
Abstract
Objective
To evaluate and identify commonalities among pediatric firearm-related injuries in the diverse metropolitan and micropolitan population of Upstate South Carolina.
Methods
A retrospective chart review was conducted of 104 patients aged 0–17 years who presented to Greenville Memorial Hospital from January 1, 2017 to July 1, 2023 and were diagnosed with a firearm-related injury.
Results
Patients were predominantly male (77.9%), Black (54.8%), with an average age of 11.9 years. Unintentional injury was the most common intent among all ages and races (44.2%). Unintentional injury was more likely among pre-teens, while assaultive/homicidal injuries were more likely among ages 13–17 (p = 0.002). Assault/homicide was more likely among Black children, and self-inflicted injuries were more likely among White children (p = 0.039). Residence was the most common location (46.2%). Of the patients eligible for psychiatric consultation, 21.5% received one. The distress level of the community impacted frequency, though it was not predictive of intent.
Conclusions
Though disparities based upon sex and race exist, unintentional firearm-related injury is universally problematic in the Upstate South Carolina. Efforts directed at reducing unintentional injuries, improving documentation, and championing psychiatric consults may reduce pediatric firearm-related injuries and sequelae in the Upstate.
Introduction
Firearm-related injuries are now one of the top five causes of death for adults, and they are on the rise in the pediatric population. 1 For years, motor-vehicle crashes had been the leading cause of mortality in the pediatric population, but firearm-related injuries surpassed motor-vehicle crashes as the leading cause of death in the pediatric population in 2020, with a mortality rate of 6% and a relative increase in firearm-related deaths that is more than twice that of the general population.2–5 More alarming is that the majority of both fatal and non-fatal firearm-related injuries occur with assaultive intent. 5 Unfortunately, despite efforts aimed at the prevention of firearm-related injuries, we have seen an increase in the number of fatal firearm-related injuries in children from 2013 to present.6–8 The reason for this dramatic increase is unknown and is most likely multifactorial.
As is the case with adults, there are certainly disparities with regard to the prevalence and frequency of pediatric firearm-related injuries. The most recent data on pediatric firearm-related injuries reported to the National Trauma Data Bank (NTDB) released in 2016 indicated that Black and male children are disproportionately affected by firearm-related injuries, with accidental discharges being more common among young children, the majority of assaults being Black children, and the majority of suicides being White children.3–5,9 Other studies have examined disparities in location. One of such studies determined that rural areas had higher rates of suicide and unintentional firearm-related death, and urban areas had higher rates of homicide for ages 0–19. 10 Another set of studies found that although firearm-related injuries are more common overall in large cities, the rate when adjusted for population is highest in smaller cities.11,12 The consensus for years has been that pediatric firearm-related injuries are not strictly an urban problem, though most literature focuses on either urban areas or rural areas and does not adequately examine social factors. 5
The importance of identifying these individual and neighborhood-level factors that may be contributing to the increase in pediatric firearm-related injuries has certainly been amplified by the scientific community. Some studies have begun to examine these factors, noting that societal issues like the density of grocery and alcohol retailers are associated with differences in rates of violent crime.13,14 Another study from a single county in Texas found that the odds of sustaining firearm-related injuries in children were higher in areas of socioeconomic disadvantage, though this was not significant when adjusted for demographics. 15 Lastly, a retrospective review of children under 16 years presenting to a single trauma center from 2010 to 2019 found that increased socioeconomic deprivation is associated with more firearm-related injuries requiring hospitalization. 16 Needless to say, further investigation is warranted in order to make clearer and better elucidate any associations between pediatric firearm-related injuries and social factors.
