
Abstract
Introduction
Standardizing patient data collection and analysis facilitates accurate reporting and enhances communication among healthcare teams. Given the high prevalence of leishmaniasis in specific geographic regions of Iran and the critical role of registry systems, this study aimed to identify the essential data elements required for developing a comprehensive registry system for patients with leishmaniasis.
Methods
This descriptive-applied study was conducted in 2024 in two phases: a literature review (2011-2024) to identify data elements for leishmaniasis, followed by expert consultation to prepare an initial draft of the minimum data set.
Results
A total of 60 data elements with a content validity ratio (CVR) ≥ 0.75 were confirmed and organized into 10 subgroups for the comprehensive leishmaniasis registry. The subgroups comprised: geographic location of registration; identity and demographic information; travel and changes of residence; characteristics of the patient’s dwelling; medical history and current medications; prior history of leishmaniasis; disease-specific information; laboratory data; therapeutic interventions; and follow-up of treatment discontinuation.
Conclusion
Considering the pivotal role of registry systems in disease management, prevention, treatment, and resource allocation, designing a comprehensive registry—particularly for endemic and region-specific diseases such as leishmaniasis is essential.
Introduction
Leishmaniasis is a zoonotic disease caused by a parasite and occurs in three clinical forms: cutaneous leishmaniasis (CL), mucocutaneous leishmaniasis (MCL), and visceral leishmaniasis (VL).1,2 Today, this disease has become one of the most prevalent diseases in certain regions, to the extent that the World Health Organization (WHO) has classified it as a “major uncontrolled disease” and recognizes it as one of the six most important and widespread tropical diseases worldwide. 1 Studies indicate that approximately 12 million people worldwide are affected by this disease, around 350 million people are at risk annually, and about 2 million new cases are reported each year, of which nearly 1.5 million are cases of cutaneous leishmaniasis. 3 This disease is reported in various countries, with about 90% of cases occurring in Bangladesh, Brazil, India, Sudan, Iran, Afghanistan, Nepal, Syria, Saudi Arabia, and Peru—countries with tropical and subtropical climates favorable for the growth and proliferation of the parasite.4,5
The Middle East, due to its climatic, geographical, and environmental conditions, is considered one of the regions with a high prevalence of leishmaniasis. 3 In Iran, the prevalence of this disease is also of great concern, with approximately 20,000 new cases of cutaneous leishmaniasis reported annually. 6 To date, cases of the disease have been reported from most regions of the country, and it is regarded as one of the most significant health challenges in 15 provinces. 7 Therefore, the control, management, and protection of individuals against this disease, both in Iran and globally, are considered fundamental goals of the WHO and health systems, necessitating the development of strategies and policies in this regard. 8
For controlling and managing the incidence and prevalence of various diseases, including leishmaniasis, the health system must not only possess a dynamic and flexible structure but also provide the foundation for the collection of health data and information based on evidence and systematic reporting. Such a system ensures the availability of accurate and meaningful data, enabling effective interventions for the prevention, control, and management of diseases, as well as evidence-based decision-making for health policy and planning.9–12
Today, due to changes in disease incidence and prevalence patterns, advancements in electronic and communication networks, population growth, migration, and similar factors, the WHO emphasizes the importance of disease surveillance systems and the need for revision and reevaluation of each country’s healthcare system in terms of implementing disease registry systems.13,14 Consequently, given the significance of effective and efficient disease registry systems for the organization and management of health information at both micro and macro levels, as well as their role in maintaining and improving patient health and enhancing the efficiency and effectiveness of care programs, many countries have established disease registries.15,16
One of the goals of health informatics is to develop electronic health information systems, and developing a comprehensive registry system for various diseases can be one of these objectives. Disease registry systems worldwide seek improved methods to address challenges in healthcare delivery.17,18 In most countries, the initial step involves establishing systematic and continuous reporting and recording of disease data. Based on information generated by the registry, healthcare systems are structured to analyze, interpret, and continuously disseminate this data while implementing necessary measures and interventions for disease control and management.19–22 Thus, disease registries are regarded as core components of national health information systems and tools for disease management. They provide critical insights into disease burden, incidence and prevalence rates, trends and patterns, and the identification and investigation of cases for epidemic control.23–25
