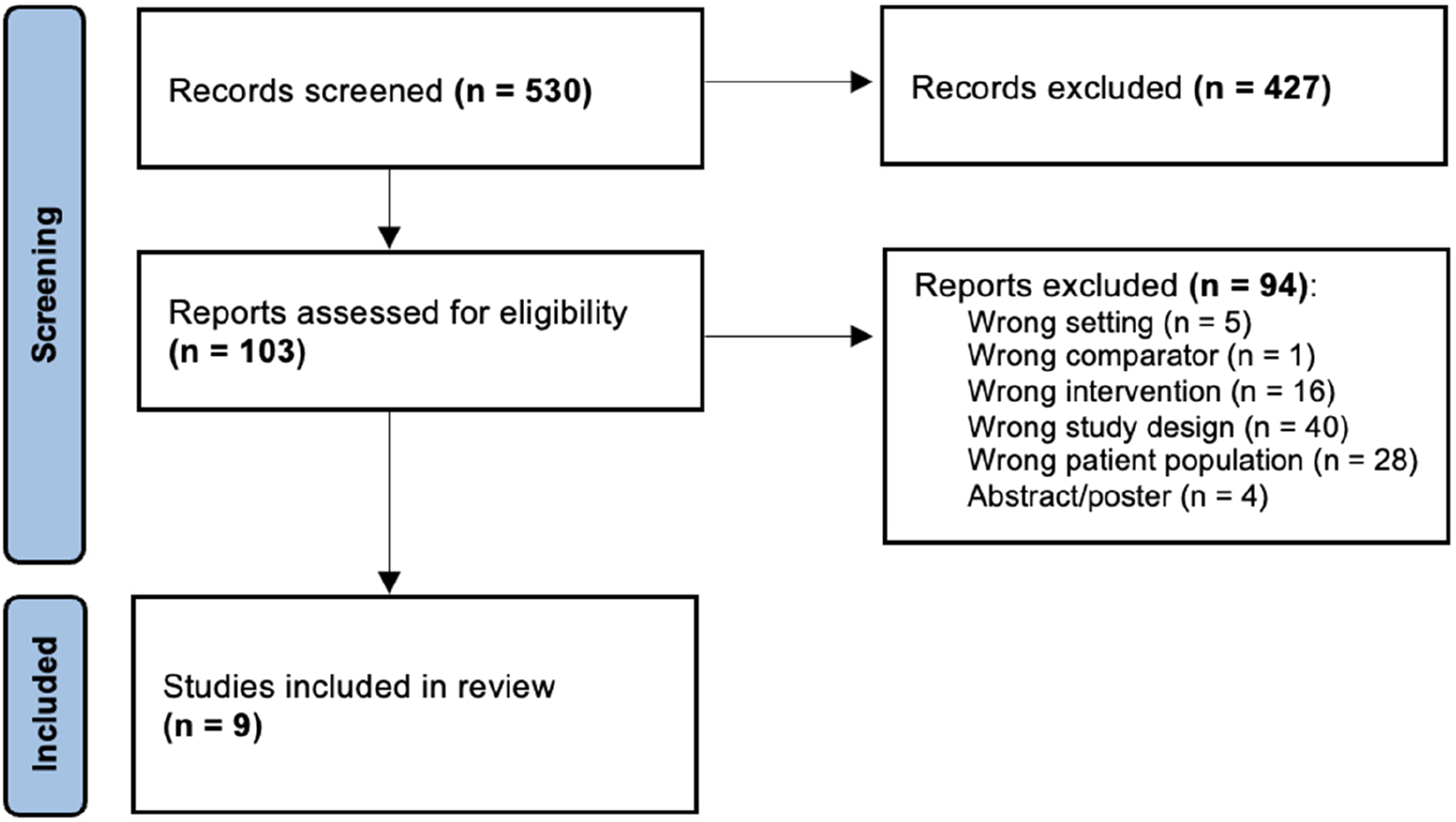
PRISMA flow diagram.
Characteristics of studies included in the review.
