
Abstract
This paper examines how expertise is treated as a separable domain of epistemics by looking at simulated intensive care shift-handovers between resident physicians. In these handovers, medical information about a patient is transferred from an outgoing physician (OP) to an incoming physician (IP). These handovers contain different interactional activities, such as discussing the patient identifiers, giving a clinical impression, and discussing tasks and focus points. We found that with respect to (factual) knowledge about the patient, the OPs display an orientation to a knowledge imbalance, but with respect to (clinical) procedures, reasoning, and activities, they display an orientation to a knowledge balance. We use ‘expertise’ to refer to this latter type of knowledge. ‘Expertise’ differs from, and adds to, how knowledge is often treated in epistemics in that it is concerned with professional competence or ‘knowing how’. In terms of epistemics, the participants in the handovers orient to a steep epistemic or knowledge gradient when it concerns the patient, while simultaneously displaying an orientation to a horizontal expertise gradient.
Introduction
In this paper we look at simulated intensive care unit (ICU) shift-handovers between resident physicians to show the participants’ different and divergent orientations to different types of epistemic statuses. During ICU shift-handovers, medical information, responsibility, and authority over patients is transferred from a team of outgoing physicians (OPs) to incoming physicians (IPs) at the change of a shift. Central to handovers, therefore, is the transfer of knowledge between two or more handover participants. The relative epistemic access to a certain knowledge domain can vary between interactants such that one can be more knowledgeable (K+) and the other less knowledgeable (K−) (Heritage, 2010, 2012a; Heritage and Raymond, 2012). In this article we will show how OPs show an orientation to their epistemic authority with respect to knowledge about the patient, while at the same time showing an orientation to shared knowledge with respect to (clinical) procedures, reasoning, and practices. One single OP phrase in our data such as ‘we do not have troponins yet’ (excerpt 1 in analysis) may embody both an orientation to information imbalance (the IP is informed) and an orientation (‘not yet’) to shared knowledge that troponins are to be expected. Thus, in terms of interactants relative knowledge positions, while our IPs are addressed as being in a K−position with respect to knowledge of the patient, they are at the same time treated as being in an equal knowledge position with respect to medical expertise. We refer to the latter with an E for expertise, to contrast it with the K for (factual) knowledge about the patient.
The first domain of professional knowledge where we encounter the display of knowledge balance concerns (clinical) procedures such as those for diagnostics or for contacting the patient’s family. The second domain of professional knowledge is the expertise in clinical reasoning. We see this when the OP presents interpretations of findings or relates results and outcomes. The last domain of professional knowledge is the orientation to expertise on clinical practices. This concerns OP’s orientation to IP’s skills in performing specific medical activities such as taking the patient’s blood gas samples or doing an endotracheal intubation. We will call these professional knowledge domains ‘expertise’, and we aim to show how it is treated as one domain of epistemics. Similar to previous studies on expertise (e.g. Mogendorff et al., 2016; Versteeg and te Molder, 2021), we treat expertise as a form of knowledge associated with participants’ professional status. However, in our data we encounter expertise not as an orientation to knowing that but as an orientation to knowing how. Moreover, in our study the term ‘expert’ or ‘expertise’ is not used by the participants themselves but assigned by us as researchers, on the basis of their orientations to know-how based on their professional status.
Expertise as epistemics
In social interaction, we see continuous orientations of participants to the distribution of knowledge over them. We see this for example in information they provide or request (Heritage, 2012a), or in the ways in which referring practices such as names or pronouns (Sacks and Schegloff, 1979) assume shared familiarity or not. The concept of recipient design (Sacks et al., 1974), one of the fundamental characteristics of talk and social interaction, relies on these orientations (Heritage, 2013). It has even been argued that unequal distributions of information and redressing these imbalances are the engine of social interaction (Heritage, 2012b).
Indeed, in the handover encounters that we have studied, information about a patient is transferred from one physician to another up to the point when both treat the imbalance as being remedied ‘for all practical purposes’ (Garfinkel, 1967: 7). On this account, we see both participants’ orientations to the OP’s epistemic authority over the IP.
Shared knowledge of the expertise type discussed here has been referred to as ‘common ground’, being ‘the sum of the information that people assume they share’ (Clark, 2006: 85). In our analysis however, our interest is not in the ‘sum’ as this would include for example participants’ choice of language as an orientation to their mutual skills in speaking Dutch. Our analysis has focused on participants’ orientations to different types of ‘knowing how’ as manifestations of professional medical knowledge.
