
Abstract
Background
Grade IIIB open tibial fractures are a severe form of open fractures usually accompanied by soft tissue loss and bone loss, which can be challenging to manage, and are associated with increased risk of complications, especially fracture-related infection. Popular management strategies include the induced membrane technique (Masquelet) and the distraction histogenesis technique by Ilizarov. These strategies are not, however, without their own challenges. Hence, a simple and inexpensive method of managing the bone loss usually found to accompany these fractures would revolutionize trauma care.
Case report
A 54-year-old patient presented with Gustilo-Anderson type IIIB open fracture of the left leg with approximately 14 cm bone loss. He was managed by fixing the fracture with an antibiotic cement-coated plate and by the use of a polymethylmethacrylate (PMMA) spacer to fill the bone defect with a plan for a second-stage Masquelet technique. The bone spacer was not removed due to delays in accessing theatre space, and subsequent clinical and radiological images showed evidence of fracture union without features of fracture-related infection.
Conclusion
This case report highlights the possibility of using PMMA as a bone substitute and also for preventing fracture-related infection in severe open fractures.
Introduction
Grade IIIB open tibial fractures, according to Gustilo and Anderson classification, 1 are a severe form of open fractures accompanied by soft tissue loss and bone loss. These types of fractures are associated with increased risk of complications, especially fracture-related infection (FRI). 2 Management strategies for the successful management of these fractures must deal with the bone gap and soft tissue reconstruction.
Several surgical techniques have gained attention in the management of these fractures, each with its own advantages and disadvantages.3,4 Prominent among these techniques are the induced membrane technique (Masquelet) and the distraction histogenesis technique by Ilizarov. The induced membrane technique is a two-stage procedure where a bone cement spacer is inserted into the area of the bone defect to allow formation of a membrane, which is later incised and filled with bone graft in the second stage, usually 4–6 weeks after the first stage. The technique has been used for the successful management of bone loss in open fractures. 5 The Ilizarov technique, on the other hand, is more versatile and dynamic. It can be used to manage bone loss either through acute shortening and bone lengthening through a proximal osteotomy or through bone transport; either version of the Ilizarov technique utilises a circular external fixator mounted on the patient's limb.6,7
Each of these techniques is associated with specific complications, apart from being expensive. Complications commonly associated with the Masquelet technique include FRI, nonunion and fatigue failure of the fixation system. 8 Pin-tract infection is a major complication of the Ilizarov technique, with others including peroneal nerve palsy, joint stiffness and limb oedema. 6
When grade IIIB fractures were initially identified by Gustilo et al., 2 they were prone to amputation due to their high susceptibility to infection. With advances in soft tissue reconstruction and bone lengthening procedures, many of these fractures are now salvageable, though the literature is replete with debate on which of the procedures offers the patient a better outcome. 9 Given the choice, however, most patients prefer limb salvage over amputation. 9 This underscores the constant attempt by trauma surgeons to continuously refine the limb salvage techniques and approaches.
Polymethylmethacrylate (PMMA) is a known and versatile biomaterial in orthopaedic practice. Some of its widely known applications include use in the cementation process of joint replacement surgeries, as a spacer and void filler in trauma surgeries, and as a carrier for local delivery of antibiotics in the treatment of orthopaedic infections. 10 This report describes the rare and incidental use of PMMA as a bone substitute in the management of critical bone loss. The report follows the CARE guidelines. 11
Case report
A 54-year-old male farmer presented to our facility unable to weight-bear on the left lower limb following a motorbike road traffic accident. He was in severe pain and distress. He had no loss of consciousness and had sustained no injuries to other parts of the body. He did not smoke or drink alcohol.
At presentation, he had a complete avulsion wound measuring 8 cm × 10 cm on the proximal third of the left leg with multiple exposed bone fragments. He was pale with a PCV of 19%, but all distal pulses were palpable. He had full resuscitation following the Advance Trauma Life Support protocol. Figure 1 shows the clinical and radiological images of the injury at presentation.

Clinical and radiographic appearances of the left leg injury at presentation. There was severe comminution.
