
Abstract
Objective
This study aimed to develop an EMR-integrated, AI-based nursing handover system (NurSync) through a needs assessment and system development process, as a first step toward improving handover efficiency, reducing documentation burden, and enhancing communication accuracy.
Methods
A mixed-methods design was used. Surveys and focus group interviews with nine shift-working nurses identified challenges in handovers and EMR use. These findings guided the development of NurSync, a dual web–mobile system based on the PASS-BAR protocol and a large language model trained on 17 nursing record types.
Results
Participants reported fragmented EMR structures, repetitive manual documentation, and ambiguity in handover scope. NurSync addressed these by automatically classifying nursing data into four structured categories, enabling real-time access and reducing redundancy.
Conclusion
NurSync was developed as a development and feasibility study integrating AI summarization with EMR data to support handover accuracy, efficiency, and consistency. Its structured design and dual-platform interface show promise for supporting clinical decision-making and communication, pending empirical validation in future studies.
1. Introduction
Population aging and the increasing societal demand for healthy living have become prominent global challenges. 1 In Korea, however, the number of active nurses remains critically low, with only 3.8 nurses per 1,000 population recorded in 2018, a figure substantially below the OECD average of 7.4. Although the number of newly licensed nurses per 100,000 population stood at 35.0—exceeding the OECD average of 26.5—this discrepancy indicates a persistent gap between the overall nurse supply capacity and the actual workforce engaged in healthcare delivery. 2 The deterioration of the nursing work environment has further exacerbated this issue, leading to frequent resignations and leaves of absence among nursing staff. 3 A 2021 survey by the Korean Health and Medical Workers’ Union revealed that more than half of nurses were dissatisfied with their workload, work intensity, and work-life balance, with many unable to secure minimal rest periods and routinely skipping meals during extended overtime shifts.4,5 In this context of systemic understaffing and unsustainable workload demands,3–5 inefficiencies in routine yet safety-critical clinical processes—such as nursing handover—are significantly amplified, making workflow optimization not merely desirable but urgently necessary.6,7
Nursing handover, performed repeatedly across every shift change by nurses already burdened by understaffing3-5 and excessive documentation demands, 8 constitutes a pivotal process for safeguarding patient safety and ensuring continuity of care. 9 Most healthcare institutions employ a combination of written and verbal handover practices, which are prone to frequent problems such as omitted information, incomplete documentation, and subjective reporting. 10 Given that inaccurate or missing information can precipitate medical errors, the necessity for precise and comprehensive documentation is paramount to patient safety.6,11 Nonetheless, several impediments—including time pressures, non-standardized terminology, outdated information, frequent interruptions, and ambiguous role delineations—undermine the quality and reliability of handovers.6,7,11,12 The average duration of a handover ranges from 20 to 30 minutes,6,7 during which novice nurses frequently experience difficulties in identifying and organizing critical information, thereby contributing to heightened stress and job dissatisfaction.13,14 The reliance on unstructured handover formats further compromises documentation integrity, 6 ultimately detracting from nursing efficiency, mental well-being, and patient safety. Consequently, there is an urgent need for standardized training and procedural enhancements to optimize the handover process.7,11,13
The Electronic Medical Record (EMR) system, which electronically captures, stores, and manages medical information, serves as a fundamental tool for healthcare institutions to enhance care quality and ensure patient safety. 15 Despite the recognized advantages of EMRs, such as real-time accessibility and improved data accuracy, many nurses report that these systems are slow, complex, and unintuitive, impeding their workflow. 8 Moreover, dissatisfaction with EMR-based handover tools is widespread, with 50% of nurses finding printed reports cumbersome and 69% criticizing them for containing excessive and irrelevant information. 8
Advances in artificial intelligence (AI) technologies, particularly in natural language processing and large-scale data analysis, have opened new avenues for innovation in healthcare. 16 AI applications in nursing are expanding across domains such as clinical decision support, patient monitoring, task automation, and education, with growing acceptance among nursing professionals.17–19 Recent evidence indicates that AI integration alleviates nursing workload, promotes patient safety, and supports patient-centered care models. 20 However, the application of AI specifically to nursing handover remains limited; a scoping review found that most existing technological solutions rely on low-complexity tools, with advanced approaches such as natural language processing largely unexplored and the majority of systems still in pilot stages. 21 Although recent evidence suggests that generative AI can reduce handover documentation time substantially, 22 few systems have been developed through systematic needs assessment or designed for direct EMR integration with structured handover protocols, underscoring the need for a clinically grounded approach.
Given the severity of Korea’s nursing shortage and the resulting workload pressures described above,3–5 interventions that reduce the burden of routine yet safety-critical clinical tasks are urgently needed.17,20AI-based nursing handover systems are expected to improve efficiency, accuracy, and consistency by automatically summarizing records and visualizing patient status, thereby allowing nurses to focus more on direct patient care. Therefore, this study aimed to identify the requirements for and develop an EMR-integrated, AI-based web and mobile handover system grounded in the PASS-BAR protocol, framed as a development and feasibility study. The findings are intended to provide a foundation for future empirical evaluation of the system’s effectiveness in enhancing handover efficiency and safety, reducing nursing workload, and improving the quality of nursing care.
2. Methods
2.1. Study design
This methodological study aimed to assess the needs for, and subsequently develop, a web- and mobile-based EMR-integrated AI system to enhance nursing handover processes. The research was conducted in two distinct phases: the needs assessment phase and the development phase. During the needs assessment phase, surveys and focus group interviews were undertaken to evaluate the current state of nursing handovers and to establish foundational data necessary for developing an EMR-linked AI application. The development phase involved completing the system through close collaboration with a multidisciplinary team of application development experts.
2.2. Needs assessment phase
2.2.1. Survey
A descriptive research design was employed to investigate the current status of nursing handovers among ward nurses working shifts. Participants comprised nine nurses engaged in rotating shifts within the oncology ward of C University Hospital in Seoul. All participants had a minimum of one year of clinical experience and provided informed consent to participate. Inclusion criteria were: (1) registered nurse status; (2) currently working rotating shifts; (3) a minimum of one year of clinical experience; and (4) employed in the oncology ward of the study site. Nurses were excluded if they were on leave of absence, assigned to non-clinical or administrative roles, or had not performed a shift handover within the preceding month. The sample was evenly stratified by clinical experience: three nurses with 1–3 years, three with 4–5 years, and three with over 6 years of experience. Data collection occurred in June 2025. The researcher personally explained the study objectives to each participant and obtained informed consent prior to questionnaire administration. Data analysis was conducted using SPSS version 22.0. Descriptive statistics—including frequencies, percentages, means, and standard deviations—were calculated to describe participant demographics and nursing handover characteristics.
2.2.1.1. General and handover-related characteristics
The general characteristics included variables such as gender, age, education level, hospital size, and work experience. The handover-related characteristics consisted of questions regarding the handover practices in the participants’ current ward.
2.2.1.2. Handover evaluation
This refers to the extent to which nurses perceive the effectiveness of the handover process between outgoing and incoming staff during shift changes in the general wards under study. A modified version of the Handover Evaluation Scale, originally developed by O’Connell et al. (2008) 23 and adapted by Kim et al. (2014), 24 was employed. The scale comprises 18 items rated on a 7-point Likert scale, with higher scores reflecting a more favorable evaluation of the handover process. The instrument demonstrated excellent internal consistency, with a Cronbach’s α of .94 at the time of development. In the present sample, Cronbach’s α was 84.
