
Abstract
Purpose
Patient-centered communication (PCC) is essential for quality healthcare. This study examined how PCC was affected by the shift to telehealth and COVID-19 safety measures.
Methods
An online survey was conducted (Sept–Oct 2020) among U.S. adults who had both in-person and telehealth visits after March 2020. PCC was assessed using the Communication Assessment Tool and analyzed with repeated measures ANOVA and multiple regression.
Results
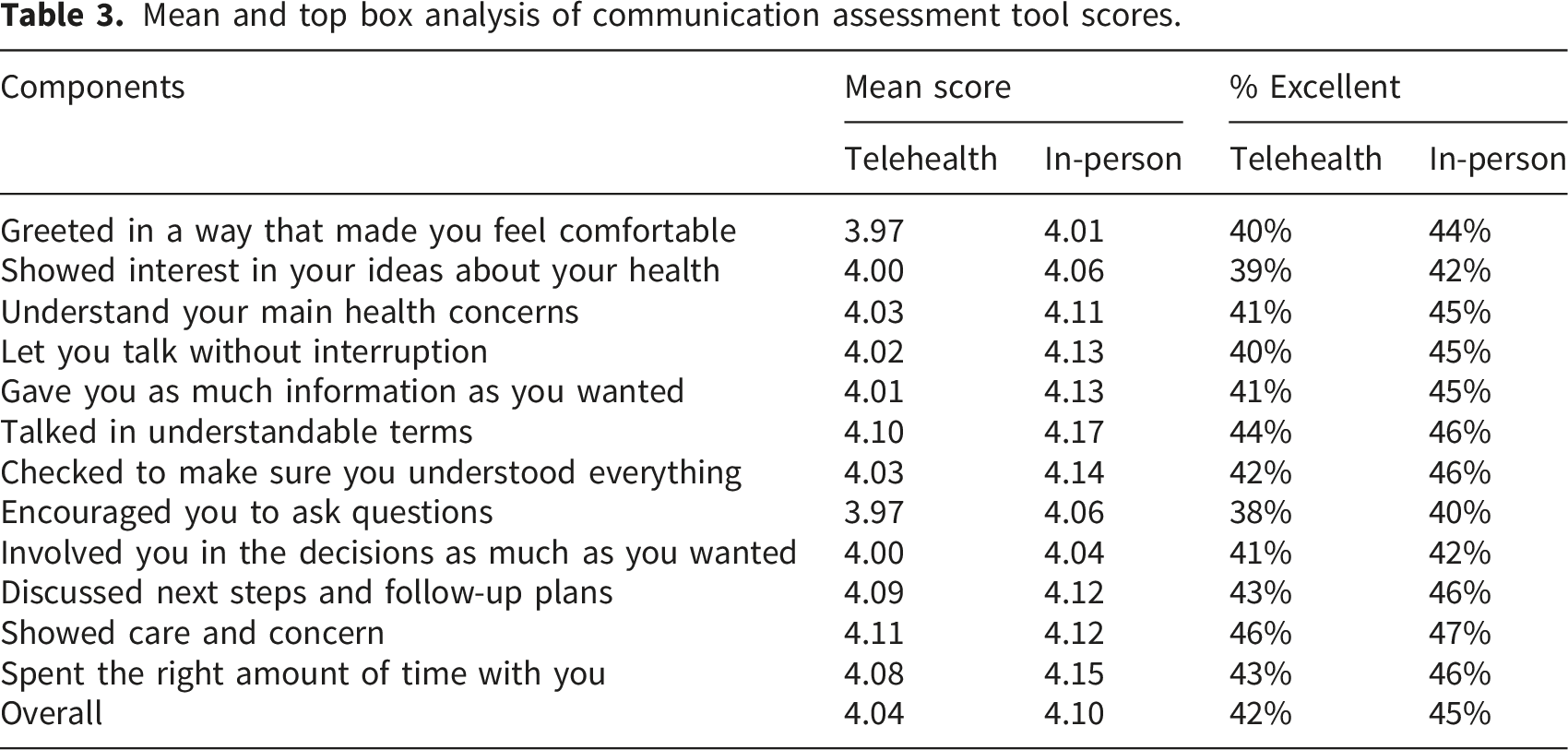
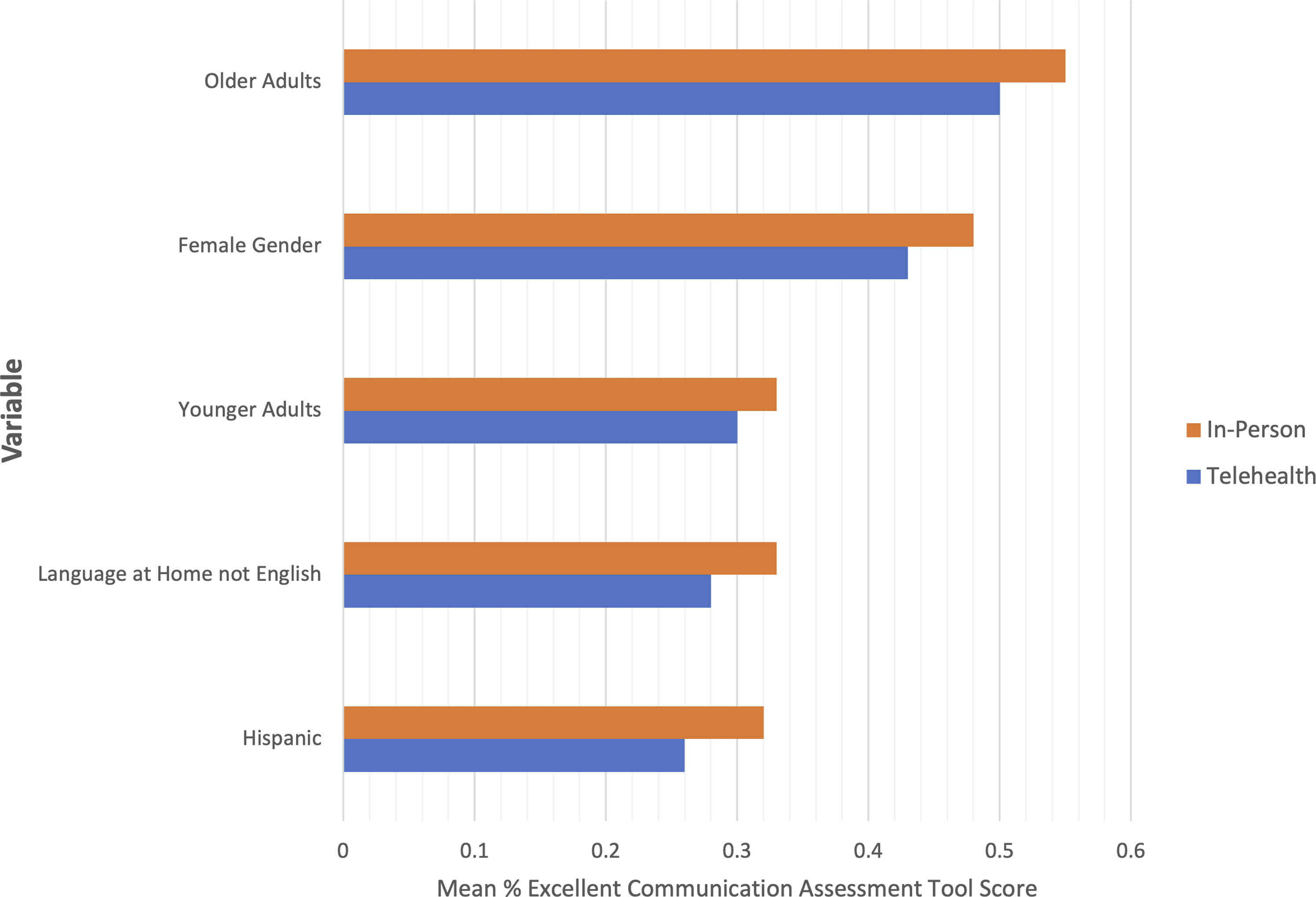
Among 522 respondents (58.2% female; mean age 46.1), PCC scores were higher for in-person visits than telehealth (45% vs. 42%, P = .003). Lower PCC during telehealth was associated with younger age and caregiver presence. For in-person visits, mask use was linked to lower PCC among older adults. More frequent visits (≥3) correlated with higher PCC in both settings.
