
Abstract
Objective
This study compared an image-based, artificial intelligence-driven instrument recognition and inventory system (AI-IRIS) with conventional manual counting (CMC) for postoperative instrument management in simulated settings.
Methods
Using a randomized crossover design, 34 operating room nurses completed two standardized counting scenarios with both methods and rated adoption using the Diffusion of Innovations Questionnaire (DOIQ).
Results
Recognition accuracy was identical between AI-IRIS and CMC under controlled, simulated conditions. However, the AI-IRIS significantly reduced counting time by 26–28 seconds per scenario, representing an approximately 33–35% reduction compared with manual counting (both p < 0.001), and achieved higher DOIQ scores (mean difference 7.9 points, p < 0.001).
Conclusions
The AI-IRIS improved efficiency and user perception without compromising accuracy. These findings suggest potential to support safety-related counting processes and streamline workflows. Future research should assess its integration in real-world perioperative environments and across diverse instrument sets and pack configurations.
Keywords
Introduction
Retained surgical items (RSIs) are considered preventable “never events,” yet they remain a persistent and serious patient safety concern. 1 Manual instrument counting, the standard practice in most operating rooms, is error-prone due to communication breakdowns, distractions, and time constraints.2,3 Effective surgical instrument management is crucial for ensuring patient safety, with accurate counts before, during, and after procedures as a critical defense against RSIs.
RSIs refer to surgically used supplies or devices intentionally introduced into the operative field but inadvertently left inside the patient following the procedure. They are not classified as “foreign bodies” because they were purposely used by the surgical team. 4 RSIs can lead to serious complications, including infections, bowel perforation, fistulas, obstructions, reoperations, and, in severe cases, death. 5 Beyond the clinical consequences, RSIs also impose significant psychological and moral distress on surgical staff, who may face professional investigations and be required to undergo remedial training. 6
Despite their preventability, RSIs continue to occur. The World Health Organization has reported that manual counting is susceptible to human error, with incidence rates ranging from 1 in 5,000 to 1 in 19,000 inpatient surgeries, and potentially as high as 1 in 1,000 in specific contexts. 7 The estimated incidence of abdominal and pelvic surgeries is 13 per 100,000 cases. 8 In 2023, RSIs accounted for 8% of the 1,411 sentinel events reported to the United States Joint Commission, ranking third after patient falls and wrong-site surgeries. 9 Alarmingly, 62% of RSIs occurred despite documentation of a correct count, demonstrating the inherent limitations of manual methods. 10
RSIs are best addressed through a layered framework that incorporates global, professional, and systems-level safety guidance. At the global level, the World Health Organization (WHO) Surgical Safety Checklist integrates RSI prevention into routine perioperative practice by requiring a team sign-out to verbally confirm the counts of instruments, needles, and sponges before the patient leaves the operating room. This reframes counting as a standardized, shared responsibility rather than an individual task. Recent evaluations of the checklist, and global patient safety frameworks, emphasize the importance of standardized, systems-based approaches to reduce adverse events. 7
At the professional level, the Association of periOperative Registered Nurses (AORN) guideline for RSI prevention advocates for a multidisciplinary approach, emphasizing standardized counting procedures, thorough wound assessments, and the strategic use of adjunct technologies such as barcoding and radiofrequency identification (RFID) systems. 6
In response to the limitations of manual methods, there has been a growing interest in automated tracking technologies designed to improve accuracy and efficiency. In one study involving 300 surgeries, a barcoded sponge system identified more counting discrepancies than manual methods. Although it introduced minor technical issues and slightly increased procedure time, it was easy to use and improved error detection. 11 Several investigations into radiofrequency detection systems have shown significant reductions in retained surgical sponges, particularly in high-risk emergency procedures. These systems have demonstrated value as adjuncts to manual counting, preventing errors and reducing costs even when counts appear correct.12–14 However, adoption remains limited due to technical and operational challenges, including signal interference from metal instruments, difficulty tagging small or complex tools, and RFID tag degradation during standard cleaning and sterilization processes. 15
In contrast to traditional tracking methods, recent advances in image-based artificial intelligence (AI) recognition systems offer a potentially more robust and adaptable solution. These systems eliminate the need for physical tags and can be trained to recognize a wide range of surgical instruments, regardless of their size or complexity. For example, a deep learning model achieved an average precision of 98.9% across 14 instrument types. 16 Another proof-of-concept study using 1,004 images encompassing 13,213 tools across 11 categories reported precision rates ranging from 94.0% to 100%, with recall between 97.1% and 100%. 17 Additional work using computer vision-based on the YOLOv4-tiny architecture demonstrated the feasibility of real-time detection in clinical settings, such as monitoring mask usage during the COVID-19 pandemic. 18 With continued improvements in computer vision algorithms and processing power, AI now holds promise for automated, real-time counting of surgical instruments, potentially serving as an additional safeguard against RSIs. 19
Compared with tag-dependent systems such as barcoding or RFID, a tag-free, vision-based AI approach may offer distinct advantages, including elimination of hardware modification to instruments, reduced susceptibility to signal interference or tag degradation during sterilization, and improved scalability across diverse instrument sets without altering established workflows.
The present study evaluates the performance of an AI-based Instrument Recognition and Inventory System (AI-IRIS) 20 in comparison with conventional manual counting (CMC). Specifically, it assesses the system’s accuracy in identifying instrument type and enumerating quantities. This study aims to generate empirical evidence on the effectiveness of AI-IRIS and support the integration of AI-driven technologies into surgical nursing workflows.
