
Abstract
Introduction
Electronic Health Record Systems (EHRS) are transforming healthcare delivery globally, yet their implementation in resource-constrained settings like Ghana remains underexplored. This study evaluated EHRS adoption in private hospitals in Ghana’s Suame Municipality, assessing structural readiness, process integration, and outcomes to identify barriers and enablers of successful digital transition.
Methods
A qualitative study design was employed, involving semi-structured interviews with 28 purposively selected healthcare workers (clinicians, administrators, IT staff) across four private hospitals. Data were analyzed using Braun and Clarke’s thematic analysis to identify patterns in infrastructure, workflow adaptations, and perceived impacts. Theoretical saturation guided sample adequacy.
Results
Three key themes emerged: (1) Structural challenges, including uneven IT infrastructure distribution, staffing gaps (e.g., reliance on single IT personnel), and inadequate training; (2) Process improvements, such as streamlined documentation and claims processing, despite intermittent system failures reverting to paper-based backups; and (3) Mixed outcomes, with reported efficiency gains (e.g., error reduction) offset by policy voids and financial constraints limiting scalability.
Conclusion
While EHRS implementation in Ghana’s private sector shows promise in improving workflows, its sustainability is threatened by infrastructural deficits, workforce capacity gaps, and unclear governance. The study recommends public-private partnerships for financing and hybrid paper-digital systems to mitigate disruptions.
Introduction
The adoption of Electronic Health Record Systems (EHRS) has emerged as a cornerstone of modern healthcare transformation, offering a digital platform that integrates comprehensive patient medical histories to support clinical decision-making, reduce medical errors, and improve care coordination across health providers. 11,2 Unlike traditional paper-based records, which were plagued by inefficiency, illegibility, and fragmentation, EHRS enables real-time access to patient information, facilitates interoperability between health facilities, and supports data-driven approaches to both individual care and population health management. 33,4 Recognizing these benefits, many high-income countries have institutionalized the adoption of EHRS through deliberate policy action, including the United States’ Health Information Technology for Economic and Clinical Health (HITECH) Act and comparable strategies in Australia, the United Kingdom, and New Zealand, which have achieved adoption rates exceeding 90% in primary care settings. 55,6 In contrast, Sub-Saharan Africa continues to lag significantly behind, constrained by inadequate infrastructure, limited standardization, and inconsistent implementation support. 77,8 Ghana’s experience is particularly instructive: despite the Ministry of Health’s National e-Health Strategy launched in 2010 and sustained government investment in digital health infrastructure, EHRS adoption remains uneven across facility types, with private health facilities representing a notably under-examined and underserved segment of the health system. 99–11 Understanding the specific barriers and facilitators of EHRS implementation in these settings is therefore not merely an academic exercise, but a policy-relevant imperative for strengthening Ghana’s mixed health system.
The potential of EHRS to enhance healthcare quality is well-documented in the literature. Beyond basic record-keeping, EHRS enables clinicians to analyze longitudinal patient data, identify clinical trends, and make evidence-based decisions that reduce diagnostic errors and optimize treatment plans. 44 By consolidating fragmented patient information into a unified, interoperable database, EHRS supports access to comprehensive medical histories, drug interaction alerts, and best-practice clinical guidelines at the point of care. 1 12 At the population level, aggregated EHRS data have proven invaluable for epidemiological surveillance, enabling researchers and policymakers to identify disease patterns, evaluate treatment efficacy, and design targeted health interventions. 1 13 Taken together, these capabilities position EHRS not only as an administrative tool but as a critical infrastructure for evidence-based medicine and health system performance. The effectiveness of EHRS, however, is contingent on its ability to ensure timely access to patient information, enhance communication among providers, and sustain continuity of care across the health system. 22,14
Evidence from high-income countries further illustrates the tangible impact of EHRS on health service delivery. Studies across the United States, Australia, and Europe consistently report reductions in patient waiting times, improvements in record accuracy, and more seamless information exchange during patient referrals. 115,16 In these contexts, EHRS has been embedded within broader national digital health strategies supported by sustained government funding, clear regulatory frameworks, and robust technical infrastructure, conditions that have enabled widespread adoption and meaningful system-level benefits. 55,6 These experiences offer important lessons for low- and middle-income countries seeking to leverage digital health tools to strengthen their health systems, though they also underscore the extent to which successful EHRS implementation is shaped by context-specific factors that cannot be straightforwardly transferred across settings.
