
Abstract
Objectives
Patient scheduling is a vital yet complex task that strongly influences patient satisfaction and optimizes healthcare efficiency. Recent studies have emphasized the importance of devising innovative approaches and developing new scheduling frameworks. Therefore, this study establishes a dedicated generative artificial intelligence (GenAI) system for patient scheduling.
Methods
The proposed system first imports scheduling data to formulate the default patient scheduling problem. Subsequently, users enter their scheduling requirements using natural language via the system interface, which are parsed using a deep neural network to establish the corresponding extended three-field notations. A customized genetic algorithm is automatically generated to solve the customized patient scheduling problem.
Results
The dedicated GenAI system was applied to a real-world case obtained from the literature, involving 12 anesthesiologists, surgeons, and anesthesia resuscitation doctors; 12 operating rooms; and 15 patients undergoing three types of surgeries, each consisting of three operations. The experimental results reveal that the difference in the optimal fitness achieved using this system and branch-and-bound was less than 1% on average, demonstrating that the proposed methodology is effective. In addition, the most complex customized patient scheduling problem could be automatically modeled and solved in 20 s. Furthermore, the scheduling performance achieved using this system was significantly higher (α = 0.05) than those achieved using two current practices. Moreover, customized patient scheduling problems are often substantially more complex than problems addressed using traditional methods reported in previous studies.
Conclusions
Applying this dedicated GenAI system improved the effectiveness of patient scheduling. This is expected to considerably enhance patient satisfaction and overall healthcare efficiency.
1. Introduction
In hospital outpatient settings, patient scheduling is a particularly prominent issue; moreover, effective scheduling systems can significantly impact patient satisfaction and overall healthcare efficiency. Recent comprehensive reviews have highlighted the complexity of patient scheduling in hospitals and indicated that innovative solutions and new scheduling models are necessary to address this.1,2 However, reviewing recent literature reveals that the use of general-purpose generative artificial intelligence (GenAI) is unsuitable for handling the diverse scheduling requirements of medical professionals.
GenAI learns underlying patterns and structures present in old data to generate new data that fulfills users’ requirements present in natural-language prompts.3–5 GenAI is typically based on transformer-based deep neural networks, 6 especially large language models (LLMs) (Radford et al., 2019; Goyal et al., 2024; Wang et al., 2025).4,7,8 Moreover, GenAI enables users unfamiliar with machine learning or deep learning to leverage these advanced artificial intelligence technologies and has achieved widespread and effective application results.9–11
Furthermore, GenAI has been widely used in hospitals and clinics for clinical administration (including healthcare-associated infection surveillance and clinical text structuring),12,13 decision support, 12 care process improvement and planning,14,15 workflow automation, 12 and other functions. GenAI systems can automatically populate available time slots for healthcare professionals. However, patients may compete for limited or even single medical resources, such as doctors, nurses, and robots, in the same time period.16,17 Therefore, applying GenAI in patient scheduling, which must be optimized overall, remains rare, mainly owing to the poor capabilities of existing GenAI systems in formulating and/or solving complex optimization problems, 18 such as those in the field of patient scheduling. 19
Another issue pertains to the inference result obtained using a GenAI system, which may be incorrect, rendering it difficult to verify owing to the complex reasoning mechanism underlying the GenAI system. 10 This issue becomes critical if the scheduling plan generated by a GenAI system is infeasible and not optimal. This study aims to address these research gaps by establishing a dedicated GenAI system for patient scheduling in hospitals or clinics. In the literature, most patient scheduling problems in hospitals or clinics have been formulated as job shop or flexible job shop problems.20–24 Therefore, the proposed system aims to solve such scheduling problems.
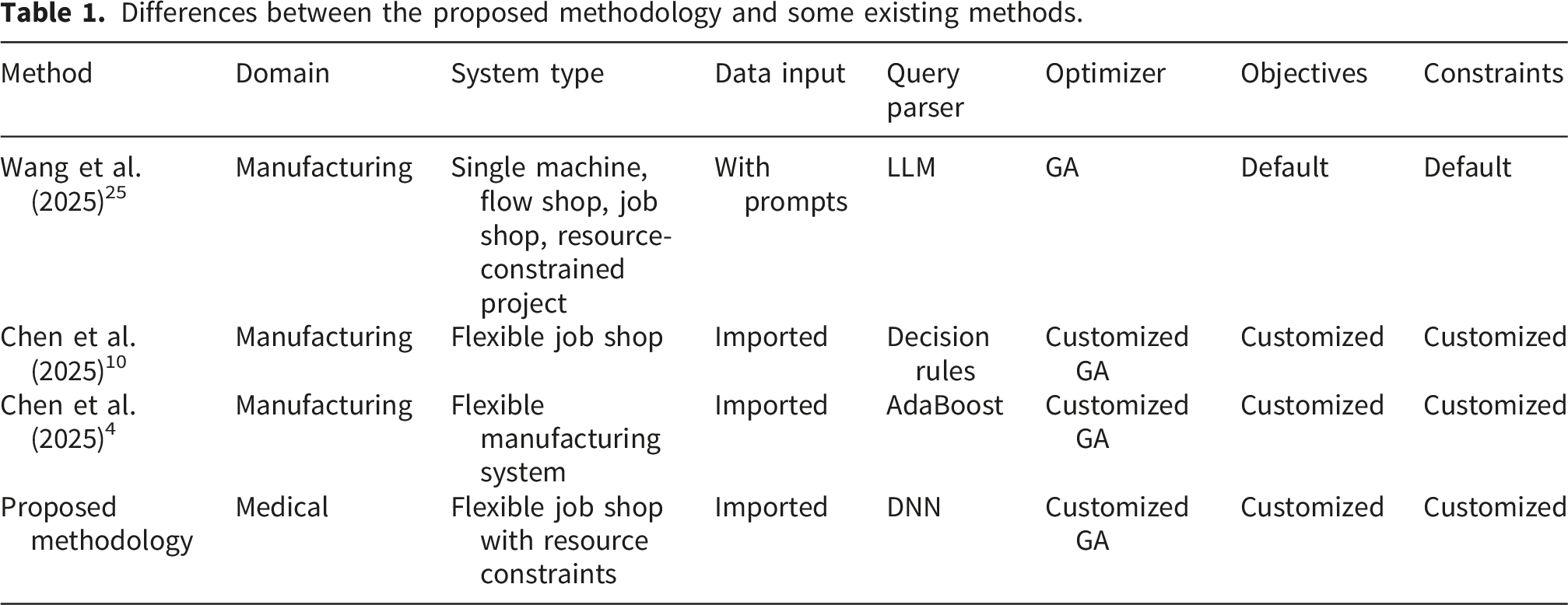
In the dedicated GenAI system, the scheduling data are imported, rather than being entered with prompts. Subsequently, planners enter their scheduling requirements in natural language via the system interface. Next, a deep neural network (DNN) is constructed and trained to extract the information regarding keywords to establish an extended three-field representation (ETFN) for the scheduling problem. 10 The high similarity of user backgrounds and the uniformity of system functions ensure that constructing a DNN can more conveniently and efficiently parse users’ natural-language queries than constructing an LLM. 10 Based on the ETFN, the corresponding optimization model is formulated and solved using a customized genetic algorithm (GA), automatically generated by modifying the default GA program. Thus, the dedicated GenAI system is flexible and can handle highly complex or special objectives or constraints, such as optimizing a special function of cycle times, thereby restricting the processing of patients in a specific operating or testing room. In contrast, Wang et al. (2025) constructed multi-agent LLMs that combined GAs with various scheduling heuristics for similar purposes. 25 However, both the description and data related to the scheduling problem needed to be provided with prompts. In addition, as the GAs had not been customized, only default scheduling objective functions could be optimized. In addition, Chen et al. (2025) established decision rules to parse users’ scheduling requirements, 10 whereas this study constructs a DNN parser. Furthermore, distinct from the problems solved in previous studies, dedicated resources (examination room or doctor) are required when performing surgery on patients, yielding flexible job shop scheduling problems under resource constraints.
Differences between the proposed methodology and some existing methods.
The remainder of this paper is organized as follows. The relevant literature is reviewed in Section 2, and the architecture and implementation procedure of the dedicated GenAI system are presented in Section 3. The effectiveness of the dedicated GenAI system is evaluated by applying it to a real-world day surgery case obtained from the literature in Section 4. Section 5 discusses the experimental results. Finally, Section 6 concludes this study and suggests some topics that can be investigated in the future.
2. Literature review
Relevant references on modeling and solving flexible job shop scheduling problems in hospitals or clinics are reviewed as follows.
Zhao et al. (2013) investigated a patient scheduling problem for a clinic. 20 Patients were assigned unequal priorities, and subsequently, the scheduling objective was to minimize the weighted sum of completion times of all patients. A mixed integer-linear programming (MILP) problem was formulated, which was non-deterministic polynomial-time (NP)-hard. However, the authors applied the existing optimization software, Cplex, to derive the (local) optimal solution, rather than applying a bio-inspired algorithm to determine the global optimal solution.
Xiang et al. (2015) solved an operating room surgery scheduling problem, which required determining the start time of existing surgeries and allocating necessary resources to the scheduled surgeries. 21 Considering resource availability and the expertise and qualifications of human resources, the authors constructed a flexible job shop scheduling problem with multiple resource constraints, characterized by a mixed integer-nonlinear programming (MINLP) model, the objective function of which minimizes the makespan. An ant colony algorithm was proposed to solve this operating room surgery scheduling problem.
Abderrabi et al. (2021) formulated an MILP model to schedule the functions related to meal preparation in hospital catering to enable collective catering. 22 This was an NP-hard flexible job shop scheduling problem, aiming to minimize the sum of the completion times of all preparations. The authors applied a GA enhanced by iterated local search to identify the optimal solution. 26
To reduce wait times for patients at a counter, Sarfaraj et al. (2021) treated patients as jobs and counters as machines, subsequently formulating and solving an MILP problem, which was an NP-hard flexible job shop scheduling problem. 23 The proposed methodology shortened the total completion time (i.e., makespan) by 13% relative to the current method of manual scheduling.