Conclusions
PCC was generally stronger during in-person visits. Pandemic-related changes may have negatively impacted communication, particularly among certain groups, highlighting areas for future improvement.
Keywords
Introduction
The COVID-19 pandemic changed in-person clinic visits with efforts to reduce COVID-19 risk. Despite public health benefits, concerns exist over Centers for Disease Control and Prevention safety protocols (face masks, visitor restrictions, social distancing, etc.) regarding depersonalization and non-verbal communication, which may impact clinician-patient communication.1–3 For example, face masks obscure the lower two thirds of the face making emotional states unintelligible. 4 Though recent randomized trials have shown benefits to empathy and trust with clear versus cloth masks, cloth masks remain the norm.5,6 The use of masks and social distancing may exacerbate experiences of suboptimal communication, particularly for patients with age-related hearing loss and those with limited English proficiency.3,4,7–10 Additionally, limits on the numbers of care partners allowed into clinic facilities is a significant concern for the 53 million informal caregivers on whom patients rely for their health management. 11
Rapidly switching from in-person visits to telehealth was a disruptive change observed in healthcare. At the peak of the pandemic, telehealth accounted for more than 32% of all visits across the country, leveling out at around 13-17% of visits by late 2021. 12 There are concerns about widespread use of telehealth and its impact on the quality of patient-centered communication (PCC) due to differences in clinician and patient training, and low health or low technology literacy leading to resistance among clinicians and patients.13–17 Technical barriers are also a concern, disproportionately affecting more vulnerable populations such as older adults, rural communities, patients of lower educational attainment and patients from racial and ethnic minority communities.16,18–20 On the other hand, if it can be measured that quality communication is maintained, a shift to telehealth options could exemplify the potential role of digital health in driving the Quadruple Aim. 21 Our goal was to explore if the shift to virtual consultations and the implementation of pandemic safety protocols impacted the quality of patient-centered communication.
Methods
Study and survey design
Between September 2020-October 2020, we conducted an online cross-sectional survey of patients in the United States who have experienced
We developed a 38-item survey, displayed over 40 webpages (1 question per page), that included both validated and newly generated questions, including: a) patient demographics (age, residency, race, ethnicity, education, preferred language, insurance), b) details of in-person and telehealth visits (reason for visit, number of visits, specialty visited, caregiver presence, instructions, summary, overall experience, and patient centered communication (PCC)), c) experiences of in-person clinic visits (safety protocols) and telehealth (technology used for visit, location, privacy, caregiver presence), and d) COVID-19 status. Question response formats included multiple choice or Likert scale, and one open response question about the experience with their healthcare provider (see Appendix B). Patients assessed the quality of PCC during telehealth and in-person visits using 12 questions from the validated Communication Assessment Tool (CAT). 23 The CAT is a 15-item survey designed to specifically assess patient perceptions of an individual physician’s communication effectiveness in a recent visit, unlike other measures in which communication items are bundled with other patient outcomes such as satisfaction and trust, or patients are expected to report experiences over a longer period of time (e.g. in the past 12 months). With a 5-point Likert scale response (poor to excellent), the CAT is scored using Top Box analysis-the mean percentage of item responses marked as excellent. The mean percent-excellent approach mitigates the ceiling effect commonly observed in positively skewed patient-reported means. 23 Effectiveness is defined by the CAT as a physician’s ability to achieve communication tasks associated with patient-centeredness and, as such, we interpret higher CAT scores as higher PCC. Psychometric testing during the development of the CAT found that results are not affected by physician specialty or patient gender, race, level of education, self-reported medical status, or any previous encounters with the physician. Therefore, from participants reporting their communication experiences during both in-person and telehealth visits, we do not expect CAT results to be inherently affected by the differences in modality after removal of more in-person specific items- “staff treated me with respect,” and “paid attention to me (looked at me, listened carefully)”.
The overall survey was informally piloted with clinicians, research staff and patient representatives in our research group to assess interpretability and online usability and technical functionality. In response to pilot feedback, questions were streamlined, reordered to improve flow, or reworded to increase clarity and be more understandable to a general audience. For example, in Q.24 when we asked about equipment needed to participate in telehealth visits, we changed the term ‘devices’ to ‘phones and computers’ based on patient partner feedback.
To protect against order effects, we randomized in-person and telehealth experiences question blocks so that 50% of respondents answered questions on their telehealth experience first, and 50% started with in-person experience items. Outside of screening questions, respondents could review or change their answers if they wished.
Participant eligibility
Eligible individuals were United States residents, ≥18 years, who completed ≥1 (each) telehealth and in-person visit since COVID-19 pandemic restrictions were put in place. We did not specify dates as different States introduced restrictions at different times, however most states had restrictions in place beginning March 2020. Telehealth visits were defined as “a planned telephone or video call with your healthcare provider that prior to the Coronavirus pandemic would have normally been conducted in person”. In-person clinic visits were defined as “a scheduled appointment with your healthcare provider at their office.” Adaptive questioning was used to capture reasons why a respondent had a telehealth or in person visit. Participants who did not select “for my own health issue or condition” for both the telehealth and in-person visits were excluded from analysis.
Recruitment
Participants were recruited using Qualtrics Panels (Qualtrics LLC, Provo, Utah, USA), an online survey platform which draws a broad demographic of participants. The survey was open to panelists who received an invitation email from Qualtrics containing a link to the survey posted online. We planned to recruit 500 patients, and constructed quotas (n=29 per group) 24 to ensure a diverse sample of participants by age (18-34; 35-64; ≥65), educational attainment (no college; ≥college) and race (Asian; Black or African American or Afro-Caribbean, American Indian or Alaskan Native, Native Hawaiian or other Pacific Islander; White), factors known to impact PCC.15,25–27 A sample of 29 respondents per group allowed us to meaningfully describe PCC by varying patient characteristics (e.g., race, ethnicity, age). All potential respondents completed the demographics and eligibility screen initially; potential respondents were removed if they were not eligible or we had already reached the quota for that demographic profile. Responses were automatically captured and Qualtrics performed quality checks based on investigator predetermined criteria for completeness, straight-lining, speeders, duplicates (based on IP address and panelist login) and gibberish/nonsense responses.