In Sub-Saharan Africa, EHRS adoption has progressed slowly and unevenly, with implementation challenges documented across multiple countries. 77,17 Key barriers include inadequate digital infrastructure, shortages of trained health informatics personnel, insufficient funding, lack of interoperability standards, and poor data governance frameworks. 88,17 These structural constraints have limited the ability of health systems in the region to translate the promise of EHRS into measurable improvements in care quality and efficiency. Ghana is no exception. Although the Ministry of Health’s 2010 National e-Health Strategy signaled a strong institutional commitment to integrating information and communication technology into healthcare, including the promotion of EHRS across health facilities, progress in actual implementation has remained inconsistent. 99 The strategy’s objectives, to enhance health information management, improve service delivery, and expand equitable access to care, have yet to be fully realized, particularly in non-public health facilities.
Despite growing interest in digital health in Ghana, the existing literature has disproportionately focused on public sector institutions, leaving private health facilities, a significant and expanding component of the national health system, largely underexplored. 118,19 This is a critical gap. Private facilities operate under distinct organizational conditions, including different regulatory obligations, resource constraints, and financial incentive structures, all of which are likely to shape EHRS adoption in ways that differ meaningfully from the public sector experience. 110,11 Moreover, most existing research on EHRS implementation in Sub-Saharan Africa has tended toward broad, national-level analyses, offering limited insight into the facility-level dynamics that ultimately determine whether digital health tools are successfully integrated into routine clinical practice. 88,17 Subnational, context-specific evidence is therefore urgently needed to complement system-level perspectives and to inform practical implementation strategies.
This study addresses these gaps by examining EHRS implementation in private hospitals within the Suame Municipality of the Ashanti Region of Ghana. By focusing on a specific facility type and geographic context, the study generates granular, context-sensitive evidence on the barriers and facilitators of EHRS adoption in an under-researched segment of Ghana’s health system. The findings are intended to contribute to the growing body of literature calling for more disaggregated analyses of digital health adoption in low- and middle-income countries, and to inform targeted policy interventions aimed at improving EHRS uptake across Ghana’s mixed public-private health system.
Methods
Study design and setting
This study employed a qualitative, cross-sectional, interpretive research design to explore the implementation and effects of EHRS in private healthcare settings. An interpretive methodology was adopted to facilitate a comprehensive understanding of the sociotechnical and organizational dynamics that influence EHRS adoption, use, and impact. The research was conducted in Suame Municipality, located in the Ashanti Region of Ghana. This municipality was deliberately selected as the study site because, at the time of data collection, it had no government hospitals, leaving private health facilities as the primary providers of healthcare services.
Participants and eligibility criteria
Participants in the study were healthcare professionals occupying leadership or supervisory positions across four purposively selected private hospitals. Eligible participants were 18 years or older, employed at any of the four facilities, and directly involved in or knowledgeable about EHRS implementation. Specifically, the study targeted individuals in roles such as medical directors, nurse managers, pharmacists, diagnostic and laboratory heads, human resource administrators, IT leads, and financial managers. Individuals were excluded if they were in non-leadership positions, employed temporarily, worked in facilities outside the study scope, or declined to provide informed consent.
Sampling strategy
A purposive sampling approach was used to ensure that participants selected could provide rich, relevant, and diverse insights into the implementation of EHRS. This strategy was considered most appropriate given the study’s interpretive orientation and the need to recruit information-rich cases capable of speaking meaningfully to the experiences, challenges, and facilitators associated with EHRS across different functional roles and facility contexts.
Participants were recruited across four private hospitals to ensure diversity in facility size, ownership model, and stage of EHRS implementation, thereby maximizing the range of perspectives captured. Within each facility, the first and second authors identified potential participants through initial contact with medical directors, who facilitated introductions to other eligible staff. Recruitment proceeded iteratively alongside data collection, consistent with the logic of qualitative inquiry.
