
Abstract
Background
The aim of this study was to review the spectrum, pattern and clinical outcome of shotgun injuries managed at a major trauma centre with limited resources.
Methods
Patients presenting with shotgun injuries between January 2012 and December 2024 were retrospectively reviewed. This was accomplished using the Hybrid Electronic Medical Registry. Data included demographics, injury pattern, regions affected, diagnostic imaging, operative interventions and clinical outcomes.
Results
During the 13-year study period, a total of 148 patients sustained shotgun injuries. The median age was 31 years and 93% (137/148) were male. The median Injury Severity Score was 9. Of the 148 patients, 76% (112/148) had plain films performed in the resuscitation room, and 76% (113/148) underwent computed tomography following initial assessment. Single body injuries were noted in around half (51%) of the patients, with the remaining sustaining injuries in multiple regions. The abdomen was most commonly injured (46%), followed by the chest (38%) and lower limb (34%). Operative intervention was necessary for 88 patients (59%), of whom 33 (38%) required multiple operations. The median total length of hospital stay was 5 days, with an overall mortality rate of 5% (8/148).
Conclusion
Shotgun injuries are associated with a range of injuries to multiple body regions. These injuries have a high requirement for operative intervention and pose a significant morbidity and mortality risk. High-quality imaging is essential but must be integrated with clinical assessment to guide management.
Introduction
Shotgun (SG) injuries are uncommon, and their management remains challenging. Unlike other ballistic injuries, SG wounds differ substantially due to the unique nature of the projectile involved. SG rounds are designed to result in a wider spread of damage than handgun or rifle rounds. This results in injuries to multiple anatomical areas, with multi-regional involvement reported in 22%–39% of cases.1,2 The ballistic design and pellet properties of an SG round, in combination with the smooth bore of the SG barrel, contribute to this widespread injury pattern, with multiple, distinct, smaller projectiles often scattered over a wide area. The size of the affected area is determined both by weapon characteristics and the distance between the shooter and the target. This difference makes SG injuries distinct from other firearm injuries, and often necessitate surgical intervention given the unpredictable projectile trajectory and injuries to more than one anatomical region. This multi-site involvement increases the risk of overutilising damage control surgery, leading to unnecessary morbidities, prolonged hospital stays and higher mortality rates, despite the fact that non-operative management or targeted surgical approaches may be sufficient. 3 Furthermore, the dispersion of radio-opaque projectiles poses challenges in diagnostic imaging due to the radiological artefacts that can severely hamper correct interpretation. 4 Even in countries with a high burden of firearm-related trauma, SG injuries constitute a minority of cases. South Africa has one of the highest incidences of firearm-related homicide in the world, and trauma is aptly described as a ‘malignant epidemic’. 5 Literature on SG injuries from South Africa is sparse and limited to small series. The aim of this study was to review the spectrum, injury pattern and clinical outcome of SG injuries managed at a major trauma centre in a resource-constrained setting.
Materials and methods
Clinical setting
This was a retrospective study conducted at the Pietermaritzburg Metropolitan Trauma Service (PMTS), Pietermaritzburg, South Africa. The PMTS provides definitive trauma care to the city of Pietermaritzburg, the capital of KwaZulu-Natal (KZN) province. It is one of the largest academic trauma centres in the province and covers a catchment population of over three million. Annual admissions exceed 4000, 50% of which are penetrating trauma.
The study
A retrospective review was conducted on all patients who presented with SG injuries from January 2012 to December 2024. Our regional electronic trauma registry, known as the Hybrid Electronic Medical Registry (HEMR), was reviewed over this period. Data included demographics, injury patterns, body region injuries, diagnostic imaging, operative interventions and clinical outcomes were reviewed. We included all patients with isolated SG injuries, where the SG was either identified by the presenting complaint or pellets on radiological imaging. All dead-on-arrival patients were excluded, and there were no age exclusions.
Injuries were coded from the HEMR using the Abbreviated Injury Scale (AIS), 2015 version (Association for the Advancement of Automotive Medicine, 2015). Injuries were grouped by anatomical region. Where multiple injuries were recorded within the same region, the highest AIS score for that region was used for analysis.
Complications were classified into seven categories (abdominal, wound, respiratory, renal, neurological, cardiac and other) and were defined as any adverse clinical event that arose during the index hospital admission. The time horizon was in-hospital only, as no post-discharge follow-up data were available. Complications were identified through the clinical documentation in the HEMR and were not prospectively coded within the registry. Abdominal complications included anastomotic leak/breakdown, intra-abdominal collections/haematoma, bowel eviscerations and post-operative ileus. Wound complications encompassed any surgical/wound site infections or fascial dehiscence. Respiratory complications included retained haemothoraces, any pneumonia or retained collections. Renal complications were either acute kidney injuries (AKIs) or catheter-associated injuries. Neurological complications included any neurological deficits that arose during the admission, including peripheral nerve injury, compartment syndrome or post-operative delirium. Cardiac complications included any acute coronary events or arrhythmias. Other complications included pressure sores, multiorgan failure and sepsis/septic shock without an attributable anatomical source. Patients could contribute complications to more than one category.