Quantitative analysis
We reported means and standard deviations for continuous data, and proportions and ranges for categorical data. We conducted repeated-measures ANOVA to determine whether there was a statistically significant difference between in-person and telehealth PCC by age, sex, race, and ethnicity. We also conducted unadjusted and adjusted linear regression analyses to identify factors associated with PCC in both in-person visits and telehealth visits. Multiple linear regression models included patient demographics, specialty seen, instructions received by the patient from the clinic, and factors specific to in-person visits (e.g., pandemic safety protocols), and telehealth visits (e.g., video or phone visit). Statistical analyses were conducted using R, v1.1.383 (RStudio, Boston, MA). Our target sample of 500 allows for at least 10 observations per parameter in our models to reduce overfitting models. 28 All models were tested for potential collinearity between variables using a variance inflation factor of 5.0. 29 A predefined alpha level of 0.05 or less was chosen for statistical significance. To increase the quality of data from the survey, only fully completed questionnaires were analyzed and responses from individuals who completed the survey in less than one-third of the median completion time, 5.1 minutes, were excluded from the final dataset. 30
Qualitative analysis
We conducted a summative content analysis of responses to the open-ended question to identify salient themes reflecting the respondents’ attitudes towards their healthcare providers during the COVID-19 pandemic. 31 A priori themes for these responses were aimed at distinguishing positive, negative or neutral comments about the participant’s clinician or about visit modality (in-person and telehealth). Each comment was independently reviewed and double-coded by two members of the research team trained in qualitative codebook generation. After initial coding, the coders met to review and adjust a priori themes, with disagreements and theme revisions resolved by the research team.