2.2.1.3. User satisfaction with the EMR system
This dimension assesses users’ satisfaction regarding system performance, utilization, and work-related factors. Satisfaction was measured using a tool developed by Kim (2006), 25 which consists of three subdomains: performance satisfaction, utilization satisfaction, and work satisfaction. The instrument includes a total of 20 items rated on a 5-point Likert scale, where higher scores indicate greater satisfaction. The tool exhibited good reliability, with a Cronbach’s α of .85 at the time of development. In the present sample, Cronbach’s α was 90.
2.2.2. Focus group interviews (FGIs)
Qualitative focus group interviews were conducted to explore difficulties, challenges, and potential improvements related to nursing handovers. Participants included nurses with at least one year of clinical experience, currently performing nursing handovers while working shifts in wards of a university hospital in Seoul. Inclusion criteria were: (1) registered nurse status; (2) currently working rotating shifts in a ward setting; (3) a minimum of one year of clinical experience; and (4) active performance of nursing handovers as part of current duties. Nurses were excluded if they were on leave, in non-clinical roles, or had not participated in a handover within the preceding four weeks. Groups of 3 to 5 members were deemed appropriate to facilitate dynamic discussions, as larger groups may hinder effective management. 26 Recognizing that nursing handover is among the most challenging responsibilities for novice nurses following independence—particularly regarding interactions with colleagues and senior staff 14 —participants were stratified by clinical experience to encourage candid and open dialogue. Accordingly, nine participants were divided into three groups based on clinical experience: 1–3 years, 4–5 years, and over 6 years. Each group consisted of three nurses. Semi-structured interview guides, developed and validated by the research team prior to data collection, directed the discussions (Appendix A).
All FGIs were conducted in a confidential setting by the first author, who also documented observations using a quality control form. Interviews were audio-recorded, transcribed verbatim, anonymized, and repeatedly reviewed by the research team. Each focus group session lasted approximately 60 minutes. Data were thematically organized and systematically coded using Atlas. ti 25. Data collection and analysis proceeded concurrently. Theoretical saturation was considered achieved when no new themes or subthemes emerged across successive focus group sessions. Coding was conducted inductively using a thematic analysis approach by the first author. To enhance the rigor of the analytical process, all coded transcripts and emerging themes were subsequently reviewed and verified by the corresponding author; any discrepancies in interpretation were resolved through iterative discussion until consensus was reached. This peer debriefing process served as a primary strategy for ensuring the dependability and confirmability of the analysis. To ensure the credibility of findings, thick description was employed throughout data reporting, and negative case analysis was conducted to identify data that did not conform to emerging themes. The first author’s background as a registered nurse with clinical experience in ward-based care was acknowledged as a potential source of interpretive influence; this was addressed through ongoing discussion with the corresponding author to maintain analytical balance. This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 27 ; a completed COREQ checklist is provided as Supplementary Material (Appendix B).
2.3. System development phase
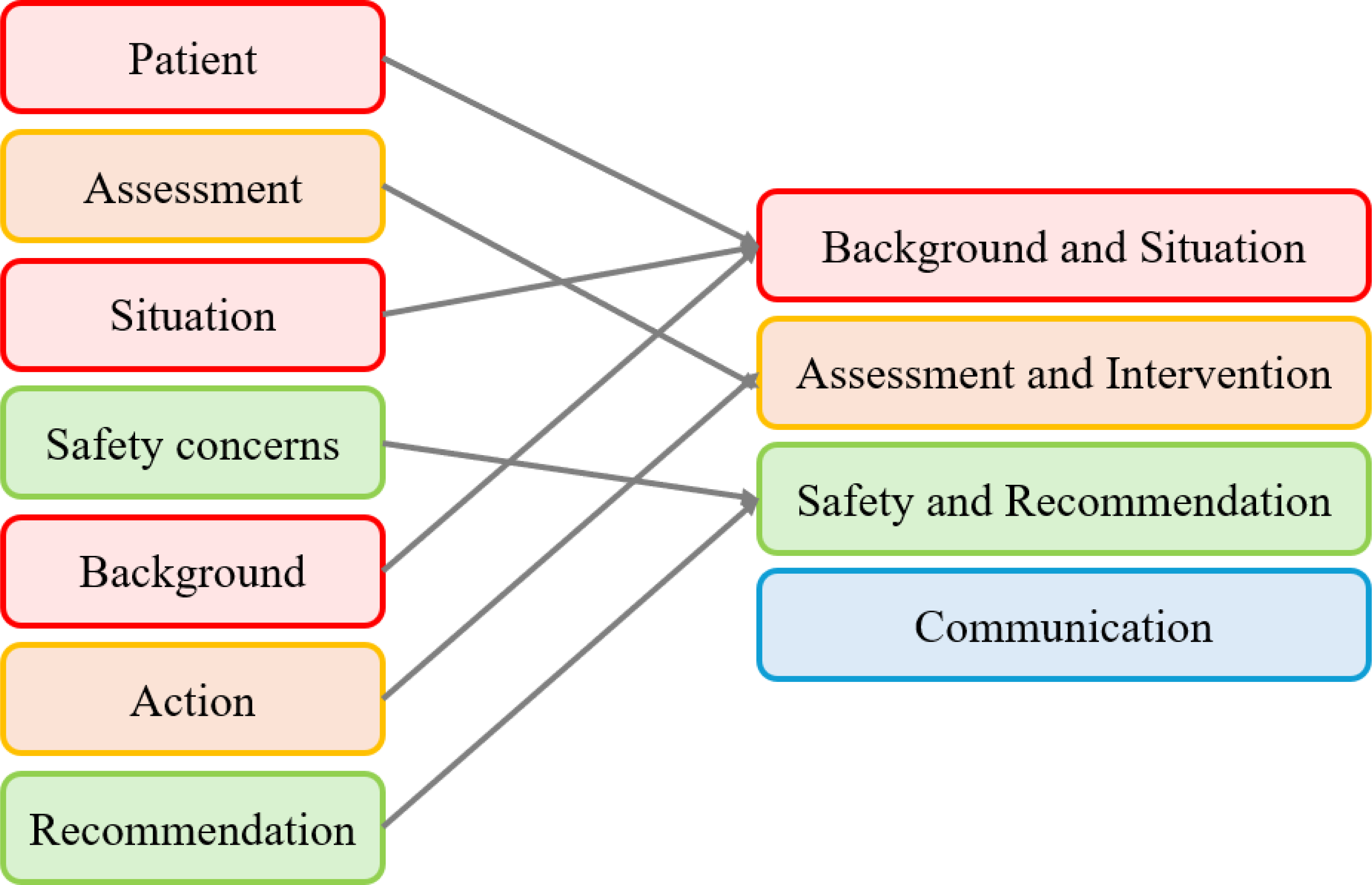
The system development was carried out collaboratively by a multidisciplinary team comprising three web/mobile application experts, one clinical nurse, and one nursing professor. A structured protocol is essential for effective information transfer during nursing handovers, and the PASS-BAR protocol has been specifically designed to meet this need. 24 It encompasses the following components: Patient information (e.g., name, room number, diagnosis), Assessment (e.g., vital signs, laboratory findings), Situation (e.g., immediate clinical concerns), Safety concerns (e.g., fall risk, infection control measures), Background information (e.g., reason for admission, comorbidities), Actions (e.g., pending tasks, interventions), and Recommendations (e.g., anticipated challenges, privacy considerations). This framework is well suited to facilitate comprehensive and systematic nurse-to-nurse handovers. 24 The PASS-BAR protocol provides structured guidance on both the content and sequence of handover information and is recognized as a critical tool for enhancing nurses’ handover competencies. 28
2.4. Ethical considerations
This study received approval from the Institutional Review Board (IRB) of C University (Approval No. MC25EASI0023). Written informed consent was obtained from all participants after they were informed of the study’s purpose, confidentiality measures, anonymity, and voluntary nature of participation. Audio recordings of interviews were used solely for research purposes.