Classification
SG injuries in this study were further classified based on the seminal study by Velmahos et al., 6 which is based on the number and distribution of body regions injured by SG pellets. This classification system offers a practical, anatomical approach in facilitating clinical decisions and an estimate of the wound-victim distance through analysing the spread and pattern of the pellet distributions. However, it is to be reinforced that classification systems serve as valuable guidelines but should not replace clinical examination, encompassing anatomical nuances and understanding the specific injury mechanism. The classification system is divided into three categories: Types I, II and III. Type III wounds involve pellets confined to a single body region. Type II wounds involve pellets spread across two adjacent regions. Type I wounds involve pellets spread across a wider area than in Type II. We applied the same criteria, where specifically, if the pellets were concentrated in the thoraco-abdominal region, the injury was graded as I instead of II. Similarly, if the lateral abdomen and the medial upper extremity were involved, the injury was also classified as I instead of II. Body regions were divided into head and neck, chest, abdomen, upper extremities and lower extremities. Injuries to the face were classified as head injuries, and injuries to the pelvis were classified either as an injury to the abdomen or the lower extremities, contingent upon the clinical context as documented in the patient record.
Statistical analysis
All relevant data were extracted and initially summarised onto a Microsoft EXCEL© spreadsheet for review. Non-parametric (asymmetrical) data were descriptively described. All statistical analyses were conducted using R version 4.5.0 and RStudio version 2024.12.1-563 (Posit, PBC).
Continuous variables were assessed descriptively and are presented as median [IQR] because several clinical variables, including Injury Severity Score (ISS) and length of stay, were non-normally distributed. Categorical variables are presented as n (%). Between-group comparisons across injury types were performed using the Kruskal–Wallis test for continuous variables and Fisher's exact test for categorical variables. Omnibus p-values are presented in the primary tables. Post hoc pairwise comparisons were performed only when the omnibus test was statistically significant, with Holm adjustment for multiple comparisons. Statistical significance was defined as a p-value < 0.05.