Consent and ethical considerations
To ensure informed consent, within the guidelines of the protocol, the Qualtrics invitation email was sent only to people who have self-selected to receive surveys. The opening screen presented an “informed consent” text block detailing the purpose of the study, risks, and data handling. The final sentence of the survey introduction read: “If you wish to participate in this project, please click the “>>” button below If you do not wish to participate in this project, please close your Internet browser.” (see Appendix B) The decision to proceed beyond the survey introduction was considered consent to participate.
Within the introduction of the survey, potential participants were informed that “Names and other identifying information will not be collected and therefore not used in any presentation or paper written about this project. You may choose not to answer any or all questions” (see Appendix B). To identify duplicate entries, IP addresses were used but not captured for identification or analysis. Only the first survey entered from a duplicate IP address was retained for quality check and analysis. Data was stored on secure servers.
Respondents receive incentives and cash honorarium from Qualtrics for taking part in surveys (e.g., gift cards). Participants self-selected their incentives based on options provided by Qualtrics.
Results
The participant flow diagram can be found in Figure 1. Of 2786 individuals who started the survey, 1935 completed the survey (Recruitment Rate: 69.5%). Of the 1935 completers, 1413 were removed from the final analytic dataset for the following reasons: low quality responses (n=276), ineligible (n=498) and quota were reached (n=629) (see Appendix C for demographic profile of those excluded due to reaching quota limits). This resulted in an analytic sample of n=522 respondents. Participant flow diagram.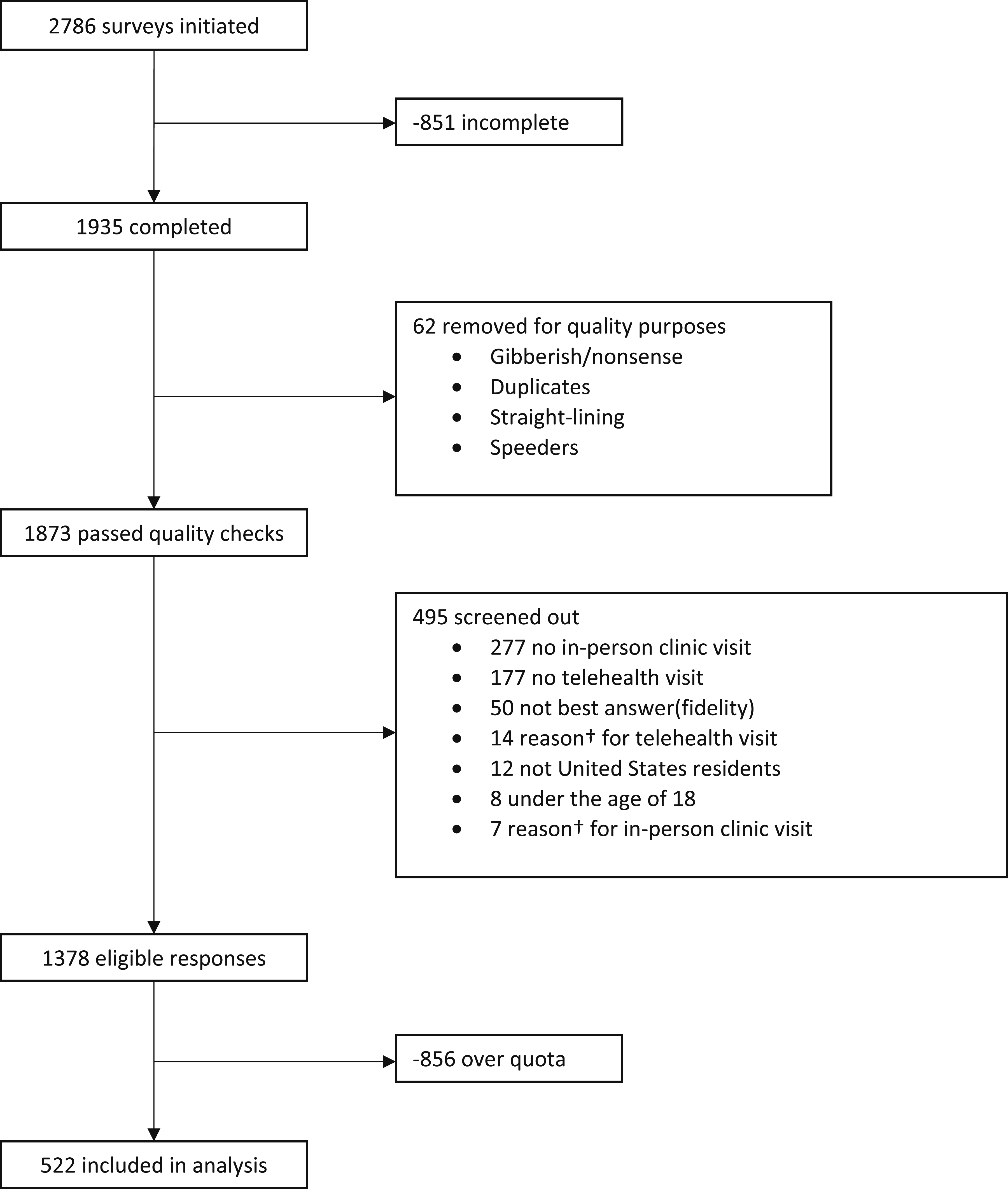
Participant and visit characteristics
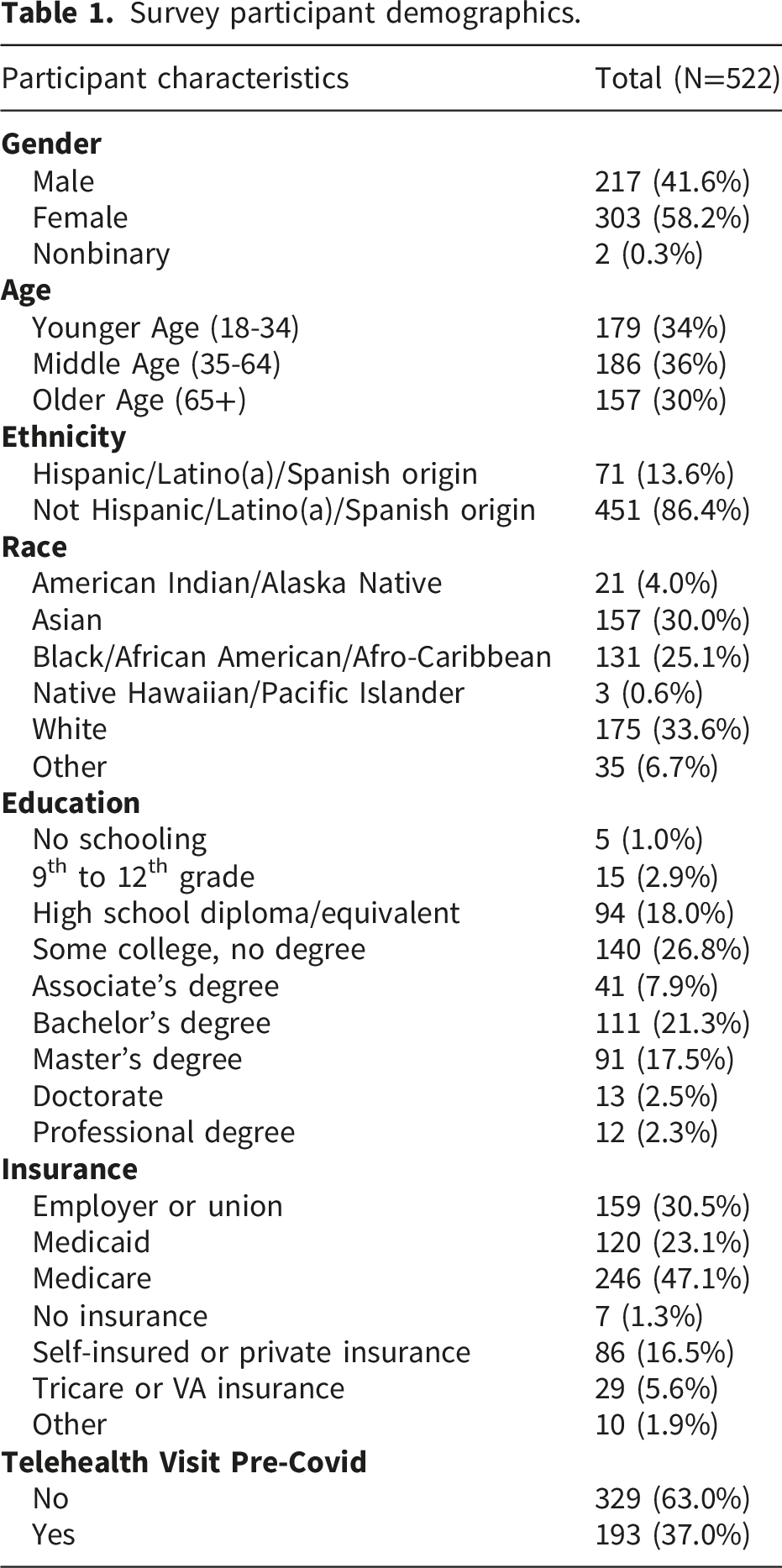
Survey participant demographics.
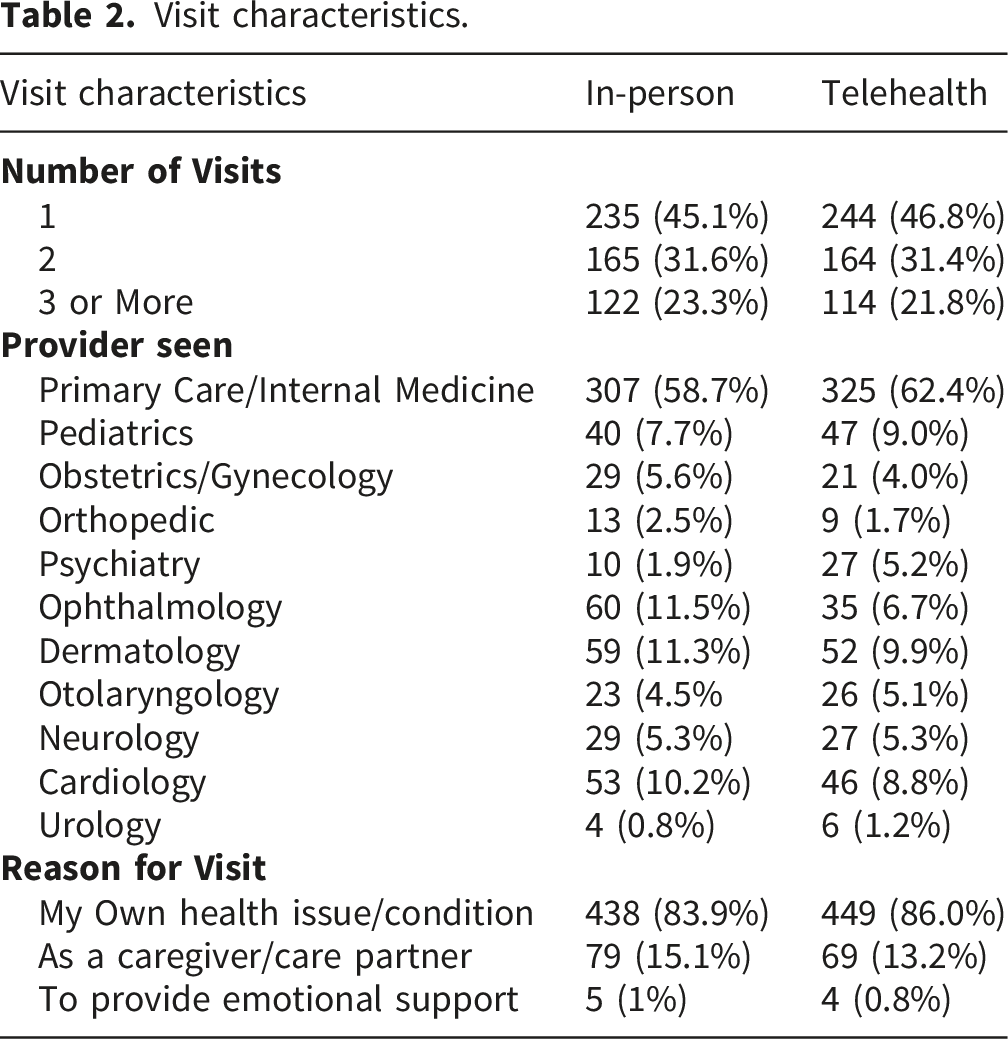
Visit characteristics.