Initial surgery
At surgery and during his first stage of the Masquelet technique, he had extensive wound debridement and copious irrigation, with removal of loose bony fragments. His fracture was bridged with a proximal left tibia anatomic plate coated with antibiotic bone-cement mixture; details of how the antibiotic cement-coated implant was prepared are detailed elsewhere. 12 Following debridement of the left tibia comminuted fractures, the 14 cm of bone defect was filled with a PMMA spacer, moulded to a bone shape. A standard ORIF protocol was followed for the fixation of the antibiotic cement-coated plate. The immediate post-operative radiograph is shown in Figure 2. Soft tissue coverage was achieved by reconstruction with a left medial hemisoleus flap, a left medial gastrocnemius flap and a superficial thickness skin graft.

The immediate post-operative radiographs after initial surgery/Stage 1 Masquelet procedure. The polymethylmethacrylate (PMMA) spacer is arrowed.
Clinical course
Post-operatively, the patient was placed on intravenous ceftriaxone, sulbactam, analgesics and anticoagulants. On post-operative day 5, he became febrile and had visible exudates from the area of the soft tissue reconstruction consistent with soft tissue infection. He subsequently had bedside debridement and a wound biopsy taken and sent for culture and sensitivity. He continued his antibiotic regimen pending those results and was also commenced on daily wound dressings.
Wound cultures grew Pseudomonas aeruginosa and Klebsiella pneumoniea, both sensitive to amikacin, which he then started. By Day 6 of intravenous antibiotics, the infection had cleared, but he completed a 14-day course intravenously followed by oral clindamycin and rifampicin. Review of the wound showed that the margin of the flap had widened slightly, exposing part of the antibiotic cement-coated plate. The decision of the managing team at this point was to retain the implant as: (1) the plate was not exposed due to the antibiotic cement coating which served as a protective layer (2) the bone was not exposed because of the cover offered by the antibiotic cement-coated plate (3) the initial exudate had stopped, except for tissue fluids oozing from the edge of the flap and (4) there was no evidence of bone or soft tissue infection.
He was counselled for the second stage of the Masquelet procedure at a later date and was subsequently discharged home on daily wound dressings, with follow-up at the surgical outpatient clinic. The clinic follow-ups were uneventful, but it was difficult getting a theatre space for him due to a long waiting list. His follow-ups radiographs, however, showed progressive callus formation and an improving clinical status, and he could not have access to theatre space until 6 months after the first surgery. At this time point, there was exuberant callus formation and progression of fracture healing (Figure 3(a)), and the original decision to do a second-stage Masquelet was abandoned, and the antibiotic cement-coated plate was removed instead, with the limb supported in a full leg cast. At the 9-month follow-up, there was radiographic evidence of a bridging callus, and the initial bone cement spacer was no longer visible (Figure 3(b)). The full leg cast was later removed, and the patient was commenced on aggressive rehabilitation. At 15 months post-injury, he had some joint stiffness and continues rehabilitation but he is able to carry out his daily activities with little support.