Lingkon et al. (2025) solved a multi-objective flexible job shop problem with resource-limited constraints in hospitals, in which three objectives were optimized. 24 These included minimizing the makespan, minimizing the maximum machine workload, and maximizing the sum of the machine workloads. 25 Owing to limited resources, certain patients could only be examined in certain testing rooms and not in all the testing rooms. The multi-objective flexible job shop problem was an MINLP problem, and the weighted sum of the three objectives was optimized instead, for which a hybrid discrete firefly algorithm was proposed. In addition, sensitivity analysis was conducted to ensure that the weights of the objective functions were appropriate.
Several scheduling problems in hospitals and clinics were modeled as job shop scheduling problems, such as day surgery scheduling, 27 green patient flow optimization, 28 and operating room scheduling, 29 which represent a special case of flexible job shop scheduling problems. Therefore, the methods proposed in the reviewed references are also applicable.
3. Methodology
The dedicated GenAI system is composed of five main parts (refer to Figure 1), namely, the system interface, DNN, optimization model formulator, GA, and system database. Main parts of the dedicated GenAI system.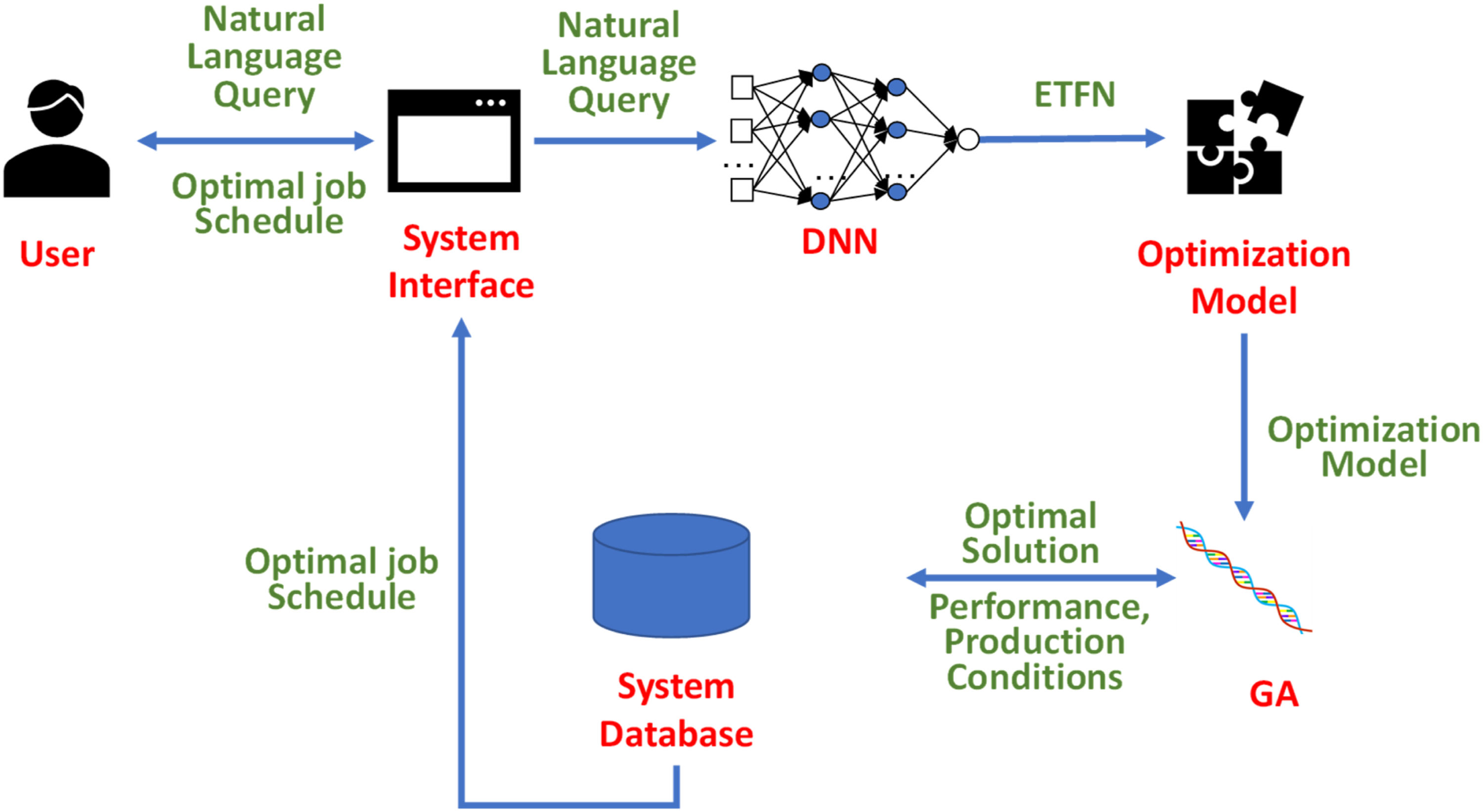
3.1. Generating the default patient scheduling model
Based on the imported scheduling data, the default patient scheduling model is automatically generated as a flow shop scheduling model with resource constraints, as provided in the Appendix.
The default patient scheduling problem is an MINLP problem, with an ETFN of
3.2. Parsing user queries