Missing data
Missing data were assessed for key demographic, injury severity, physiological, laboratory, imaging, management, and outcome variables and are reported in online Supplemental Table 1. Completeness varied across variables. Injury type, number of injured regions, sex, and imaging variables were complete. ISS was available for 111/148 patients (75.0%). Laboratory completeness was lower, including lactate available for 96/148 patients (64.9%), pH for 101/148 (68.2%), and base excess for 99/148 (66.9%). Analyses used available-case denominators for each variable; no statistical imputation was performed. Blank, unknown, or unavailable entries were treated as missing. For categorical variables, percentages were calculated using the number of patients with non-missing data for that variable as the denominator. For continuous variables, summary statistics and group comparisons were calculated using complete observations for the variable being analysed.
Results
Overview
During the 13-year study period, a total of 148 patients sustained an SG injury and were included in this study. The median age was 31 [25–40] years, and 93% (137/148) were male. The median ISS was 9 [4–16]. The 148 patients were classified into the three groups in the same system stated by Velmahos et al., comprising 29 (20%) patients with Type I injuries, 44 (30%) in Type II and 75 (50%) in Type III. Table 1 summarises the demographics, clinical parameters and outcomes for the three types. The ISS was greatest in Type I injuries, followed by II and III. (19 [12–22] versus 10 [8–13] versus 4 [4–9]; p < 0.001).
Demographics, clinical parameters and outcomes between the three different classification groups.
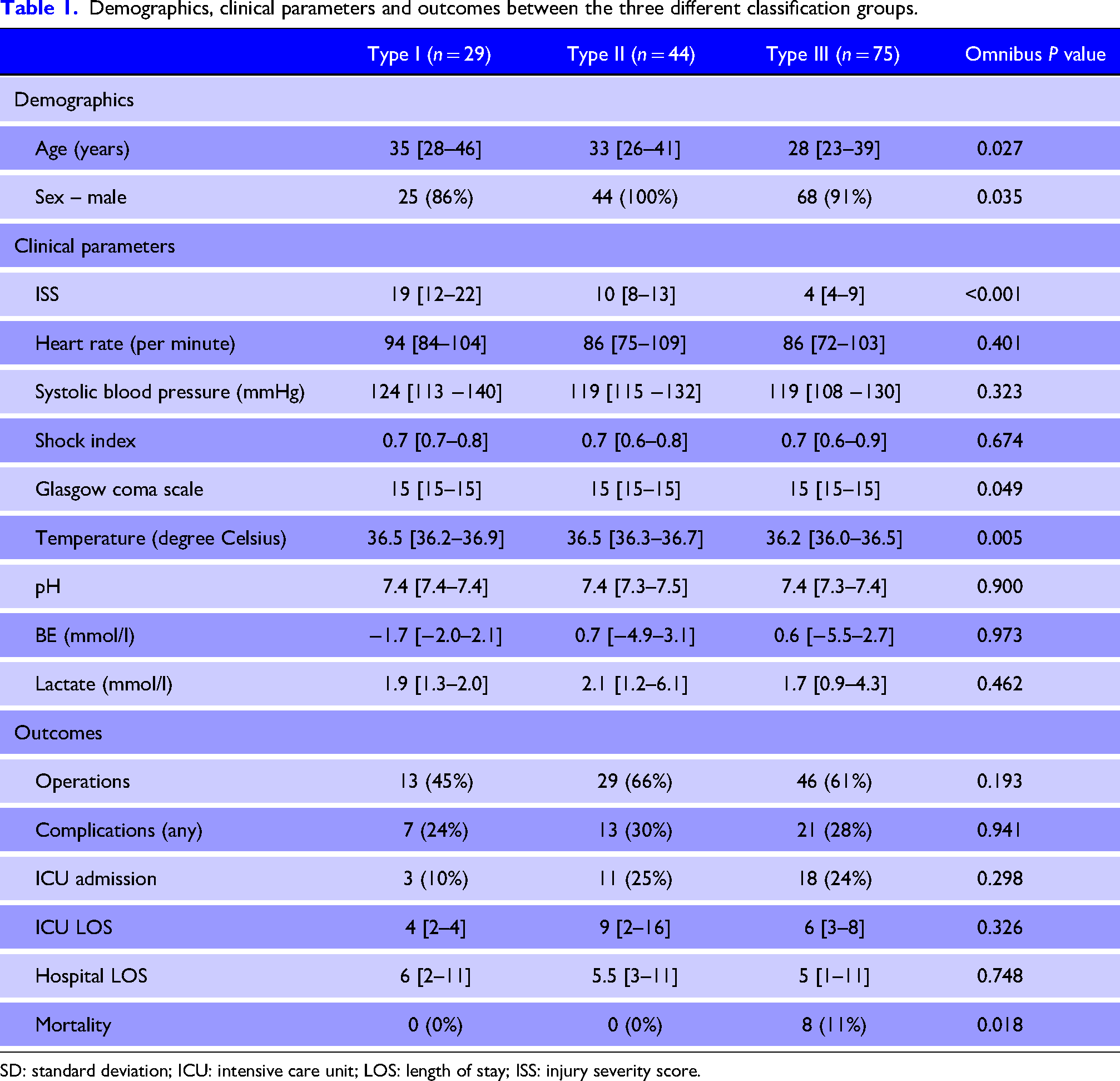
SD: standard deviation; ICU: intensive care unit; LOS: length of stay; ISS: injury severity score.
Spectrum of injury
Of the 148 patients, 76% (112/148) had plain films performed in the resuscitation room, and 76% (113/148) underwent computed tomographic (CT) scans following initial assessment. Table 2 summarises the radiological imaging undertaken.
Imaging modalities undertaken.
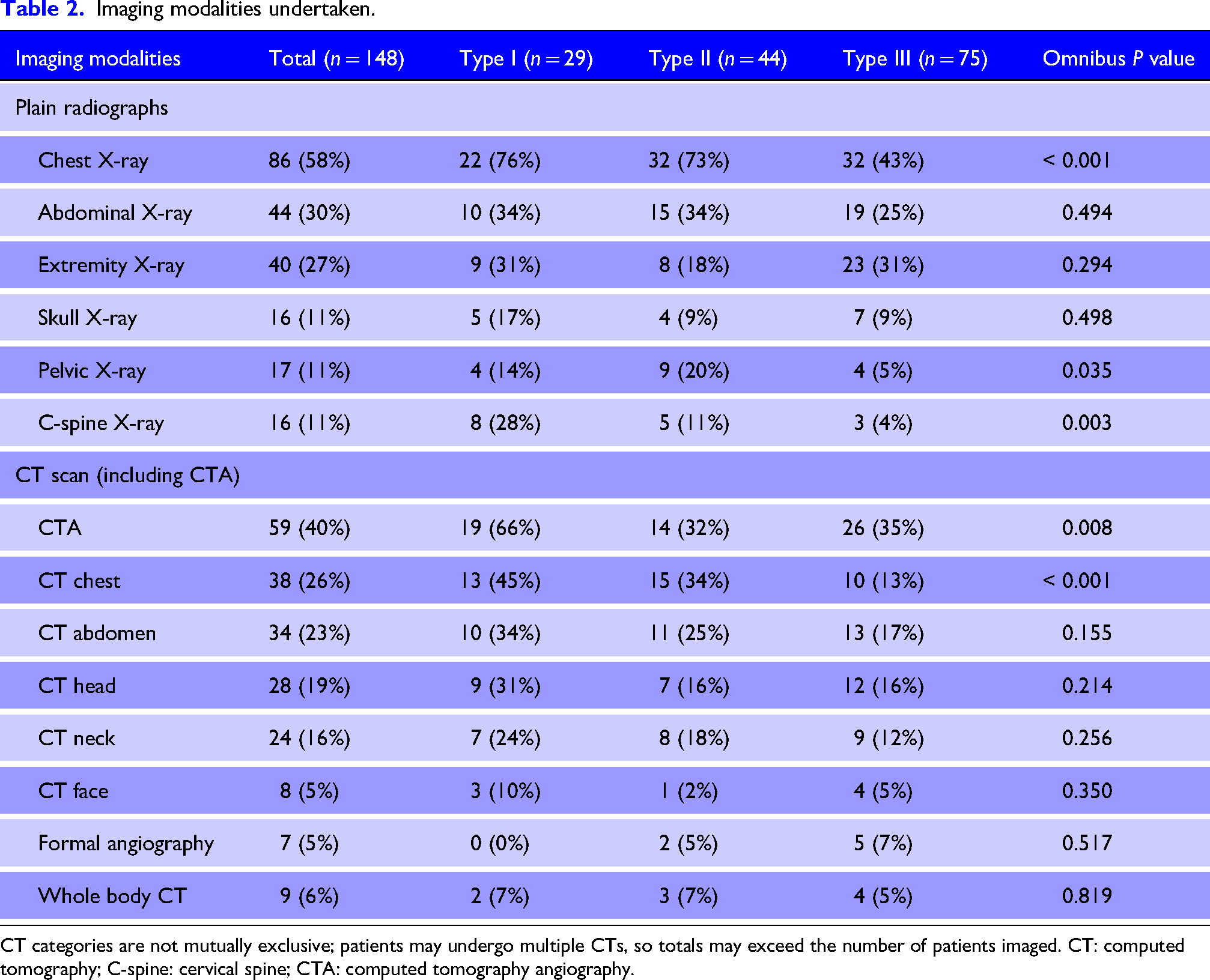
CT categories are not mutually exclusive; patients may undergo multiple CTs, so totals may exceed the number of patients imaged. CT: computed tomography; C-spine: cervical spine; CTA: computed tomography angiography.