This descriptive study aims to evaluate all firearm-related injuries in the Upstate of South Carolina (SC) in children ages 0 to 17 years and identify any commonalities amongst the events surrounding and children sustaining firearm-related injuries. This includes assessment of the social factors, the incident itself, and what happens to and for the child after the injury has occurred. Notably, this study addresses prevalence of psychiatric consultation at the time of injury, and it also utilizes community resources and quantified distress levels to evaluate for location and community-based trends in pediatric firearm-related injuries. The northwestern corner of SC, also known as the Upstate, is of particular interest due to its diversity of urban and rural, micropolitan and metropolitan areas with a population of variable demographics and socioeconomic status. This information may assist in determining the impact of community distress and resources, if any, on trends in pediatric firearm-related injuries. This information may also assist in identifying trends present in areas with a mixture of metropolitan and micropolitan populations. This may offer directional change and provide more insight into factors that may reduce pediatric firearm-related injuries and associated sequelae.
Methods
General information
Institutional Review Board (IRB) approval was obtained to conduct this study. The IRB waived the requirement for the obtention of a signed informed consent form for participants. Neither patients nor guardians were contacted for further information. In cases where the numbers are few, information was omitted in order to protect patient confidentiality.
Data collection
A retrospective chart review was performed for patients 0–17 years presenting to the Prisma Health Greenville Memorial Hospital emergency department and trauma center from January 1, 2017 to July 1, 2023, diagnosed with a firearm-related injury. Data collection included patient name, patient demographics (age, date of birth, sex, race, ethnicity), medical record number, zip code and county of residence, injury mechanism (self-inflicted, accidental, intentional, etc.), place and date of injury, need for operative intervention, presence of psychiatric consultation, length of hospital stay, and disposition at discharge. Pediatric psychiatric consult was not applicable for children whose disposition was death.
Additional patient and community-centered data pertaining to social factors were collected. Department of Social Services (DSS) involvement, history of DSS involvement, history of Department of Juvenile Justice (DJJ) involvement, and concern for or confirmed gang involvement were also factors identified. The number of grocery stores and alcohol retailers in each zip code was obtained. The Distressed Communities Index (DCI) was also determined for each zip code. DCI is a measure that utilizes census data to assign a value that quantifies community distress for each zip code, rated 0 (most prosperous) to 100 (most distressed). Measures factored into DCI score include education level, housing vacancy rate, employment status, poverty rate, median income ratio, changes in employment, and changes in establishments in the area.
Residence and injury zip codes were not utilized if the patient’s chart had contradictions or inconsistencies in those areas of the medical record. If the chart had stated that the patient was not living at the address listed in the contact information or at the residence of the legal guardian, the address that best reflected where the child was actively living was utilized.
“Unknown” and “Unspecified” were used in the cases of ambiguous information, for example, an unknown location or unspecified history of DSS involvement. Children of all ages were included, seeing as SC does not have a lower limit for delinquency offenses.
Data source
Patient information was obtained from the Prisma Health Upstate medical record system called Epic Systems, patient charts, and trauma registry. RedCAP was utilized to consolidate information. Accessible visits at other hospitals before and after the incident of interest were utilized when applicable (e.g., DSS and DJJ history) and accessible. Interactions, contact information, notes, and media files from the patient record were utilized to obtain patient and incident information. Demographic information was utilized as it was displayed in the medical record.
The Department of Health and Environmental Control (DHEC) was utilized to obtain the number of grocery retailers in both the injury and residence zip codes. Grocery stores were identified from the SC Food Grades database. The data provided is from July of 2020 (the earliest available to the public) to July of 2023. Each store was only included once. Fresh food markets were pulled from the Farmers’ Markets and Roadside Markets database. The Department of Revenue (DOR) databases were utilized to obtain the number of alcohol retailers for each zip code. “Off Premises Beer & Wine” and “Retail Liquor Store” license types were included. The two lists were cross-referenced to ensure each location was only counted once.
Rural Urban Community Area (RUCA) codes provided by the United States Department of Agriculture were utilized. DCI scores were obtained using the Economic Innovation Group's interactive map. Zip codes for each injury and residence were typed into the search bar, and the resultant DCI was recorded.
Great-circle distance on a sphere was utilized in conjunction with Google Maps to obtain distance between the residence and injury locations for each incident. Google Maps alone was used for residence-injury pairs within the same zip code. A specific address was utilized when provided. Distance between the injury and residence site was obtained using best judgment, for example, in cases of “the woods next to our house.”