Although surgical instrument counting and verification are required throughout the perioperative period, this study focused on the postoperative phase. This stage was selected to ensure that data collection and system testing would not interfere with aseptic technique or infection control practices during the preoperative and intraoperative processes. Moreover, this period is also recognized as the most vulnerable stage for retained surgical instruments, when items may inadvertently remain within the patient or become concealed in drapes or linens.
Methods
Study design and procedures
This randomized crossover study evaluated the performance of the AI-IRIS compared with CMC during postoperative instrument verification (Figure 1). Thirty-four operating room nurses were enrolled and randomly assigned (1:1) to one of two testing sequences using a computer-generated random number table. In Sequence A, participants completed two standardized scenarios using AI-IRIS followed by a 5-minute washout and then repeated the same scenarios using CMC. Sequence B followed the reverse order. Both methods were demonstrated prior to testing, and participants practiced until achieving proficiency through a return demonstration. The specific tasks undertaken in the two study scenarios are outlined in Appendix 1. Study flowchart.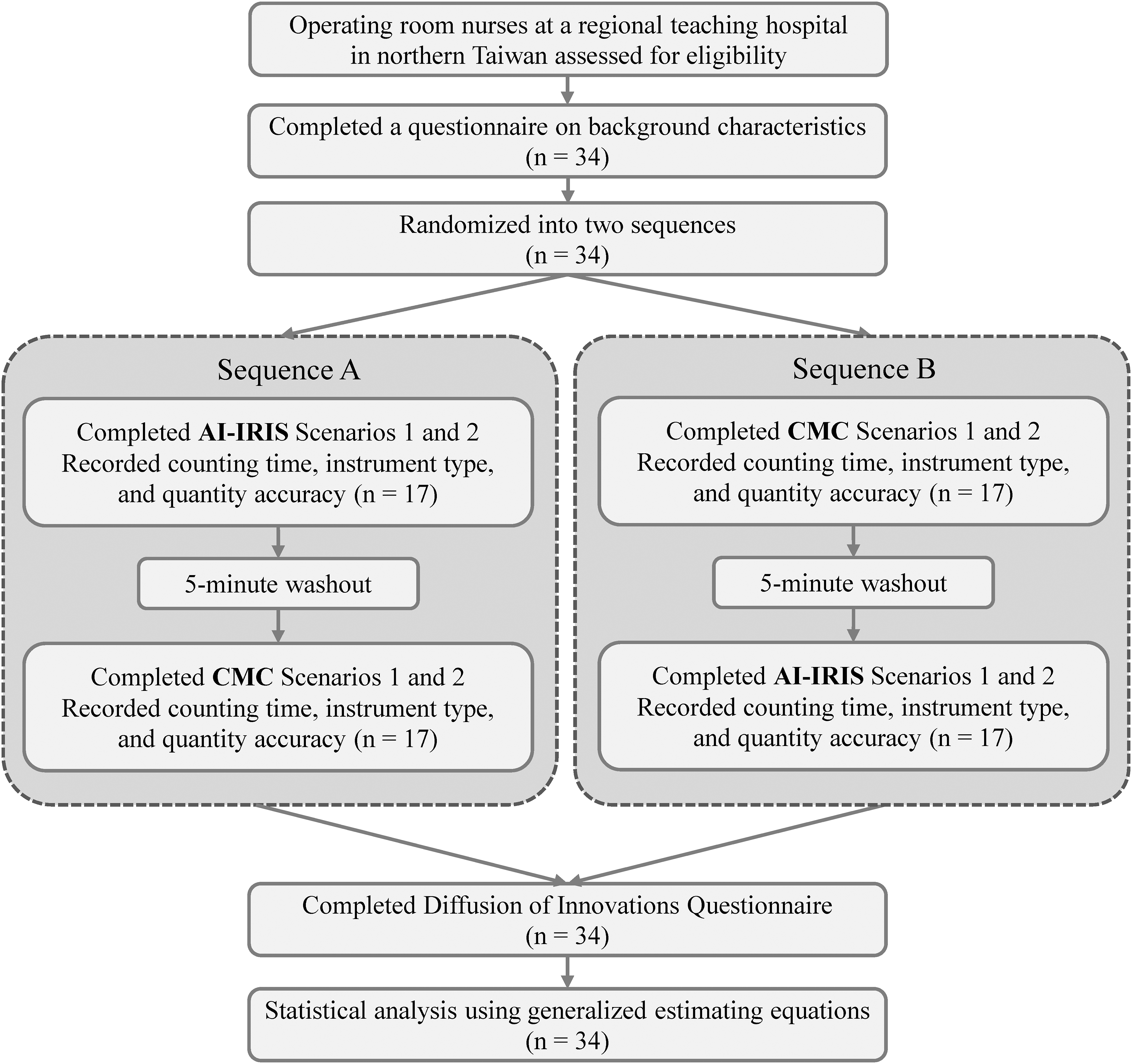
The scenarios were developed using actual orthopedic instrument sets routinely used at the study hospital to reflect typical postoperative counting tasks. Each scenario required participants to identify instrument types and confirm quantities against predefined inventory lists under controlled tray-based conditions. Instruments were arranged according to standard postoperative layout practices to mirror routine workflow. Lighting conditions and camera positioning were fixed to ensure consistency across participants and testing sessions. These design choices enabled controlled comparison between AI-IRIS and CMC while maintaining relevance to routine postoperative instrument verification.
During each scenario, participants verified surgical instruments and quantities using the assigned method. Counting time, recognition accuracy, and quantity accuracy were recorded with a scenario-based record form. After completing both methods, participants filled out the Diffusion of Innovations Questionnaire (DOIQ) to assess perceptions of effectiveness, ease of use, workflow integration, and willingness to adopt. Each session lasted approximately 15–20 minutes per participant.