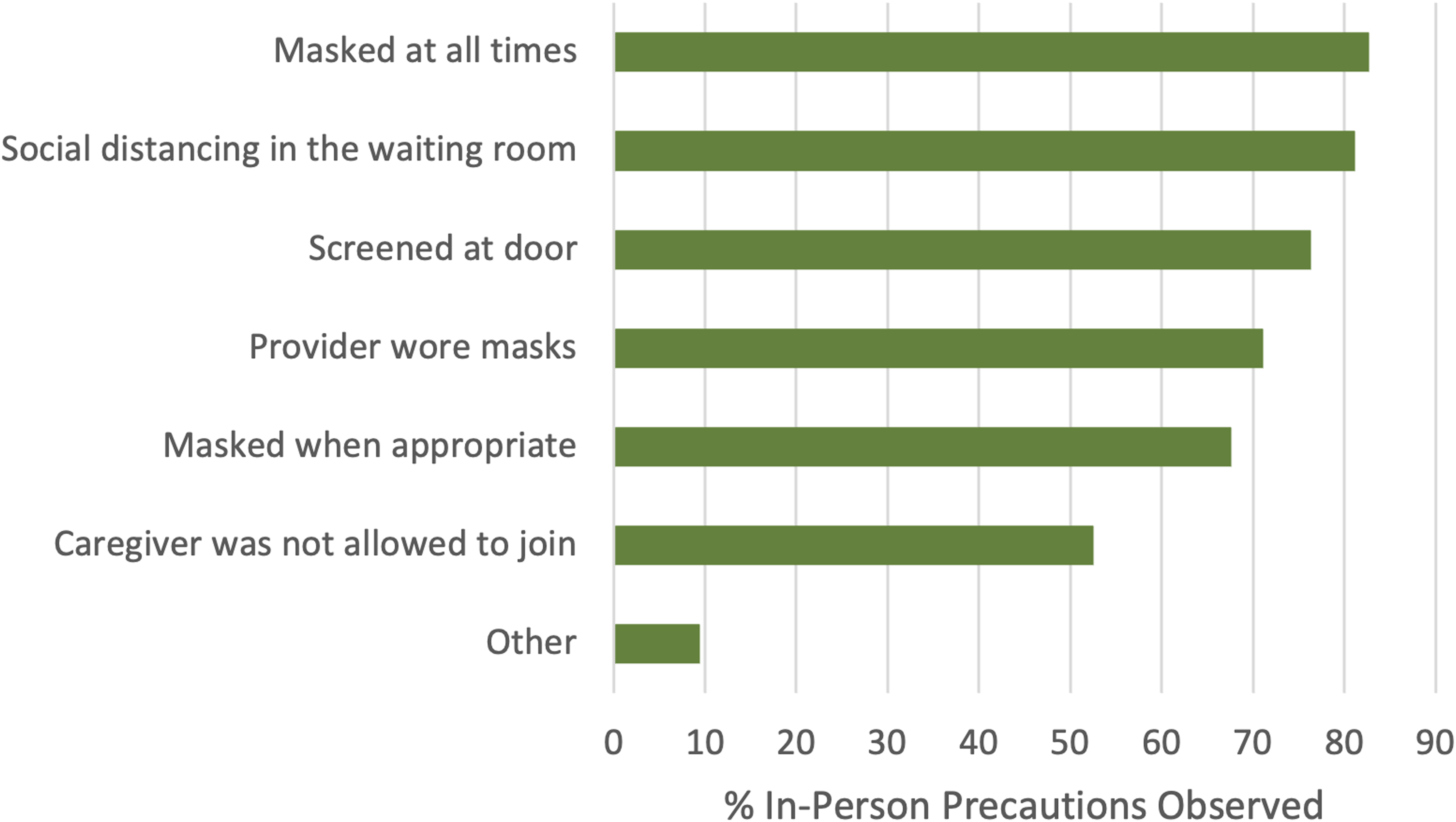
Reported in-person safety precautions.
Quantitative analysis
Patient-centered communication during in-person and telehealth visits
Mean and top box analysis of communication assessment tool scores.
Anova of differences between in-person and telehealth communication assessment tool scores.
Factors associated with in-person visit patient-centered communication
Unadjusted and adjusted linear regression analysis of factors associated with patient centered communication (CAT Scores) in-person clinic visits.
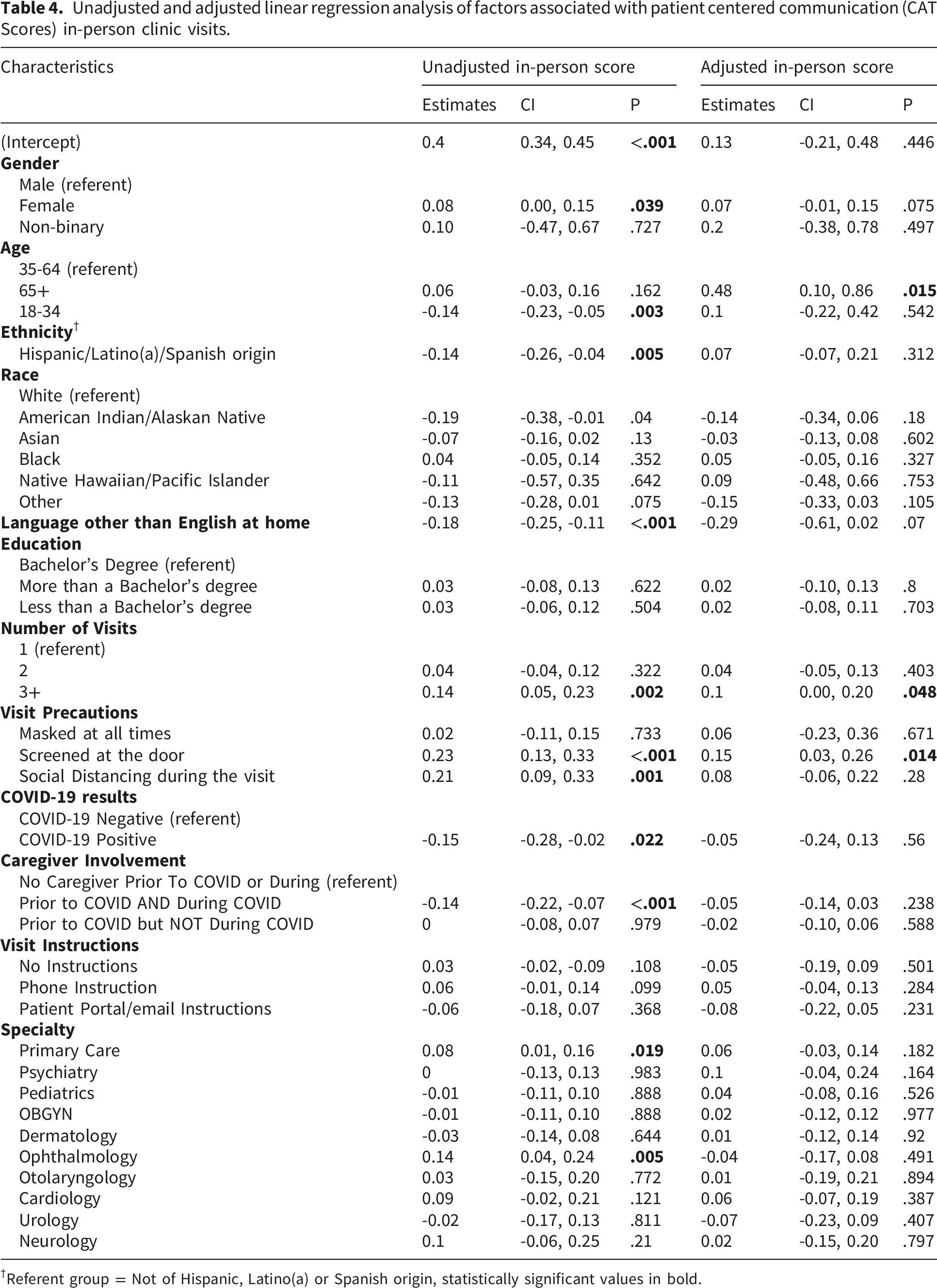
†Referent group = Not of Hispanic, Latino(a) or Spanish origin, statistically significant values in bold.