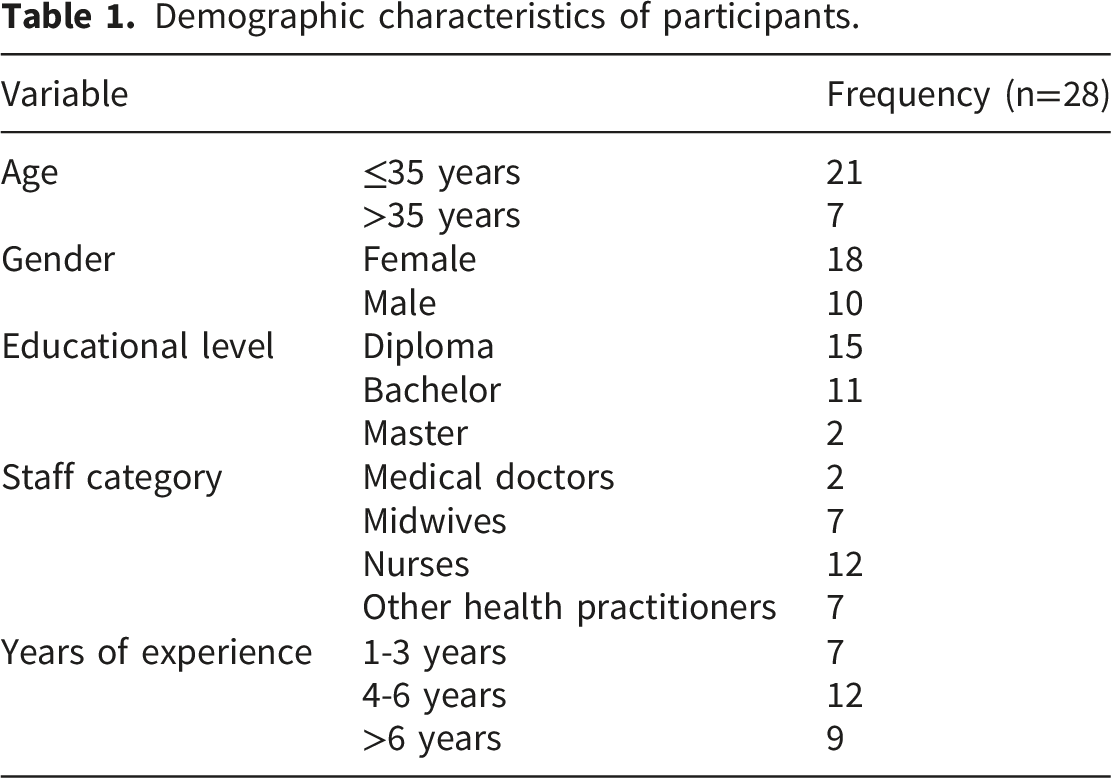
Sampling continued until theoretical saturation was reached, the point at which no new themes, concepts, or insights emerged from successive interviews. Saturation was assessed through an ongoing, iterative process during which the research team reviewed emerging codes and themes after each interview, discussed whether new information was being generated, and made a collective determination to cease recruitment when successive interviews consistently confirmed existing themes without introducing new analytical dimensions. A total of 28 participants were interviewed across the four facilities. This sample size was considered sufficient to achieve saturation and generate meaningful, transferable patterns in the data, consistent with recommendations for purposive qualitative samples of this scope.
Data collection
Data collection was conducted through semi-structured, in-depth interviews using a standardized, pre-tested interview guide developed through a systematic process. The guide was initially constructed by the research team through a review of relevant literature. Draft questions were mapped against the study’s three thematic dimensions, structural factors (including system design and infrastructure), process elements (such as workflow integration and user adaptation), and outcome measures (including changes in care quality and administrative efficiency), to ensure comprehensive coverage of the research objectives. The guide comprised open-ended questions and follow-up probes designed to elicit detailed, experience-based responses. For example, participants were asked to describe their facility’s journey toward EHRS adoption, reflect on challenges encountered during implementation, and assess perceived changes in care delivery since adoption. Pre-testing was conducted through trial interviews with four individuals similar to the study participants but not included in the study. Feedback from pre-testing informed revisions to question clarity, sequencing, and probing depth, after which the guide was finalized.
Interviews were conducted face-to-face in English by the first and second authors at the participating hospital premises between November 2023 and March 2024. Each interview lasted approximately 30 to 40 minutes and was audio-recorded with the participant’s consent to ensure accurate data capture. Conducting interviews within the hospital environment supported contextual relevance, minimized participant inconvenience, and facilitated incidental observation of the physical and operational setting. The entire study was conducted over 12 months. Before the start of the data collection, formal introductions of the researchers were done by the management of the various health facilities to their staff.