The leishmaniasis registry system in healthcare centers systematically records and maintains patient information and enables the assessment and comparison of patients’ conditions before and after treatment interventions. 8 The objectives of patient data registration include standardization of recording, collection, and analysis of clinical data; providing accurate and up-to-date statistics on the number and treatment of patients; monitoring patient status; documenting medical history, laboratory findings, clinical signs, treatments, clinical course, and treatment outcomes; organizing drug prescriptions; unifying treatment approaches based on standardized clinical guidelines in healthcare centers; and enabling information exchange with other hospitals.8,14
Considering the significance of disease registries on the one hand and the prevalence of leishmaniasis in different regions of the country on the other, this study was conducted to identify the essential data elements for a comprehensive cutaneous leishmaniasis patient registry system. This study focused specifically on cutaneous leishmaniasis (CL). Other clinical forms of leishmaniasis, including visceral leishmaniasis (VL) and post-kala-azar cutaneous leishmaniasis (PKDL), were not included in the scope of this study due to their distinct epidemiological, clinical, and therapeutic characteristics.
Methods
The present study was an applied, descriptive cross-sectional study conducted in 2024 to determine the data elements of a comprehensive registry system for patients with leishmaniasis and was approved by the Ethics Committee of the Faculty of Medical Sciences, Esfarayen (Ethical code: IR. Sfarayenums.REC.1400.008).
The study was performed in two stages to identify the data elements and to establish a minimum data set.
The first step of this study aimed to identify the data elements of a comprehensive registry system for patients with leishmaniasis. A fast search was conducted to retrieve articles related to the research objective that focused on minimum datasets and data elements for patients with leishmaniasis were searched in the PubMed, Web of Science, and Scopus databases. The keywords used in this search included “dataset,” “minimum dataset,” “leishmaniasis,” “registry,” and “information system.” The inclusion criteria comprised data elements related to patients diagnosed with cutaneous leishmaniasis (CL). Data elements associated with other clinical forms of leishmaniasis, including visceral leishmaniasis (VL) and post-kala-azar dermal leishmaniasis (PKDL), were excluded due to substantial differences in disease pathophysiology, diagnostic approaches, treatment protocols, and follow-up requirements compared to cutaneous leishmaniasis. Newspapers, reports, short communications, and abstracts were considered exclusion criteria and were therefore removed from the study. Ultimately, thirteen relevant articles that met the inclusion criteria remained for review. After reviewing these articles and based on the available sources, the data elements for the registry system were extracted. In the second stage, in order to categorize and classify the extracted data elements, a meeting was held with the participation of subject matter experts and specialists in health information management and medical informatics. The data elements were categorized and organized into a preliminary draft. The first part of the draft was devoted to the information of the respondent, and the second part focused on evaluating the importance of the minimum data set. At the end of the draft, a section was provided so that respondents could add any missing data elements or offer suggestions.
Prior to data extraction, an initial framework of data elements was established, informed by the study objectives and a preliminary review of literature concerning Leishmaniasis registries and Minimum Data Sets (MDS). These predefined domains served as a guide for the extraction process. Throughout the review of eligible studies, the data element list was iteratively refined and expanded to encompass additional relevant variables identified within the included articles. Subsequently, the finalized set of extracted data elements was organized and subjected to expert validation in the following phase of the study.
For the validation of the identified data elements for the comprehensive leishmaniasis registry system, three infectious disease specialists, two epidemiologists, and three health information management experts were invited to review the identified data elements. To validate these elements, each expert was asked to rate the importance of each item using a Likert scale ranging from 1 to 5 (5 = strongly agree, 4 = agree, 3 = neutral, 2 = disagree, 1 = strongly disagree).