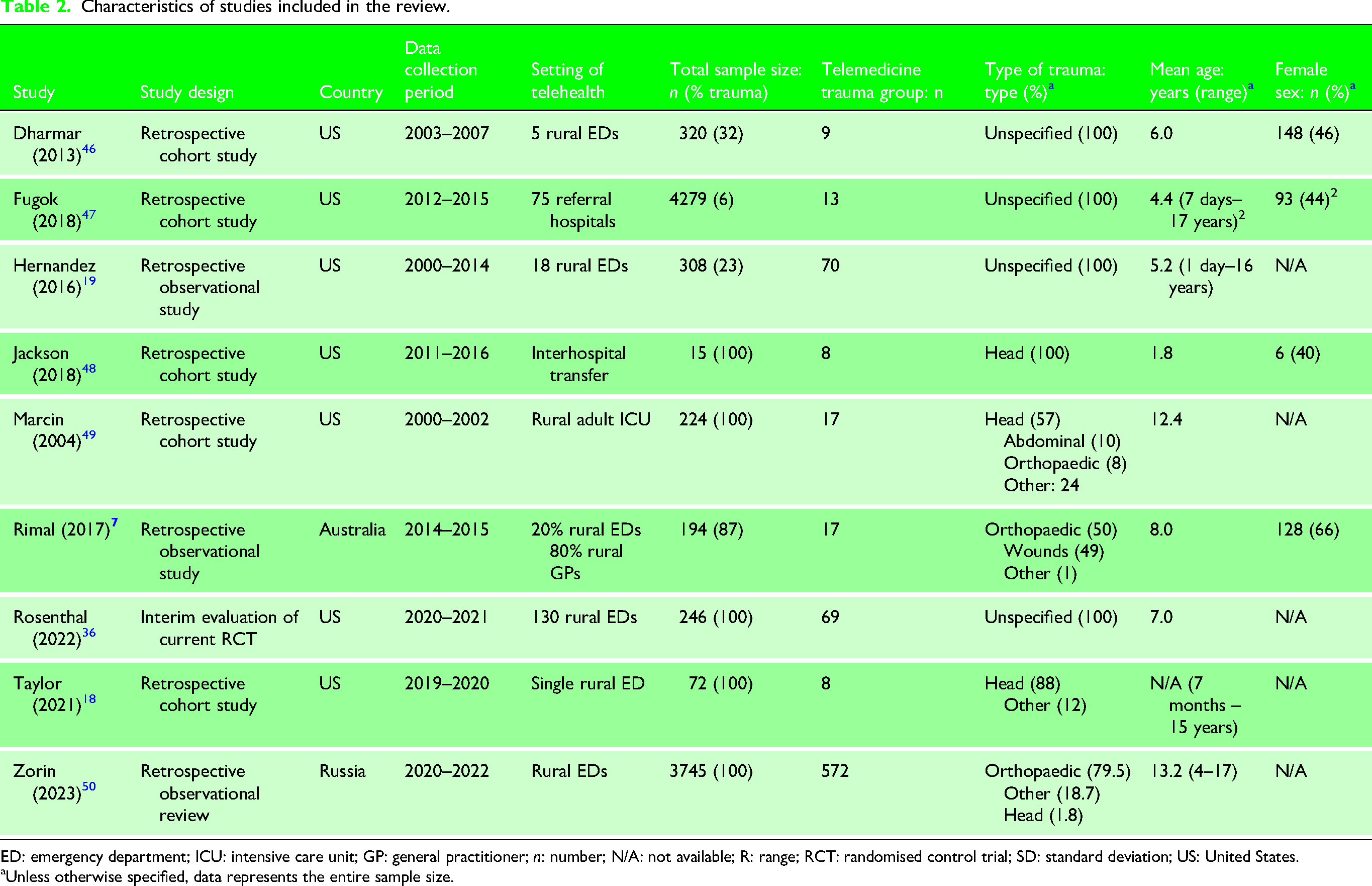
ED: emergency department; ICU: intensive care unit; GP: general practitioner; n: number; N/A: not available; R: range; RCT: randomised control trial; SD: standard deviation; US: United States.