3. Results
3.1. System needs assessment
3.1.1. Survey
3.1.1.1. General and handover-related characteristics
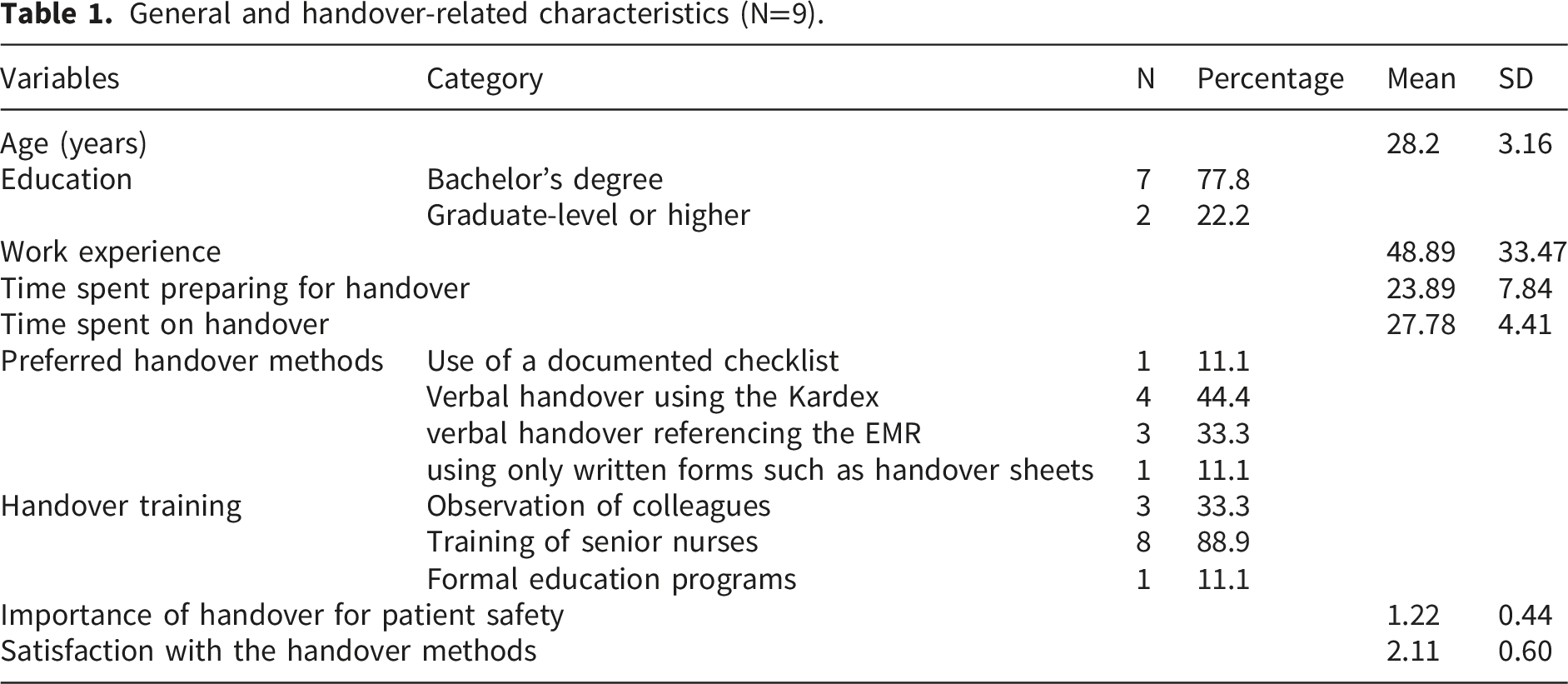
All participants were female registered nurses employed in the oncology ward. The mean age was 28.2 years, with seven participants (77.8%) holding a bachelor’s degree and two (22.2%) possessing graduate-level or higher qualifications. The average clinical experience was 48.89 months.
General and handover-related characteristics (N=9).
3.1.1.2. Handover evaluation
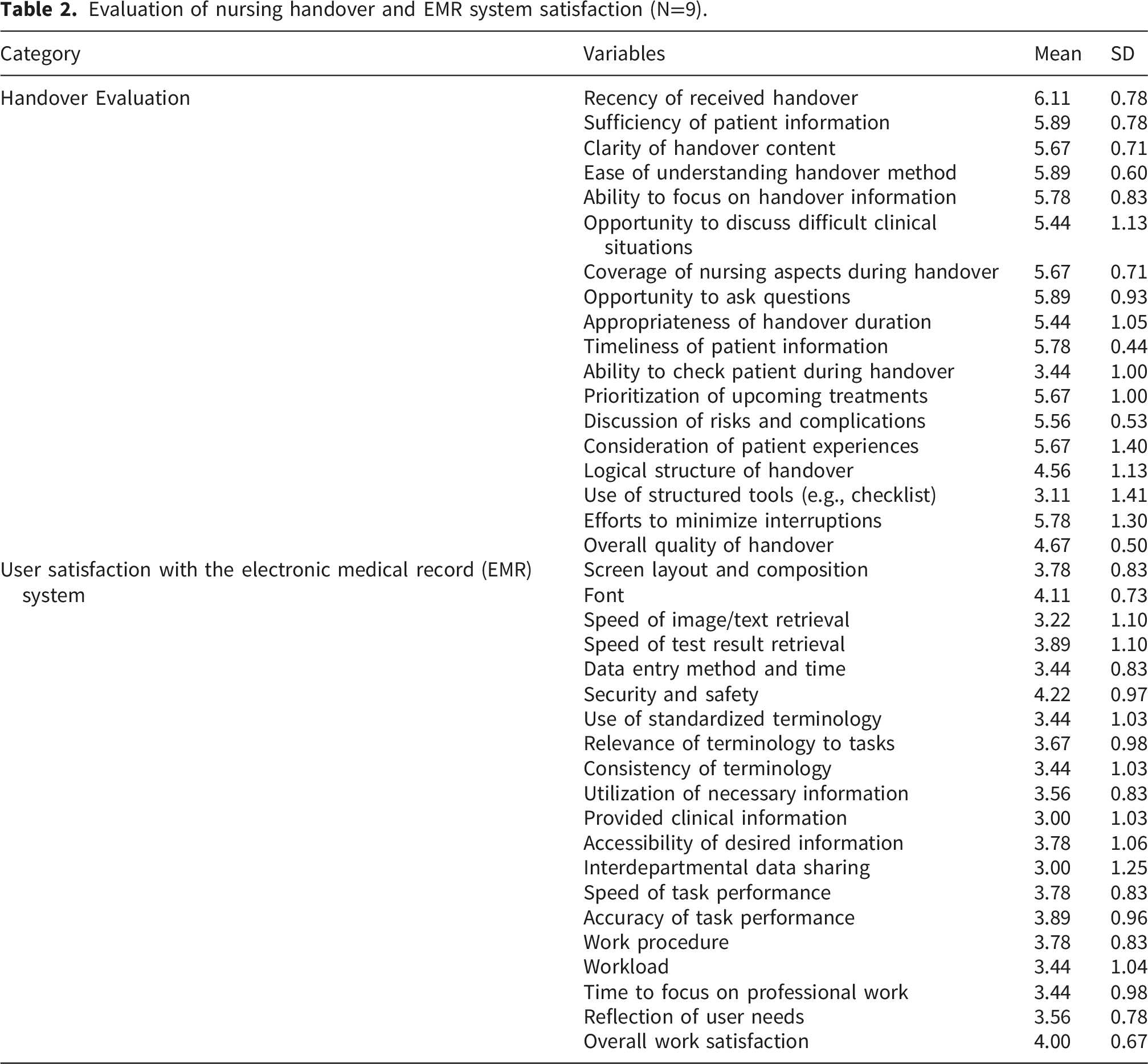
Evaluation of nursing handover and EMR system satisfaction (N=9).