Of the 113 patients who underwent a CT scan, one patient (1%) was thought to have a normal CT scan (no injury identified). This patient underwent serial clinical examinations and subsequently clinically deteriorated, prompting a laparotomy, revealing a bladder and rectal injury. All other patients had surgical findings consistent with the CT scan results or did not require any intervention for the region that was scanned. Across the three types of injuries, chest x-rays were most frequently performed in Type I injuries (76%), compared to Type II (73%) and Type III (43%) injuries (p < 0.001). Similarly, CT chest scans were performed in Type I (45%), Type II (34%) and Type III (13%) (p < .001). Overall, 51% of patients had injury confirmed to a single body region, and the remaining had more than one region injured. The most common body region injured was the abdomen (46%), followed by the chest (38%) and the lower limb (34%). Table 3 summarises the body region injured, and Table 4 summarises the AIS by body region.
Body regions injured.

Median AIS by region.
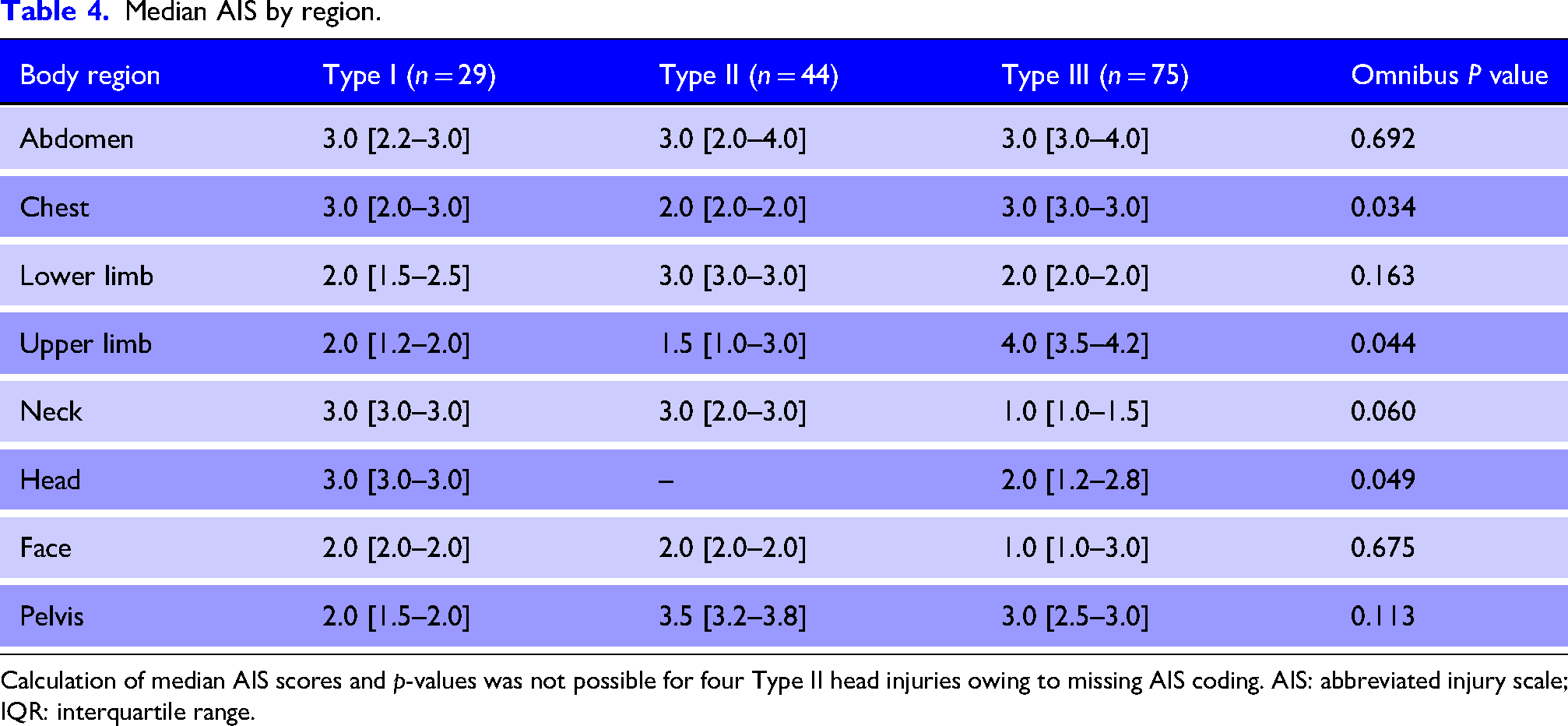
Calculation of median AIS scores and p-values was not possible for four Type II head injuries owing to missing AIS coding. AIS: abbreviated injury scale; IQR: interquartile range.