Unless otherwise specified, data represents the entire sample size.
Patient demographics
The mean age of paediatric trauma patients ranged from 1.8 to 13.2 years, with five of the nine included studies reporting a mean age of less than eight years.19,36,46–48 Gender was reported in four studies, ranging from 40% to 66% female.7,46–48 No study reported on ethnicity.
Setting
Requests for a telemedicine consultation frequently originated from rural settings (n = 7).7,18,19,36,46,49,50 The majority (n = 7) happened between mixed EDs and paediatric critical care specialists in tertiary children's hospitals, with the exception of one study between an adult intensive care unit (ICU) and a specialist paediatric ICU, 49 and one study using telehealth during interhospital transfer between a mixed ED and a tertiary paediatric centre. 48
Trauma characteristics
Five studies focused solely on trauma,18,36,48–50 with the others including trauma and non-traumatic emergency presentations.7,19,46,47 Four studies did not specify the type of trauma.19,36,46,47 One reported the external cause of trauma, but not the body regions injured. 19 One focused solely on head trauma. 48 The others reported a combination of orthopaedic (n = 3),7,49,50 head (n = 2),18,49 abdominal (n = 1), 49 wounds (n = 1) 7 and/or multiple (n = 1) 50 or grouped other injuries (n = 3).7,49,50 No study commented on the influence of trauma type on the use of telehealth.
Trauma severity was not uniformly reported, with only three studies analysing its influence on the use of telehealth. Dharmar et al. used the Paediatric Risk of Admission Score (PRISA), 51 demonstrating that those in the telemedicine cohort had a significantly higher mean PRISA than those with no telemedicine consult (17.8 vs 10.9, p < 0.05). 46 Similarly, Marcin et al. found a correlation between a higher mean injury severity score (ISS) and telemedicine consult (18.3 vs 14.7, p = 0.07). 49 Zorin et al. also used the ISS for patients with multisystem trauma (mean 31, range 9–57), all of whom received a telemedicine consultation. 50