Factors associated with telehealth visit patient-centered communication
Unadjusted and adjusted linear regression analysis of factors associated with patient centered communication (CAT Scores) of telehealth visits.
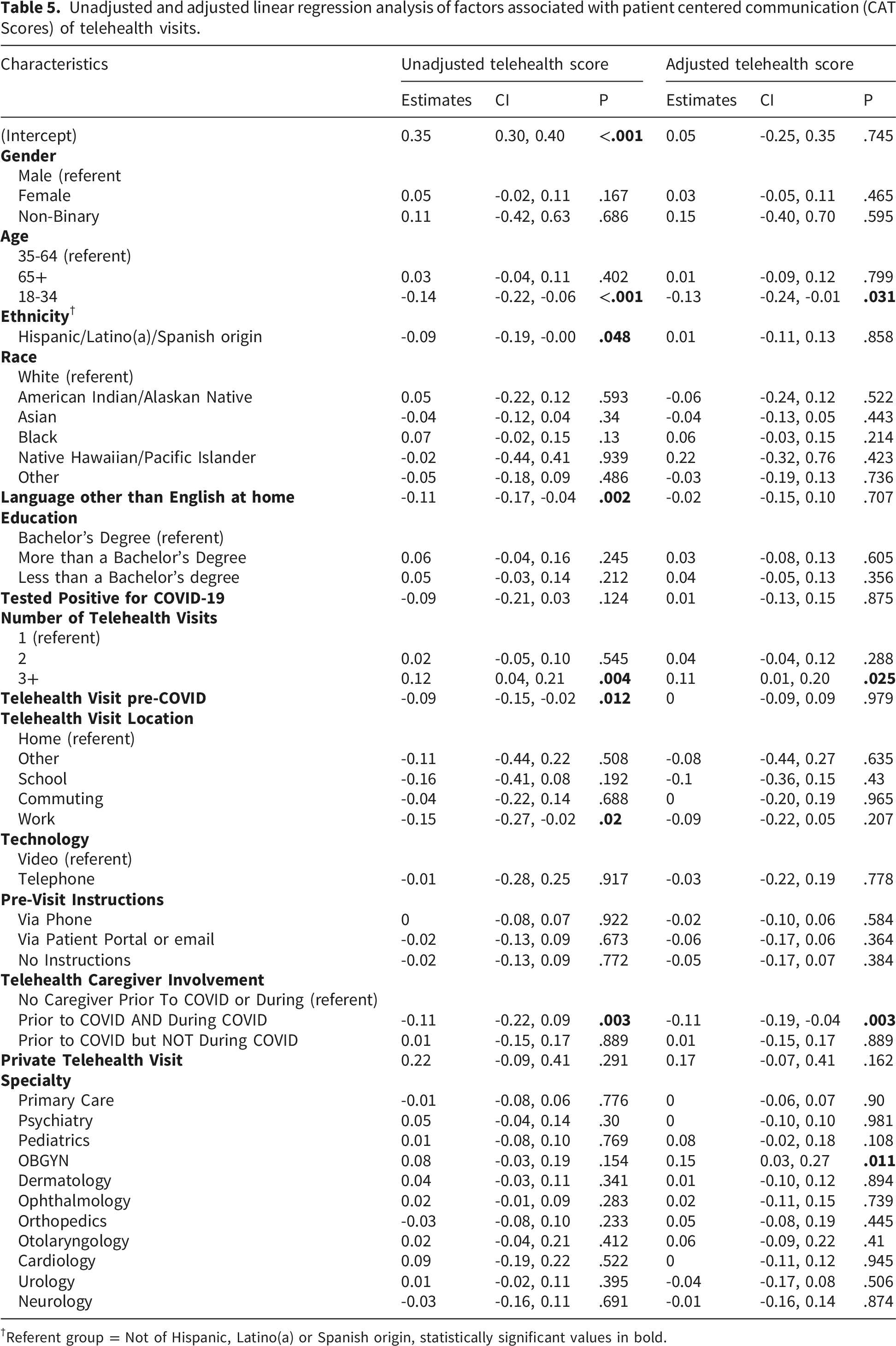
†Referent group = Not of Hispanic, Latino(a) or Spanish origin, statistically significant values in bold.