The idea of a distinction made between on the one hand ‘knowing that’ (i.e. ‘factual’ knowledge) and on the other hand ‘knowing how’ (i.e. practical knowledge) was discussed by Ryle (2002 [1949]) in his critique of Cartesian mind-body dualism (see also Snowdon, 2004). Although we accept his observation that shown skills and competencies cannot be reduced to underlying mental processes, we have chosen to talk about the orientations to competencies by the participants in our data in terms of orientations to ‘knowing how’. Our study aims to contribute to CA studies of epistemics by showing how participants can simultaneously orient both to information balance and to information imbalance, and by showing how participants’ concern with knowledge in recipient-designing their talk can deal not only with ‘knowing that’ but also with ‘knowing how’.
CA studies so far of epistemics in interaction have been mainly concerned with knowing that. In their introduction to the volume on the moral aspects of knowledge in conversation, Stivers et al. (2011) argue that studies have shown participants’ orientations to ‘access’ to knowledge, ‘rights’ to knowledge, and to ‘responsibilities’. Examples of access studies are Heritage (2012a) which shows that participants’ orientations to each other’s epistemic status – that is, what we believe the other to know – are responsible for treating utterances as either providing or requesting information, and Heritage (2012b) which argues that achieving equal access to information is the basis of all interaction. An example of a study of epistemic rights is Raymond and Heritage (2006) single case analysis of the tacit dispute between two friends on who has the primary rights to evaluate the behavior of children of whom one of them is the grandmother. Yet, studies of epistemics in terms of orientations to ‘knowing how’ are rare, and this paper aims to contribute this perspective to the research of epistemics in social interaction.
We will use the concept of expertise to, on the one hand, establish a relation between the three types of professional medical knowledge to which the participants in the handover encounters orient, and on the other hand to single out these orientations from the more amorphous domain of ‘common ground’. Although our use of ‘expertise’ is related to its use in studies of identity and membership categories (e.g. Versteeg and te Molder, 2021), we will treat expertise primarily as part of the domain of epistemics.
Data and method
This paper is part of a more extensive study that explores how handover participants establish intersubjectivity in simulated ICU shift-handovers (Leenstra et al., 2018). Ethical approval for the study was granted by the ERB’s of the University Medical Center Groningen (UMCG), Netherlands, and the Dutch Association for Medical Education (NVMO, #688). In total, 12 resident physicians took part in the study. They were informed by email about the study’s purpose: getting insight into how handovers are executed. They were also notified that they would not be assessed on their performance or medical know-how. The resident physicians participated in pairs of two. Every physician acted out one handover in the outgoing physician’s role and one as the incoming physician. This brought us to a total of 12 videotaped and transcribed dyadic handovers. The handovers had a duration ranging from 4 to 7 minutes. The collection of the data was done in March and April of 2017. Ten of the handovers were carried out in a vacant ICU wing and 2 at the simulation center, all of them at the UMCG. A simulated environment was chosen to satisfy the larger study’s aim to control handover conditions (e.g. maintaining equal case complexity and ambiguity) and to avoid ethical dilemmas (e.g. asking permission from the critically ill and invading the ward with cameras). An unintended but fortunate consequence of our simulated set-up is that all the handover participants were physicians in training. For our analysis, this means that we are dealing with interactants of similar professional knowledge levels.
For the handovers, we used adjusted medical cases of former ICU patients that were written down and adjusted to suit our study by a member of the ICU staff. The resident physician who first took on the OP’s role, was handed the written description of the medical case, including appendices such as lab results, EKG, and any other diagnostic information required to understand the patient’s illness trajectory. They were then given unrestricted time to study the case and were afterwards instructed to carry out the handover as close to normal as possible. The handovers were then performed at the side of a bed with a mannikin on it, attached to medication pumps, intravenous fluids, and a monitor displaying the patient’s vital signs.
We used three cameras to record the handovers, one at the head of the ‘patient’ and two at opposite sides of the bed’s foot-end. Using three angles meant we could not only observe all of the verbal interaction, but also the participants’ non-verbal conduct such as eye-gaze and head nods. Afterwards, the handovers were transcribed according to Jeffersonian (2004) conventions. For analyzing our data, we used conversation analysis (CA). One of the key-characteristics of CA is that it treats meaning as a social construct, established through interactions and any analytical observations are based upon participant’s utterances in interactions. We analyzed the data by focusing on how linguistic expressions display an orientation to shared knowledge. Therefore, we looked at both the videotapes as well as the transcripts to identify different categories, eventually leading to the three categories we will describe in detail in the analysis section. In the analysis we included the excerpts that are the most illustrative for their respective category.