Study outcomes
Thematic grouping of study results found six common outcomes reported in at least two of the nine included studies. These included: patient care and treatment outcomes (mortality, length of stay, disposition and quality of care) (Table 3); stakeholder satisfaction; and barriers and facilitators to the implementation of telemedicine.
Summary of reported impact of telemedicine on care and treatment outcomes.
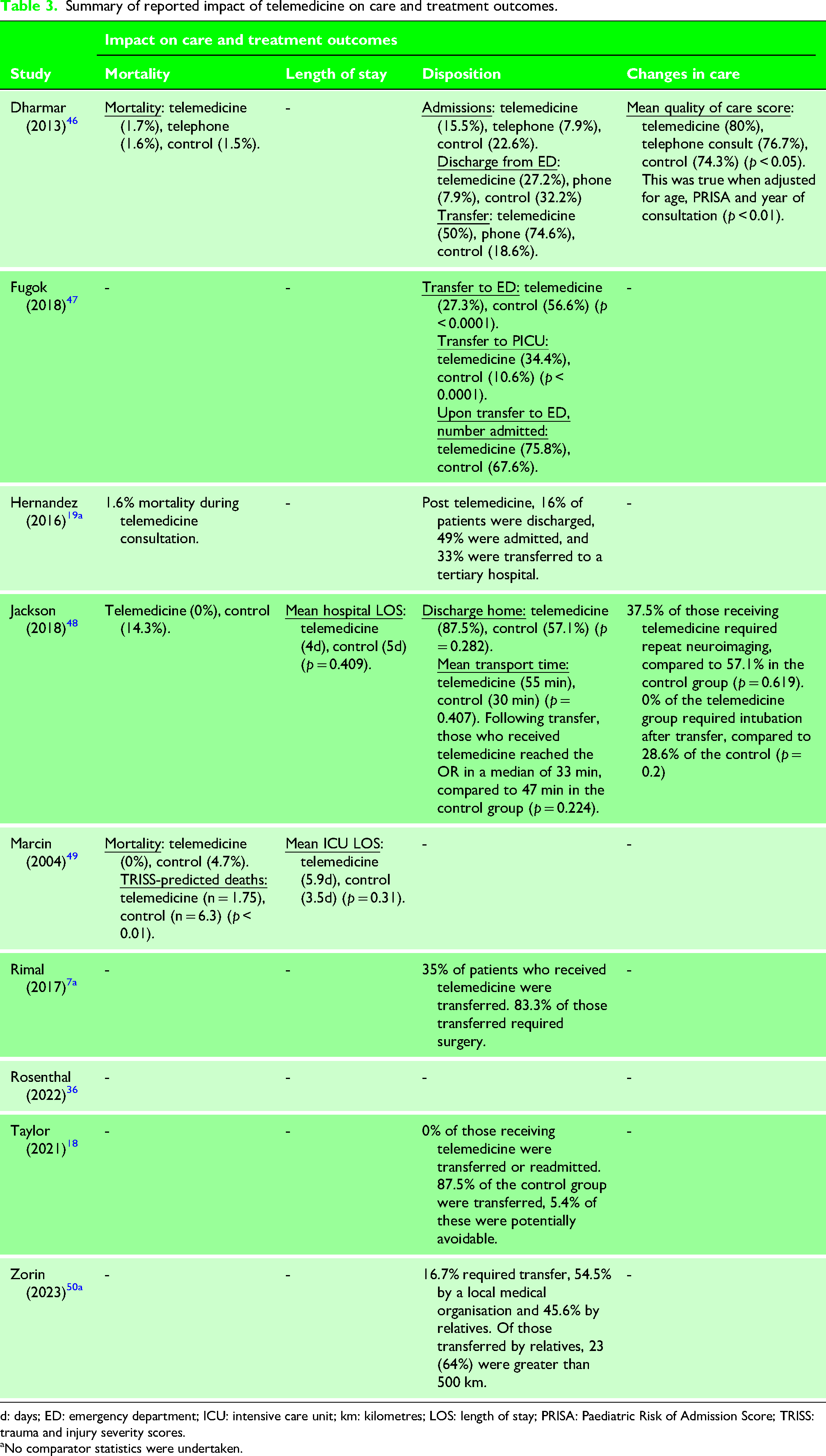
d: days; ED: emergency department; ICU: intensive care unit; km: kilometres; LOS: length of stay; PRISA: Paediatric Risk of Admission Score; TRISS: trauma and injury severity scores.
No comparator statistics were undertaken.
Impact on patient care and treatment outcomes
Eight retrospective studies reported the impact of telemedicine on patient care and treatment outcomes, all of which were retrospective.7,18,19,46–50 Five of these studies included a control group.18,46–49
Mortality
Four studies assessed the effect on mortality.19,46,48,49 Mortality rates ranged from 0% 48 to 1.7% 46 for the telemedicine cohorts, and 1.5% 46 to 14.3% 48 in the control cohorts. Marcin et al. 49 was the only one to find a significant survival benefit. The authors utilised the trauma and injury severity scores (TRISS) to calculate predicted deaths between the intervention group (n = 17) and historical controls (n = 207) in a cohort of patients with head, abdominal, orthopaedic or other trauma. The telemedicine cohort had zero deaths compared to the predicted 1.8 deaths, whereas the historical control group had six deaths with a predicted 6.3 deaths (p < 0.01).