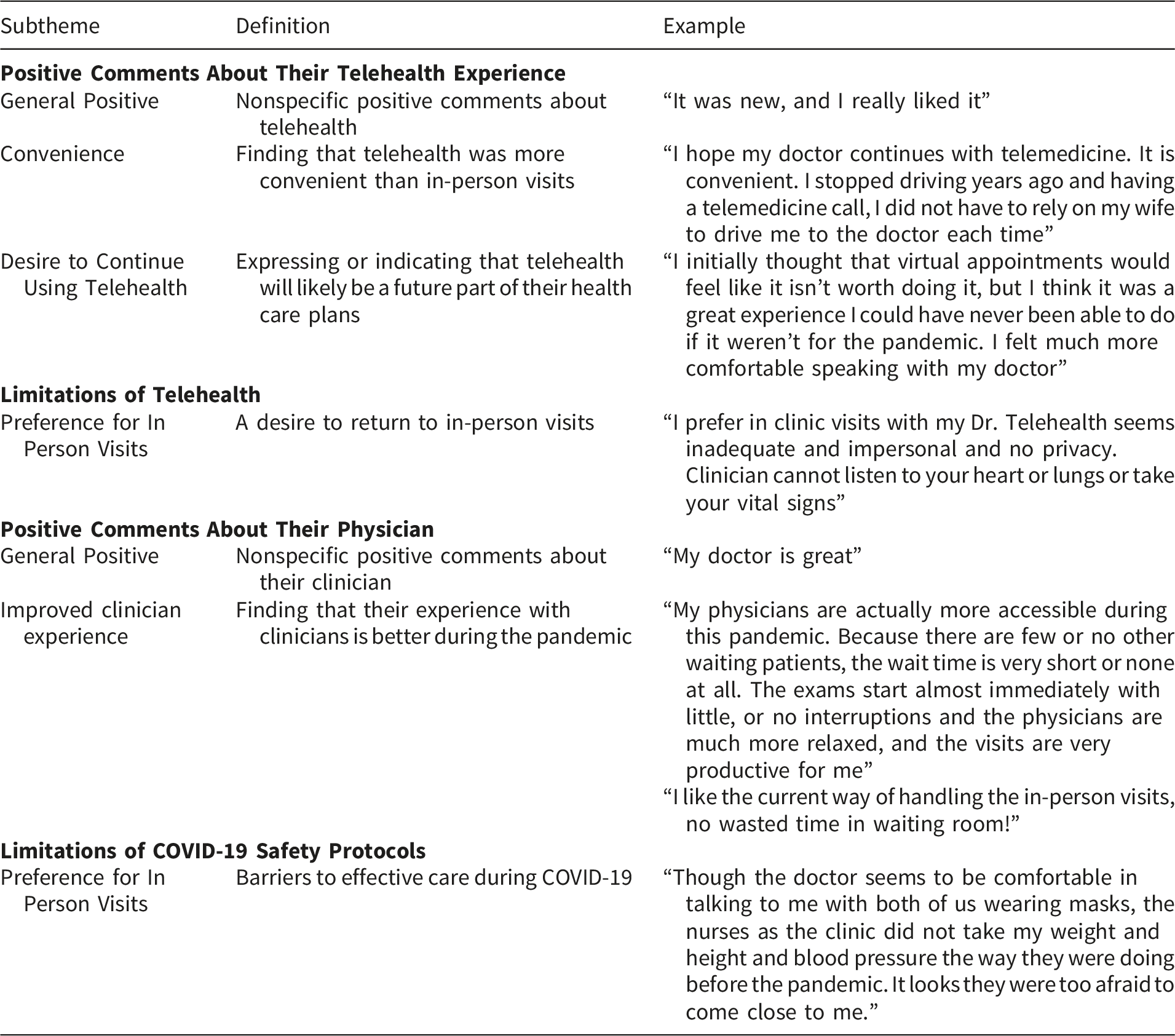
Qualitative analysis
Box 1. Qualitative analysis of patient clinic visit experiences during the pandemic
Discussion
Principal results
In this cross-sectional, online survey of U.S. adult patients conducted in Fall 2020,within-participant experiences of PCC during the COVID-19 pandemic were moderately but consistently lower for telehealth visits compared to in-person visits. PCC in telehealth compared to in-person visits was significantly lower for respondents from the youngest and oldest age groups, females, those who identify as Hispanic and those who speak a language other than English at home. Experiences of more clinic visits, regardless of visit modality (telehealth or in-person) was associated with improved PCC. Lower PCC during telehealth visits was reported by respondents aged <35 years and those who stated that, prior to and during the pandemic, a caregiver attended their visit.
Limitations
Two core items of the CAT were not included in the survey: “staff treated me with respect,” “paid attention to me (looked at me, listened carefully).” However, Top Box CAT analysis would unlikely be affected by their omission, especially given the high internal consistency between items. 23 Communication quality may be confounded by familiarity with one’s clinician or disease burden, two factors we did not explore directly in this study.32–34 However, we did capture number of clinic visits, which may indicate patients with greater familiarity and indeed, this variable was observed to be related to higher PCC. Our online survey is a convenience sample of self-selected participants who may be more comfortable with technology. This may alter the effect that the “digital divide” has on older and/or remote populations. Therefore, the perceived gap in PCC between in-person and telehealth visits may be larger than reported.13,34 Although whole online survey panels carry some selection bias, they have been found to produce reliable findings and can act as a good starting point for further research.35–37
Comparison with prior work
Research to date suggests that PCC during telehealth is similar to in-person visits.38–40 Yet in our analysis, where respondents experienced both telehealth and in-person visits, serving as their own controls, we found that PCC during telehealth visits was rated lower across various demographic groups. A prior systematic review found that patients were overall satisfied with telehealth, though similar to our findings, reported a preference for in-person visits. 1 Interestingly, the CAT item “let you talk without interruption” received a higher percentage excellent rating during in-person clinic visits (45%) than in telehealth visits (40%), contrary to the finding by Agha and colleagues that patients perceive clinicians to be more attentive and less likely to interrupt during telehealth encounters. 40 The patient experience reported by Agha and colleagues 40 may have been more streamlined as the video telehealth visits were conducted in a clinic facilitated by a nurse, compared to the experience of telehealth during the COVID-19 pandemic which is typically conducted independently by the patient at home. Similar to a recent systematic review, we did not find any differences in PCC when telehealth visits were conducted by phone or video. 41
While younger adult patients may be more accustomed to technology, with higher overall telehealth visit completion rates, 42 those in this study reported lower levels of telehealth visit PCC compared to older adults, similar to prior research. 43 Older adults are likely to have longer more trusting relationships with their clinicians. The association between visit frequency and higher PCC may reflect an ‘existing’ clinician-patient relationship, known to create a stronger therapeutic alliance.33,34 Additionally, as younger adults are more experienced with technology they may have expectations about the capabilities of telehealth. Yet with the pace and scale of telehealth roll out technical challenges were common 44 which may have impacted younger adults’ perceptions of telehealth visit quality. Challenges related to privacy and security (crowded homes, taking calls at work and discomfort with conducting sensitive exams may impact PCC) may differentially impact vulnerable populations.39,45–47
Participants in this study who had a caregiver join telehealth visits reported decreased PCC. Despite the opportunity to enable engagement of caregivers via telehealth, 19 the presence of a caregiver at telehealth visits can result in greater technical complications and unintended interruptions (e.g. arranging three people to join a telehealth visit) and security and privacy concerns (e.g. shared passwords, discussion of sensitive patient issues when a caregiver may normally be in a separate waiting area). 47 Common tips for cybersecurity in healthcare, such as recommendations for users to have strong passwords that are changed regularly and limiting network and physical access to user devices, are increasingly difficult with the addition of one or more caregivers. For example, patients often share passwords to their accounts with loved ones or share their devices with family members. Per Jayousi and colleagues, concerns about device comfort, data privacy and digital literacy create human-centered and ethical obstacles for telemedicine integration. 48 The rigidity of regulatory solutions and the need to accommodate dynamic care partner networks and shifts in health status creates ample opportunity to incorporate stakeholder preferences in standardization recommendations.