The dedicated GenAI system permits users to enter queries in natural language. Subsequently, information regarding possible keywords is extracted from each query, including the number of keywords and their relative positions. 10
To facilitate the extraction process, users are instructed to divide their queries into segments using semicolons.
31
Subsequently, each segment is preprocessed using lowercase conversion, stemming and lemmatisation, and entity linking (refer to Figure 2). Preprocessing of segments.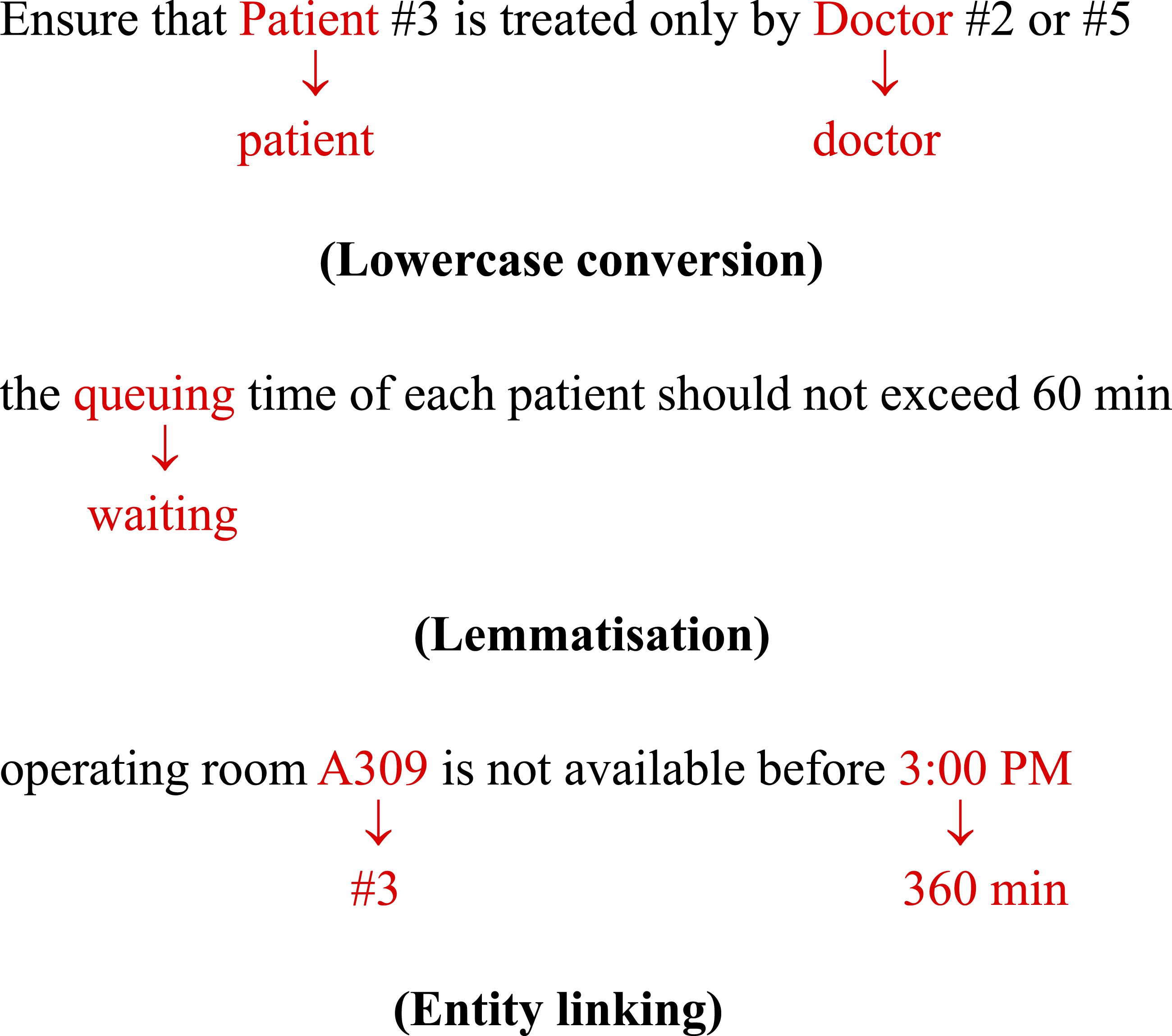
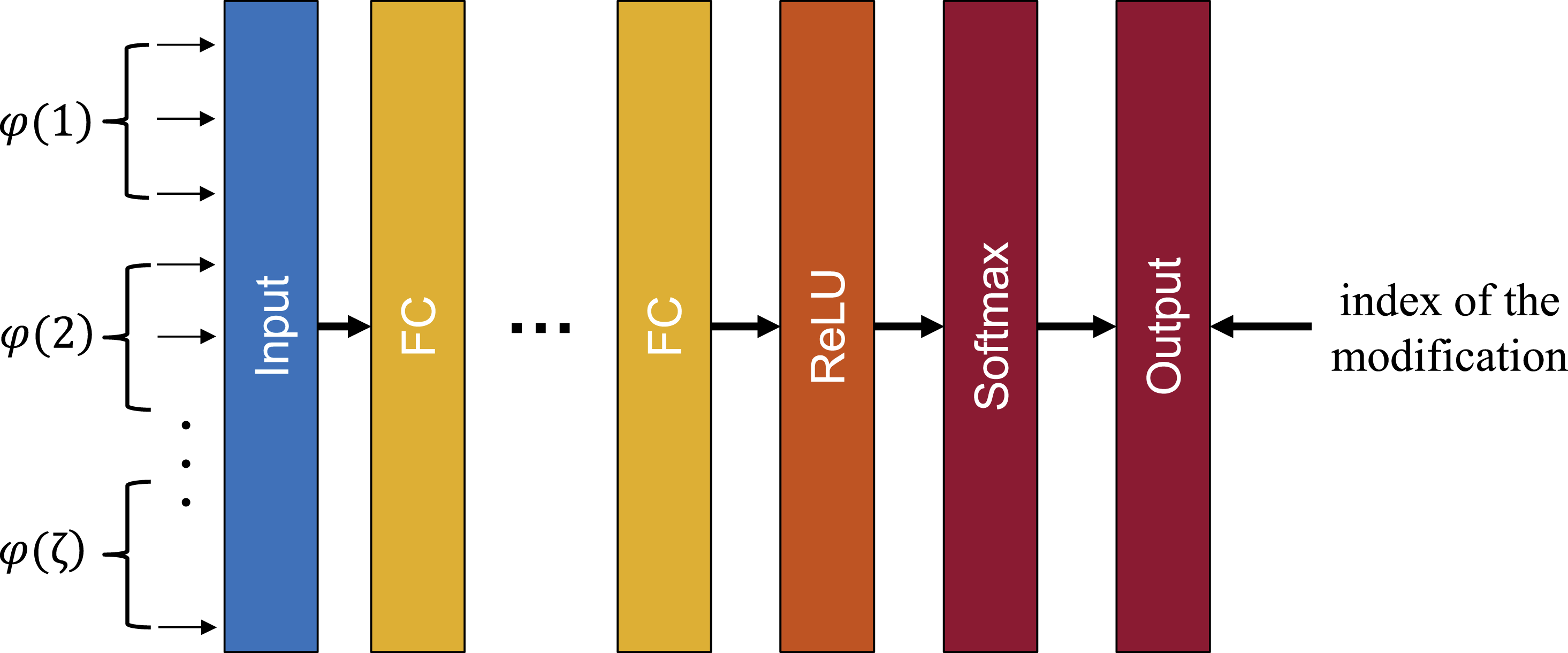
The DNN for parsing users’ queries is a feed-forward, fully connected neural network for classification
32
with the following configuration (refer to Figure 3): ● Input layer: There are ● Hidden layers: The DNN has ten hidden layers. The activation functions on the nodes of the first nine layers include a rectified linear unit (ReLU), hyperbolic tangent (tanh), and sigmoid functions to minimize cross-entropy loss. ● Output ( DNN parser.


Then, ● Actual value ( ● Training algorithm: The Broyden-Fletcher-Goldfarb-Shanno quasi-Newton algorithm (LBFGS)
33
is applied to train the DNN, and the classification performance is determined in terms of hit rate (HR).


The identified modifications associated with all segments are applied to the ETFN of the default patient scheduling problem to generate the ETFN of the scheduling problem that addresses the user’s requirements. For example, after the modification presented in Figure 4, the ETFN changes from Inputs to the DNN.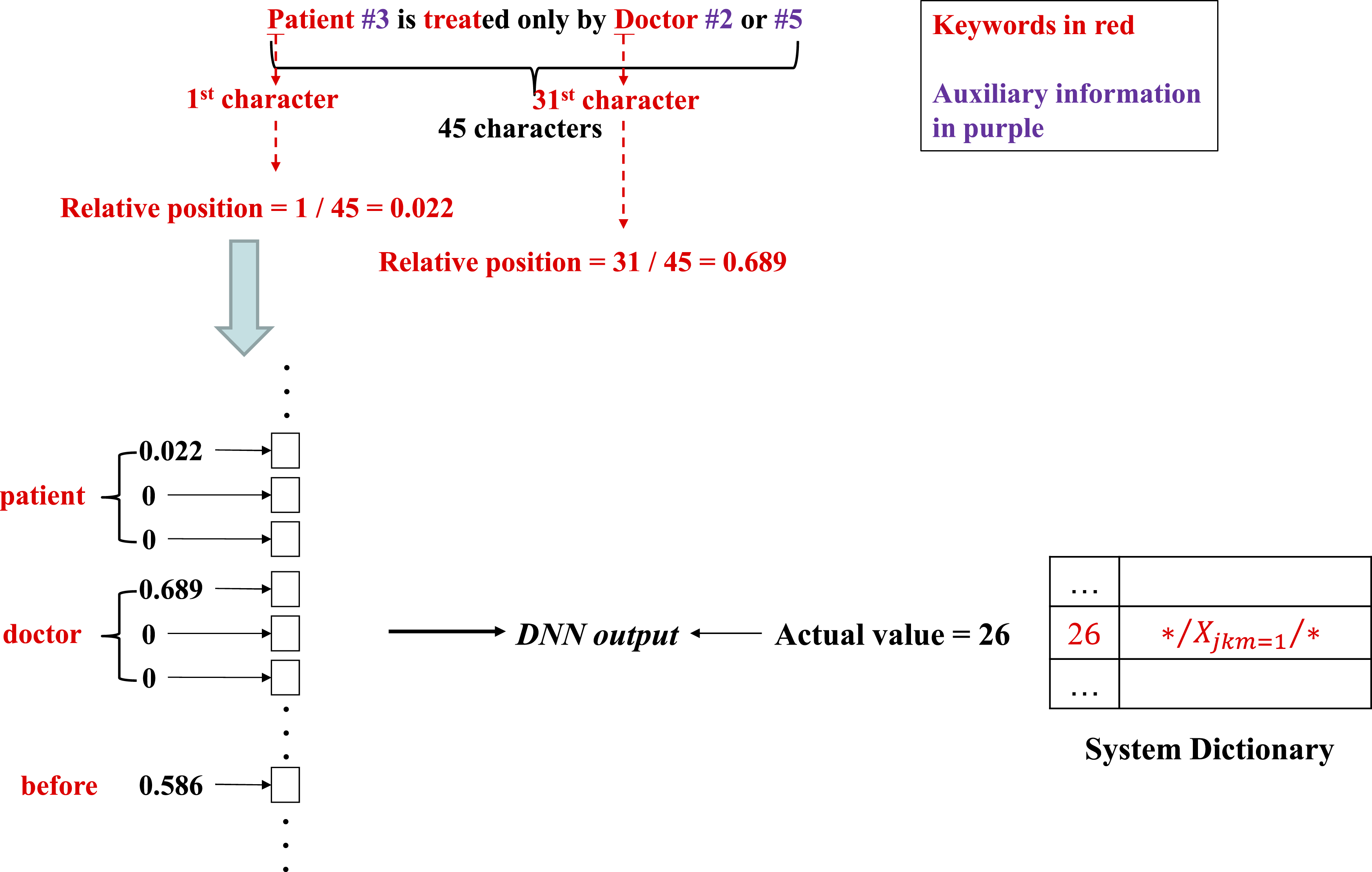
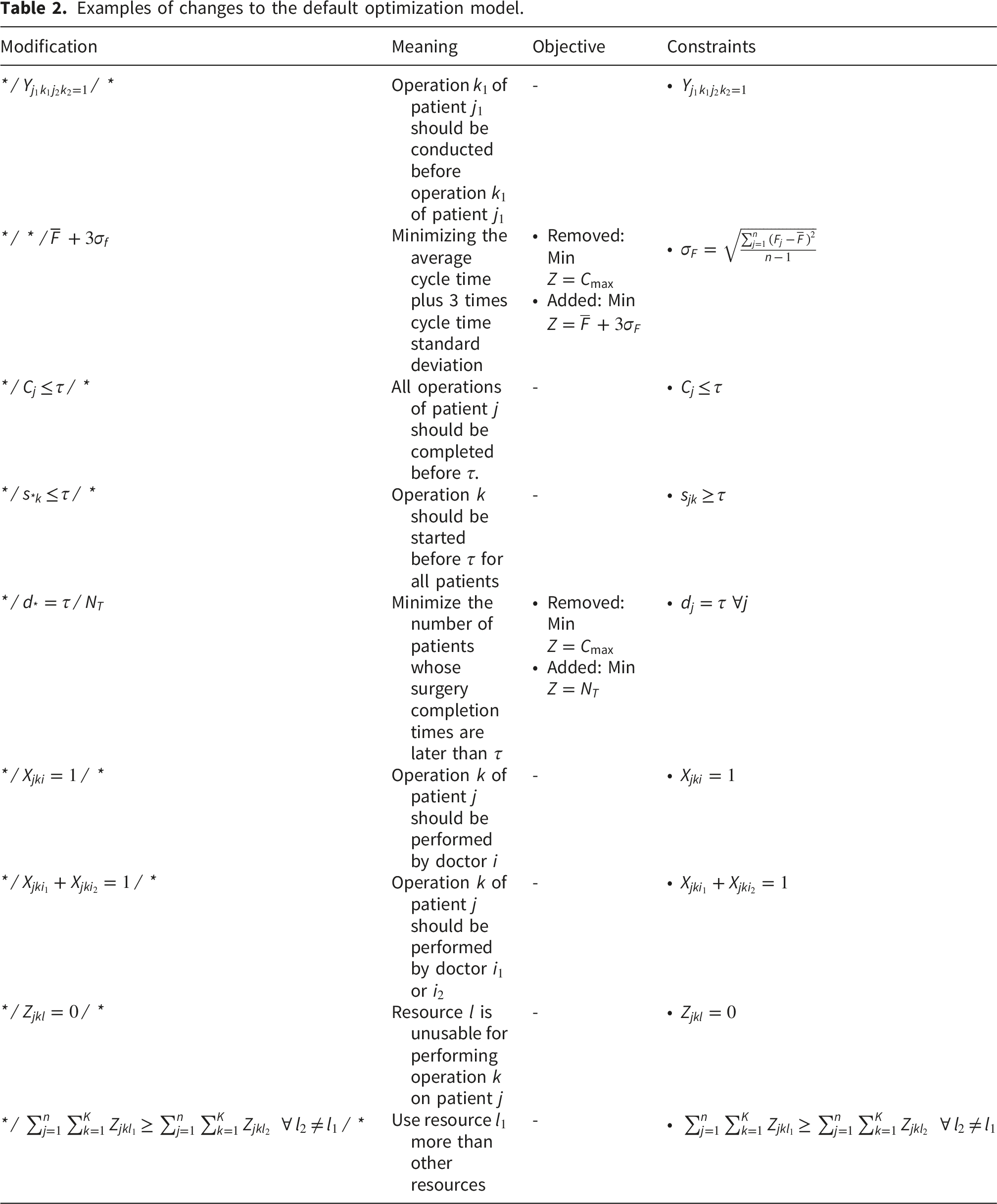
3.3. Formulating the customized optimization model
Examples of changes to the default optimization model.