Study participants
Sample size was calculated using G*Power 3.1.9.7 for a Wilcoxon signed-rank test (effect size = 0.65, α = 0.05, power = 0.8), yielding a minimum sample size of 30. Allowing for a 10% attrition rate, the final sample size was set at 34 participants.
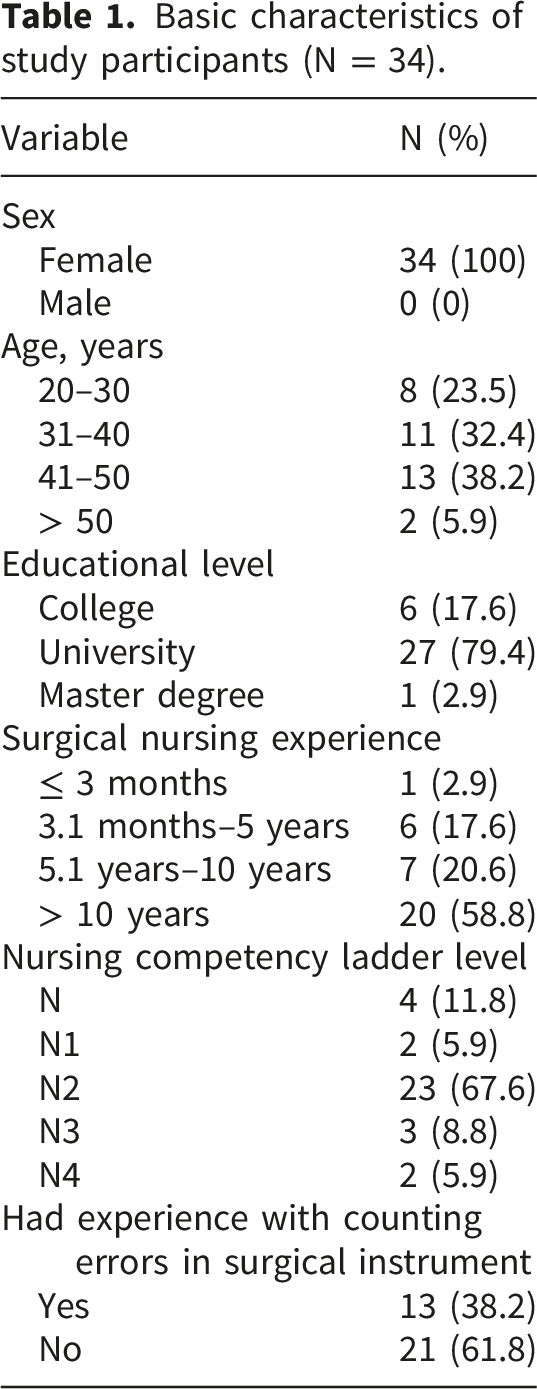
Participants were recruited from a regional hospital in northern Taiwan. Eligible participants were full-time nursing staff aged ≥ 20 years, holding a valid nurse or registered nurse license, and currently employed in the operating room of the study hospital. Head nurses and operating room assistants were excluded. Recruitment was conducted via posters displaying QR codes in the surgery debriefing room. All participants completed a background characteristics questionnaire covering age, sex, education, surgical nursing experience, nursing competency level, and history of instrument counting errors. Moreover, the questionnaire included a multiple-choice item prompting participants to select the top three perceived causes of instrument counting errors from ten predefined options.
Artificial intelligence-based instrument recognition and inventory system (AI-IRIS)
The AI-IRIS was developed to automate surgical instrument recognition and counting (Figure 2). The system integrates a red-green-blue (RGB) camera module, an NVIDIA Jetson Xavier NX edge-computing platform, and a real-time information dashboard for detection and inventory management (Figure 3(a)).