Analysis
With this analysis, we want to show how the handover participants orient to a knowledge difference concerning the patient while simultaneously displaying an orientation to shared expertise. In the next paragraphs, we will show how, with respect to (factual) knowledge about the patient, the OPs display an orientation to a knowledge difference, whilst displaying an orientation to equal knowledge when it comes to (clinical) procedures, reasoning, and activities.
Orientation to expertise on procedures
One domain of professional knowledge where we see how the OP orients to a level of expertise of the IP is in his narration of the carried-out procedures. The way in which these are described by the OP, display that knowledge about these procedures is expected to be shared by the IP. These procedures may be carried out before admission at the ICU or at the ICU itself. Excerpt 1 below is from the part of the handover in which the patient’s clinical situation is explained. In this part, some of the carried out diagnostic procedures are discussed by the OP. As will become clear, this specific part shows more than one example of how certain procedures address the oriented-to expertise of the IP.
65.
66. zien= 67. 68. 69.
70. 71. 72.
73. 74.
75.
76.
In the first couple of lines of the transcript, the OP discusses an EKG (electrocardiogram) made by the emergency department, which we will go into detail about later. In line 70–75, the OP then reports on two of the carried out diagnostic procedures. He starts with ‘we do not have troponins yet’ (line 70) and continues with ‘and the blood gas [analysis] has just come in I see’ (line 72). The first one, the troponins, are a diagnostic marker for cardiac problems and the second one, the blood gas, refers to the arterial blood gas analysis and measures the oxygen and carbon dioxide levels in a patient’s blood to evaluate lung function. In contrast to the EKG in line 65, both of these diagnostic procedures are formulated using either a definite article (the blood gas) or no article at all (troponins). Both formulations implicitly suggest that these specific procedures are known, maybe even standard procedures and that they are supposed to be known by the IP as well. Also, using these words that can be seen as typical medical terminology, the OP makes both himself and his handover partner part of the group of medical professionals, thereby actively bringing about a certain expert status (Mackiewicz, 2010). This suggestion is enhanced by how the reporting on the troponins is formulated as ‘not yet’ (line 70), indicating that this is something that can be expected and thus deniable. Formulating it this way displays an orientation by the OP toward the IP’s knowledge of this specific procedure.
What we want to bring forward here is the idea that what we are dealing with is not just an orientation to epistemic knowledge as we know it. During the handover, the OP is the one that displays a K+ position: he is the one transferring the patient to the IP and the one giving the information. As seen in the excerpt, he knows and reports on the procedures that were carried out and the results that still have to come in. With respect to this, the IP is in a K− position: he is oriented to as not knowing which procedures were or were not carried out. From this orientation to knowledge imbalance, it is relevant to state the availability of the blood gas analysis (line 72) and deny the availability of troponins (line 70). But by using formulations that make it clear that specific procedures are standard – such as using a definite article or using ‘yet’ – the OP displays an orientation to a more horizontal expert status between himself and the IP. They are, so to speak, in an equal E (expert) position or status. Thus, concerning the patient, we are dealing with a steep knowledge gradient, while on the other hand, we could argue that the expertise gradient is less steep or even horizontal.
Aside from standard medical procedures, there are also more ‘practical’ procedures the handover participants treat as shared expertise. An example of this is the contacting of the patient’s family, which is often discussed at the end of the handover when they discuss the tasks and focus points of the upcoming shift. If the OP does not cover this topic by the end of the handover, it is often inquired after by the IP. Excerpt 2 below is from a handover in which the OP has not brought up the contacting of the patient’s family yet, on which the IP asks about it herself (line 190–191):
190. 191.
192.
193.
194.
195. 196.
197. 198.
199. 200. 201. 202. → 203.