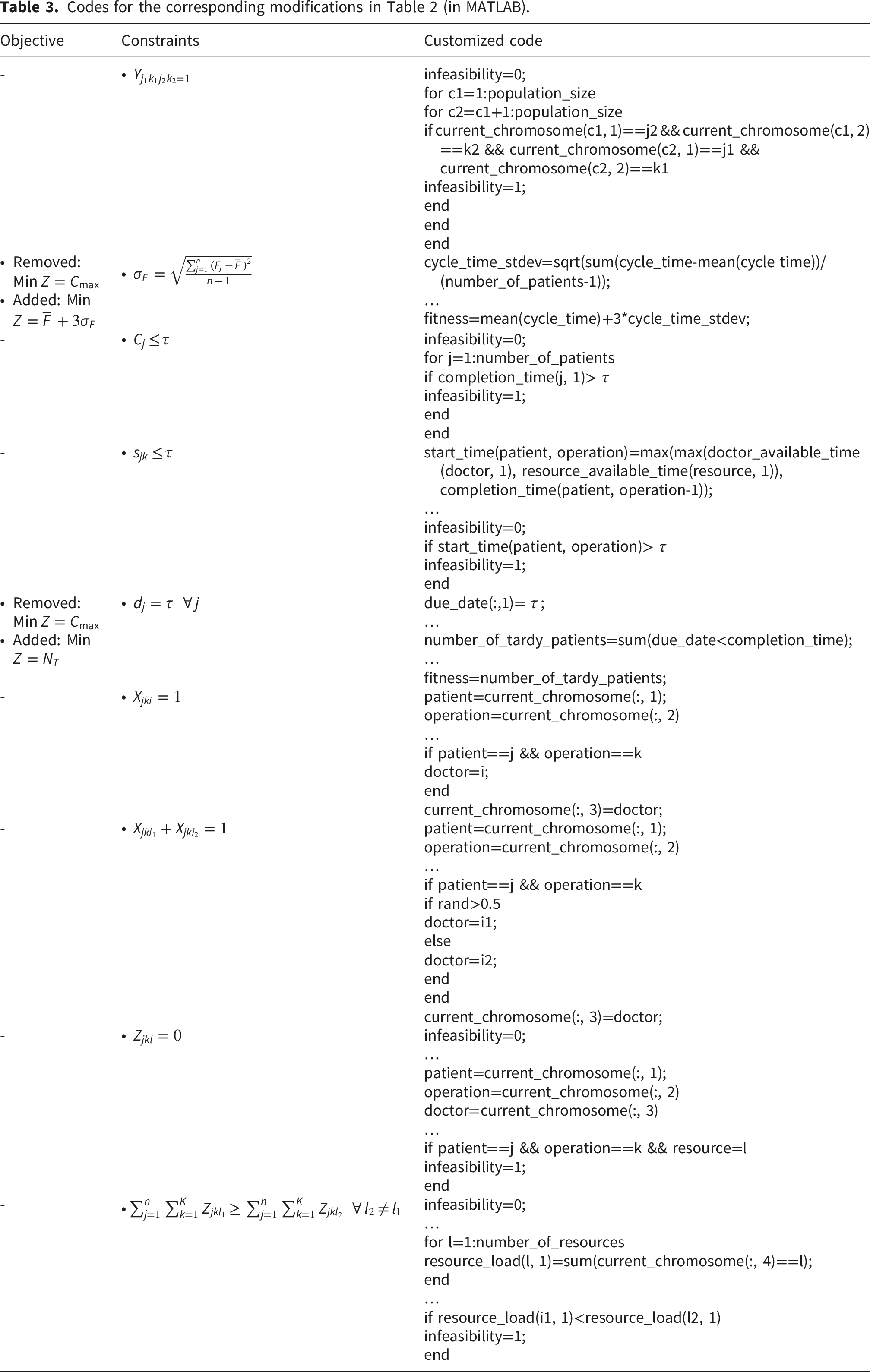
3.4. GA for solving the customized scheduling problem
In this study, the GA is automatically customized to satisfy users’ job scheduling requirements in terms of feasibility checks and/or fitness assessments. To this end, codes were pre-written to solve the default patient scheduling problem and implement all possible modifications. After extracting a user’s scheduling requirements using the DNN parser, codes for the corresponding modifications replace or are inserted into the code for the default patient scheduling problem.
3.5. Statistical analysis
Statistical methods applied in this study include a system usability scale (SUS) test and a paired t-test. The former was employed to examine the usability of the dedicated GenAI system, whereas the latter was employed to examine whether the scheduling performance of the dedicated GenAI system is significantly better than those of current practices.
4. Case study
4.1. Materials and method
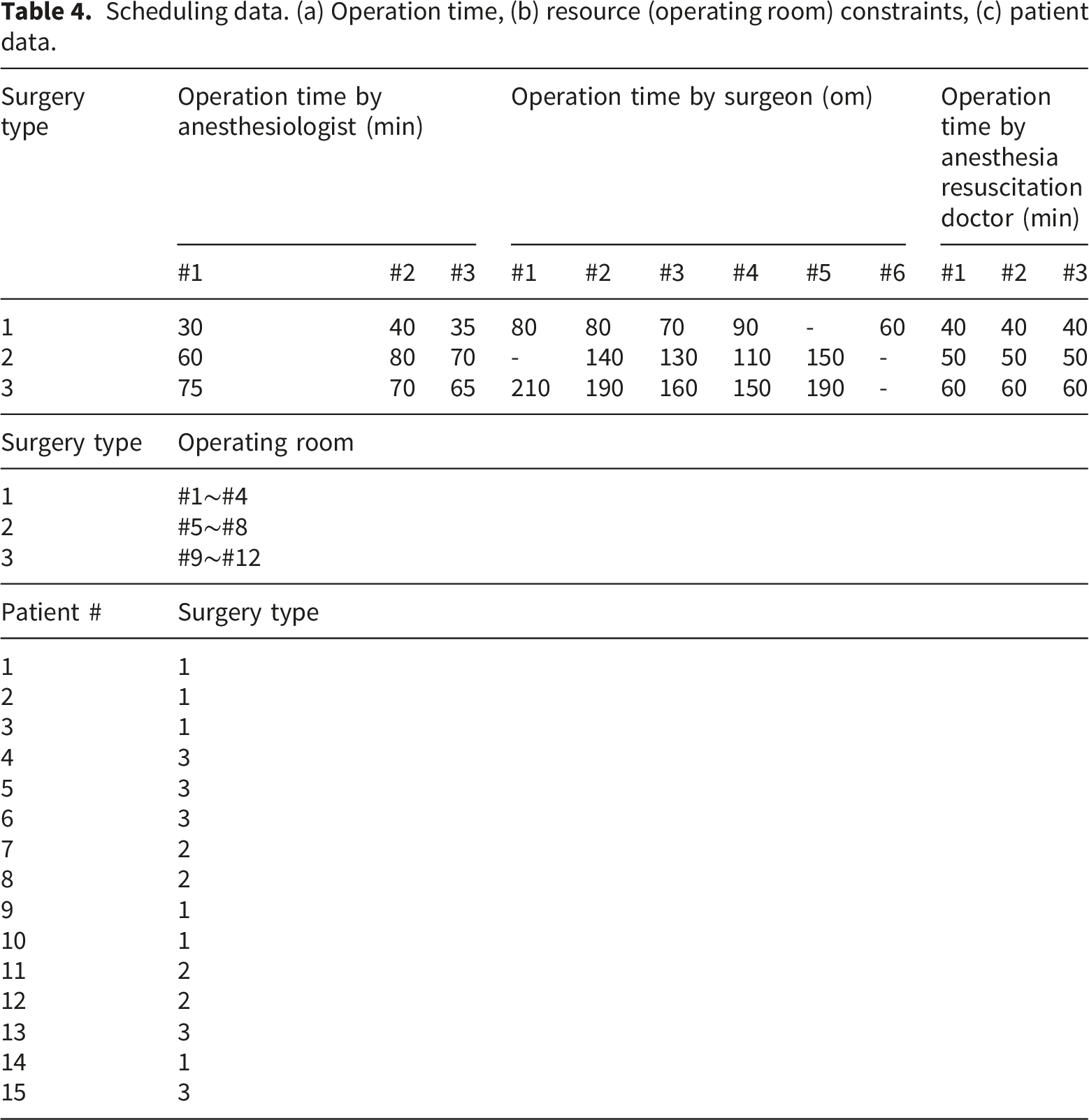
The dedicated GenAI system was applied to a real-world day surgery case obtained from the literature, involving the scheduling of patients on the verge of undergoing biliary surgery at a large public hospital in China. 27 In this case, three types of surgeries were to be performed on patients, namely, laparoscopic cholecystectomy, cholecystectomy, and common bile duct exploration T-tube drainage, each involving preoperative anesthesia, surgery, and anesthesia resuscitation. To perform these surgeries, three anesthesiologists, six surgeons, and three anesthesia resuscitation doctors were present. Four operating rooms were available for each type of surgery, which constituted the resource constraint in this case, and there were no missing data.