20
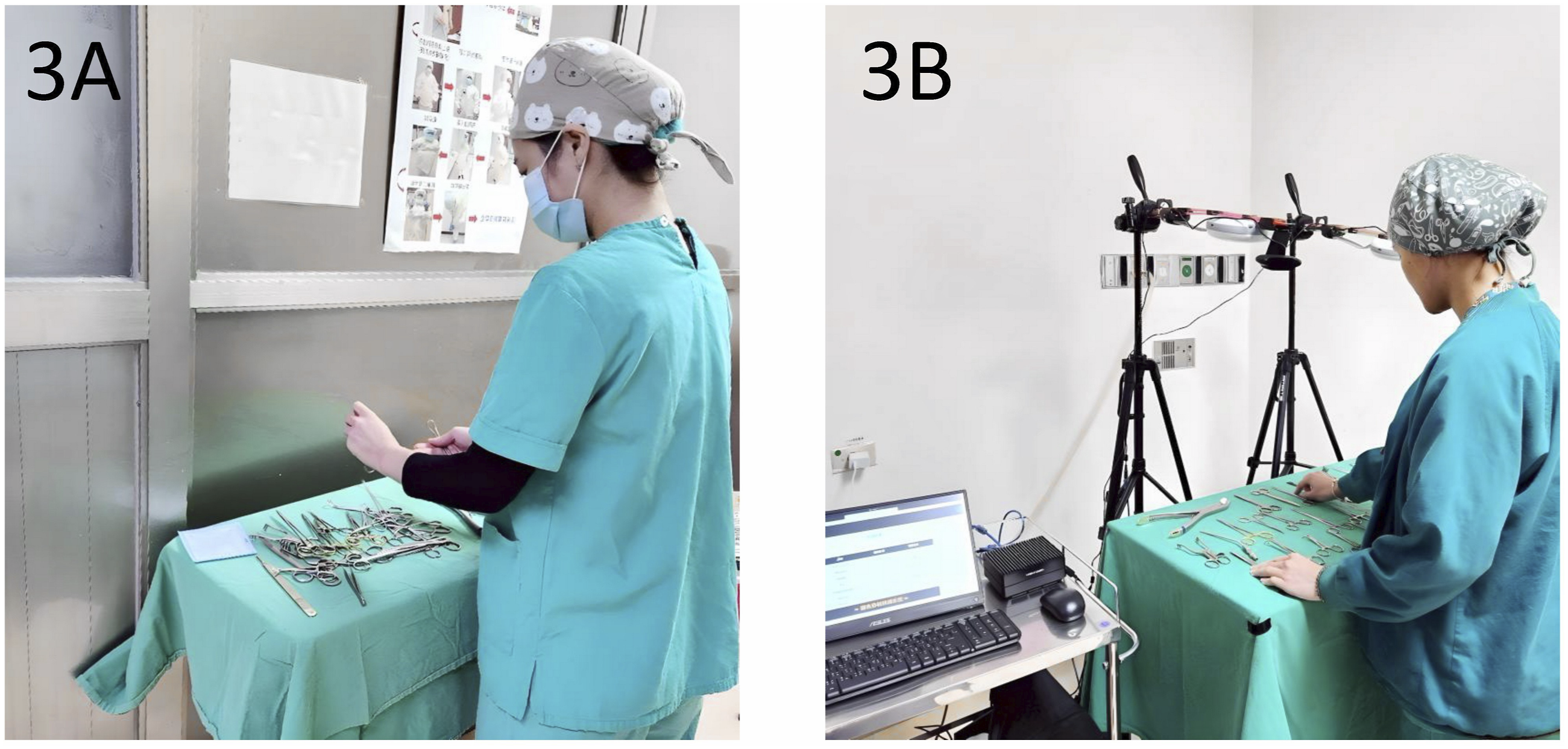
Workflow of the artificial intelligence-based instrument recognition and inventory system (AI-IRIS). A surgical tray is placed in the instrument recognition area, where an RGB camera captures images for processing. The system performs real-time, on-device inference using YOLOv7 on the NVIDIA Jetson Xavier NX platform. Recognition results and inventory are displayed on the AI-IRIS dashboard, enabling immediate verification by clinical staff. Conventional manual counting and artificial intelligence-based instrument recognition. (a) Manual counting performed by a scrub nurse using a standardized checklist. (b) AI-IRIS system automates recognition using an RGB camera and real-time dashboard display for verification.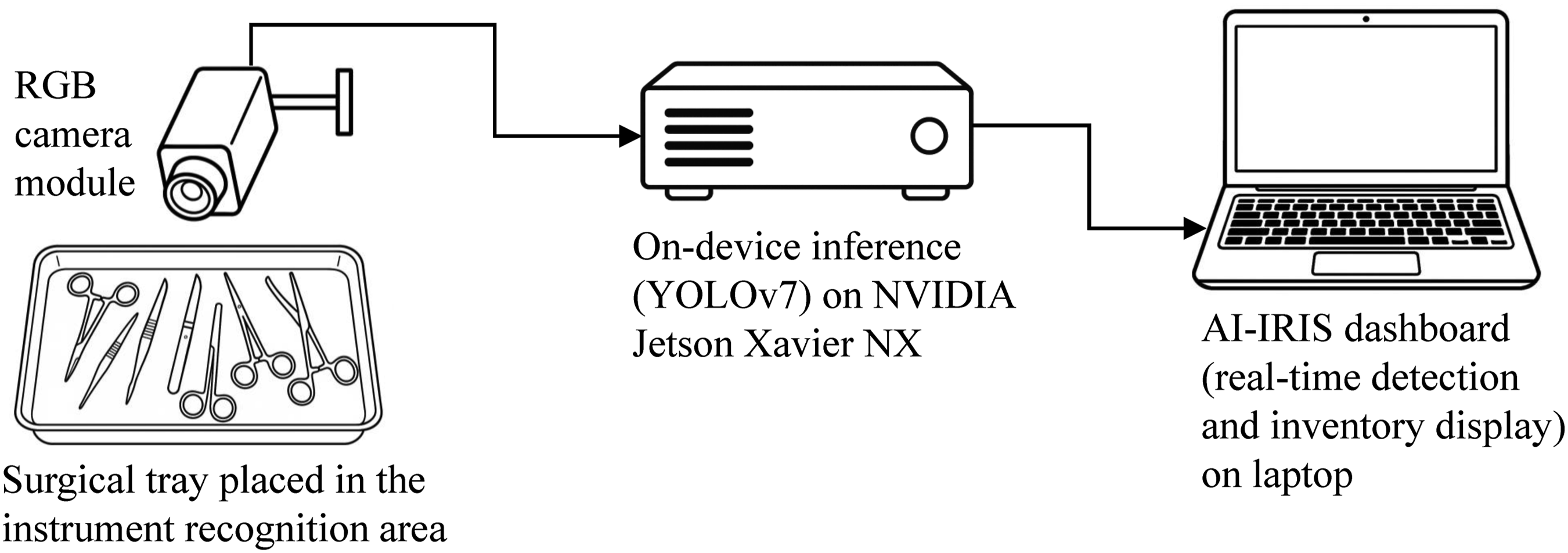
Tray images are processed by a YOLOv7-based recognition model pre-trained on 30 orthopedic surgical instruments (e.g., hemostats, scalpels, needle holders). Each instrument was photographed 200 times from different angles. Data augmentation techniques, including scaling, rotation, and cropping, were applied to improve robustness. The dataset was split in an 80:20 ratio for training and validation, yielding 8,000 test images (160 per instrument class).