Data processing and analysis
The recorded interviews were transcribed verbatim by the first author and cross-checked against audio recordings and field notes by the second author to ensure transcription accuracy. Transcripts were then imported into NVivo version 14 for systematic management and analysis.
Thematic analysis was conducted following Braun and Clarke’s six-step framework, comprising familiarization with the data, generation of initial codes, construction of preliminary themes, review and refinement of themes, definition and naming of final themes, and production of the analytical report. 2 20 Both deductive and inductive analytic strategies were employed concurrently. The deductive strand was guided by the study’s conceptual framework, focusing analysis on structure, process, and outcome dimensions to ensure systematic coverage of the research objectives. The inductive strand allowed additional themes grounded in participants’ own framings and experiences to emerge organically from the data, enriching the analytical depth beyond the a priori framework.
Code development followed a structured iterative process. During the initial familiarization phase, the first and second authors each read all transcripts independently and generated preliminary descriptive codes grounded in the raw data. These initial codes were discussed collectively and organized into a provisional codebook, with each code assigned a clear definition, inclusion criteria, and an illustrative data excerpt. The codebook was refined iteratively as coding progressed, with new codes added inductively and existing codes revised where the data demanded greater conceptual precision. To strengthen inter-coder reliability, both authors independently coded a randomly selected subset of 30% of transcripts using the agreed codebook. Coded outputs were then systematically compared using a code comparison query in NVivo, and percentage agreement was calculated. Discrepancies were resolved through structured deliberation, during which each coder explained their interpretive reasoning, and consensus was reached collaboratively. Where interpretive disagreements persisted after discussion, a third author was consulted to adjudicate, ensuring that analytical decisions were not driven by individual perspective alone. This iterative co-coding process enhanced the consistency and dependability of the final coding framework.
Trustworthiness, reflexivity, and positionality
Several strategies were employed to enhance the trustworthiness and rigor of the study, alongside ongoing critical reflection on how researcher positionality may have shaped the research process. Credibility was supported through researcher triangulation, whereby the first and second authors, both health systems researchers with professional familiarity with digital health implementation in Ghanaian healthcare settings, independently coded transcripts and reconciled interpretations through structured discussion. While this insider knowledge facilitated rapport with participants and informed the depth of probing during interviews, the team remained alert to the risk of confirmatory interpretation. To mitigate this, reflexive memos were maintained throughout data collection and analysis, documenting emerging assumptions and interpretive decisions at key analytical junctures to ensure findings remained grounded in participant accounts rather than researcher preconceptions.
Member checking was conducted with a purposively selected subset of eight participants, representing diversity in facility type and professional role. Preliminary findings were shared via email and follow-up telephone calls, and participant feedback was used to verify the accuracy, completeness, and resonance of interpretations. Where participants identified nuances not adequately captured in the initial analysis, these were incorporated into the final thematic structure, ensuring that participant voices were authentically represented.
Transferability was facilitated through thick description of the study context, participant characteristics, and analytical process, enabling readers to assess the applicability of findings to comparable settings. Dependability and confirmability were supported through a comprehensive audit trail documenting the sampling rationale, iterative coding decisions, theme development discussions, and revisions made in response to member checking. This audit trail was maintained in a shared, secure folder accessible to all authors, providing a transparent account of methodological and analytical choices throughout the research process. Collectively, these strategies reflect a commitment to methodological integrity consistent with established standards for trustworthiness in qualitative health research.
Results
Demographic characteristics of participants.
The findings reveal a complex landscape of progress and persistent challenges, characterized by uneven infrastructure deployment, varying user experiences, and systemic barriers to full adoption. While hospitals demonstrated commitment to digital transition through vendor selection and initial training, critical gaps in resources, policy frameworks, and technical support emerged as limiting factors. The results are organized into three thematic areas: (1) structural implementation, examining IT infrastructure and staffing; (2) process adoption, assessing usability and workflow changes; and (3) outcomes, analyzing benefits and unresolved challenges. Together, these findings provide a nuanced understanding of EHRS integration in resource-constrained settings, highlighting both the transformative potential and the need for targeted interventions to achieve sustainable digital health transformation.