3.1.1.3. User satisfaction with the EMR system
User satisfaction with the EMR system was evaluated using a 5-point Likert scale. The highest satisfaction was reported for system security and safety (4.22 ± 0.97), followed by satisfaction with the fonts used (4.11 ± 0.73), and overall satisfaction with work supported by the system (4.00 ± 0.67). Satisfaction with the accuracy of work (3.89 ± 0.96) and the speed of accessing test results (3.89 ± 1.10) were also relatively high. Moderate satisfaction was noted for screen layout and composition (3.78 ± 0.83), the speed of task performance (3.78 ± 0.83), work procedures (3.78 ± 0.83), and accessibility of desired information (3.78 ± 1.06). The clinical relevance of standardized terms scored 3.67 ± 0.98, followed by satisfaction with how well user needs were reflected in the system (3.56 ± 0.78) and the ability to utilize necessary information (3.56 ± 0.83). Lower satisfaction was observed for the method and time required for data entry (3.44 ± 0.83), consistency of terminology (3.44 ± 1.03), use of standardized terminology (3.44 ± 1.03), workload (3.44 ± 1.04), and available time to focus on professional tasks (3.44 ± 0.98). The speed of retrieving images and text records was rated 3.22 ± 1.10. The lowest satisfaction scores were observed for the quality of clinical information provided (3.00 ± 1.03) and interdepartmental data sharing (3.00 ± 1.25) (Table 2).
3.1.2. Focus group interviews (FGIs)
Themes and subthemes.
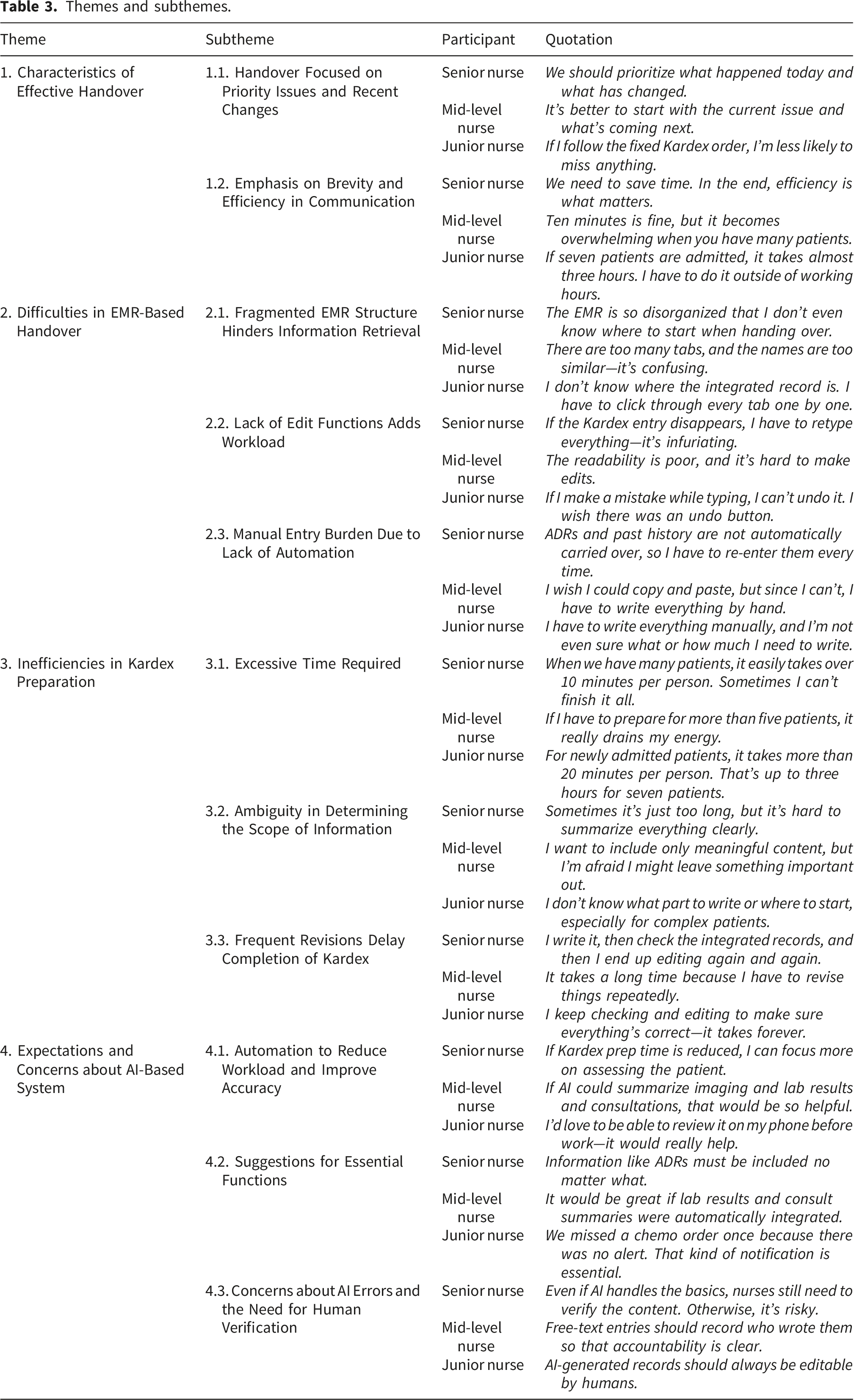
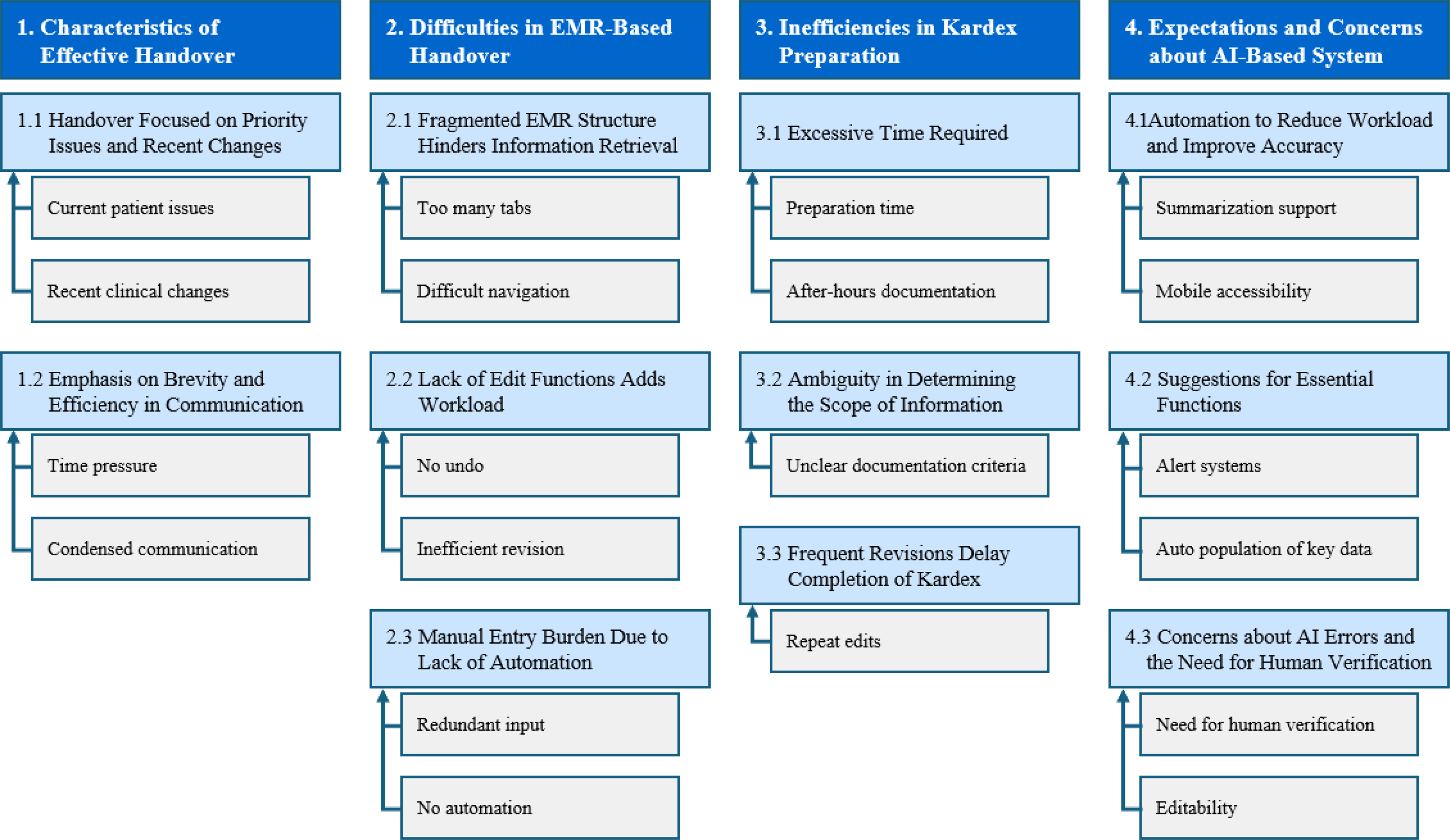
Key themes from focus group interview.
3.1.2.1. Theme 1. characteristics of effective handover
3.1.2.1.1. Subtheme 1.1. handover focused on priority issues and recent changes
Participants emphasized that effective handover prioritizes current patient problems and recent clinical changes. Senior nurses advocated concise communication focused on day-to-day updates rather than repeating entire patient histories. Mid-level nurses concentrated on communicating current problems and future care plans, while junior nurses preferred structured formats to ensure completeness.
3.1.2.1.2. Subtheme 1.2. emphasis on brevity and efficiency in communication
All participants agreed that handovers must be conducted efficiently within limited time. Senior nurses preferred summarizing key points based on clinical judgment. Mid-level nurses stressed minimizing time per patient when handing over multiple patients. Junior nurses reported spending excessive time verifying and organizing information, sometimes during off-duty hours.
3.1.2.2. Theme 2. difficulties in EMR-Based handover
3.1.2.2.1. Subtheme 2.1. fragmented EMR structure hinders information retrieval
Participants consistently reported that information was scattered across multiple EMR tabs, impeding prompt access and retrieval. Senior nurses expressed frustration with the lack of a structured interface; mid-level nurses noted tab similarities causing confusion; junior nurses found the layout challenging to understand, leading to excessive time spent searching.
3.1.2.2.2. Subtheme 2.2. lack of edit functions adds workload
Participants reported difficulty due to limited or absent undo and edit functions. Senior nurses explained that minor errors often necessitated rewriting entire sections. Mid-level nurses described the system as difficult to revise and poorly readable. Junior nurses emphasized the absence of an “undo” button, leading to lost entries after input errors.