Management
A total of 88 patients (59%) required operative interventions to manage injuries, and 33 (38%) of these patients had more than one operative procedure. Among patients sustaining Type I injuries, 13 (45%) required an operation, compared to 29 (66%) in Type II and 46 (61%) in Type III; however, there was no statistical significance in the operation rates between the three types (p = 0.193
Summary of the spectrum of operative procedures of the three classification of injuries.
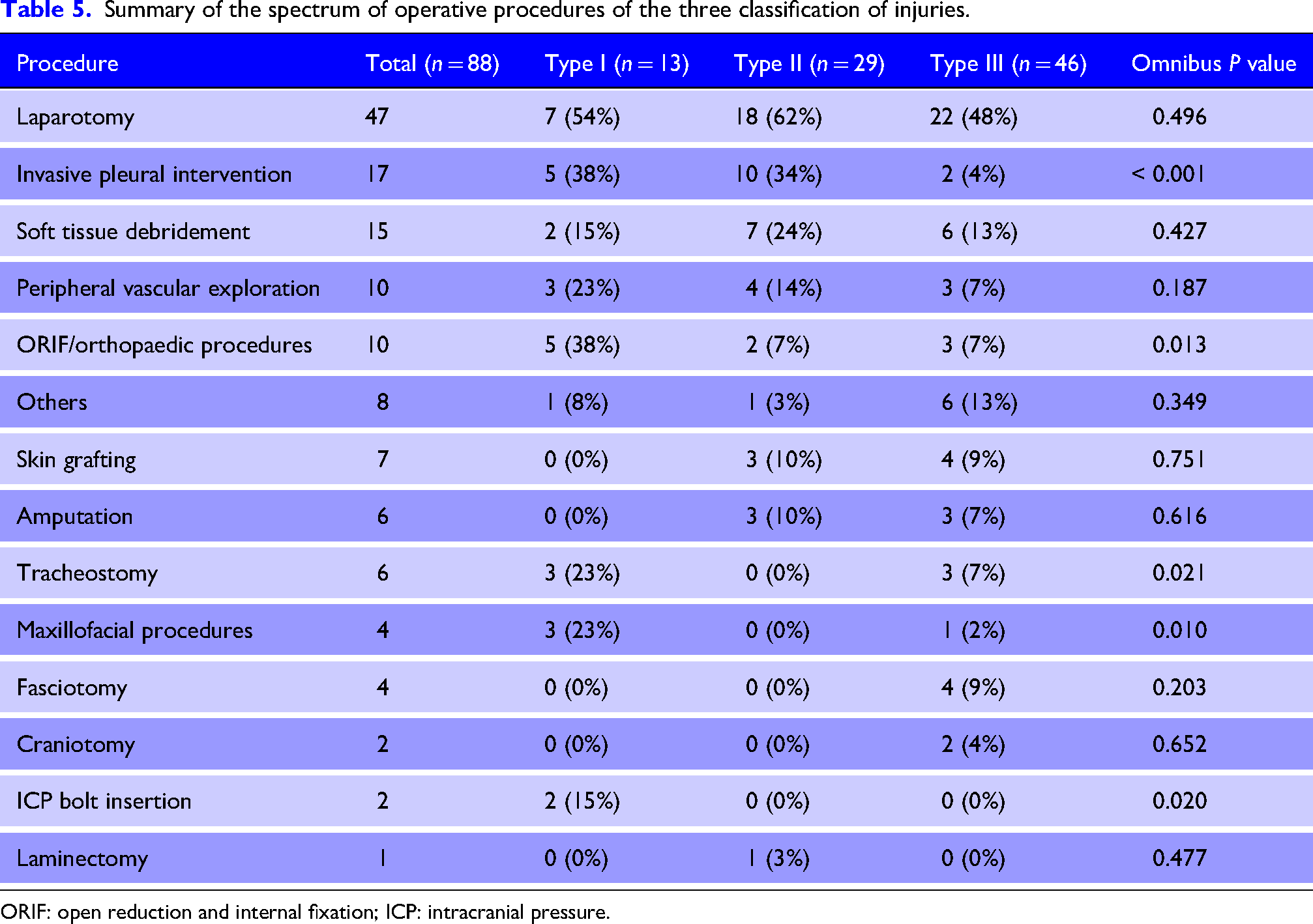
ORIF: open reduction and internal fixation; ICP: intracranial pressure.
Clinical outcome
A total of 41 patients (28%) had one or more complications. The most common complications were wound/surgical site sepsis (n = 8), retained haemothorax (n = 5), anastomotic leak/breakdown (n = 4), hospital-acquired pressure sores (n = 4), and AKIs (n = 4). Table 6 summarises the complications in all 41 patients.