In line 192 the OP answers with ‘no uhm’ upon which she wants to elaborate, but the short pause of 0.5 seconds causes overlap in which the IP asks if the patient’s wife has passed away (line 193). Earlier in the handover the OP explained how the patient was anxious for a heart attack because his wife died from one, so line 193 of the IP can be treated as a request for confirmation. We find the reaction in line 194 – ‘yes his wife passed away’ – and in lines 196–197, the OP continues with her answer on the initial question about how she has not spoken with the patient’s family yet and formulates this in terms of ‘haven’t been able to’ and ‘yet’, both indicating that it is something that is supposed to happen but which she had been prevented from. In lines 198–199 she then provides an account for why she has not, namely that she took the patient directly from the lung department and that the nurse there probably knows who the contact person for the patient is (lines 200–201). In line 202 the OP then says ‘so they have yet to be contacted’. Using both ‘so’ as well as ‘have to’ and ‘yet’, it is presented as a standard procedure to contact the family which is assumed to be known by the IP as well. In terms of knowledge of this particular patient, the IP is in a K− position: she asks if the family is contacted, while the OP shows to possess knowledge that this has not happened yet, so her knowledge status concerning the patient is higher. In terms of expert status though, we could speak of a horizontal gradient: both the OP and the IP know that it is a standard procedure to contact the family.
Orientation to expertise on clinical reasoning
The second domain of professional knowledge that the OP orients to, is clinical reasoning. During the presentation of the patient’s clinical situation, the OP not only sums up the current clinical impression of the patient but often also assesses the running treatment. Some of the utterances regarding the clinical impression are formulated as more factual, objective statements, such as when specific parameters or symptoms are discussed (e.g. line 73 and 75 in excerpt 1). In others, the OP presents impressions more analytically by interpreting findings or linking results and outcomes. In these utterances, the OP displays his/her clinical reasoning and often shows an orientation to the IP’s similar reasoning skills. By explicitly stating his/her thought processes and line of reasoning, the OP on the one hand addresses the expert status of the IP, but on the other hand formulates expertise as relevant to the interaction. Let’s take another look at excerpt 1 from paragraph 4.1 and focus on the first few lines of the transcript in which we find a reporting on an EKG (line 65–68):
65.
66. 67. → 68. 69. 70. 71.
In line 65, the OP says that the emergency department has made an EKG (electrocardiogram) before admission at the ICU. Following this, he evaluates the results in lines 66–68, which he starts by saying that the EKG did not show any apparent abnormalities (line 66). Subsequently, in lines 67–68, he adds ‘in any case no ST[-segment] elevation or negative T[-waves] or signs of myocardial ischemia’. By using the formulation ‘in any case no’, the results of the EKG are presented in a way that indicates that these three results are the main possible outcomes of an EKG and that this is expected to be known by the IP as well, thereby bringing about a shared expertise on this topic. The incoming physician responds in line 69 with the minimal response ‘hmhm’ which can be understood here as claiming good enough understanding to proceed the handover Schegloff (1982). Both physicians thus display an orientation to an equal expertise or E status, even though the sharing of the information about the EKG puts the OP in a K+ position in relation to the IP’s K− position.
Excerpt 1 showed an example of how the IP is supposed to be familiar with interpreting a type of visual result. We see these kinds of interpretation more often in our handovers, for example when the OP discusses an X-thorax, visible physical symptoms, or an EKG like in excerpt 1. Possibly an even more straightforward example of how the formulation of these kinds of interpretation can display an orientation to the expert status of the IP can be found in excerpt 3 below. This excerpt is again part of the description of the clinical situation:
56. 57. 58. 59. 60. 61. → . 62. 63. 64. 65. 66.
In the first couple of turn-constructional units (TCUs), the OP reports on a procedure that has been set into action: the monitoring of the digoxin level by the pharmacist (lines 56–58) on which the OP points out that it will probably take a while before the results will come in (lines 59–60). The TCU we want to focus on is the one in lines 61–62, in which the OP discusses a clinical observation visible on the bedside monitor which shows the patient’s vital signs. The OP says: ‘uhm hemodynamic as you can see on the monitor, he has a bit of a moderate blood pressure’. The way he formulates this, indicates that it is something that the IP is supposed to be able to see as well: ‘as you can see’ (line 61). In other words: by stating this, the OP suggests the IP can derive the same conclusion as himself from the information presented on the monitor, namely that the visible information indicates a low blood pressure, thereby both orienting to shared expertise and contributing to it. Before the handover and before the monitor was made into an interactional topic, the IP could not know about the patient’s lower blood pressure. Hence his knowledge status for this is lower than that of the OP. The expert status however, by using the formulation ‘as you can see’ is treated by the OP as equal to that of the IP.