3.1.2.2.3. Subtheme 2.3. manual entry burden due to lack of automation
The absence of automation required manual entry of large volumes of data. Senior nurses reported repeatedly entering adverse drug reactions, past histories, and treatments. Mid-level nurses cited lack of copy-and-paste functionality causing redundant entries. Junior nurses struggled with uncertainty regarding required information and lacked standardized guidance.
3.1.2.3. Theme 3. inefficiencies in kardex preparation
3.1.2.3.1. Subtheme 3.1. Excessive Time Required
Participants reported significant time demands in Kardex preparation, especially with multiple patients. Senior nurses noted that time per patient often exceeded ten minutes on busy days. Mid-level nurses described increased physical and mental strain when managing over five patients. Junior nurses often spent two to three hours outside work hours completing documentation for new admissions.
3.1.2.3.2. Subtheme 3.2. ambiguity in determining the scope of information
Participants expressed uncertainty about the amount and type of information to include. Senior nurses found condensing lengthy histories into summaries difficult; mid-level nurses worried about omitting meaningful details; junior nurses struggled especially with patients having extensive histories or ICU backgrounds.
3.1.2.3.3. Subtheme 3.3. frequent revisions delay completion of kardex
Participants noted Kardex documents required frequent updating as new information emerged. Senior nurses reported repeated revisions after reviewing integrated records. Mid-level nurses experienced delays due to ongoing edits. Junior nurses found continuous double-checking and modifications significantly slowed completion.
3.1.2.4. Theme 4. expectations and concerns about AI-Based system
3.1.2.4.1. Subtheme 4.1 automation to reduce workload and improve accuracy
All participants expressed optimism about AI automating repetitive documentation. Senior nurses hoped AI would reduce Kardex preparation time and free more time for patient care. Mid-level nurses believed automated summaries of tests and consultations would facilitate handovers. Junior nurses were particularly enthusiastic about AI-generated content review on mobile devices before shifts.
3.1.2.4.2. Subtheme 4.2. suggestions for essential functions
Participants identified key desired features for an AI handover system. Senior nurses emphasized inclusion of critical information such as adverse drug reactions, current medications, and surgical plans. Mid-level nurses advocated automatic integration of medical history, treatment records, and lab results. Junior nurses requested auto-population of patient complaints, procedural history, and alert systems for chemotherapy or imaging orders.
3.1.2.4.3. Subtheme 4.3. concerns about AI errors and the need for human verification
Despite high expectations, participants voiced concerns about relying solely on AI. Senior nurses warned erroneous data might propagate through AI, risking patient safety. Mid-level nurses stressed the importance of traceability and accountability for AI-generated entries. Junior nurses emphasized the need for manual editing capabilities to correct AI errors.