Theme 1: Structural implementation of EHR
•
The study revealed uneven IT infrastructure preparedness across all four hospitals, with hardware distribution favoring administrative units over frontline clinical areas, particularly inpatient wards. A Medical Superintendent shared this: “The EHR covers computers to be dispatched to the wards and other user departments, though they were inadequate, but mechanisms were put in place to acquire more computers and other sophisticated equipment.” (Medical Superintendent) •
Human resource constraints, particularly inadequate IT staffing, emerged as the most consistently reported barrier across all four facilities, creating structural fragility that affected every dimension of EHRS functionality, from routine troubleshooting to system maintenance, reflecting a sector-wide limitation rather than isolated institutional failure. An Administrator illustrated the severity of this gap: “The EHR system administrators include only one IT personnel and an intern who are tasked to oversee the full functionality of the system daily.” (Administrator) •
System instability and EHRS downtime forced facilities to periodically revert to paper-based documentation, introducing risks of data fragmentation, transcription errors, and discontinuity in patient records. An IT professional’s account revealed this: “Everything is electronic, but when we encounter any problem, we resort to the old system, that is, the paper-based work, and revisit the EHR system when the problems are resolved.” (IT Personnel) •
Inadequate training represented a structurally embedded implementation weakness, disproportionately affecting frontline clinical staff. A notable disconnect existed between management’s perception of training sufficiency and the lived experiences of day-to-day system users. A Midwife-In-Charge articulated this: “We had some level of training, but it was woefully inadequate.” (Midwife-In-Charge) •
Despite significant resource constraints, facilities demonstrated methodical vendor selection approaches, reflecting strategic deliberation at the procurement stage. However, this creates an analytical tension between the diligence applied during procurement and the inadequate resourcing that characterized subsequent implementation. A Medical Superintendent shared this: “The management finally settled on the HAMS solutions from InfoTech after considering other vendors of similar functionalities and capabilities.” (Medical Superintendent)
Theme 2: Process implementation of EHRS
•
EHRS deployment had reached most departments across all four facilities, representing meaningful digitalization progress. However, adoption breadth did not uniformly translate into functional proficiency, with clinical staff reporting more positive usability experiences while administrative and financial personnel expressed greater frustration with complex data entry and claims processing functions. A Medical Superintendent shared this: “The EHR is easy to use due to the simplified design features and their readiness to learn new things.” (Medical Superintendent)
Consistent with existing evidence, EHRS usability varied across professional roles, reflecting the fit between system design and specific workflow demands, rather than being a uniform system property, signaling the need for role-sensitive interface design considerations. An account officer shared this statement: “The problems encountered during use are numerous, so I’m not overly satisfied.” (Account Officer) •
EHRS adoption consistently and positively transformed documentation workflows across all facilities and professional roles, with participants reporting meaningful reductions in administrative burden, a convergence that strengthens confidence in this as a genuine implementation outcome rather than individual experience. A Nurse’s testimony captured the nature of this transformation: “The system has really streamlined workflow, and the tedious documentation work has vastly reduced.” (Nurse)
Beyond convenience, reduced documentation burden carries broader implications for care quality and staff wellbeing, as time previously spent on administrative tasks becomes available for direct patient care. This efficiency gain was most pronounced in the claims processing domain. A Claims Officer described a particularly concrete manifestation: “We used to spend a lot of time in claims preparation and processing before final vetting, batch them into groups for onward submission to NHIS, but through the software, there’s automatic generation of claims, and our workload has greatly reduced.” (Claim Officer) •
While workflow improvements were widely acknowledged, persistent competency gaps stemming from inadequate training constrained EHRS benefits, bridging structural and process themes. A midwife articulated this limitation: “My problem is the inadequacy of training received, hence difficulty with the learning process.” (Midwife)
Another Nurse added “The training wasn’t adequate to conceptualize everything about the system.” (Nurse) •
User satisfaction was positive but role-differentiated, with clinical staff, particularly those who experienced direct reductions in documentation burden, reporting the highest levels of satisfaction. A Nurse’s reflection captured the practical basis for this appreciation: “For me, I am satisfied because there is less documentation, unlike using folders.” (Nurse)
However, satisfaction was tempered in cases where implementation had proceeded without adequate prior assessment of staff readiness. A Midwife’s critical observation introduced an important institutional accountability dimension: “Management rushed into things without assessment of staff competencies and IT skills.” (Midwife)
Theme 3: Outcomes of EHR Implementation
•