In prior technical validation, most instrument classes achieved 100% precision and recall, with an overall classification accuracy of 98%. In multi-instrument testing scenarios, recall remained 100% when up to 15 instruments were simultaneously present and ranged from 98% to 99% when 20 or more instruments were placed together. The trained model was deployed on the edge device to enable rapid, offline inference during clinical testing. 20
Following image analysis, the system automatically displays recognition results. A “Recognition correct” message confirms concordance between detected and expected instruments, whereas a red “Recognition error” alert indicates missing or mismatched items, enabling immediate verification by scrub nurses.
Conventional manual counting
In the manual process (Figure 3(b)), scrub nurses transferred instruments from the operating field to the decontamination area for sorting and verification against a standardized checklist. On average, manual counting required approximately 90 seconds per tray, with duration varying by surgical complexity.
In routine clinical practice, any discrepancies or missing instruments would trigger the hospital’s count-discrepancy protocol, which includes reinspection of trays, drapes, linens, and waste or suction containers. However, in the simulated scenarios used for this study, this search protocol was not implemented because the focus was on comparing counting performance rather than discrepancy resolution.
Diffusion of Innovations Questionnaire (DOIQ)
User perceptions of AI-IRIS and CMC were assessed using the DOIQ, based on Rogers’ Diffusion of Innovations theory. 21 The 16-item instrument evaluates relative advantage, compatibility, ease of use, trialability, and observability, rated on a five-point Likert scale (“strongly disagree” to “strongly agree”). Higher scores indicate greater perceived innovation and adoption likelihood. Cronbach’s α was 0.933 for the AI-IRIS group, 0.953 for the CMC group, and 0.948 overall.
Ethical considerations
The study protocol was approved by the Research Ethics Committee of the study hospital (Approval No. 2025E01). Written informed consent was obtained from all participants, who were assured of anonymity and their right to withdraw at any time without consequence. Each participant received a NT$200 token of appreciation upon completion.
Statistical analyses
Statistical analyses were conducted using IBM SPSS Statistics version 25.0 (Armonk, NY, USA). Participant characteristics were summarized as frequencies and percentages. The Stuart-Maxwell marginal homogeneity test, an extension of the McNemar test, was utilized to compare individual DOIQ item responses between AI-IRIS and CMC.
Generalized estimating equations (GEE) with an unstructured working correlation matrix were employed to account for within-subject correlations inherent to the crossover design. An interaction term “group × sequence” was included to test for sequence effects. Adjusted marginal mean differences and 95% confidence intervals were calculated for between-method comparisons.
Results
Basic characteristics of study participants (N = 34).
Respondents’ top three perceived causes of surgical instrument counting errors.
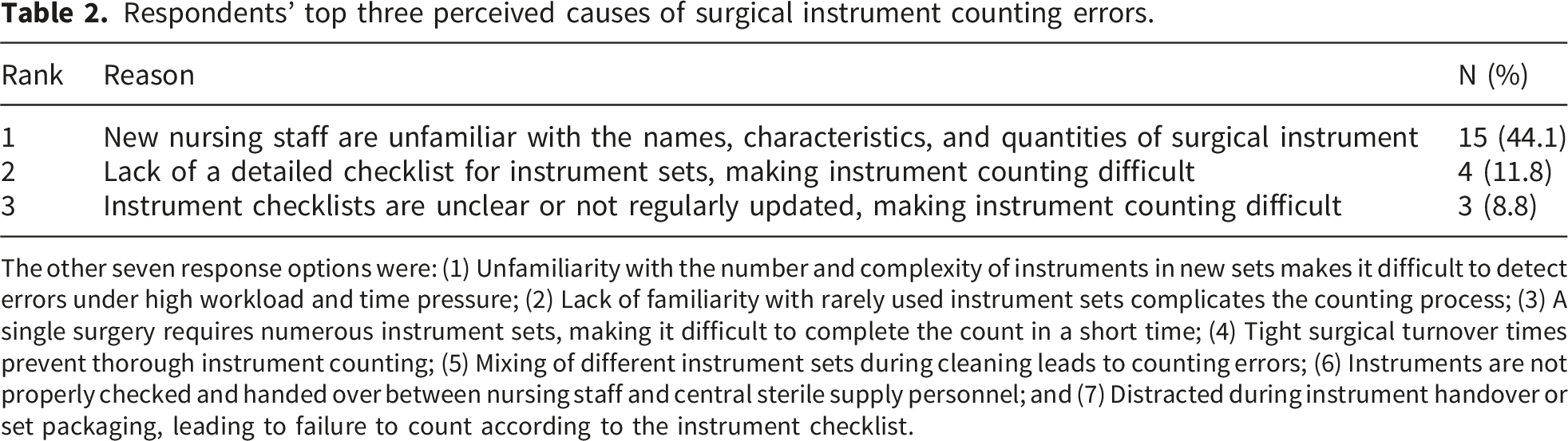
The other seven response options were: (1) Unfamiliarity with the number and complexity of instruments in new sets makes it difficult to detect errors under high workload and time pressure; (2) Lack of familiarity with rarely used instrument sets complicates the counting process; (3) A single surgery requires numerous instrument sets, making it difficult to complete the count in a short time; (4) Tight surgical turnover times prevent thorough instrument counting; (5) Mixing of different instrument sets during cleaning leads to counting errors; (6) Instruments are not properly checked and handed over between nursing staff and central sterile supply personnel; and (7) Distracted during instrument handover or set packaging, leading to failure to count according to the instrument checklist.