A customized GA was employed in the dedicated GenAI system to solve patient scheduling problems. The primary endpoint of this GA was whether the patient scheduling performance had satisfied the user’s expectations, which was used to determine the convergence target of the GA evolution.
4.2. Application of the proposed methodology
Scheduling data. (a) Operation time, (b) resource (operating room) constraints, (c) patient data.
Based on the scheduling data, the default scheduling problem was automatically identified as
Users enter their scheduling requirements in natural language via the user interface, as displayed in Figure 5. The requirements were segmented, from which all possible keywords, the corresponding relative positions, and auxiliary information were automatically extracted (refer to Figure 6). User interface of the dedicated GenAI system. Parsing process of natural-language queries.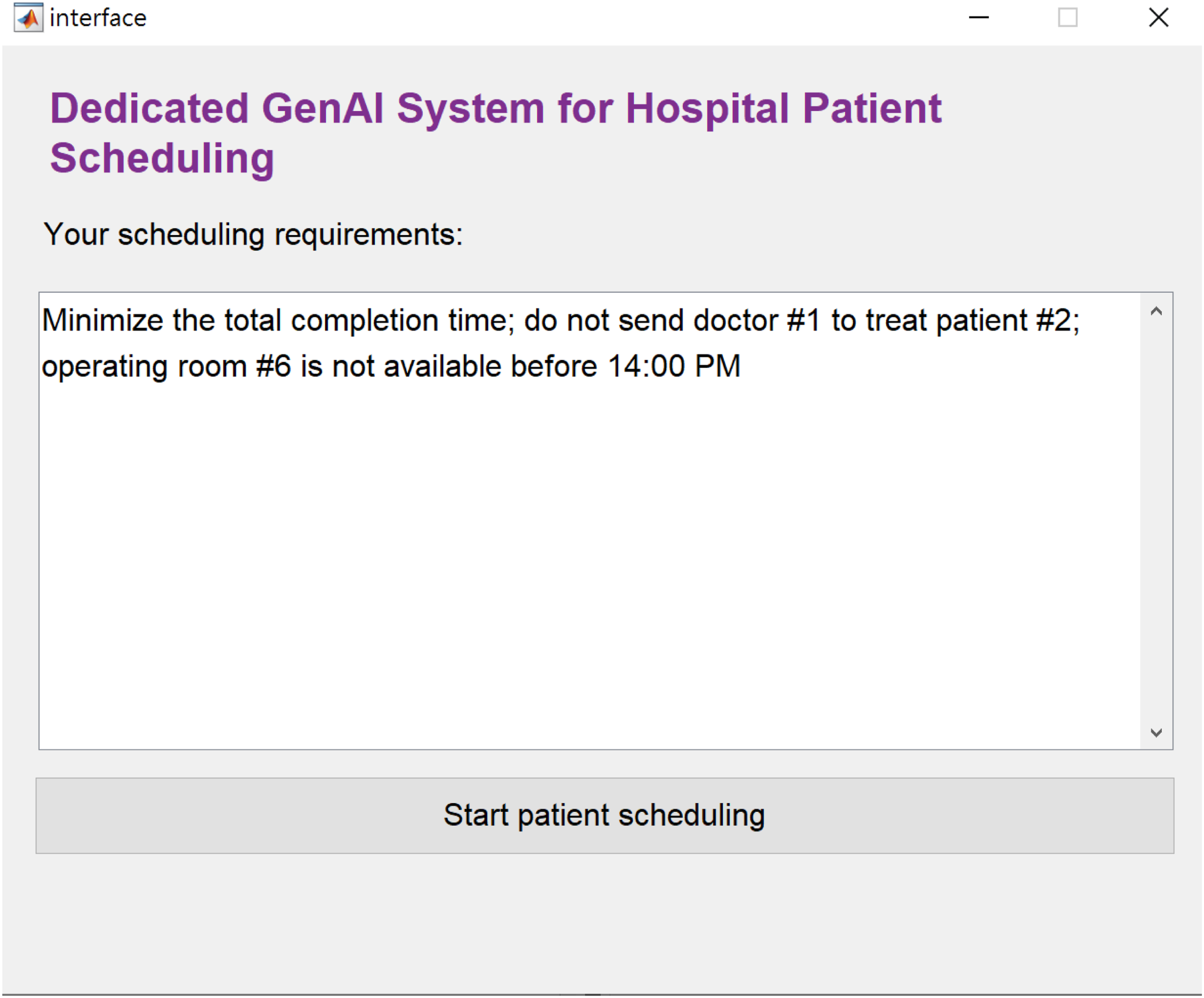

The extracted keywords and their relative positions were input to a DNN to determine the modifications required to the ETFN. The DNN had 63 inputs and 10 hidden layers, and the activation functions employed by the hidden and output layers were ReLU and softmax, respectively. The output was the index of the required modification (without auxiliary information) to the ETFN.
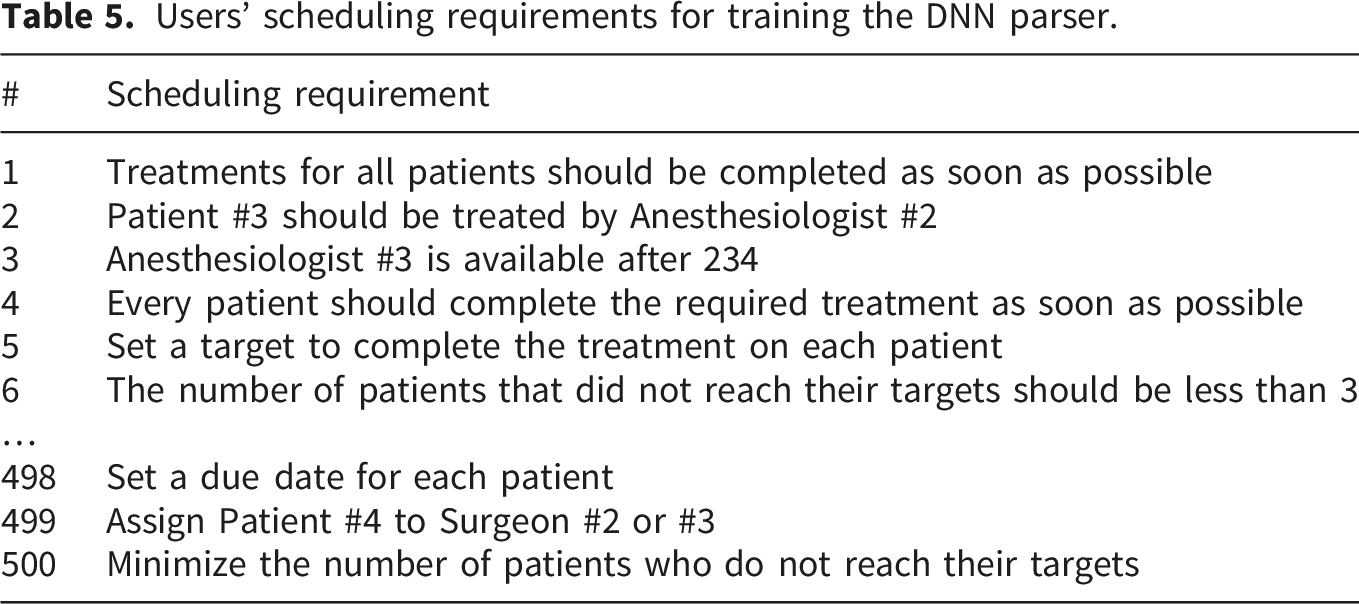
Users’ scheduling requirements for training the DNN parser.
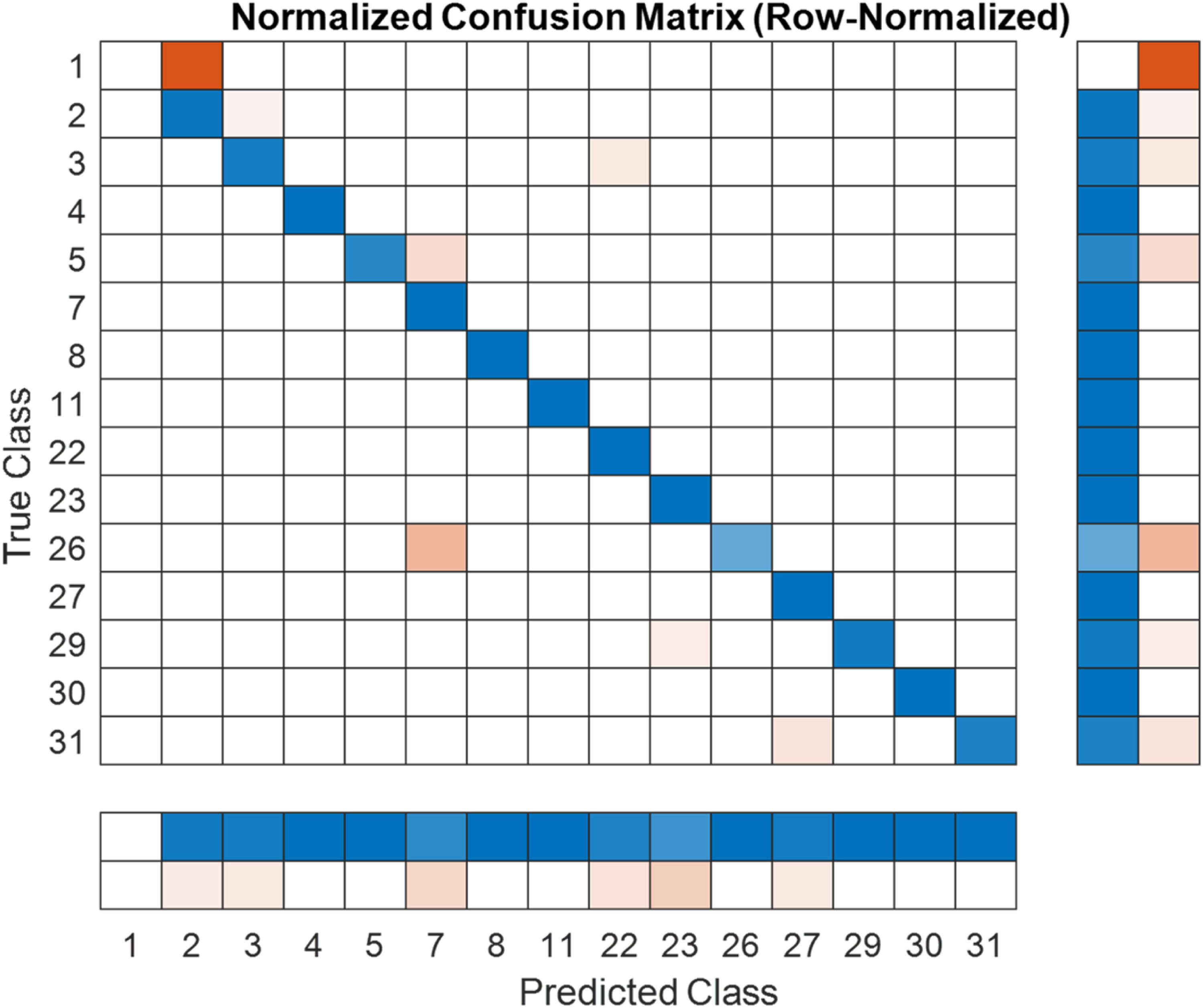
Confusion plot of the test data.