Complications.
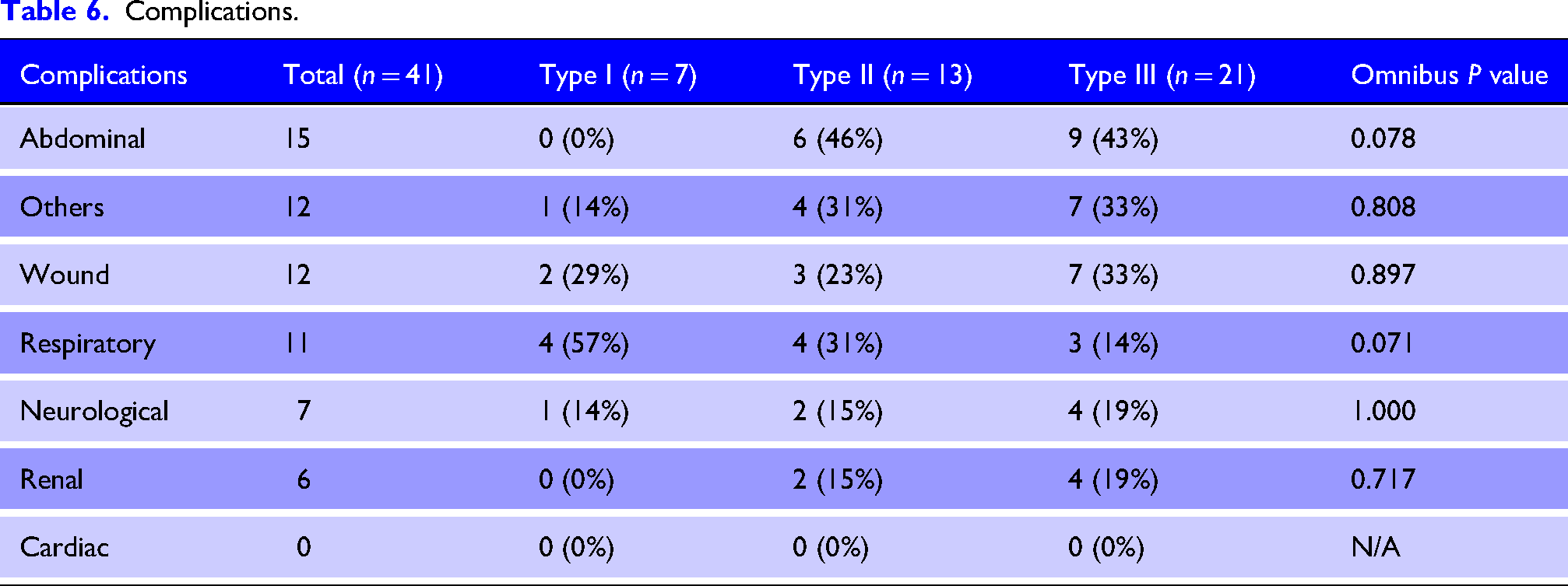
Type II injuries had the highest rate of complications (30%), followed by Type III (28%) and Type I (24%); however, this was not statistically significant (p = 0.941). There was a total of 32 (22%) patients who required intensive care unit (ICU) admissions. Of the 41 patients with complications, 20 patients (49%) required ICU admission, 12% required ventilatory support and the median length of ICU stay of 6 [3–8] days. The median total length of hospital stay was 5 [2–11] days. There was no statistical significance in any of these parameters across the three types of injuries. The overall mortality rate was 5% (8/148). All eight mortalities came from Type III patients and were statistically significant (p = 0.018). Most of the deaths (6/8) were deemed late deaths (>72 h since arrival), and all patients initially underwent an operation. One patient developed an abdominal compartment syndrome (ACS) in the ICU, which was the treating clinician's diagnosis based on haemodynamic deterioration, worsening respiratory mechanics and oliguria; and a relook laparotomy identified necrotic bowel, subsequently leading to palliation. Their primary body region injured and the cause of death are summarised in Table 7.
Summary of deaths.