3.2. System development
Based on the results of the needs assessment, we developed a dual-platform (web and mobile) AI-based nursing handover system, hereby referred to as NurSync (Figure 2). The system pipeline operates as follows: (1) structured nursing records (17 types) are retrieved from the data source; (2) each item is processed by the on-device AI model to assign a PASSBAR rank and mapped to protocol categories (Figure 3); (3) nurses may add supplementary notes; (4) items are formatted into structured inference prompts with record-type-specific context; and (5) ranked items are assembled into a handover summary under four PASSBAR categories, representing a reorganization of existing EMR data rather than newly generated content. To mitigate the risk of AI errors, three architectural safeguards were implemented: (1) every AI-prioritized item maintains a direct link to its source nursing record for instant verification; (2) AI-generated handover summaries are presented on a dedicated screen, while all 17 original record types remain fully accessible in their unaltered form; and (3) on-device inference ensures no patient data is transmitted to external servers. The system operates as a decision-support tool, with nurses retaining full authority to review, override, or supplement AI prioritizations. System development flow. Components of the study based on the PASS-BAR framework.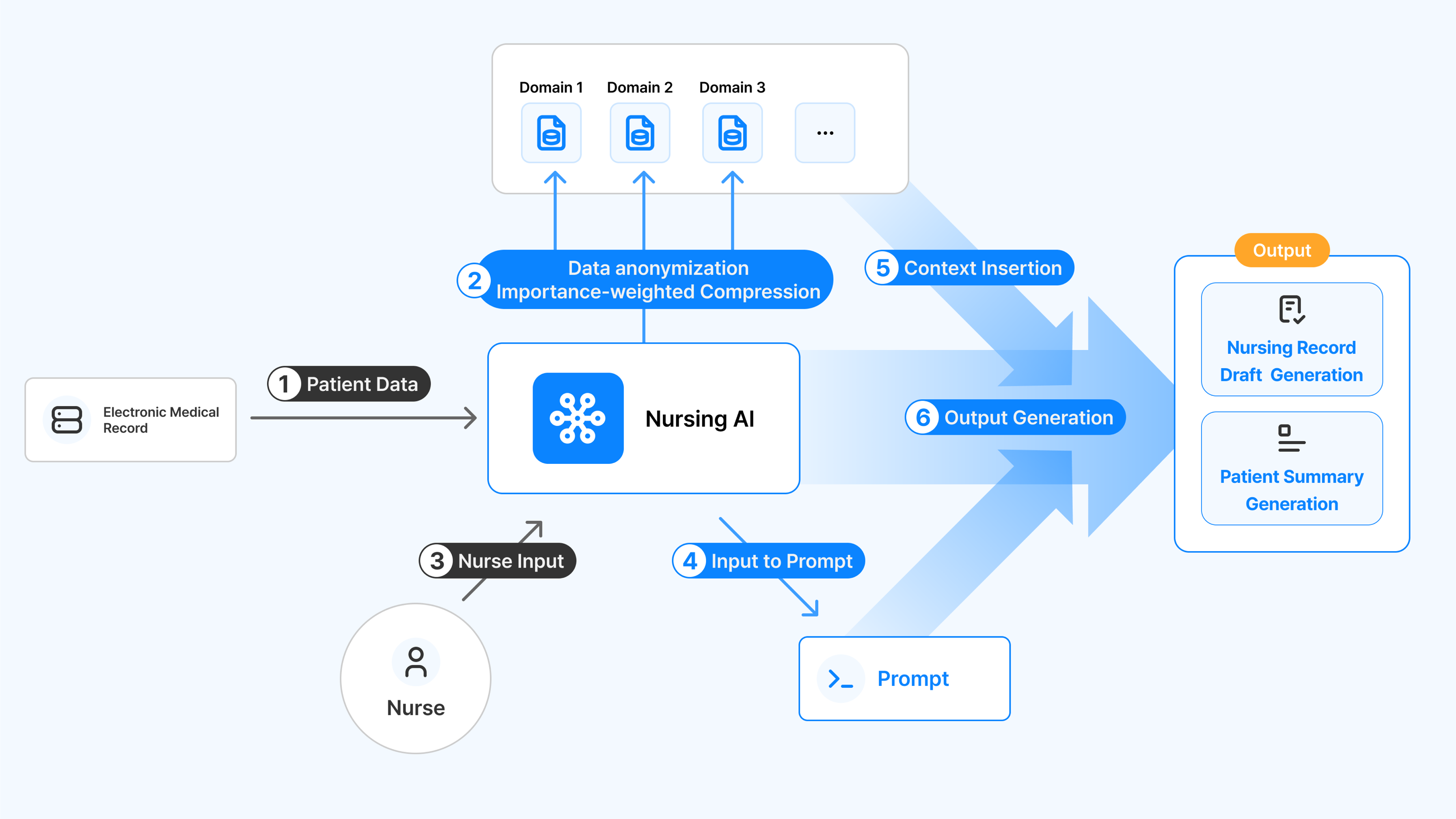
3.2.1. Planning and design
Based on survey and focus group findings, this study targeted major challenges in nursing handovers, such as repetitive documentation, omission of critical information, and inefficiencies from dual recording. Four objectives guided system development: automating data input, enabling AI-based extraction and summarization, reducing last-minute revisions, and integrating handovers with EMR documentation. Accordingly, web- and mobile-based platforms with unified structures were designed for both desktop and mobile use. The system adopted a streamlined PASS-BAR model, reorganized into four categories—Background & Situation, Assessment & Intervention, Safety & Recommendations, and Communication—allowing AI to analyze 17 nursing record types and provide standardized, efficient handover support. In the current development phase, the system was tested using a simulated dataset based on first-cycle chemotherapy nursing records, designed to reflect the structure and content of actual clinical EMR data without accessing live hospital databases. Data privacy and security were ensured throughout development by using de-identified, simulated data.
3.2.2. Software design (UI/UX design)
The UI/UX design was guided by a needs assessment to optimize handover efficiency and reduce cognitive load. The web application employed a table-based layout reflecting EMR structures, enabling simultaneous viewing of multiple records and categorization of content into four clinically relevant sections: Background & Situation, Assessment & Intervention, Safety & Recommendations, and Communication. Visual features, such as keyword chips, vital sign trends, and consultation notifications, enhanced clarity and real-time recognition. The mobile application adopted a card-based interface with expandable bottom sheets and threaded memos, supporting ward rounds and decentralized care through real-time synchronization. Prototyping with Notion and Figma allowed iterative refinement to resolve issues of fragmented information, lack of editing, and documentation burden. Overall, the design ensured usability, clinical relevance, and workflow integration to facilitate accurate, timely, and efficient communication.
3.2.3. AI model development
An AI model was developed to classify and prioritize critical nursing information for clinical handovers. A 2.1B-parameter language model (Kanana-nano) was fine-tuned via a two-stage sequential LoRA strategy: Stage 1 (domain adaptation) used 63,953 instruction-response pairs of Korean language and medical corpora (90/10 split); Stage 2 (task-specific tuning) used 28,055 pairs in which experienced clinical nurses manually classified handover items by PASSBAR rank (1 = routine, 2 = conditionally important, 3 = essential; 95/5 split). All training data comprised entirely fictitious patient scenarios authored by clinical nurses; no real patient records were used. Model validation used a separate, independently sampled dataset of 320 items derived from real clinical records, with full de-identification applied. The model achieved 77.9% accuracy on the KorMedMCQA-Nurse benchmark (17 percentage points above the base model) and 96.28% accuracy on PASSBAR rank classification against expert nurse-annotated ground truth; misclassifications occurred predominantly between adjacent ranks, carrying minimal clinical risk. The model underwent independent external verification by the Korea Artificial Intelligence Verification Institute.