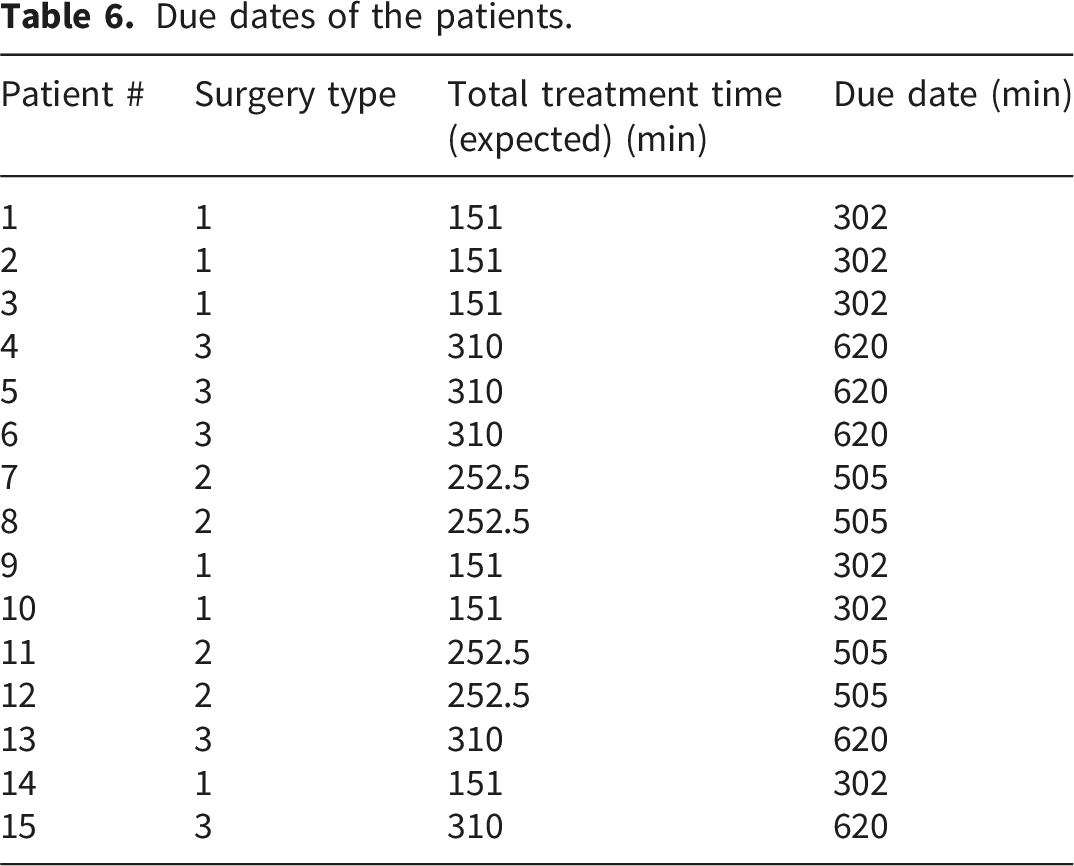
Due dates of the patients.
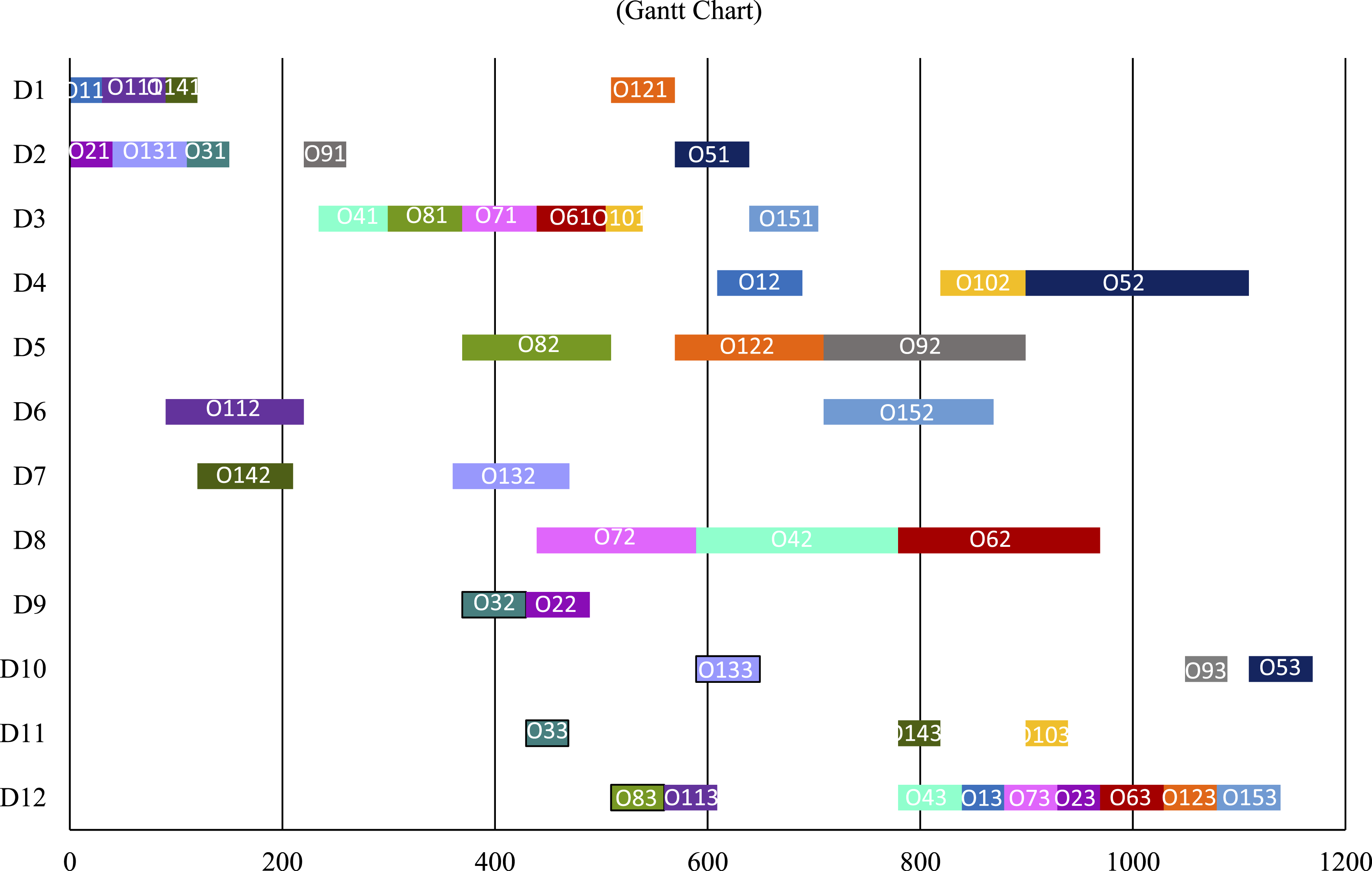
Subsequently, the DNN parser assisted users in formulating and solving scheduling problems that addressed their requirements. For example, the first user set the following scheduling requirements: “Treatments on all patients should be completed as soon as possible; patient #3 should be treated by Anesthesiologist #2; Anesthesiologist #3 is only available after 234.” The required modifications were determined using the DNN parser as “// Line chart for observing fitness fluctuations during the evolution process. Gantt chart.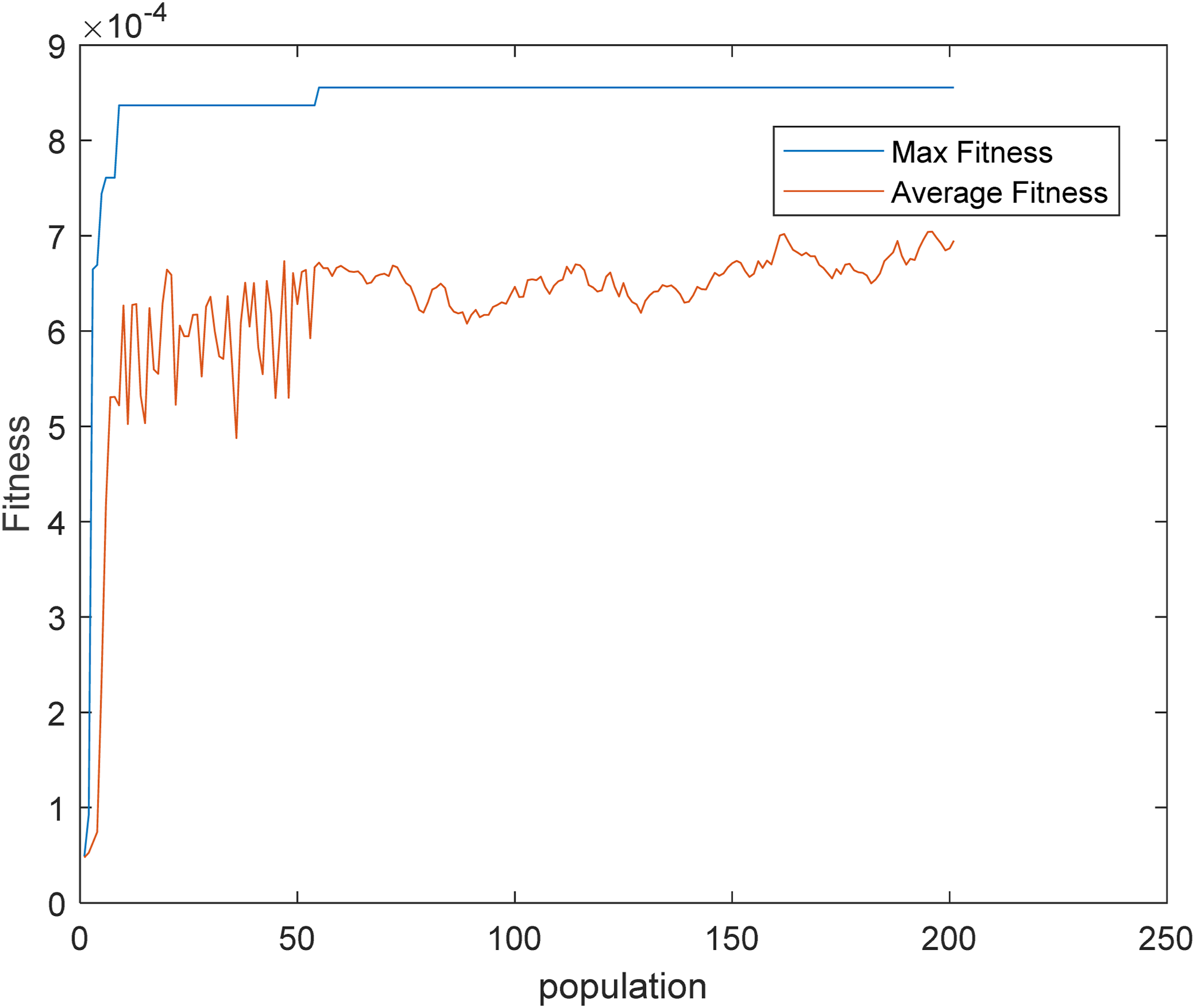
The experimental results revealed the following:
5. Discussion
The experimental results indicate the following: ● Allowing users to use natural language as input enabled them to express their scheduling requirements in as much detail as possible. In this case, the scheduling problem became increasingly constrained, shrinking the feasible region. Therefore, the customized GA could converge with a reduced number of iterations or populations. In this case, only approximately 110 iterations or populations were sufficient for the evolving process to converge in the case of the maximum fitness. ● Patient scheduling in hospitals or clinics differs from job scheduling in manufacturing. Hospitals prioritize fairness in scheduling results, ensuring that each patient spends the same duration in the hospital, whereas factories usually optimize overall performance, instead of focusing on individual