EHRS satisfaction was positive across all four facilities, though its nature and depth varied meaningfully by role, competency level, and degree of workflow integration, revealing a nuanced satisfaction landscape rather than uniform enthusiasm. A Medical Officer’s measured assessment captured a widely shared, qualified form of approval: “The implemented EHR system supports our work to some extent.” (Medical Officer)
Among clinical personnel, satisfaction was further nuanced by the recognition that engagement with the system remained an ongoing learning process rather than a completed transition. A Midwife’s reflection exemplified this adaptive orientation: “I am satisfied but still taking my time to learn everything about the system.” (Midwife) •
Despite documented structural and process challenges, participants across all facilities reported substantive operational and clinical benefits from EHRS adoption, spanning record access, inter-professional communication, medication safety, and administrative efficiency, suggesting meaningful value even amid incomplete implementation. A Medical Officer shared: “The electronic health records help make immediate access to patients’ records.” (Medical Officer)
In Ghana’s private healthcare context, where paper-based systems are prone to fragmented filing and retrieval delays, EHRS-enabled immediate access to complete patient records supports informed clinical judgement, reduces diagnostic duplication, and facilitates safer care, particularly in time-critical emergency presentations. A Nurse shared this: “It facilitates the sharing of information among healthcare providers and has improved the image of nurses.” (Nurse) • St
Beyond record accessibility, participants valued EHRS-enabled automated medication safety checks as a significant clinical outcome, representing a qualitative shift from reliance on individual vigilance, susceptible to fatigue and distraction, toward systematic algorithmic verification. A Nurse articulated this benefit directly: “The system automatically checks for medication errors, drug interactions, and allergies.” (Nurse)
This finding is analytically significant in the context of private healthcare facilities that may operate with lean clinical staffing and high patient throughput. In such environments, automated safety features serve as a critical compensatory mechanism, catching errors that human oversight might miss under conditions of workload pressure. A Midwife highlighted this: “The new software has reduced errors associated with prescribers’ handwriting and ensures continuity of care.” (Midwife) •
Notwithstanding these gains, participants identified significant barriers that constrained the full realization of EHRS’s potential and threatened the sustainability of adoption. The most structurally consequential of these was the absence of formal policy frameworks governing EHRS use, a gap that created ambiguity about standards, accountability, and data governance. A Midwife’s account captured this: “We don’t know any policy backing the use of the new system.” (Midwife)
The absence of perceived policy backing reflects a genuine governance deficit in Ghana's private health sector, where no sector-specific EHRS regulatory framework existed, resulting in inconsistent facility-level decisions on system standards, interoperability, and data protocols. Financial constraints further compounded these governance limitations, restricting necessary infrastructure investments. “Finance is a challenge; if we had money, we could have better IT infrastructure.” (Medical Officer) •
Workforce limitations and system vulnerabilities continued to manifest as outcome-level constraints, reinforcing findings from the structural theme and demonstrating that unresolved structural deficits translate directly into operational impairments. An IT specialist shared: “Lack of skilled personnel in computer literacy made data entry problematic.” (IT Personnel)
EHRS implementation represents not merely a technology challenge but a workforce development challenge, as data entry errors stemming from low digital literacy compromise record integrity, undermining the accuracy that distinguishes EHRS from paper systems, with infrastructure instability further compounding these human resource limitations. A Nurse shared: “Sometimes, the system is brought to a temporary halt due to switch failures.” (Nurse)
Discussion
The implementation of EHRS in private hospitals in Ghana’s Suame Municipality reveals a mixed landscape of progress and persistent challenges, consistent with broader trends in low- and middle-income countries (LMICs). Findings are interpreted through sociotechnical systems theory, which posits that successful EHRS implementation requires simultaneous alignment of technical infrastructure, organizational processes, and human factors. 2 21 This framing explains why technically functional deployments produced uneven outcomes, reflecting sociotechnical misalignment rather than technology failure per se, and supports calls for implementation frameworks that treat workforce capacity, governance, and contextual fit as coequal determinants of digital health success. 2 22
Infrastructure disparities, particularly the systematic underservicing of frontline clinical areas relative to administrative units, represent a distinctive finding that extends existing LMIC evidence. While studies from Nigeria and Kenya have documented infrastructure deficits primarily at the network connectivity level, this study identifies departmental-level inequity as a more granular and clinically consequential barrier, as gaps in clinical areas directly compromise care quality in ways that administrative inefficiencies do not. 223–25 Similarly, infrastructure planning in Sub-Saharan African health systems has been found to prioritize administrative over clinical functions, 88 a pattern this study confirms in Ghana’s private sector. These findings underscore the need for infrastructure planning frameworks that center on clinical workflow requirements from the outset of EHRS deployment.