To assess quantitative content validity, the Content Validity Ratio (CVR) was applied using the Lawshe method. Based on the experts’ ratings, where each data element was scored from 1 to 5, the CVR for each element was calculated using the following formula: CVR= (ne-N/2)/(N/2) where N represents the total number of experts and ne the number of experts who rated the item as essential. The CVR values calculated for each item ranged between -1 and +1. The closer the value to +1, the higher the validity of the item. A value of 0 indicated that half of the experts considered the item essential, while a value of -1 indicated that none of the experts considered the item essential and it should therefore be eliminated. The minimum acceptable CVR depends on the number of experts. In this study, with eight respondents, a minimum CVR value of 0.75 was considered acceptable. Data elements meeting this threshold were identified as essential elements for inclusion in the system.
Results
The present study was conducted to identify the data elements and develop a minimum dataset for a comprehensive registry system of patients with leishmaniasis. Based on the findings from the first stage of the study, 32 relevant articles on leishmaniasis registries were identified (13 articles from PubMed, 9 articles from Web of Science, and 10 articles from Scopus).
Subsequently, in the first phase, we reviewed 13 related articles. Based on these 13 articles, the relevant data elements for a leishmaniasis registry system were extracted. Using a Likert scale (strongly agree = 5, agree = 4, neutral = 3, disagree = 2, strongly disagree = 1), a preliminary draft of the registry’s data elements was developed. The initial draft included 