Length of stay
Effect on length of stay was examined in two retrospective comparative cohort studies,48,49 both of which only included trauma cases. Neither found an effect. Jackson's small study of 15 children experiencing head trauma found that use of telemedicine resulting in transfer to a tertiary hospital (n = 8) was not significantly related to a different median LOS or rate of discharge home without inpatient rehabilitation, when compared to no telemedicine (n = 7) (4 vs 5 days, p = 0.49; 87.5% vs 57.1%, p = 0.282). 48 Similarly, Marcin et al. found no significant difference between ICU LOS in the telemedicine group (5.9 days) and the historical control group (3.5 days) (p = 0.31). 49
Disposition
Disposition was defined as the location of care after the initial presentation to the hospital, including discharge from ED, admission to the hospital or transfer to another hospital. Seven studies examined the effect of telemedicine on disposition7,18,19,46–48,50 and two found an effect, both of which also included non-trauma cases.46,47 In the first, a study of children with unspecified trauma presenting to rural EDs in the United States found that, compared to a telephone-only consultation, telemedicine resulted in significantly more frequent changes in disposition (37.7% vs 20.0%, p < 0.01), however disposition was not defined. 46 In the second study, an evaluation of the first 24 months of a telemedicine program connected a designated level II trauma centre in the United States to paediatric critical care specialists at the closest children's hospital, 47 only 7.1% (n = 15/212) of the telemedicine cohort were not transferred. When compared to their historical non-telemedicine cohort (n = 4067), those who were transferred after telemedicine (n = 197/212) were significantly less likely to enter the ED of the transfer hospital (n = 58/212, 27% vs n = 2302/4067, 56%, p < 0.0001), and more likely to be admitted directly to the paediatric ICU (n = 73/212, 34% vs n = 431/4067, 10%, p < 0.0001). Those that were transferred to the tertiary ED were less likely to be discharged from the ED if they had been transferred following telemedicine than the historical non-telemedicine control group (n = 14, 24% vs n = 756, 32.4%, no p-value reported). In the telemedicine group, of those admitted to the tertiary paediatric ICU (n = 73), 90.4% had care requirements that could have only been provided at the tertiary hospital.
Patient care
Two studies examined the relationship between the use of telemedicine and clinical investigations and interventions.46,48 Jackson et al.'s study of 15 children experiencing head trauma in Maryland, United States, found no correlation between telemedicine usage during transfer and intubation rates, need for repeat neuroimaging on arrival to the tertiary centre or time to surgery. 48 Dharmar et al.'s study of 320 children presenting as the highest triage category to rural EDs in California found that when compared to a telephone only consultation, referring providers utilising telemedicine perceived significantly more changes in diagnostic studies (n = 68, 47.8% vs n = 16, 13.3%, p < 0.01) and therapeutic interventions (n = 68, 55.2% vs n = 16, 7.1%, p < 0.01). 46 The investigators also examined the effect on quality of care, with two independent paediatric ED consultants utilising a validated five-item instrument to evaluate included ED medical records on data gathering, development of diagnoses, initial treatment plan, plan for disposition and overall assessment of quality of care. After adjusting for the confounders of age, risk of admission score and year, patients receiving telemedicine had a higher quality of care than those who received no telemedicine or telephone consultation (5.76 vs 5.26; p < 0.01). 46
Stakeholder satisfaction with telemedicine
Clinicians
Three studies assessed referring clinician satisfaction with the telehealth experience.36,46,49 Two used surveys immediately following the consultation: one just for physicians 46 and one for both physicians and nurses. 49 One collated information contained in emails from both nurses and physicians about their experiences. 38 Measures included the referrer's perceptions of: importance for the child 46 ; clinical skills of the paediatric clinicians 46 ; the degree to which it helped medical management36,46; the importance of care being received in the local hospital 49 ; technical aspects of the use36,49; quality of the communication 49 ; and the overall telehealth experience.36,46,49 Satisfaction of receiving clinicians was not evaluated in any study.