Comparison of counting time and Diffusion of Innovation Questionnaire scores between the Automatic Recognition & Inventory System and the manual counting method using generalized estimating equations.
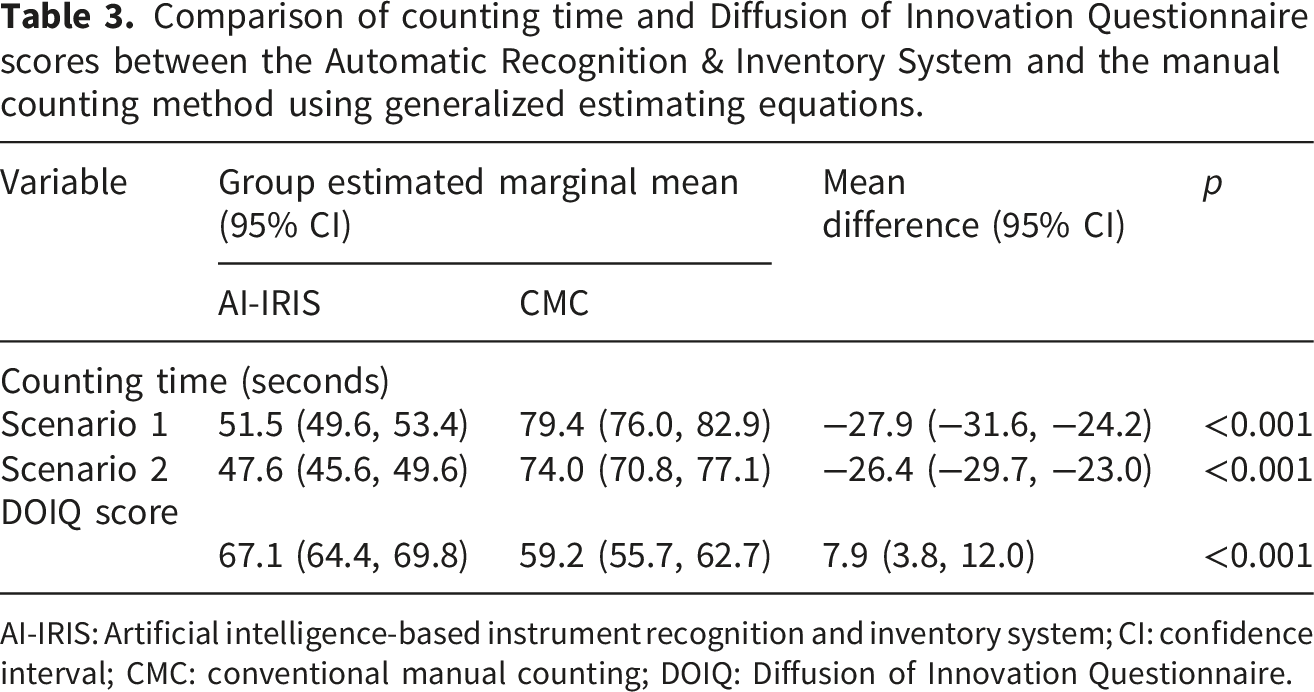
AI-IRIS: Artificial intelligence-based instrument recognition and inventory system; CI: confidence interval; CMC: conventional manual counting; DOIQ: Diffusion of Innovation Questionnaire.
The AI-IRIS also achieved significantly higher DOIQ scores, with a mean of 67.1 (95% CI: 64.4–69.8), compared to 59.2 (95% CI: 55.7–62.7) for the CMC. The mean difference was 7.9 points (95% CI: 3.8–12.0; p < 0.001). These results indicate that the AI-IRIS enhances efficiency and is also more favorably perceived by users regarding innovation adoption.
Distribution of Response of the distribution of the responses for the 16-item Diffusion of Innovation Questionnaire (DOIQ) between the artificial intelligence-based instrument recognition and inventory system and conventional manual counting groups.
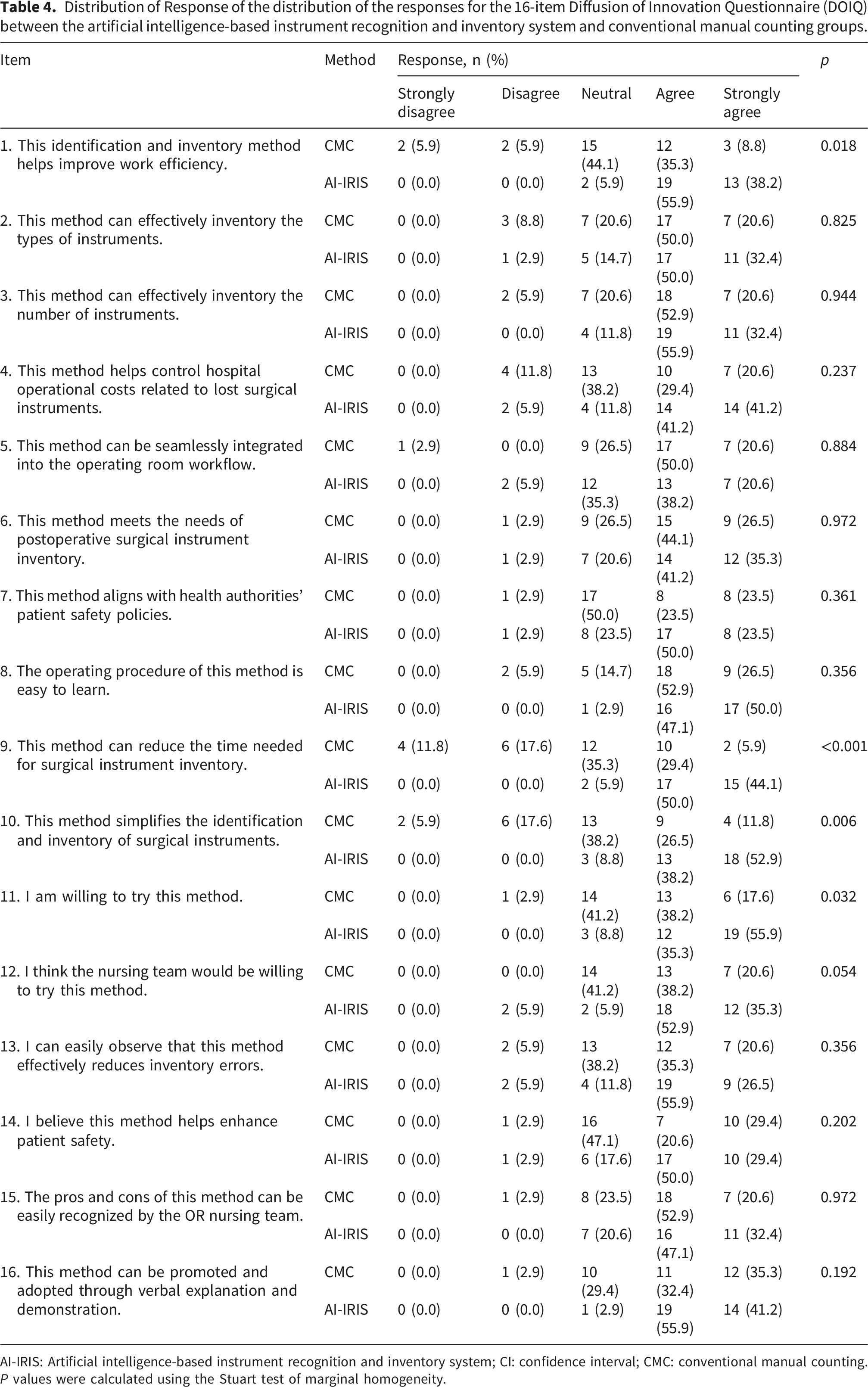
AI-IRIS: Artificial intelligence-based instrument recognition and inventory system; CI: confidence interval; CMC: conventional manual counting.
P values were calculated using the Stuart test of marginal homogeneity.
Discussion
This study demonstrated that while AI-IRIS and CMC showed equivalent accuracy in identifying and enumerating orthopedic instruments, AI-IRIS significantly outperformed CMC regarding time efficiency and user acceptance. These findings support the potential of AI-based systems to address persistent challenges in operating room workflows, including time constraints and staff workload, while aligning with patient safety practices.
The identical and perfect recognition accuracy observed for both AI-IRIS and CMC reflects a ceiling effect under the controlled study conditions. Because the simulated scenarios did not intentionally introduce counting discrepancies or challenging visual conditions, the present design does not permit assessment of comparative error detection performance. Accordingly, this study should be interpreted primarily as an evaluation of efficiency and user perception rather than evidence of superiority in identifying discrepancies under high-risk conditions. Future studies incorporating intentional mismatches or more complex visual environments are needed to evaluate system performance in error-prone scenarios.
AI-IRIS reduced counting time by approximately 27 seconds per scenario. In high-volume surgical settings, where multiple counts are conducted before, during, and after procedures, these savings could substantially improve workflow efficiency. For complex surgeries involving numerous instruments, the cumulative reduction in time could translate to meaningful improvements in operational throughput and reduced cognitive load on staff. Previous studies have identified time pressure, distractions, and fatigue as key contributors to errors in manual counting. 22 By automating this process, AI-IRIS may alleviate these factors, enabling staff to concentrate on critical perioperative tasks, such as maintaining sterility and monitoring patient status. These benefits align with broader efforts to enhance operating room efficiency through technological innovation, including robotic-assisted surgery and RFID systems.23,24