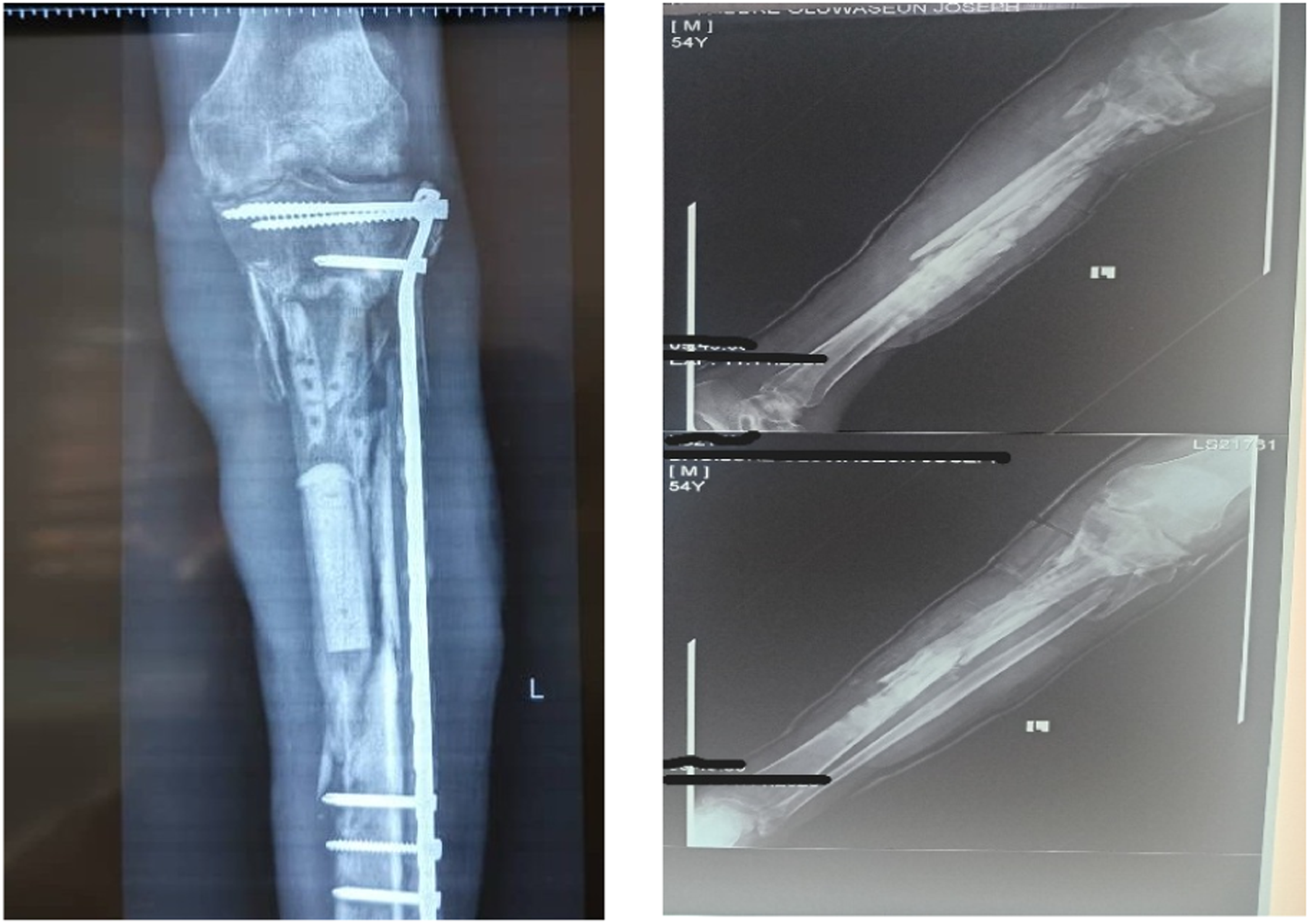
Follow-up radiographs (a) showing the exuberant callus formation at 6 months and (b) showing the bridging callus at 9 months with the polymethylmethacrylate (PMMA) spacer no longer visible.
Discussion
This case report highlights the possibility of using PMMA as a bone substitute and also for preventing FRI in severe open fractures.
PMMA has proven effective in managing bone loss and infection in joint replacement surgeries. 13 Because of its unique characteristics such as near-bone mechanical properties, short curing time, mechanical interlocking and affordability, it is a suitable material for void fillers in comminuted fracture. 10 There is no previous report of using PMMA as a bone substitute to manage a critical bone defect in severe open fractures, and this case report may be the first, albeit as an incidental finding.
Furthermore, the documented successes achieved in using antibiotic cement-coated implant to manage infected nonunion were extended to prevent FRI in severe open fractures. 14 Apart from preventing FRI in this case, the antibiotic cement-coated implant also protected the underlying bone from desiccation and necrosis when the marginal flap necrosis progressed. This case highlights another incidental discovery of a potential use of PMMA in the protection of exposed bone.
Another important focus of this case report is the single-stage nature of the procedure. There are only a few documentations of single-stage reconstruction of soft tissue and bone defects not involving the distraction osteogenesis technique.10,15 These procedures are, however, complex, time-consuming and expensive. They may not be feasible in low-resource settings where the appropriate facilities and technical knowledge may not be available.
While the technique discussed in this index case is simple, cheap and effective, it is important to highlight some measures that might increase the chances of success: the antibiotic cement coating on the implant should be as thin as possible to prevent the whole construct from occupying too much space in the limb. This may affect wound closure or wound healing. The technique to achieve this is described elsewhere. 12 The PMMA was moulded to simulate a bone structure but the contributory effect of this method requires further investigation.
Conclusion
This case report highlights the versatility of PMMA in the management of a complex open tibial fracture. It shows the possibility of PMMA being used as a bone substitute, beyond its current use as a temporary void filler or spacer. The study also confirms that an antibiotic cement-coated plate can be safely used to prevent FRI in severe open fractures.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
The consent form signed by the patient is part of the document submitted