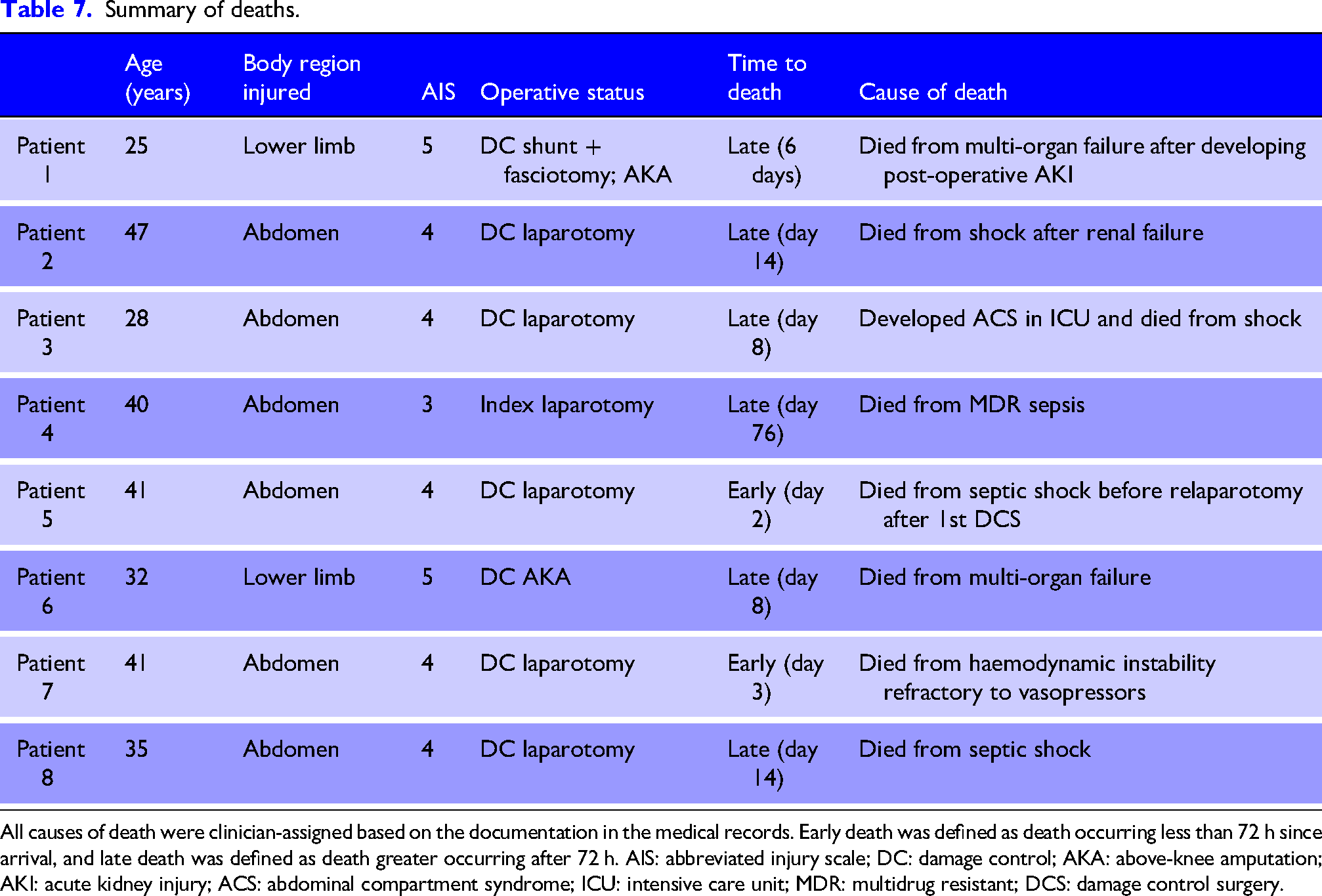
All causes of death were clinician-assigned based on the documentation in the medical records. Early death was defined as death occurring less than 72 h since arrival, and late death was defined as death greater occurring after 72 h. AIS: abbreviated injury scale; DC: damage control; AKA: above-knee amputation; AKI: acute kidney injury; ACS: abdominal compartment syndrome; ICU: intensive care unit; MDR: multidrug resistant; DCS: damage control surgery.
Discussions
SG injuries are uncommon and represent less than 2% of all gunshot wounds (GSWs). 4 SG injuries are challenging to manage due to several unique factors. The primary difference from other forms of missile injury is the dispersion of multiple pellets causing a wide spectrum of injuries. The paths of pellets vary in depth of tissue penetration and are often unpredictable. Although SGs are classified as low velocity weapon (<2500 feet/s), 7 the distance between the weapon on discharge and the victim significantly impacts the severity of injuries. 8 At close range, the entire charge can act as a single missile with kinetic energy equalling that of a high velocity projectile and can cause both penetrating injury and blast effect. At longer range, the scattering of pellets acts as multiple individual missiles striking the tissue, often with relatively lower kinetic energy per discrete projectile.9,10
This study implemented the classification system by Velmahos et al., 6 as a framework for categorising SG injury patterns and their implied relationship to discharge distance. The expectation that greater dispersion, that is, longer weapon to victim distance, would result in greater physiological insult is, on first inspection, supported by the ISS data, where Type I injuries had the greatest median ISS, followed by Type II and Type III (19 versus 10 versus 4, p < 0.001). However, this relationship was contradicted by mortality outcomes, as all eight deaths occurred among Type III patients, revealing a dissociation between ISS-derived severity and actual lethality.
This should not be interpreted as evidence that anatomically localised pellet spread is intrinsically more fatal than wider dispersion. Rather, the finding highlights an important limitation of any classification based primarily on the distribution of the pellets. Single-region injuries can occur after closer-range discharge, with pellets remaining concentrated. This may result in a greater energy transferred to an isolated anatomical region. When this localised injury involves a critical structure, such as major abdominal vasculature, visceral organs, the airway, or the central nervous system, mortality may occur despite relatively limited anatomical spread and lower overall ISS. In our descriptive review of Type III deaths, most involved abdominal or major limb injury and several were associated with substantial physiological derangement, including severe acidosis, elevated lactate, greater shock index, or prolonged length of hospitalisation. These observations suggest that pellet dispersion should be interpreted alongside physiology, range when available, and critical structure involvement, rather than in isolation.