106 data elements classified into 10 categories: geographic information of the disease registration location (10 elements), patient identification and demographic information (17elements), travel and relocation history (12 elements), residential characteristics (9 elements), past medical history and current medications (14 elements), previous history of leishmaniasis (8 elements), disease-related information (14 elements), laboratory information (5 elements), treatment interventions (11 elements), and follow-up of treatment discontinuation (6 elements).
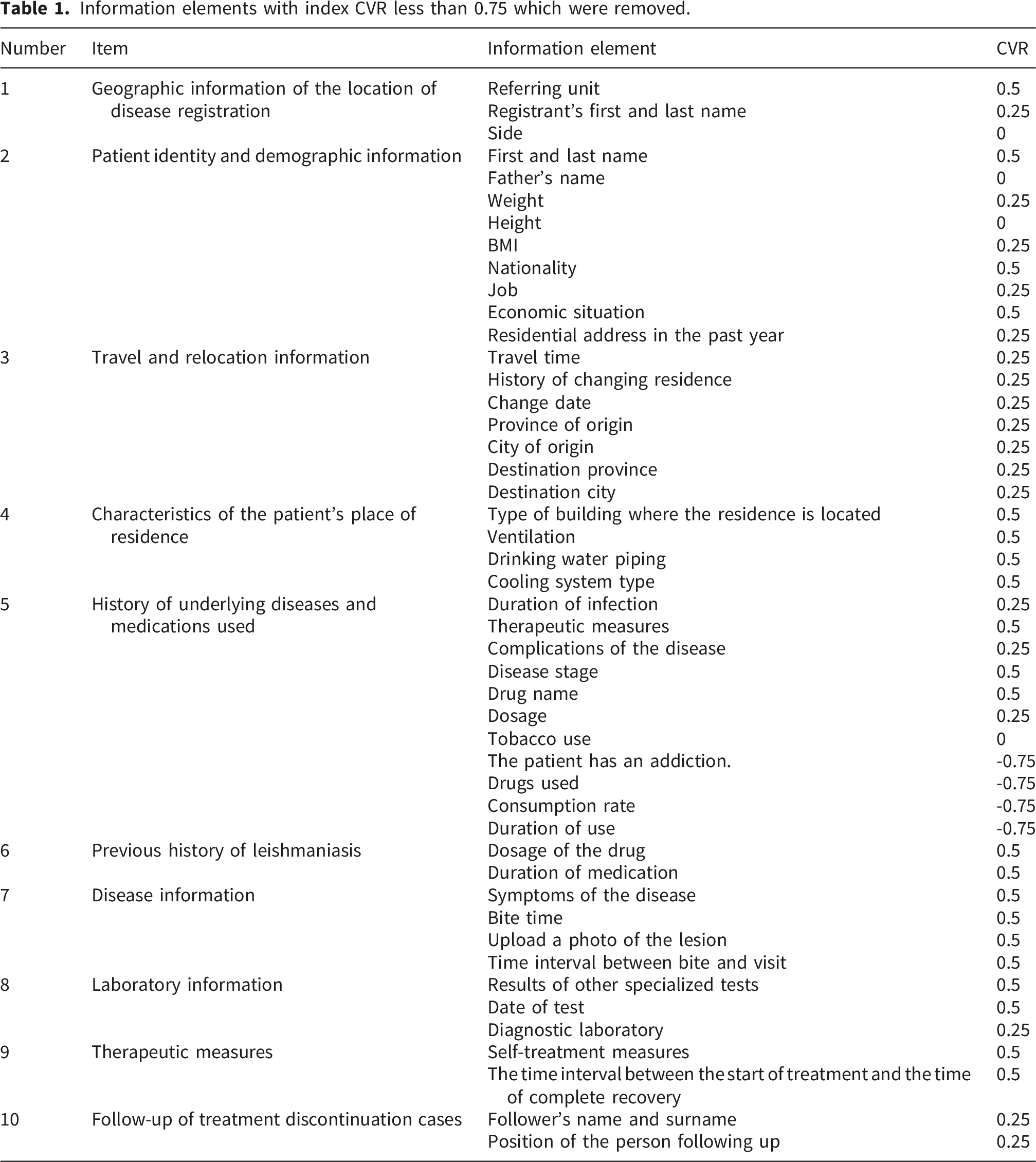
Information elements with index CVR less than 0.75 which were removed.
Final and essential data elements.
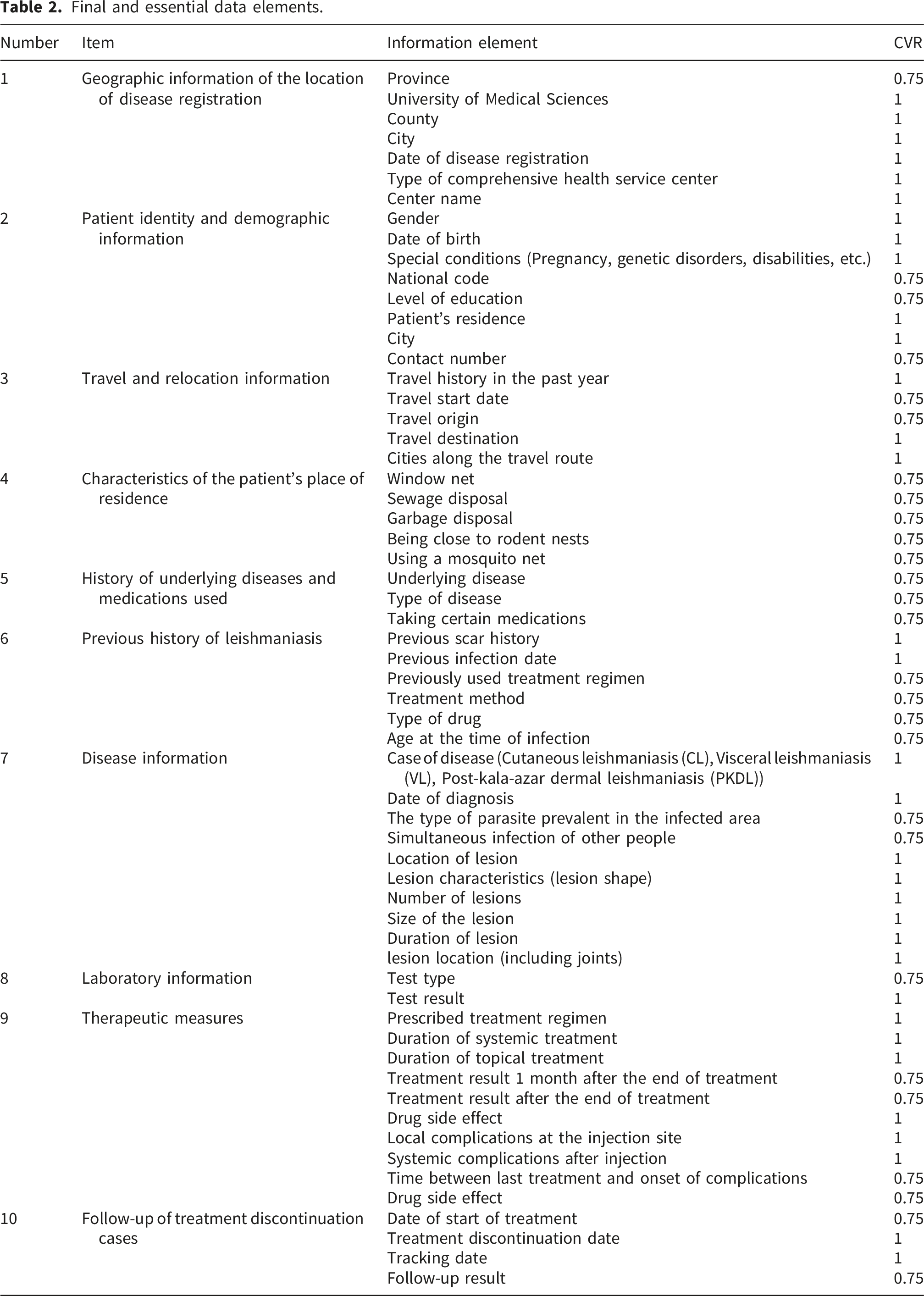
As shown in Table 2, three data elements were confirmed in the domain of geographic information of the disease registration location; nine data elements in the domain of patient identification and demographic information; seven data elements in the domain of travel and relocation history; four data elements in the domain of residential characteristics; eleven data elements in the domain of past medical history and current medications; two data elements in the domain of previous history of leishmaniasis; four data elements in the domain of disease-related information; three data elements in the domain of laboratory information; two data elements in the domain of treatment interventions; and two data elements in the domain of follow-up of treatment discontinuation.