Statistical analysis
Fisher's exact test was utilized to assess potential associations between patient characteristics and intentionality of firearm injury. P-values <0.05 were considered to be statistically significant. SAS Enterprise Guide 8.3 statistical software was used for all statistical analyses (SAS Institute, Cary, NC, USA).
Results
Demographics and patient history
Of the 104 pediatric patients who sustained firearm-related injuries, 77.9% were male, 54.8% were Black, 81.3% of known residences were metropolitan by RUCA score, and the average age was 11.9 years (CI 10.9–12.7 years) (Table 1). Of the patient histories obtained, 25.0% had confirmed history with DSS, 15.4% had confirmed history with DJJ, and a combined 15.4% had confirmed or concern for gang involvement. The history of DJJ involvement was not correlated with the intent of the shooting when children under 12 years of age were excluded (p = 0.263, Online Supplementary Material A). Children ≤12 years old with a firearm-related injury were significantly more likely to have a history of DSS involvement than children 13–17 years old with a firearm-related injury (p = 0.023, Online Supplementary Material B). The history of DJJ involvement was a category too small to analyze by Fisher's exact test, though no demographic category was significantly more likely to have had DSS or DJJ involvement when evaluated together (Online Supplementary Material C).
Demographics of pediatric patients with firearm-related injuries.
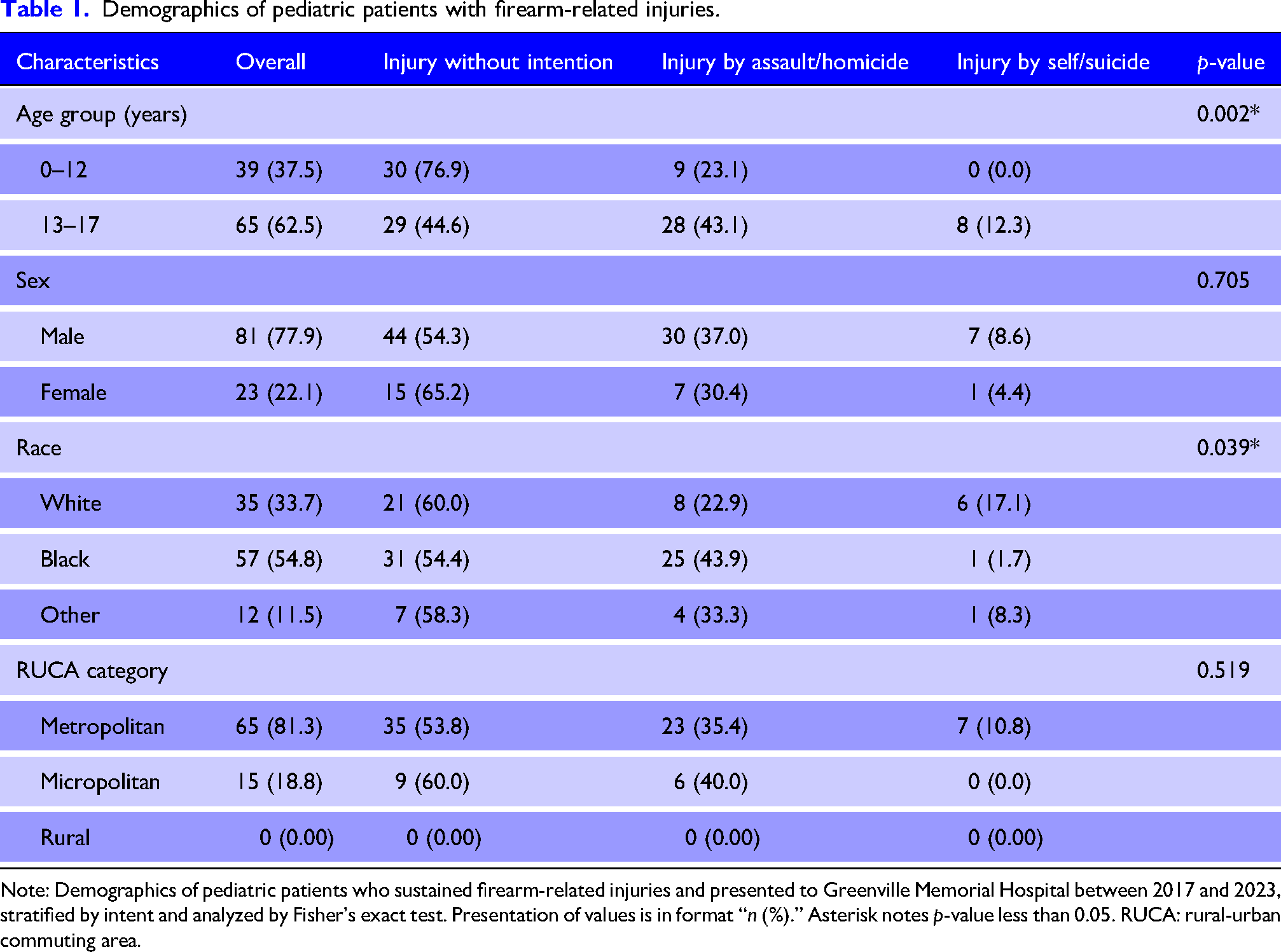
Note: Demographics of pediatric patients who sustained firearm-related injuries and presented to Greenville Memorial Hospital between 2017 and 2023, stratified by intent and analyzed by Fisher's exact test. Presentation of values is in format “n (%).” Asterisk notes p-value less than 0.05. RUCA: rural-urban commuting area.