The AI-IRIS offers distinct advantages compared to RFID systems that rely on radio waves. RFID systems require each instrument to be individually tagged, which is resource-intensive and prone to limitations such as signal interference from metallic objects and damage to tags during sterilization. In contrast, the AI-IRIS uses image-based AI recognition, eliminating the need for physical tags. The system can also provide direct visual feedback, allowing surgical staff to see and confirm instrument presence in real time, which enhances accuracy and workflow efficiency. Moreover, the AI system can be further trained to assess instrument conditions, such as cleanliness or the need for sterilization. These are capabilities beyond RFID’s limited presence detection. Finally, unlike RFID, which can be disrupted by metal, optical systems remain unaffected by such interference, offering more reliable performance in complex surgical environments.
The significantly higher DOIQ scores for AI-IRIS, and item-level evidence of stronger agreement on specific advantages such as improved work efficiency, reduced inventory time, and simplified recognition processes, suggest favorable user perceptions across key domains of innovation adoption. These findings align with Rogers’ Diffusion of Innovation theory, emphasizing ease of use, compatibility with existing workflows, and observable benefits as critical factors influencing adoption. While resistance to new systems often arises from concerns about complexity or workflow disruption, 21 the positive reception of AI-IRIS, even on items related to perceived effort and team willingness, indicates that it addresses many of these barriers. This favorable pattern of responses suggests that AI-IRIS not only meets essential adoption criteria but also holds promise for broader implementation, especially with appropriate training and integration strategies. These results reinforce previous findings that healthcare professionals are more inclined to adopt AI-based tools when they improve efficiency and safety without radically changing established practices. 25
Our findings of high DOIQ scores and strong willingness to adopt AI-IRIS contrast with reports that nurses may express concerns regarding artificial intelligence integration, including apprehension about reliability, professional role displacement, and increased cognitive burden. A recent study examining perceived worries related to AI adoption among neonatal intensive care nurses, found that uncertainty regarding system trustworthiness and potential workflow disruption influenced acceptance. 26 In contrast, the favorable perceptions observed in our study may reflect the system’s clear operational benefits, minimal workflow disruption, and its role as a supportive adjunct rather than a replacement for clinical judgment. These findings suggest that perceived usefulness and compatibility with existing practice are central determinants of AI acceptance in nursing contexts.