The reliance on a single IT staff member to manage full EHRS functionality mirrors challenges documented in South Africa and Uganda, where understaffed IT departments drove system maintenance failures and sustainability risks. 226,27 Human resource constraints have been identified to be among the most structurally consequential yet underestimated barriers to sustainable EHRS implementation in Sub-Saharan Africa, 228,29 a conclusion strongly corroborated here. It has further been reported that IT understaffing creates a compounding effect, eroding staff confidence in EHRS and accelerating reversion to paper-based workflows. 1 17 Addressing this requires sector-wide health informatics workforce development strategies that treat IT staffing as a core component of digital health infrastructure.
System downtime and reversion to paper-based documentation have been widely documented in LMIC health systems experiencing power instability and connectivity disruptions. 330,31 This study extends existing evidence by documenting the specific clinical risks of workflow reversals in high-volume private facilities, including data fragmentation, transcription errors, and medication record discontinuity, risks amplified where administrative throughput is a commercial imperative. These findings align with calls for context-adaptive EHRS designs that incorporate structured downtime protocols as standard deployment components rather than reactive afterthoughts. 3 31
Training inadequacy, particularly the disconnect between management perceptions of sufficiency and frontline staff experiences of preparedness, mirrors findings from Tanzania, where insufficient training duration and absent post-deployment support limited EHRS utilization. 332,33 Training adequacy has been argued to be evaluated from end users’ perspectives rather than program managers’, as managerial assessments systematically overestimate initial training while underestimating the need for continuous, role-sensitive capacity building. 2 22 This organizational disconnect may reflect power dynamics within private healthcare organizations that shape how implementation challenges are acknowledged. Rwanda’s experience offers a compelling alternative, demonstrating that phased, mentorship-supported training significantly improves user proficiency and system acceptance, suggesting that continuity and role-specificity, rather than training volume alone, are the critical differentiating factors. 3 34
Role-differentiated usability experiences, with clinical staff reporting more positive outcomes than administrative and financial personnel, are consistent with evidence from Ethiopia, where poor system customization contributed to dissatisfaction among diverse user groups. 3 35 Usability has been argued as not being a fixed system property but a relational outcome constructed between system design and specific workflow demands, a theoretical position supported by the present findings. 336,37 These results highlight the need for more granular pre-deployment needs assessments that explicitly account for the workflow requirements of administrative and financial roles alongside clinical ones.
Workflow improvements, particularly in claims processing and patient record retrieval, are consistent with international evidence from Tanzania, Brazil, and the United States demonstrating that EHRS reduces documentation burden and streamlines administrative processes. 115,38,39 In Ghana’s context, NHIS claims automation represents a particularly compelling value proposition for private sector adoption, offering a business case that policymakers could leverage to incentivize broader EHRS uptake among facility owners motivated by operational efficiency and financial sustainability.