3.2.4. Web application development
The web application was built with a reusable component-based architecture, integrating specialized tables for 17 nursing record types. AI inference was supported through a custom Web Assembly (WASM) module with cache optimization, while real-time synchronization using Supabase ensured consistency between nursing records and AI outputs (Figure 4). Sample page of NurSync system (webpage).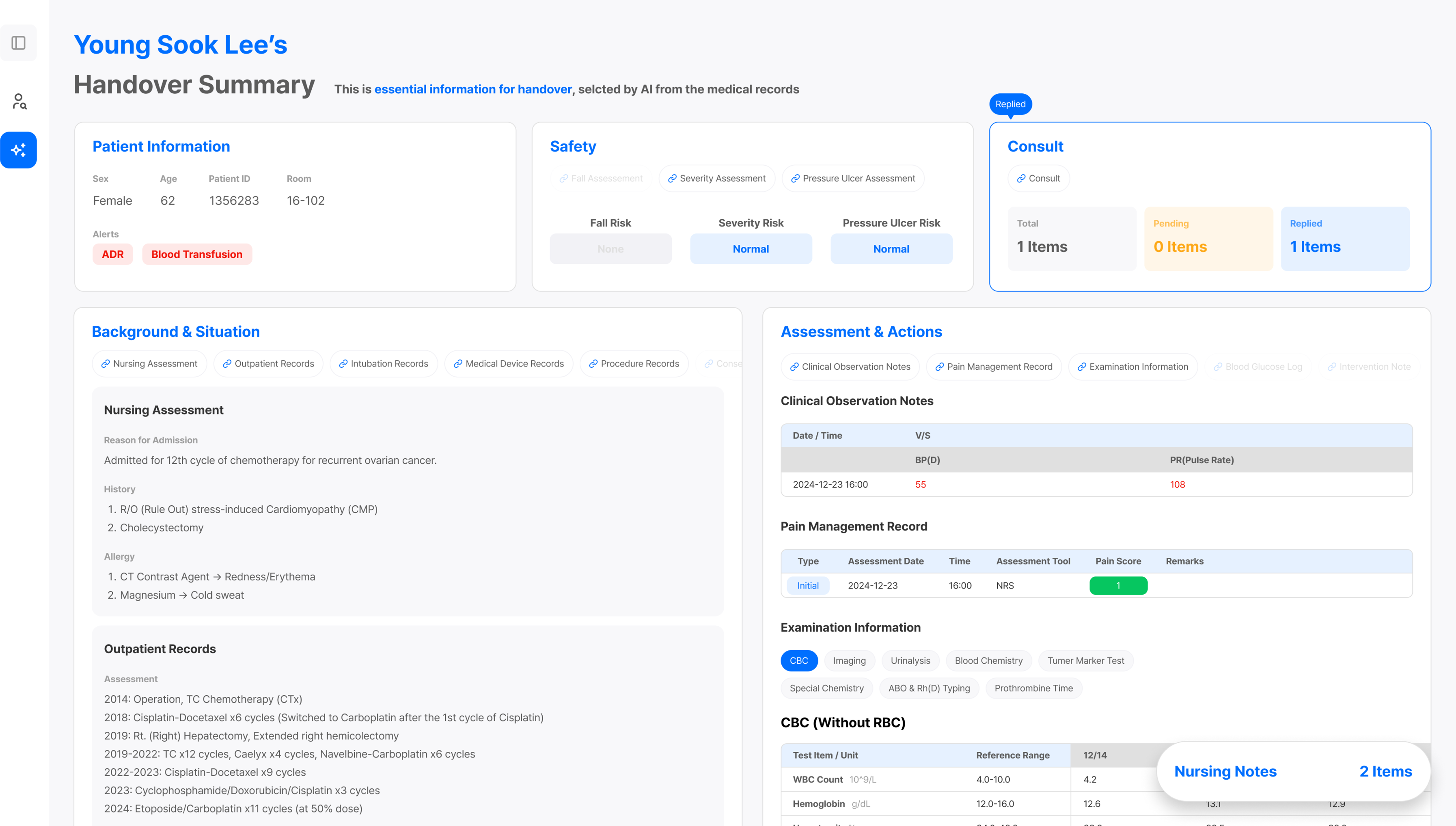
3.2.5. Mobile application development (iOS)
The iOS mobile app maintained functional and data consistency with the web version while optimizing for touch-based interactions. Core components and handover screens were implemented with Supabase for data storage and llama. cpp for embedded AI inference. Iterative quality assurance addressed UI and performance issues, enhancing usability and system stability (Figure 5). Sample page of NurSync system (mobile application).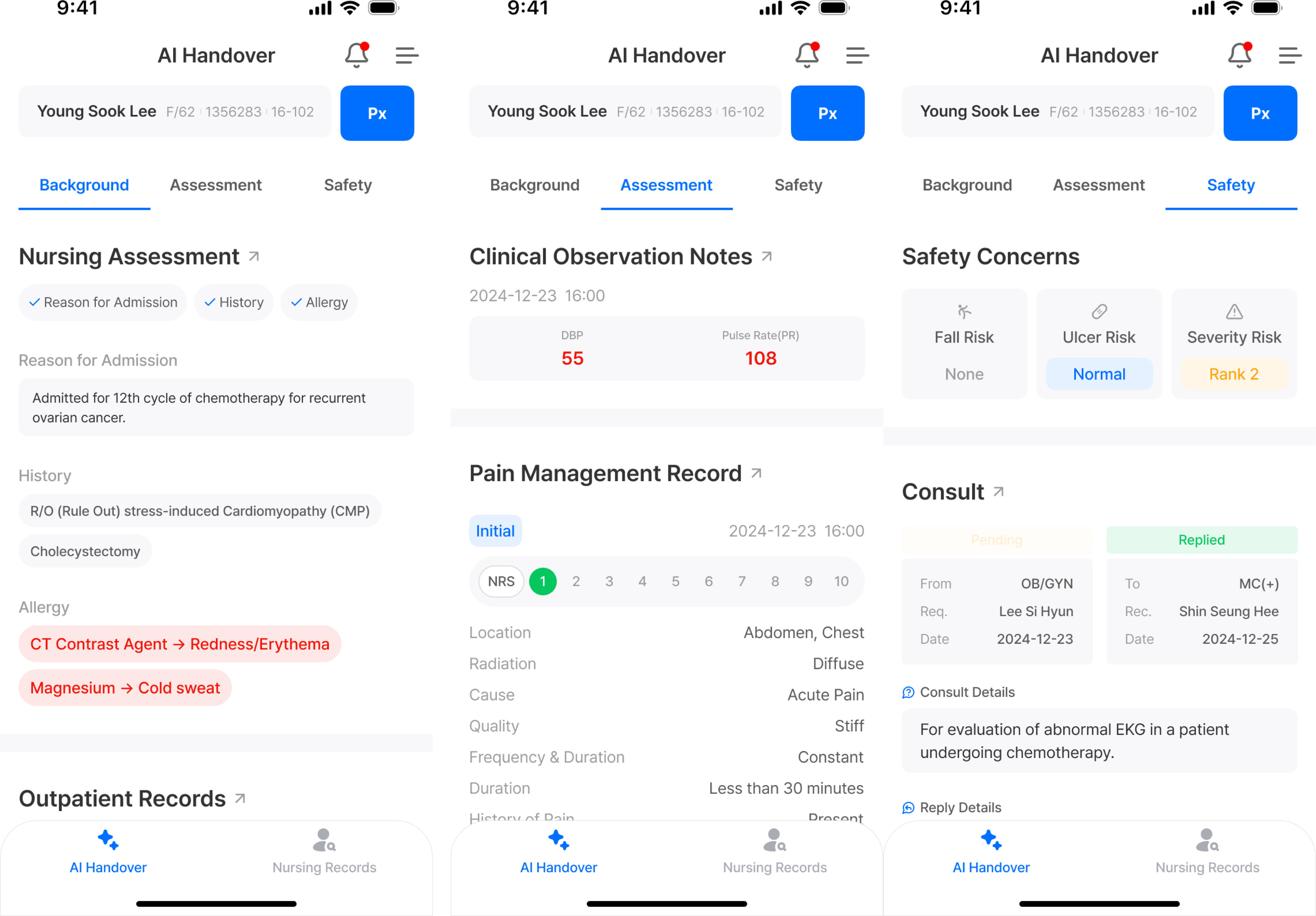
4. Discussion
The findings of this study indicate that nurses spent an average of 23.89 ± 7.84 minutes preparing for handovers, with the handover process itself taking an average of 27.78 ± 4.41 minutes. These results underscore that handovers impose a considerable time burden on nurses, potentially reducing work efficiency. 29 Given that handovers are conducted multiple times daily, non-standardized processes can exacerbate inefficiencies and increase the risk of information omissions and communication errors. 30 To address such issues, structured communication protocols such as SBAR and ISBAR have been widely implemented, demonstrating effectiveness in reducing handover time, minimizing information omissions, and enhancing nurse satisfaction.31,32 In this study, NurSync was developed based on the PASS-BAR protocol and integrated AI technology to automatically summarize and classify handover information into clinically relevant categories. This approach is expected to effectively reduce time burdens, prevent information omissions, and enhance the standardization and efficiency of nursing handovers.