According to the values presented in Table2, the highest frequency percentage (100%) with a CVR index of 1 corresponded to the following data elements: in the domain of geographic information of the disease registration location, six data elements including the name of the university of medical sciences, name of the county and city, date of disease registration, type of comprehensive health service center, and the name of the center; in the domain of patient identification and demographic information, 7 data elements including gender, date of birth, Special conditions of residence, and county name. Three data elements include history of travel within the past year, travel destination, and cities along the travel route, which, which also achieved this score in the domain of travel and relocation history. In the domain of the previous history of leishmaniasis, the data elements included previous scar history and date of previous infection.
In the domain of disease-related information, the data elements with CVR = 1 included case identification, date of diagnosis, lesion site, lesion type, lesion count, lesion size, duration of lesion occurrence, and lesion on joints. The data element “laboratory result” also received CVR = 1 in the laboratory information domain. In the treatment interventions domain, six data elements—prescribed treatment regimen, duration of systemic treatment, duration of topical treatment, drug adverse effects, local injection site complications, and systemic complications after injection—were confirmed. Additionally, in the follow-up of the treatment discontinuation domain, the data elements “date of treatment discontinuation” and “date of follow-up” were confirmed with the highest frequency percentage.
Some data elements were also confirmed with the lowest frequency percentage (87.5%) and a CVR index of 0.75 for inclusion in the comprehensive leishmaniasis registry system, as presented in.