Injuries
With regards to the year of presentation for firearm-related injury, 13 occurred in 2017, 15 occurred in 2018, 12 occurred in 2019, 20 occurred in 2020, 24 occurred in 2021, 17 occurred in 2022, and three occurred in the first 7 months of 2023. Children 12 years and younger were more likely to sustain a firearm injury unintentionally, while children ages 13–17 were more likely to sustain a firearm injury by assaultive or homicidal intent (p = 0.002, Table 1). Unintentional injury was the most common reason for injury among all races and ethnicities, as well as in both metropolitan and micropolitan areas (Table 1). Unintentional injury was the most common reason for injury in the years 2018, 2021, and 2022, while assaultive or homicidal intent was the most common reason for injury in the years 2017 and 2020. Assault or homicide was more likely among Black children, while self-inflicted injuries were more likely among White children (p = 0.039) (Table 1). The average residence to injury distance was 13 miles (CI 28.2–0 miles). The in-state average residence to injury distance was 4 miles. Of the firearm-related injuries sustained, 44.2% of incidents were unintentional, 35.6% were sustained by assaultive or homicidal intent, and 6.7% of cases were sustained by suicide attempt (Figure 1). Of the firearm-related injuries sustained, 46.2% of the incidents occurred in a residence, 14.4% occurred in a garden or yard, 13.5% occurred in a vehicle, 10.6% occurred on a street or highway, and 5.8% of locations were unspecified in the medical record (Figure 2). Of the 46 unintentional firearm-related injuries, 67.4% were sustained in a residence. No statistically significant relationship existed between either current DSS involvement or DJJ involvement with intent (p = 0.065, p = 0.263, Online Supplementary Material A).