Six of the eight deaths (75%) were late (beyond 72 h since admission), and all patients underwent operative management prior to death, confirming that none represent immediate intra-operative or non-operative mortality in patients not offered intervention. Thus, the dominant mechanism of death was therefore physiological failure following damage control surgery: sepsis/septic shock in three cases, multi-organ failure in two, ACS with bowel necrosis in one, renal failure leading to shock in one and only one dying from haemodynamic instability refractory to vasopressors.
The late, sepsis-driven mortality pattern following damage control laparotomy for SG injury is well established in previous South African series and reflects the high contamination burden of close-range SG wounds to the abdomen.3,11,12 Our study underscores a practical clinical message that late death from sepsis and multi-organ failure following damage control surgery constitutes the dominant in-hospital mortality pathway in our setting, rather than immediate haemorrhagic death.
The SG classification system proposed by Velmahos et al., has meaningful clinical utility; however, the limitations arise from where we ought to know that there are other significant factors that determine the severity of the SG injuries. Pellet dispersal patterns serve as a surrogate and a fairly accurate proxy for discharge distance and, therefore, wound energy density. Ammunition type, shot size, barrel length, and choke configuration all influence dispersal at a given range. For example, a tightly choked weapon may produce a Type III pattern at a distance where a cylinder-bore configuration would generate Type I scatter, 4 and thus two patients classified identically may have sustained wounds of substantially different ballistic severity. Furthermore, the system does not weigh for critical structure involvement. A single-region wound to the head or neck carries a fundamentally different prognosis from the extremities, and yet both are classified as Type III. Although ISS partially addresses this through the AIS scoring system, the ISS itself is also subjected to the inflation artefact, especially for Type I injuries, where high pellet counts across multiple regions drive the score independently of physiological lethality.
Our study demonstrated that a significant proportion of patients sustained injuries to more than one body region. This mandated the liberal use of cross-sectional imaging, including computed tomography angiography (CTA) as part of the diagnostic workup. This aligns with several other studies, which have shown a growing reliance on CT imaging with patients sustaining SG wounds, as it has become an integral part of the diagnostic workup.11–13 However, in this study, there was a single patient with a rectal and bladder injury overlooked on the CT scan but subsequently identified at laparotomy, which highlights the need for astute clinical assessment. Despite the clear advantages, it is important to acknowledge that CT interpretation can be complicated by interference due to radiological scatter and the presence of multiple individual projectile tracts. 4 Overall, 59% patients in this study required an operative intervention. These included laparotomy, peripheral vascular injury repair and soft tissue debridement. This is consistent with reports from other centres in North America.2,4,14,15 The management of these patients is resource-intensive, with a high rate of ICU admission, prolonged hospital stays and significant morbidity and mortality.
Limitations
There are several limitations to this study. Firstly, this is a single-centre retrospective study and reflects the injury patterns seen in our locality. There was also no data available for SG load and distance, which are important determining on the spectrum and severity of injury. Further studies in conjunction with data from other centres may provide a better understanding of the injury pattern.
Conclusion
SG injuries are associated with a wide spectrum of injuries to multiple body regions and a high requirement for operative intervention and significant morbidity and mortality. High-quality cross-sectional imaging is essential to identify and detect remote and occult injuries; however, it should complement ongoing clinical assessment in guiding management decisions.
Supplemental Material
sj-docx-1-tra-10.1177_14604086261462350 - Supplemental material for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa
Supplemental material, sj-docx-1-tra-10.1177_14604086261462350 for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa by Daniel Lee, Victor Kong, Surya Akash Boppana, Jonathan Ko, Joshua Ahn, Howard Wain, Cynthia Cheung, William Yeung, Grant Laing and Damian Clarke in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086261462350 - Supplemental material for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa
Supplemental material, sj-docx-2-tra-10.1177_14604086261462350 for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa by Daniel Lee, Victor Kong, Surya Akash Boppana, Jonathan Ko, Joshua Ahn, Howard Wain, Cynthia Cheung, William Yeung, Grant Laing and Damian Clarke in Trauma
Supplemental Material
sj-docx-3-tra-10.1177_14604086261462350 - Supplemental material for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa
Supplemental material, sj-docx-3-tra-10.1177_14604086261462350 for Shotgun injuries – Analysis of 148 patients managed at a major trauma centre in South Africa by Daniel Lee, Victor Kong, Surya Akash Boppana, Jonathan Ko, Joshua Ahn, Howard Wain, Cynthia Cheung, William Yeung, Grant Laing and Damian Clarke in Trauma
Footnotes
ORCID iDs
Ethical considerations
Ethics approval for the maintenance of this registry for both clinical care and research has been formally endorsed by the Biomedical Research Ethics Committee (BREC) of the University of KwaZulu Natal (UKZN) and is in accordance with the 1964 Helsinki Declaration and its later amendments. The original number was BCA 207/09 and subsequently BCA 221/13. Where applicable, formal consent from patients for the use of clinical photographs pertaining to this study was obtained.
Author contributions
DL, VK and DC were involved in manuscript writing. DL, JK and SAB were involved in data extraction and statistical analysis. All authors (DL, VK, SAB, JK, JA, HW, CC, WY, GL and DC) were involved in manuscript revision and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.