The substantive clinical benefits reported, including improved record accessibility, inter-professional communication, and automated medication safety checks, are consistent with systematic reviews identifying these as the most commonly reported positive outcomes of EHRS implementation in LMICs. 22,15 Medication safety improvements are particularly salient in Ghana’s private sector, where pharmacovigilance infrastructure remains underdeveloped, and medication errors are a recognized patient safety concern. 4 40 Similarly, automated drug interaction alerts have been identified among the highest-impact patient safety contributions of EHRS, demonstrating that targeted system features can generate clinically meaningful outcomes even in resource-constrained settings with incomplete implementation, 4 41 a finding aligned with the WHO’s Framework for Action on Interoperable Digital Health. 4 42
The absence of formal EHRS governance frameworks reflects a broader pattern across Sub-Saharan Africa, where digital health technology adoption has consistently outpaced regulatory development, creating governance lag that threatens data integrity and system sustainability. 443,44 Kenya’s eHealth Policy, which established standardized implementation guidelines, interoperability requirements, and data governance frameworks, offers an instructive benchmark, with Mburu and Kamau. 4 45 demonstrating that formal national eHealth policy is associated with more standardized and accountable facility-level EHRS implementation. Financial constraints, echoing findings from Uganda where scalability depended on donor financing, further threaten sustainability. 2 27 India’s Ayushman Bharat Digital Mission demonstrates the transformative potential of dedicated state financing for EHRS infrastructure at scale, 4 46 offering a model Ghana could adapt through innovative mechanisms, including public-private partnerships and performance-based financing linked to EHRS adoption.
To strengthen EHRS implementation in Ghana, several interventions are recommended. Adopting Rwanda’s phased, mentorship-supported training model would address competency gaps among frontline staff. 3 34 Developing a national EHRS policy modelled after Kenya’s eHealth framework would standardize implementation and ensure accountability across facility types. 4 45 Fostering public-private partnerships with technology firms could offset infrastructure costs and improve system maintenance, 4 47 while implementing structured hybrid paper-digital downtime protocols, as demonstrated in Malawi, would preserve data integrity during outages. 3 30 These recommendations collectively address the sociotechnical misalignments identified in this study and are consistent with WHO principles emphasizing the interdependence of infrastructure, governance, workforce capacity, and financing as pillars of sustainable digital health transformation. 4 42 Future research should examine EHRS implementation in public sector facilities and other Ghanaian municipalities, and explore longer-term adoption trajectories as facilities mature in their digital health journeys.
Strengths and limitations
A qualitative, interpretive design was adopted to generate contextually rich insights into EHRS implementation, consistent with health informatics research recognizing the limitations of quantitative approaches in capturing organizational and human dimensions of technology adoption. 448,49 Braun and Clarke’s thematic analysis framework strengthened methodological credibility through its rigorous and flexible analytic approach. Key limitations include a cross-sectional design that precludes assessment of long-term adoption trajectories, sampling restricted to leadership roles that may underrepresent frontline staff experiences, and a single-municipality scope that limits transferability of findings. Nevertheless, researcher triangulation, member checking, iterative co-coding, and a comprehensive audit trail strengthen the credibility and dependability of findings, consistent with established trustworthiness standards in qualitative health research.
Conclusion
The implementation of EHRS in Ghana’s private hospitals demonstrates both the transformative potential and systemic challenges of digital health adoption in LMICs. While infrastructural and financial barriers persist, the documented improvements in workflow efficiency and patient care align with global evidence supporting the efficacy of EHRS. Strategic investments in workforce training, policy development, and sustainable financing are essential to ensure Ghana’s successful transition to a robust digital healthcare ecosystem.
Supplemental material
Supplemental material - Implementation of electronic health record systems in private health facilities: A qualitative study in Ghana
Supplemental material for Implementation of electronic health record systems in private health facilities: A qualitative study in Ghana by Eva Saeh Afriyie, MPhil, Richard Abeiku Bonney, MPhil, Loretta Adu-Boahemaa Antwi, MPhil, Mary Yeboah, MPhil, Kofi Akohene Mensah, PhD in Health Informatics Journal
Footnotes
Acknowledgments
The authors acknowledge the staff of all health facilities who participated in the study.
Ethical considerations
This study received ethical clearance on April 5, 2023, from the Committee for Human Research, Publications, and Ethics at Kwame Nkrumah University of Science and Technology, with reference number CHRPE/AP/238/23, along with administrative approvals from municipal health authorities and the leadership of participating hospitals. This study adhered to the Helsinki Declaration.
Consent to participate
All participants provided written informed consent after being thoroughly briefed on the study’s voluntary nature, confidentiality protections, and their right to withdraw without consequence. The researchers conducted interviews in secure settings, implemented strict anonymization protocols by removing all personal identifiers, and maintained data securely to ensure participant privacy throughout the research process in accordance with ethical research standards.
Authors’ contribution
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Health facilities involved in the study
Breman SDA Hospital, God’s Glory Hospital, Kropo Charity Hospital, and Wisdom Hospital.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.