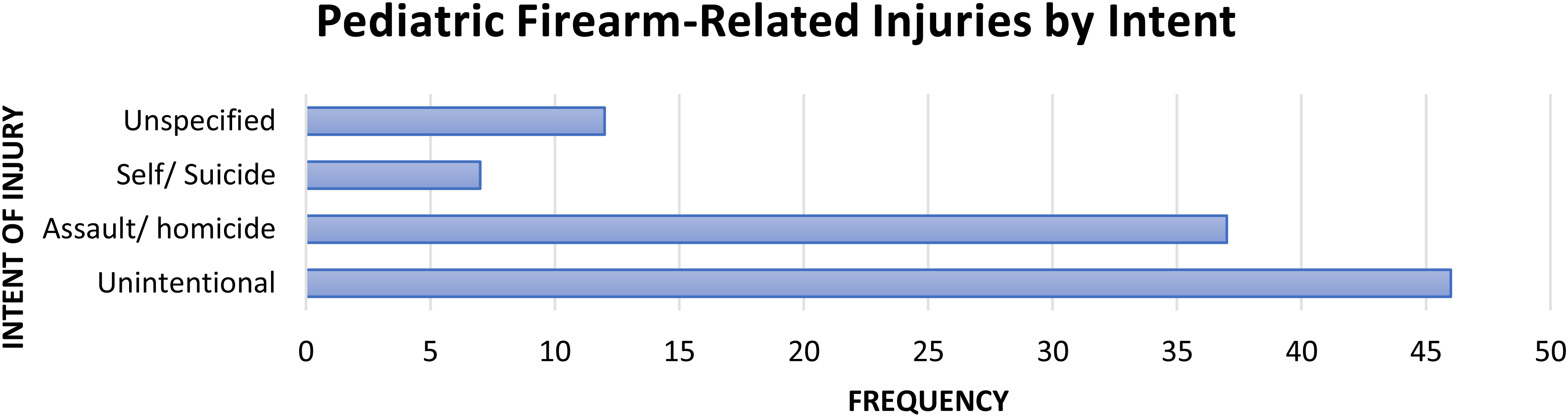
Pediatric firearm-related injuries by intent. Firearm-related injuries of pediatric patients ages 0–17 years who presented to Greenville Memorial Hospital from January 1, 2017 to July 1, 2023 and were diagnosed with a firearm-related injury, stratified by intent of injury.
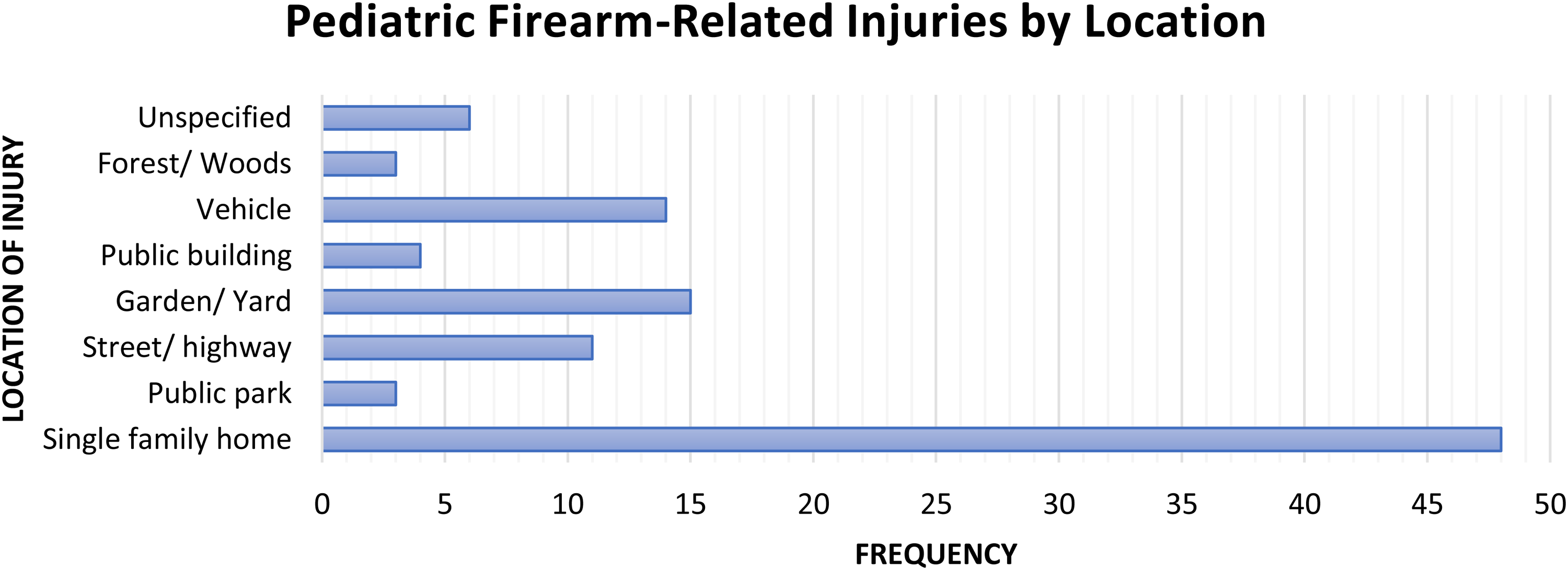
Pediatric firearm-related injuries by location. Firearm-related injuries of pediatric patients ages 0–17 years who presented to Greenville Memorial Hospital from January 1, 2017 to July 1, 2023 and were diagnosed with a firearm-related injury, stratified by location of injury.