Our research supports prior work regarding language differences: individuals with limited English proficiency and those who identify as Hispanic experience lower CAT scores for telehealth and in-person clinic visits.33,49,50 This could be secondary to the slower uptake of telehealth in the Hispanic community, 43 lack of captioning and interpreter services,51,52 or the requirement of a working patient portal for scheduling purposes. From a system perspective, it’s important to consider evidence-based communication protocols to aid providers and removing barriers to telehealth for this population such as: 1) the requirement for a patient portal13,53 and 2) lack of multilingual support, a key equity consideration in addressing access issues and the digital divide. 54 At the time of data collection, siloed digital infrastructures limited flexibility of communication protocols resulting in a dearth of solutions to unforeseen challenges, such as the lack of captioning and translator services. 54 The normalization of telehealth delivery should prompt more up-to-date examination of language support services, paying special attention to involvement of vulnerable populations in designing flexible, scalable solutions to care delivery disparities. 55
Our stratified analysis of observed mask use and CAT score, by age, revealed that mask use was associated with lower CAT score in older adults. This finding lends support to concerns that mask use could result in greater communication challenges in older adults due to the higher prevalence of age-related vision, hearing and memory loss.3,8,10,56 The presence of screening at the entry of the clinic was associated with higher perceived PCC. While the mechanisms by which this may impact PCC are unclear, it may be related to what Scheid describes as the “psychological need for competence” in which comfort can be provided by a consistent message that gives the impression that clinicians are “effective, capable and have mastery over our circumstances”—in this case management of COVID-19 pandemic risks. 57
In our study, each item on the CAT was rated lower for telehealth visits. In theory, some of the communication issues may be mitigated by teaching clinicians to treat communication skills as clinical skills. Social cues of when to talk and listen are more difficult to identify over telephone and video, and disruptions by others present in the patient’s space offer less opportunity for patients to speak privately with their clinician. 40 A potential factor accounting for the lower reported quality of PCC experienced in telehealth may be the absence of non-verbal cues, essential to building rapport and trust during clinic visits. 58 It would be useful to study the outcomes of some of the following interventions on PCC: 1) incentivizing clinicians to learn and more frequently use verbal cues that convey warmth and support; 2) clinician training in the teach back method to demonstrate engagement; 3) teaching doctors to use empathetic body language that remains visible on the screen or at a distance. 59 This includes maintaining eye contact, using gestures and open posture; or 4) patient education about the necessity of safety measures with reassurance that providers are still thinking about their needs and emotions. Feinberg and colleagues report that resident physicians believe they are already using the teach back method but increase their actual use of it after training. Extension of this research into the perception of patients is ongoing.59,60
Conclusions
Within broader health informatics frameworks, our research contributes to the evaluation of telemedicine communication quality, a critical step in technological assessment aimed at standardization of telehealth delivery. 48 Following the pandemic, telehealth services have become more prominent, yet lessons learned from the pandemic must be applied. Telehealth can help reduce barriers to care, but caution must be taken in how we address disparities in PCC experienced in telehealth. Of immediate concern is supporting visit communication both in-person and via telehealth for patients with limited English proficiency, young adults, and those who benefit from the presence of a caregiver. Translation services and on-screen captioning of visit communication can help reduce observe disparities in quality of communication experienced by patients with limited English proficiency and with hearing difficulties, including those with mild age related hearing loss.51,52 This need is pressing: approximately 20% of US adult population speak a language other than English, half of whom report limited English proficiency. 61 The availability or translator services in telehealth settings is critical to meet needs of these patients. While mask use is an effective protective tool in clinic, it can impair PCC in older adults; new strategies are emerging where transparent masks allow the clinicians face to be seen which may mitigate the impact of masks on PCC. 4 Low levels of perceived PCC have significant implications and inadequate communication can impede self-management of care. These challenges result in longer-term negative health outcomes. This disruption of care delivery and impact on PCC points to the need for more careful co-design of care delivery processes to reduce disparities experienced by these populations.
Supplemental material
Supplemental material - The impact of telehealth on patient-centered communication during the COVID-19 pandemic
Supplemental material for The impact of telehealth on patient-centered communication during the COVID-19 pandemic by W. Moraa Onsando, Paul J. Barr, Reed W. Bratches, Kerri L. Cavanaugh, Jesse A. Schoonmaker, Noah Freundlich, Yasir Salih, Gregory Makoul, and Meredith C. Masel in Health Informatics Journal.
Supplemental material
Supplemental material - The impact of telehealth on patient-centered communication during the COVID-19 pandemic
Supplemental material for The impact of telehealth on patient-centered communication during the COVID-19 pandemic by W. Moraa Onsando, Paul J. Barr, Reed W. Bratches, Kerri L. Cavanaugh, Jesse A. Schoonmaker, Noah Freundlich, Yasir Salih, Gregory Makoul, and Meredith C. Masel in Health Informatics Journal.
Supplemental material
Supplemental material - The impact of telehealth on patient-centered communication during the COVID-19 pandemic
Supplemental material for The impact of telehealth on patient-centered communication during the COVID-19 pandemic by W. Moraa Onsando, Paul J. Barr, Reed W. Bratches, Kerri L. Cavanaugh, Jesse A. Schoonmaker, Noah Freundlich, Yasir Salih, Gregory Makoul, and Meredith C. Masel in Health Informatics Journal.
Footnotes
Acknowledgements
We would like to acknowledge the review and piloting of our survey by: Linda Wilkinson and the Patient and Family Advisors of Dartmouth-Hitchcock, our patient partners, Sheri Piper and Roger Arend, and all the members of our Open Recordings team-particularly Drs. Renata West Yen and Alejandra Martinez-Pereira.
Ethical considerations
This research was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and the protocol information that follows was deemed exempt from further review by the Trustees of Dartmouth College Committee for the Protection of Human Subjects on June 29, 2020 (CPHS# STUDY00032099) and the University of Texas Medical Branch Institutional Review Board on August 18, 2020 (IRB#20-0206). The requirement for written consent was waived.
Consent to participate
Our survey was distributed online from September to October 2020 through Qualtrics. To ensure informed consent, within the guidelines of the protocol, the Qualtrics invitation email was sent only to people who have self-selected to receive surveys. The opening screen presented an “informed consent” text block detailing the purpose of the study, risks, and data handling. The final sentence of the survey introduction read: “If you wish to participate in this project, please click the “>>” button below If you do not wish to participate in this project, please close your Internet browser.” (see ![]() ) The decision to proceed beyond the survey introduction was considered consent to participate.
) The decision to proceed beyond the survey introduction was considered consent to participate.
Author contributions
Authorship CRediT statement has been included as a supplement.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by Oliver Center for Patient Safety and Quality Healthcare at The University of Texas Medical Branch (grant #OC200206).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.