Dhamar et al. found that referring clinicians who had participated in a telemedicine consultation with a paediatric critical care physician rated the consulting physician's clinical skills higher on a 10-point scale (6.82 vs 6.13, p < 0.01) and the quality of the care provided higher (6.69 vs 6.20, p < 0.05) than those who had participated in telephone-only consultations. 46 However, there was no significant difference in the perceived assistance in the patient's medical management (6.20 vs 5.87, p = 0.29). Marcin et al. echoed these findings, although with no comparator. 49 Physicians and nurses expressed similar levels of content with telemedicine consultations as they related to: audiovisual quality (physician, 86%; nurse, 100%); the ease of use of the equipment (physician, 88%; nurse, 80%); their ability to understand the consultant (physician, 94%; nurse, 100%); and their overall satisfaction with the consultation (physician, 92%; nurse, 100%). 49
Rosenthal et al.'s interim implementation evaluation of their RCT on telemedicine usage in consultations for paediatric trauma between mixed EDs and a PTC in California, United States, found positive perceptions of telehealth were almost exclusively expressed by trauma surgery nurse practitioners, who were the main instigators of its use. This positive sentiment was evidenced in: ‘The parents recognized me on arrival and both smiled upon seeing a familiar face. Mom said that she appreciated the video visit because she knew what to expect and that eased her anxiety’. Areas of reported dissatisfaction included technological challenges, ease of use and the learning curve. Trauma surgeons and referring physicians mostly focused on these process challenges, felt the main benefit was in giving patients/families further understanding rather than influencing clinical decisions around transfer. 36
Consumers
No study reported on patient satisfaction. Parent/guardian satisfaction was reported in three studies.36,46,49 Two used surveys46,49 and one collated feedback from the study's family advisory board. 38
Dharmar et al. reported parents of children presenting to rural EDs in California, United States in the highest triage category had significantly better satisfaction on a 10-point scale with care given via telemedicine (n = 48/68) compared to telephone consultation (n = 27/27), including: ED nurse courtesy (6.69 vs 5.74, p < 0.01); ED physician courtesy (6.60 vs 5.74, p < 0.01); knowledge and skills of ED physician (6.45 vs 5.56, p < 0.01); explanation of what was done (6.39 vs 5.41, p < 0.01); overall ED quality of care (6.41 vs 5.63, p < 0.02); and overall ED experience (6.37 vs 5.33, p < 0.01). 46 Most parents (91%) indicated that they would take part in a future telemedicine consultation, with a similar number (87%) rating it as ‘extremely important’ in their child's care. High parental satisfaction was also reported in Marcin et al.'s study of telemedicine usage in the treatment of paediatric trauma patients in an adult ICU in California, United States, although with no comparator: 76% satisfaction with telemedicine; 90% satisfaction with the quality of medical care; 84% satisfaction with the ability to communicate; and 74% satisfaction with their questions being answered appropriately. 49
Rosenthal et al.'s evaluation of telemedicine use in paediatric trauma consultations in California, United States, supported the notion that telehealth improves the experience of receiving care, particularly the relationship with providers and the ability to ask questions. However, this was mostly gleaned from nursing comments about the benefits to families: ‘Mom said that she appreciated the video visit because she knew what to expect and that eased her anxiety’. 36
Intervention uptake, including barriers and facilitators to implementation
Three studies suggest that telemedicine is increasingly being utilised.7,19,50 Hernandez et al.'s study of telemedicine usage for paediatric patients presenting to rural Californian EDs demonstrated a steady increase in the number of consultations and number of centres from 2000 to 2014. 19 Zorin et al.'s study of telemedicine requests for paediatric trauma in Russia found a threefold cumulative increase in the number of telemedicine requests between 2020 and 2022. 50 Rimal et al.'s study on telemedicine usage in paediatric orthopaedic trauma in Western Australia published a 30% increase in telehealth during the two years of the study. 7
Two studies explicitly explored barriers to the onboarding of telemedicine programs,19,36 with one reporting facilitators as well. 36 Hernandez et al. suggested barriers associated with the usage of telemedicine throughout rural hospitals in the United States included equipment failure/technology issues and staff changes requiring ongoing education. 19 In Rosenthal et al.'s interim report of their RCT in the United States, barriers included: staff not remembering or being confused about when to utilise telemedicine; staff perceptions about medical utility in an acute situation; receiving hospital staff unavailable; and resuscitation bays lacking space for a telemedicine cart. 36 The only reported facilitator was positive clinician perception about telehealth prior to usage. 36
Discussion
This scoping review is the first to focus exclusively on telemedicine in acute paediatric trauma, although others have included paediatric patients as a subset of a broader group. 52 We found a paucity of high-quality evidence: existing studies being few, mostly retrospective, often mixed with conditions other than trauma, reporting disparate outcomes, and not always including a comparator. Nevertheless, the limited available literature highlights the application of telemedicine for a range of trauma types, predominantly to support links between mixed EDs and paediatric critical care specialists in tertiary children's hospitals. The available evidence indicates that telemedicine may alter clinical investigations and initial management and streamline disposition, leading to improvements in the quality of care and survival. End-user satisfaction was generally higher with real-time audio and visual communication than with telephone consultations alone, and highest amongst nurses and parents, with some evidence that trauma surgeons may be sceptical about its utility in the acute setting.