Community information
The mean RUCA score was 1.7. The average DCIs of the residences and injury sites were 57.9 and 59.3, respectively. Of the residence DCIs, 25.5% were categorized as distressed, 23.5% as at risk, 23.5% as mid-tier, 17.7% as comfortable, and 9.8% prosperous. Of the injury DCIs, 29.1% were categorized as distressed, 19.0% as at risk, 25.3% as mid-tier, 17.7% as comfortable, and 8.9% as prosperous (Figure 3). Of the 102 residence-injury zip code pairs, 55 injuries occurred in a zip code with the same DCI, 10 injuries had a higher DCI, and 37 injuries had a lower DCI. However, no statistically significant relationship exists between DCIs of residence and injury locations (Figure 3). The majority of both residence and incidence zip codes had more alcohol retailers than grocery retailers. DCIs of injury and residence were not correlated with intent of the shooting (p = 0.475, p = 0.396, Online Supplementary Material A). Unintentional injury was the most common reason for injury in almost all DCI tiers (Table 1).
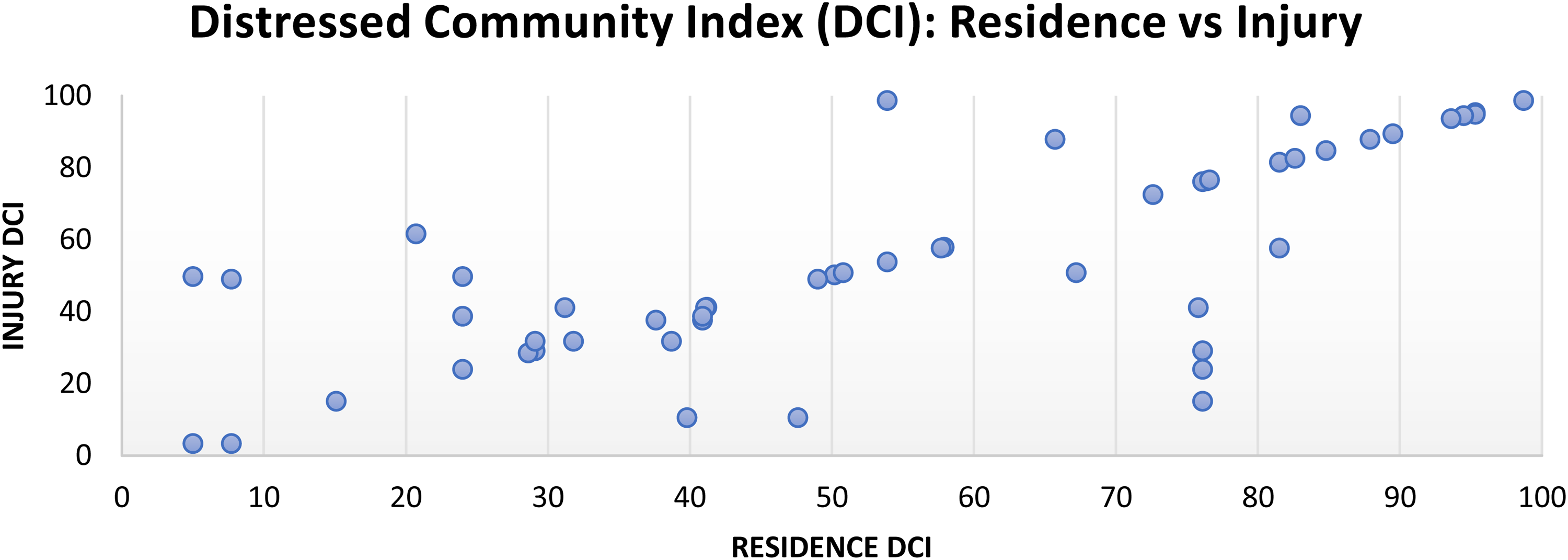
Pediatric firearm-related injuries by Distressed Community Index (DCI). DCI of residence and injury locations for each firearm-related injury of a pediatric patient age 0–17 years who presented to Greenville Memorial Hospital from January 1, 2017 to July 1, 2023 diagnosed with a firearm-related injury.