Survey findings revealed moderate satisfaction with the existing EMR system, with scores ranging from 3.00 to 4.22. Notably, data retrieval speed (3.00) and editing functions (3.11) received particularly low ratings. These findings align with previous studies indicating that limitations within EMR systems not only hinder nursing work efficiency but also increase time consumption through repetitive data entry and corrections, thereby contributing to heightened work-related stress. 33 In response, this system was developed to integrate AI-based functionalities that facilitate rapid data retrieval and streamline editing processes, thus reducing nurses’ workload and potentially improving overall usability and satisfaction.
Focus group interviews revealed four major thematic areas: characteristics of effective handover, challenges in EMR-based communication, inefficiencies in Kardex documentation, and expectations and concerns regarding AI-based systems. Nurses emphasized the need for concise, priority-focused handovers; however, they reported difficulties arising from fragmented EMR interfaces and the repetitive nature of Kardex documentation. While participants expressed positive expectations regarding AI’s potential to reduce workload and improve accuracy, they also highlighted concerns related to transparency and the need for manual editing capabilities. These concerns are consistent with previous research indicating that although AI contributes to enhancing efficiency and accuracy in nursing tasks—such as automated documentation and clinical decision support—it also raises ethical and practical issues, including algorithmic bias, opacity, and the necessity for human oversight.17,18,34
To address these multifaceted challenges, this system was developed as an AI-based handover system structured on the standardized PASS-BAR protocol. Specifically, the system reorganized PASS-BAR into four clinically relevant categories—Background & Situation, Assessment & Intervention, Safety & Recommendations, and Communication—and employed AI to automatically classify and summarize 17 types of nursing records. This design mitigates information fragmentation by enabling the simultaneous review of critical data on a single interface, thereby improving both the speed and accuracy of handovers. By minimizing repetitive documentation and providing structured, real-time overviews of patient information, this system is expected to reduce the likelihood of information omissions and communication errors during shift changes while enhancing system usability.
Furthermore, to support diverse work environments, this system was developed as both a web-based and a mobile-based platform. The web application was optimized for desktop use within nurses’ stations, while the mobile version was designed for quick access during ward rounds or shift transitions. This dual-platform approach enhances flexibility and accessibility, enabling nurses to efficiently retrieve structured handover information in real time regardless of their location. The unified design and consistent structure across platforms minimize the learning curve, thereby improving usability, particularly in dynamic clinical settings.
These findings align with the broader trajectory of AI-driven handover research. Recent evidence demonstrates that generative AI integration into nursing information systems can substantially reduce handover documentation time, 22 consistent with the efficiency gains observed in the design of NurSync. Furthermore, the limited adoption of NLP-based approaches in existing handover technology underscores the contribution of this study, 21 which combines a fine-tuned large language model with direct EMR integration and a structured handover protocol, offering a clinically grounded direction for advancing the field.
This study has several limitations. First, generalizability is constrained by the single-center design and small sample size (N = 9). Although participants were purposively stratified by clinical experience to maximize variation in perspectives, and data collection continued until theoretical saturation was achieved, the findings reflect the specific context of a single oncology ward at one university hospital in Seoul and may not be transferable to other clinical settings, specialties, or healthcare systems. Second, as pre- and post-implementation evaluations were not conducted, the actual impact of this system on workflow efficiency, user satisfaction, and patient safety remains unassessed. In particular, no experimental validation of the AI model’s outputs in real clinical environments was conducted in this phase; while model accuracy was evaluated against expert-annotated ground truth and verified externally, the potential impact of AI misclassification on clinical decision-making has not been empirically assessed. Although architectural safeguards were implemented to minimize risk, the safety and reliability of the system in live clinical use requires rigorous prospective evaluation. Future research should systematically evaluate these outcomes following system deployment to determine its effectiveness and inform further improvements.
5. Conclusion
This study developed NurSync, an AI-based, EMR-integrated web and mobile system designed to enhance the efficiency and effectiveness of nursing handovers. By automatically extracting and summarizing key information from 17 types of nursing records, this system substantially reduces the time and effort required for handover preparation and documentation.
In conclusion, this study developed NurSync as a development and feasibility study, providing a structured AI-based EMR-integrated system designed to streamline nursing handovers through automatic extraction and summarization of key information from nursing records. NurSync is designed to reduce documentation burden, support accurate information delivery, and enhance shift-to-shift communication, particularly for novice nurses and those managing heavy caseloads. The system’s dual-platform design ensures flexible, real-time access, ultimately improving efficiency, accuracy, and patient safety. Future studies should further evaluate its long-term effects on workflow, nurse satisfaction, and patient outcomes.
Supplemental material
Supplemental material - Needs assessment and development of an EMR-integrated AI system to enhance nursing handover: NurSync
Supplemental material for Needs assessment and development of an EMR-integrated AI system to enhance nursing handover: NurSync by Sojung Park, Jeongseok Kang, Namhun Kim and Yaelim Lee in Health Informatics Journal.
Footnotes
Ethical considerations
Ethical approval for this study was obtained from the Institutional Review Board of C University (Approval No. MC25EASI0023).
Consent to participate
Written informed consent to participate in this study was obtained from all individual participants included in the study.
Author contributions
Authors’ initials are used to designate them. Conceptualization: YL, SJ, data curation: JS, NH, data validation: JS, NH, formal analysis: YL, SJ, investigation: SJ, methodology: YL, SJ, project administration: YL, software: JS, NH, supervision: YL, visualization: SJ, writing—original draft: YL, SJ, writing—review & editing: JS, NH.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Korea Technology and Information Promotion Agency for SMEs (TIPA) in 2025.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.