Discussion
The current evidence-base for recommendations on the treatment of leishmaniasis is generally weak, and it has been hampered by inconsistent methodologies used to assess treatment effects.23,24 In the present study, a set of 105 data elements was identified through a systematic literature review, and using the Delphi method and a CVR index ≥ 0.75, a total of 60 data elements were finally recognized as essential for the development of a leishmaniasis registry system. These elements were classified into ten subgroups, including geographic information of the disease registration location, patient identification and demographic information, travel and relocation history, patient residential characteristics, past medical history and current medications, previous history of leishmaniasis, disease-related information, laboratory information, treatment interventions, and follow-up of treatment discontinuation. The method of selecting data elements from developing the initial draft to finalizing the essential information elements in this study was similar to that of many studies that aim to determine data elements for health-related registries.
Pigott et al. designed a database to store cases of leishmaniasis worldwide. Spatial and temporal data were recorded with high accuracy in this database, highlighting the importance of spatio-temporal elements such as date of infection, city, region, and patient residence. The data elements related to this category in the present study were also confirmed with the highest CVR scores. 25
Among the most important data elements identified as determinants of leishmaniasis transmission in the study by Firouzi and colleagues, which analyzed spatio-temporal patterns of cutaneous leishmaniasis during 2011–2020, were patient travel history and precise residence information. These findings are consistent with the present study’s emphasis on travel history, relocation, and residential characteristics. 26
In a study conducted by Khazaei et al. on leishmaniasis parasite species in Iran, it was found that L. major and L. tropica are the most prevalent species. Therefore, recording the species type of each leishmaniasis case is highly essential. In our study as well, parasite type was identified as a critical element for treatment planning and disease management, and it was included in the “disease-related information” category. 27
Ranasinghe et al. developed a tool to assess treatment response and clinical outcomes of leishmaniasis. Key considerations in this tool included lesion site and severity, drug adverse effects, and treatment effectiveness. In the leishmaniasis registry system examined in this study, all elements highlighted in Ranasinghe et al.’s research were also identified as essential data elements, demonstrating that this registry can serve as an infrastructure for treatment evaluation. 28
Certain elements, such as weight, height, tobacco use, economic status, and residential address during the past year, received CVR scores below the acceptable threshold and were eliminated to exclude non-strategic and less valuable data elements from the registry. The elimination of low-priority elements is a common and necessary step in similar studies to ensure that only essential data elements are retained. 29
Localization of data elements in disease registries to the specific needs and geographical conditions of each country aligns with the World Health Organization’s (WHO) recommendations for addressing neglected diseases. WHO emphasizes that the design of each registry system must be tailored to local conditions, disease burden, and analytical capabilities. 30
Limitation
In this study, we performed a rapid search of three databases to identify relevant articles and reviewed only those in English. There may be data published in articles in other languages that we did not have access to.
Conclusion
In this study, we identified the essential data elements required for the development of a comprehensive leishmaniasis patient registration system. Given the high prevalence of leishmaniasis in some regions of the world, the implementation of such a registration system is an undeniable necessity for disease control and disease burden reduction. It is recommended that future research examine the requirements for the development and implementation of leishmaniasis registration systems in areas prone to this disease. It is also recommended that future studies focus on the technical and operational development of the system, using the valid data elements identified in this study, and then evaluate its effectiveness in practice.
Footnotes
Acknowledgements
This study was conducted as part of a research project approved by the School of Medical Sciences of Esfarayen, with ethical approval code IR. ESFARAYENUMS.REC.1400.008. The authors would like to express their sincere gratitude to the Vice-Chancellor for Research of the School of Medical Sciences of Esfarayen and to all individuals who contributed to and supported the research process.
Ethical considerations
Approved by the Ethics Committee of Esfarayen Faculty of Medical Sciences. Ethic code: IR.ESFARAYENUMS.REC.1400.008
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study are available from the corresponding author upon reasonable request.