Clinical course
Of the pediatric patients who sustained firearm-related injuries, 53.8% presented initially to Greenville Memorial Hospital, and the remainder were transferred in. Initial presentation was by ambulance in 48.1% of cases. Emergency department disposition was to the floor in 44.2% of cases, intensive care unit in 21.2% of cases, and operating room in 27.9% of cases. In 3.8% of cases, the patient died prior to disposition to a secondary location. The average length of hospital stay was 6.37 days (CI 4.0–8.8 days). Of the patients eligible to receive a psychology or psychiatry consult, 21.5% received one. Unfortunately, 10.6% of these firearm-related injuries resulted in death of the child. Of these firearm-related injuries that resulted in death, four occurred with assaultive or homicidal intent, three occurred with the intent of suicide or self-harm, and three were unintentional.
Discussion
Results from this study are generally consistent with a mixture of present literature from both rural-based and urban-based studies. Much like data out of urban centers, this study demonstrates that disparities exist with regard to race and sex. This study also demonstrates that unintentional injury is a significant contributor to firearm-related injuries in pediatric patients, similar to results from rural centers. Additionally, unintentional injuries were the most common cause of injury in both age groups, both sexes, all races, almost all DCI tiers, and both metro and micropolitan areas. This differs from national data that suggests that the most common cause for pediatric firearm-related injury is assaultive or homicidal intent. When it comes to children in the Upstate, no group is left unaffected by accidental and unintentional pediatric firearm-related injuries. The Upstate may therefore benefit from efforts directed at addressing unintentional firearm-related injuries specifically.
When considering the fact that results in the Upstate varied in this regard, one must consider generalizability and potential disparities present in national data, as well as the local sociopolitical environment and cultural factors pertaining to the area. While the Upstate did share similarities with urban centers with regard to demographic data, the Upstate also shared similarities with rural centers with regard to intent. Despite being considered one of the most populous cities in South Carolina with rapid population growth, Greenville holds thousands of acres of sparsely populated farmland and rural catchment with gradual loss to development.17–19 While none of the zip codes in this study were considered to be rural, it is reasonable to suspect that the rapid growth, paired with the culture of the rural landscape, lends well to the array of results seen here. Of course, this is likely multifactorial and further research would need to be conducted to better characterize these findings in context.
While disparities in the Upstate do exist, pediatric firearm-related injuries are not barred by the distress level of the community or the history of the patient. While other studies suggest that measures of socioeconomic factors were correlated with intent, this study found no such association. 16 On the other hand, greater numbers of firearm-related injuries were seen in locations with higher DCI scores, indicating that addressing social determinants may still be helpful. While we found no association between DCI and intent, DCI is merely one conglomerate score of a variety of socioeconomic factors, and this does not mean that an association between one or more socioeconomic factors and intent does not exist. In addition, the majority of both residence and incidence zip codes pertaining to these injuries had more alcohol retailers than grocery retailers. It is important to remember, however, that DCI is not all-encompassing with regard to the assessment of socially relevant factors, and further investigation of other socioeconomic and social determinants is still warranted. It may be useful to parse out individual factors used to generate these indices, as it may allow for a more detailed investigation of the factors at play.