Another noteworthy finding of this study was that the most frequently cited cause of counting errors was unfamiliarity with instrument names, characteristics, and quantities among new nursing staff. This finding indicates that knowledge gaps, rather than procedural failure alone, contribute substantially to counting discrepancies. Conventional manual counting relies heavily on individual experience and memory, making novice nurses particularly vulnerable when managing complex or unfamiliar instrument sets. By providing standardized visual identification and real-time feedback, AI-IRIS may help reinforce instrument recognition and reduce reliance on memory-based verification. In this way, the system may function not only as an efficiency-enhancing tool but also as a supplementary educational resource that supports onboarding, competency development, and sustained familiarity with instrument inventories. This dual role of workflow support and experiential learning may help address contributors to retained surgical item risk and aligns with surgical safety guidelines that emphasize continuous competency development. 7
This study also identified outdated or incomplete inventory lists as key contributors to errors (20.6%). Manual systems often struggle to remain up-to-date with frequent instrument turnover. AI-IRIS’s digital infrastructure offers opportunities for real-time inventory updates and alerts for missing or unlisted items, further streamlining surgical workflows.
Despite these strengths, the study has limitations. First, the sample was drawn from a single hospital in northern Taiwan, which may limit generalizability. Organizational culture, leadership attitudes toward innovation, and prior exposure to digital technologies may influence user perceptions and adoption readiness. In addition, all participants were female, reflecting the local operating room nursing workforce. The absence of male participants limits assessment of potential sex-based differences in technology acceptance. Perceptions of artificial intelligence, including trust in automation and willingness to adopt new technologies, may vary across demographic groups.27,28 Future multi-center studies involving more diverse samples are warranted to evaluate the consistency of these findings across institutional and demographic contexts.
Second, the identical and perfect recognition accuracy observed for both AI-IRIS and CMC was obtained under controlled, simulated conditions. The use of standardized scenarios with non-overlapping instruments and ideal lighting does not fully replicate real-world operating room environments, where instrument overlap, occlusion, variable lighting, or blood contamination may affect recognition performance. Therefore, further validation in routine clinical settings is necessary before broader implementation.
Third, the AI-IRIS model was trained on 30 orthopedic surgical instruments. Although this provided a focused proof of concept, its performance with larger, more complex instrument sets or different surgical specialties, such as cardiac or neurosurgery, remains unknown. Future research should evaluate scalability across diverse instrument categories and assess model retraining or transfer learning strategies to enhance adaptability.
Conclusion
In a simulated postoperative setting, AI-IRIS significantly improved instrument counting efficiency and was more favorably perceived by users without compromising recognition accuracy. These findings provide proof-of-concept evidence supporting its role as a workflow-support tool.
Validation in routine clinical environments is necessary to determine system performance under real-world conditions characterized by visual variability, instrument overlap, and workflow complexity. Future research should also assess scalability across diverse surgical specialties and evaluate long-term adoption, implementation barriers, and cross-cultural acceptance.
Beyond efficiency gains, AI-IRIS illustrates how image-based health informatics solutions may support the digital augmentation of perioperative nursing practice, enhance standardization, and contribute to continuous quality improvement. With continued refinement and clinical evaluation, AI-IRIS may serve as a valuable adjunct to traditional counting practices, supporting processes associated with safer and more efficient surgical care.
Supplemental material
Supplemental material - Integrating artificial intelligence into surgical nursing workflows: Evaluation of an image-based Instrument verification system
Supplemental material for Integrating artificial intelligence into surgical nursing workflows: Evaluation of an image-based Instrument verification system by Zu-Chun Lin, Hui-Chien Huang, Malcolm Koo, Yu-Ju Lin, and Tzu-Chuan Hsu in Health Informatics Journal.
Footnotes
Acknowledgments
We express sincere appreciation to Professor Wan-Jung Chang of National Kaohsiung University of Science and Technology and the Intelligent Cyber-Physical System Lab (iCPS) for providing the AI-Based Instrument Recognition and Inventory System, which enabled the successful completion of this study.
Ethical consideration
The study protocol was approved by the Research Ethics Committee of the Taiwan Adventist Hospital (2025E01) issued on February 27, 2025.
Author contributions
Zu-Chun Lin: Conceptualization, Supervision, Resources, Methodology, Investigation, Writing – original draft, Writing – review & editing. Hui-Chien Hung: Conceptualization, Data curation, Writing – original draft. Malcolm Koo: Formal analysis, Writing – review & editing. Yu-Ju Lin: Conceptualization, Data curation. Tzu-Chuan Hsu: Conceptualization, Methodology, Resources, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Taiwan Adventist Hospital through the Industry-Academia Collaboration Project (Project No. TCCTIC1122C005).
Declaration of conflicting interests
This study was investigator-initiated and was not commissioned by any external organization. The artificial intelligence-driven instrument recognition and inventory system evaluated in this study, AI-IRIS, is covered by Taiwan Patent No. I907322 and was developed by three of the authors: Tzu-Chuan Hsu, Hui-Chien Hung, and Yu-Ju Lin. The authors declare no other competing interests relevant to this work.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.