All nine included studies were undertaken in high-income countries with large geographic coverage (US, Australia and Russia). This is not surprising, given that telemedicine has the potential to address the disparities in access to healthcare that countries with large distances between tertiary paediatric hospitals face. As well as firming up infrastructure and guidelines for the use of telemedicine in high-resource countries where it already exists, it has the potential to be beneficial in lower-resourced countries with a dispersed population and poorer access to specialist care. In addition, large distances need not be a prerequisite to its use and benefit, with the potential for telehealth to be integrated into the assessment and stabilisation of injured children at any mixed ED prior to and during transfer by paediatric and trauma retrieval services. Its usefulness in supporting non-specialist physicians to provide quality care has been demonstrated in adult trauma. 52 Indeed, rural mixed EDs typically have more experience treating paediatric patients than urban mixed EDs located close to PTCs, where paediatric trauma is often diverted towards. Outcomes and use of telemedicine in these urban mixed EDs remain understudied.
Further, the available evidence indicates a tendency for telemedicine consults to be more likely requested for younger and more severely injured patients. The mean age of patients in five of the nine studies in this review was less than 8 years, while the mean age of childhood trauma is around 9–11 years. 53 Contrary to our finding that telemedicine is utilised for more severely injured patients, one study in non-trauma populations demonstrated that when telemedicine is involved in the referral and transfer of children from remote EDs, the child has lower illness severity on arrival. 54 This is likely due to the lack of paediatric expertise, equipment and experience in referring peripheral mixed EDs. 27
The benefits of telemedicine in paediatric trauma settings are important to establish, as paediatric trauma patients suffer higher mortality rates when treated in adult-focused hospitals. 55 One included study revealed that telemedicine decreased predicted mortality rates. 49 However, it is important to note that the goal of telemedicine in the setting of acute trauma care is not to replace the value of the local physician, but to augment care with sub-specialised paediatric experience. Considering this, our review and others 32 indicate that telemedicine is likely to improve patient outcomes, although further research that is adequately powered for safety-related outcomes is required.
Our review also suggests that telemedicine has the propensity to better allocate resources, decreasing rates of unnecessary transfers to a tertiary hospital or admission to the local hospital. When transferred, telemedicine allows for care to be streamlined, with patients more likely to bypass the transfer ED and be admitted directly to the tertiary paediatric ICU or operating theatres. Although our review did not report a difference in length of stay attributable to telemedicine, decreasing the time that children spend in the hospital maximises the use of health resources and decreases healthcare expenditure. 56 Delivery of care in hospitals closer to home also improves the quality of life for both children and their vital support networks, as well as decreasing personal travel and accommodation costs for families. 57
The available evidence demonstrates a trend for clinicians and parents to have higher satisfaction rates with care provided with telemedicine than those provided via telephone or transfer without any consultation. This is significant as stakeholder satisfaction is an important facilitator in the uptake of new technologies. Measuring patient and provider satisfaction has numerous limitations that have been well described in the literature, 58 including lack of uniformity in instruments across studies, use of non-validated measurements and demonstrable ceiling effects of inability to detect differences at higher thresholds. 59 Future research is needed to explore the various domains of satisfaction, that is, which specific elements of the telemedicine visit patients and clinicians find satisfactory and unsatisfactory, and how these can be improved. 34 Also, satisfaction scores inherently favour satisfaction with the process of care, rather than the care efficacy itself, 58 which can be negated by using independent and qualified observers, as used in Dharmar et al.'s study. 46
Notably, no studies to-date have evaluated patient satisfaction with telemedicine. Assessment of paediatric patient satisfaction with care is notoriously difficult, although tools do exist. 60 This is compounded by the trauma setting of this review, in that children suffering from severe trauma may have variable levels of consciousness, making an assessment of satisfaction increasingly difficult. Nevertheless, this is an outcome that should be further quantified and studied in future research.