Additionally, the impact of the COVID-19 pandemic must be considered. The Upstate saw its greatest number of pediatric firearm-related injuries during 2020 and 2021, which is consistent with increases in pediatric firearm-related injuries seen during the COVID-19 pandemic nationally. 20 While all age groups and sexes experienced an increase in firearm-related injuries during the COVID-19 pandemic, children ages 0–14 years experienced the greatest increase in firearm injury emergency department visits, and the Upstate was no exception. 21 The pandemic has been considered an inciting event for pediatric firearm-related injuries, particularly due to the increase in firearm sales during the time period, limited parental supervision, disruptions to daily routines and schooling, social isolation, housing and financial insecurity, and reduced access to mental health services. 21 This increase is not surprising, considering the fact that COVID-19 exacerbated many socioeconomic factors, some of which have been correlated with increases in pediatric firearm-related injuries.16,22 The COVID-19 pandemic has been considered an inciting event for these reasons, though this increase in incidence had been seen prior to the COVID-19 pandemic and far exceeded pre-pandemic trends, suggesting this issue is likely multifactorial.2,23
Lastly, it is important to recognize that children sustaining firearm-related injuries are more likely to suffer mental health disorders, substance-related disorders, and addictive disorders in the future. 24 It is also important to recognize that ensuring access to psychiatric care following a firearm-related injury lends to improved outcomes for the child. 25 Moreover, socioeconomic disparities exist with regard to which children have access to mental health resources following a firearm-related injury.19,21 It is imperative that psychiatric consults be administered to children who sustain firearm-related injuries in order to prevent mental health sequelae. With so few patients receiving consultation at the time of the incident, it is imperative that this be addressed to ensure affected children are properly assessed and cared for.
With regards to limitations of this study, social factors (e.g., DSS/DJJ history) were not reliably reported in the medical record. Given that SC also has no minimum age for sentencing, we included patients of all ages in the analysis of DJJ and gang involvement, which may affect the statistical significance. Location was also difficult to discern from the information documented. Many children were living with friends or extended family, moving, or experiencing homelessness. Many of the temporary addresses in these cases were left unspecified. Inclusion of housing instability as a factor was considered, though reporting was far too inconsistent and too unclear to be recorded more formally or quantified. It would be to the benefit of future research efforts to improve documentation and describe in greater detail the socially relevant factors that pediatric patients and their guardians face when children present to the hospital with firearm-related injuries. More importantly, documentation of patient location is paramount for contact, follow-up care, connecting patients with accessible resources, and maintaining patient safety. Hopefully, these efforts will assist in both improving patient welfare and developing future studies that may identify these socially relevant factors that need to be addressed.
Conclusions
Our results show similarities with those of both urban and rural centers. Disparities based upon gender and race exist with regard to prevalence of firearm-related injuries in the Upstate of SC, with Black and male children being disproportionately affected. Unintentional injuries are the most common cause of injury in both age groups, both sexes, all races, almost all DCI tiers, and both metro- and micropolitan areas. No correlation was found between socioeconomic factors and intent, though greater numbers of firearm-related injuries were seen in locations with higher DCI scores; addressing social determinants of health may be helpful. There is room for improvement with regard to the documentation of patient location and the administration of psychiatric consults for children who sustained firearm-related injuries. Firearm-related injuries are a public health concern, and innovative strategies are required to address the underlying issues. Seeing as unintentional firearm-related injuries are universally problematic in the Upstate, this area may benefit from efforts directed at addressing unintentional firearm-related injuries.
Supplemental Material
sj-docx-1-tra-10.1177_14604086261458045 - Supplemental material for Pediatric firearm-related injuries in the South Carolina upstate: A descriptive analysis
Supplemental material, sj-docx-1-tra-10.1177_14604086261458045 for Pediatric firearm-related injuries in the South Carolina upstate: A descriptive analysis by Haley Wymbs, Vanessa Hernandez and Robert Ricca in Trauma
Footnotes
Acknowledgments
The authors would like to acknowledge Dawn Blackhurst, DrPH, for the clinical data analysis performed.
Ethical approval
This project has been approved by the Prisma Health IRB.
Author contributions
Haley Wymbs prepared the original manuscript. Vanessa Hernandez revised and edited the manuscript. Robert Ricca supervised the project, revised and edited the manuscript, and provided critical guidance and support.
Data availability statement
The data may be made available upon request to the corresponding author.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.