jobs. This difference becomes highly apparent when using GenAI to facilitate users in expressing their scheduling requirements. ● To further investigate the effectiveness of the dedicated GenAI system, a branch-and-bound (B&B) algorithm
34
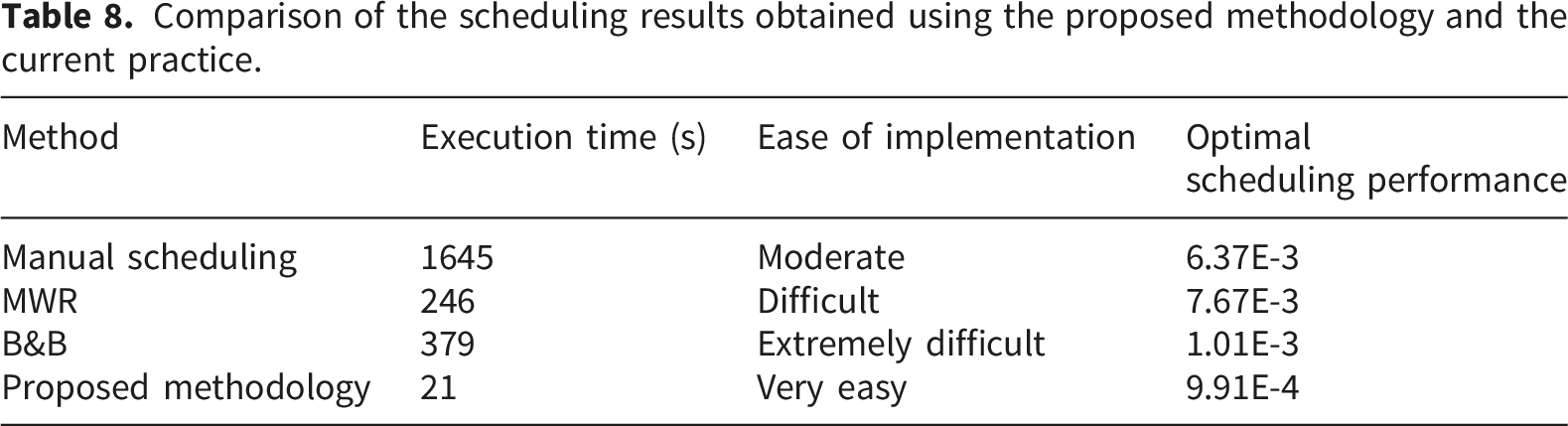
was proposed to solve the customized patient scheduling problem written in Lingo on the same platform. Manually creating and refining the customized patient scheduling problem (if it was found to be infeasible) required approximately 3 h. The two methods found the same optimal solution, proving the effectiveness of the dedicated GenAI system. Comparison of the scheduling results obtained using the proposed methodology and the current practice.
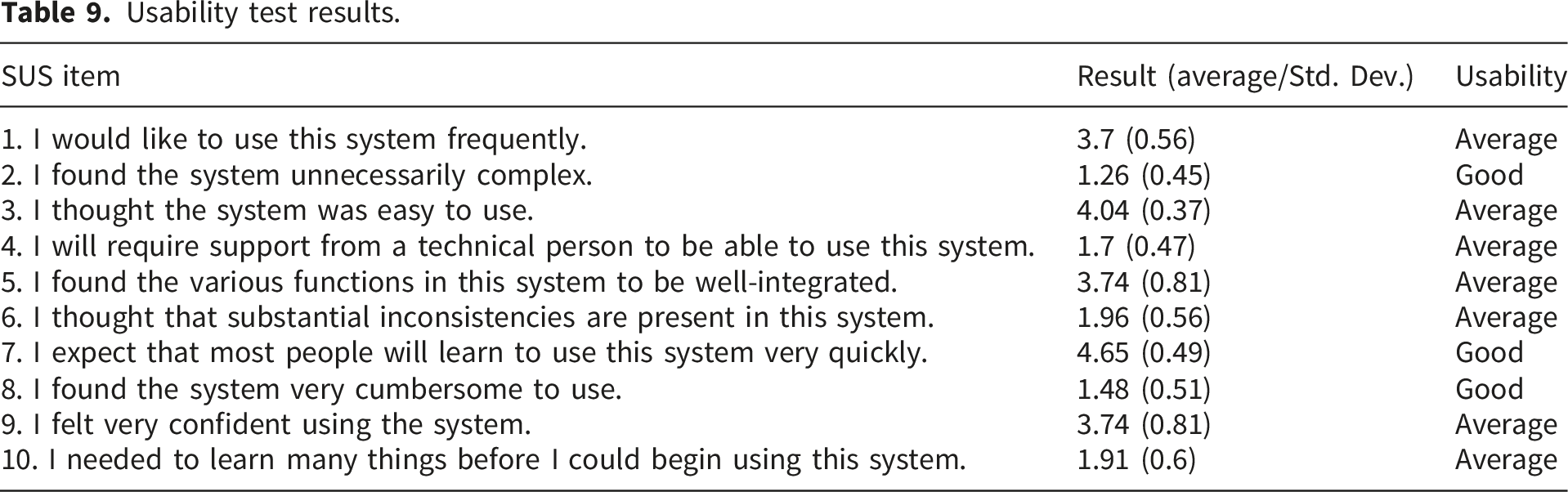
● The results of the SUS questionnaire showed that the usability of the dedicated GenAI system was particularly satisfactory in reducing perceived complexity or cumbersomeness, thereby accelerating the expected learning time., which was due to enabling users to express their scheduling requirements in natural language and the ability of the dedicated GenAI system to interpret these queries with high accuracy. Nevertheless, traditional patient scheduling systems offer users a wide range of scheduling options. With the dedicated GenAI system, users must enter their appointment requirements, which may not be easy for users with little scheduling experiences, making them feel that they need to learn many things.
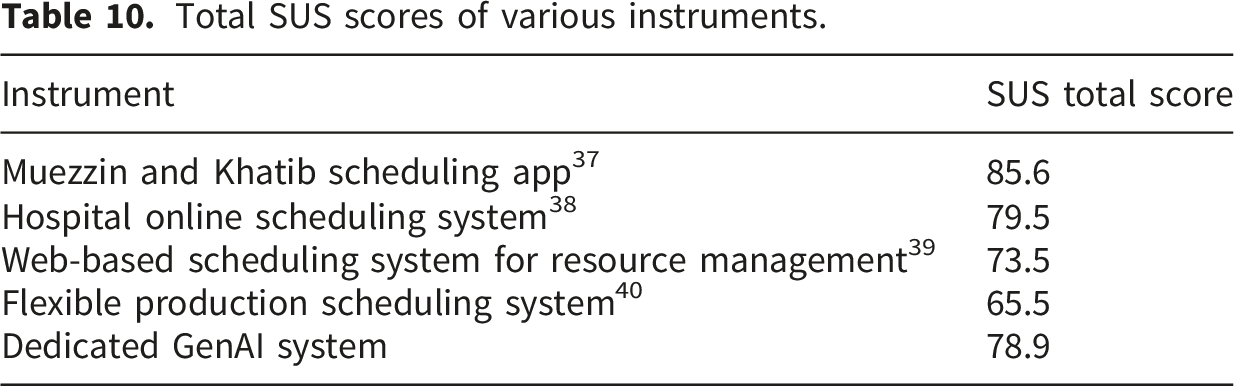
Total SUS scores of various instruments.