Limitations
The findings of our review should be considered in the context of the following limitations. Given our objective of determining the evidence base for telemedicine in the acute setting of paediatric trauma, we excluded the use of telemedicine for other paediatric patient populations, as well as its use in non-acute trauma situations, such as for patient follow-up. We also excluded tele-interventions that did not involve real-time audiovisual interfacing, as this best aligned with the current standard of acute telemedicine care in New South Wales, Australia. Nevertheless, it should be recognised that image store and forward technology and audio-based phone calls still play a role in trauma cases, particularly low-severity orthopaedic or plastic trauma. 61 By limiting the search to English language publications, relevant studies in other languages and potentially lower-resourced settings may have been missed. This may have contributed to the narrow geographic coverage of included studies and limited diversity in patient cohorts.
There are also limitations inherent to scoping reviews. To adequately explore all available evidence, we included some papers that were not exclusively made up of trauma patients, with one study having only 6% of the patient population as suffering from acute trauma. Hence, the included results may not be representative of a paediatric trauma population, given the small sample size of included trauma patients, instead representing a broader population of those with acute paediatric illnesses. The overall quality of the included literature was also poor, with all but one study being retrospective in nature and three studies not having control cohorts. This reflects the limited breadth of the evidence base and highlights the need for prospective study designs in future research.
Conclusion
When employed to connect rural and mixed urban EDs with PTCs, the available evidence shows that real-time telemedicine has the potential to influence initial management and improve appropriate disposition rates, with demonstrated improvement in care quality and survival rates, as well as improved stakeholder satisfaction. It is also well accepted by parents, although it still faces challenges in acceptance by clinicians. However, significant gaps in our understanding of the process and outcomes of telemedicine-supported care models in the care of paediatric trauma patients remain. Further high-quality research examining both the process and impact of telemedicine in the management of paediatric trauma populations is needed to inform the design, delivery and optimisation of care models. These results may contribute to a paradigm shift, allowing for the safe treatment of paediatric trauma patients in rural and mixed ED settings where access to specialist paediatric services is limited.
Supplemental Material
sj-docx-1-tra-10.1177_14604086261458038 - Supplemental material for The use of telemedicine in paediatric trauma: A scoping review
Supplemental material, sj-docx-1-tra-10.1177_14604086261458038 for The use of telemedicine in paediatric trauma: A scoping review by James Cope, Anna Palagyi, Chiara Lamond, Emily Smelt, Michael McCarron, Julie Brown and Susan Adams in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086261458038 - Supplemental material for The use of telemedicine in paediatric trauma: A scoping review
Supplemental material, sj-docx-2-tra-10.1177_14604086261458038 for The use of telemedicine in paediatric trauma: A scoping review by James Cope, Anna Palagyi, Chiara Lamond, Emily Smelt, Michael McCarron, Julie Brown and Susan Adams in Trauma
Supplemental Material
sj-docx-3-tra-10.1177_14604086261458038 - Supplemental material for The use of telemedicine in paediatric trauma: A scoping review
Supplemental material, sj-docx-3-tra-10.1177_14604086261458038 for The use of telemedicine in paediatric trauma: A scoping review by James Cope, Anna Palagyi, Chiara Lamond, Emily Smelt, Michael McCarron, Julie Brown and Susan Adams in Trauma
Footnotes
Author contributions
Study conception and design: AP, JB, SA; data acquisition: JC, AP, CL, ES; analysis and data interpretation: JC, AP, CL, SA; drafting of the manuscript/critical revision: JC, AP, CL, ES, MM, JB, SA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
The study protocol was registered in PROSPERO (CRD420250568405).
Provenance and peer review
Not commissioned, externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.