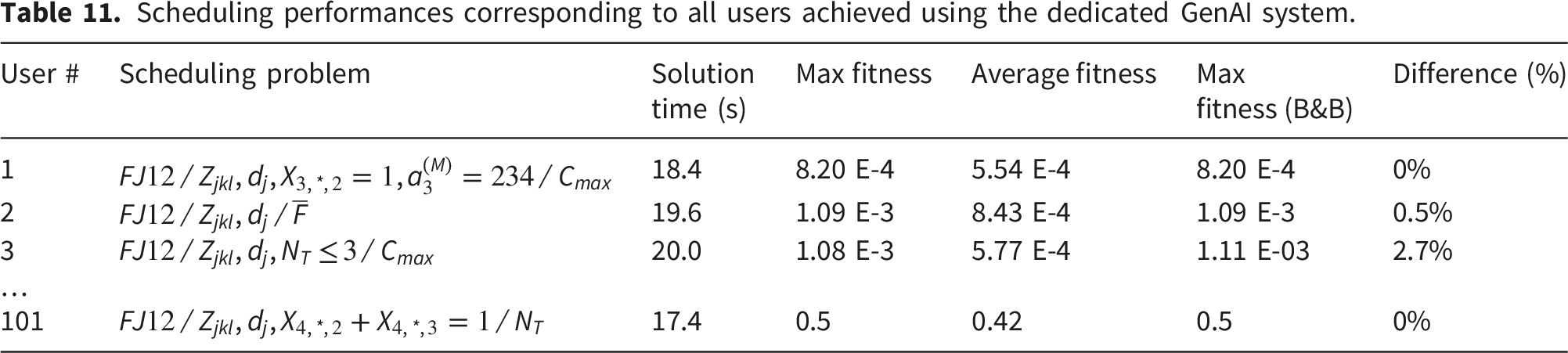
Scheduling performances corresponding to all users achieved using the dedicated GenAI system.
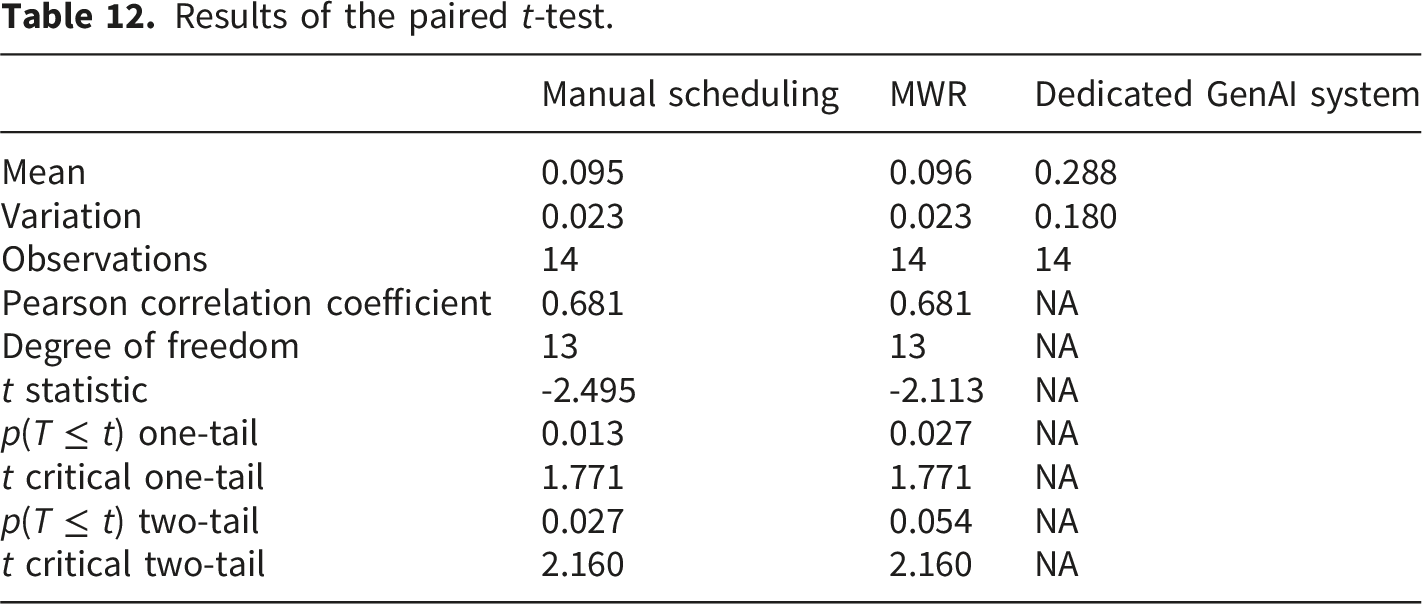
● A paired t-test was conducted to examine the following hypotheses to ascertain whether the advantage of the dedicated GenAI system over current practices was significant.
H0: The scheduling performance in terms of the maximum fitness achieved using this system would be the same as those achieved using the current practices.
H1: The scheduling performance in terms of the maximum fitness achieved using this system would be higher than those achieved using the current practices.
Table 12 lists the results obtained from the paired t-test. Specifically, H0 was rejected if α > p(T ≤ t) in a one-tailed test. The proposed methodology outperformed two current practices, namely, manual scheduling and MWR. The scheduling performance achieved using the dedicated GenAI system was significantly higher (α = 0.05) than those achieved using both current practices. ● However, the proposed methodology possesses certain limitations. First, eliminating the requirement for users to construct and encode optimization algorithms is a black-box approach,
36
which may reduce users’ understanding and trust in the dedicated GenAI system.
37
Furthermore, allowing users to input scheduling requirements in natural language may cause multiple scheduling objectives to be inadvertently included, which requires the use of multi-objective GAs to handle.
38
● Another bio-inspired algorithm, such as ant colony optimization, particle swarm optimization, agent system, or artificial bee colony, can also be applied to solve the patient scheduling problem.39–42 Results of the paired t-test.
6. Conclusions
GenAI systems have rarely been applied to patient scheduling in hospitals or clinics. Such applications are particularly urgent because people responsible for patient scheduling usually lack the relevant expertise, distinct from engineers responsible for job scheduling in factories. In addition, patient scheduling results affect each patient, whereas operation scheduling results are only meaningful to the production controller. Therefore, a dedicated GenAI system for patient scheduling in hospitals or clinics is established in this study. First, this system imports the scheduling data to formulate the default patient scheduling problem. Users enter their scheduling requirements in natural language via the system interface to formulate their customized patient scheduling problems, for which a DNN parser extracts information regarding keywords to establish the corresponding ETFNs. Subsequently, a customized GA is automatically generated to solve the customized patient scheduling problem.
The dedicated GenAI system was applied to a real-world case obtained from the literature, involving 12 anesthesiologists, surgeons, or anesthesia resuscitation doctors, 12 operating rooms, and 15 patients undergoing three types of surgeries, each consisting of three operations. The experimental results yielded the following conclusions: ● The DNN parser achieved very high classification performance for queries in the training data and effectively classified unlearned scheduling requirements. ● Given the scheduling requirements of users, the complexity of customized patient scheduling problems was higher than those of problems addressed using traditional methods in previous studies. Therefore, applying existing general-purpose GenAI systems was difficult, as minimal historical cases are available for learning. ● Increasing the number of incorporated scheduling requirements increased the number of constraints in the customized patient scheduling problem, thereby shrinking the feasible region and enabling the customized GA to converge within a reduced number of iterations or populations. ● The optimal solution obtained using the dedicated GenAI system was verified using the B&B method. The difference in the optimal fitness achieved using the two methods was under 1% on average, demonstrating the effectiveness of the proposed methodology. ● The most complex customized patient scheduling problem could be automatically modeled and solved within 20 s.
One straightforward means of monitoring and verifying a scheduling plan generated by the dedicated GenAI system is to export the scheduling results to a project management system to check the correctness of the optimal scheduling performance, identify any resource conflicts, and monitor activities as the plan progresses. In addition, system updates are accomplished by updating the information contained in the data input to the dedicated GenAI system.
This proposed system, however, poses a few limitations. Scaling the dedicated GenAI system to large hospitals handling numerous patients will be challenging. Furthermore, this study only considered two resources, namely, doctors and operating rooms, to constrain the patient scheduling problem. Considering additionally resources, such as machines or robots in rehabilitation and other healthcare scenarios,16,17,43 will significantly increase the scale of the patient scheduling problem and expand the feasible region owing to increased dimensionality. Determining whether the dedicated GenAI system will remain effective under such circumstances requires further investigation, constituting some directions for future research.
Footnotes
Author contributions
All authors contributed equally to the writing of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request.
Appendix
Other variables ∈ R+where
In addition, the cycle time of patient j can be derived as
Therefore, the average cycle time and cycle time standard deviation are calculated as
respectively. When scheduling patients, it is especially important to ensure that all patients finish their consultations earlier or later by roughly the same amount, which requires minimizing cycle time standard deviation. Furthermore, the available time of doctor i is indicated with
Although there is no specific due date for a patient, the patient does have an expected end time for his/her consultation, which is similar to the concept of a due date. Schedulers can set the due date for each patient to be the patient’s arrival time plus the historical average cycle time. Schedulers can also set the due date for each patient to be the closing time of the hospital/clinic. Then, then the lateness and tardiness of the patient can be derived as