Orientation to expertise on clinical activities
In the previous paragraph, we showed how the OP orients to the expert status of the IP in displaying certain kinds of clinical reasoning. In this paragraph, we want to elaborate on how the OP orients to the IP’s expert status when he/she talks about clinical activities. In our data, we found that the OPs discuss the implementation of specific clinical activities in ways that treat them as actions the IPs are capable of carrying out. The difference with the domains of knowledge we named in 4.1 and 4.2 is that these were about expertise on clinical reasoning or clinical knowledge. We want to show here that the OPs also display an orientation to expertise to perform medical activities. Excerpt 4 below is from almost the end of a handover, where the IP can ask questions. Just before this excerpt, the IP has asked something about the treatment plans upon which the OP starts to name some treatment options:
190. 191. 192. 193. 194. 195. 196. 197. 198. 199. 200. 201.
In lines 190–191 the OP says the IP could think about giving the patient sodium bicarbonate but argues that this is only helpful if the patient has a metabolic acidosis and that he currently does not have this (lines 193–194). The OP, therefore, presents an alternative option in line 196, namely check the patient’s blood gas analysis and that if all of that is not an option, start hemodialysis (line 199). These two options are both clinical activities, so by naming these as treatment options – and formulating it as ‘you could check’ (line 196) – the OP assumes that the IP has the competence to do this. In other words, he believes the IP has the expertise to perform these actions. As we can see, on both of these suggestions the IP gives a positive response: ‘okay’ in line 197 and ‘yes clear’ in line 200, with which he aligns with OP’s attribution of expertise. Whether or not he is actually able to do this is another question; from an interactional perspective we see an orientation to shared expertise. The clinical activities named in lines 196 and 199 display an orientation to a K+/K− position – or the OP would not have shared it in this context – whilst simultaneously displaying an orientation to a shared E position with respect to the implementation of the clinical activities.
A vital remark that should be made here is that in the discussion of clinical activities, we find an exciting interplay between deontics and epistemics. Deontic authority refers to the right to determine others’ actions (Heritage and Raymond, 2005; Stevanovic and Peräkylä, 2012). Although in our data where all participants were physicians in training there is no deontic hierarchy, the OP, by pointing out clinical activities that have to be performed by the IP, displays a high deontic stance. He is able to take this stance because he knows that the IP will be able to perform these activities. Both here and in excerpt 5 below, OP’s deontic stance shows his orientation to IP’s expert knowledge of medical activities.
Excerpt 5 shows a second example of how the OP displays an orientation to a horizontal expertise gradient when discussing clinical activities. Like the previous one, this excerpt is from the last part of the handover in which some last focus points are discussed and where is room for questions. In this fragment the OP makes some suggestions on how to proceed with the patient:
101. 102. 103. 104. 105.
With ‘sixty percent’ (line 101) the OP refers an earlier mentioned oxygen mask which had initially been set to 40%. By naming this as a possible activity, as well as the subsequently mentioned optiflow, the OP treats the IP as being capable to perform these actions, by which she displays an orientation to and brings about an equal expert status.
Conclusion and discussion
This paper aimed to show that expertise is treated as a separable domain of epistemics, concerned with professional competence or ‘knowing how’. We looked at simulated ICU shift-handovers between resident physicians who transfer information on a patient so that both physicians arrive at a point where they treat knowledge as shared ‘for all practical purposes’ (Garfinkel, 1967). In our handover interactions, the OPs always start with a relative K+ position and the IPs are oriented to as being in a K−position with respect to knowledge of the patient. However, we found that besides this orientation to unequal knowledge positions, a clear orientation to a more equal status when it comes to (clinical) procedures, reasoning, and activities. This latter domain of knowledge we refer to as expertise. In other words, in terms of participants’ relative knowledge positions, whilst our IPs are addressed as being in a K− position with respect to knowledge of this patient and treatment so far, they are also treated as being in an equal E position with respect to expertise. This orientation to the equal expert status becomes visible through turn design, such as the use of lexical markers as ‘not yet’, to describe how certain procedures are supposed to be known as standard, or ‘as you can see’ to display how it is expected that they have the same level of professional vision (Goodwin, 1994). Besides these lexical characteristics, we also found the orientation to an equal E position in the discussion of clinical activities: by saying that an action has to be or suggesting that it can be performed by the IP and by underspecifying this action, the OP orients to IP’s competence to execute this action. Subsequently, by not denying, the IP interactionally displays himself as being in this presupposed E position.
On the one hand, our paper shows how participants can simultaneously orient to both information balance and imbalance as is shown in Figure 1, and on the other hand how participants’ concern with knowledge can deal not only with ‘knowing that’ but also with ‘knowing how’. In our data, ‘knowing how’ is concerned with professional and clinical procedures, reasoning, and activities.
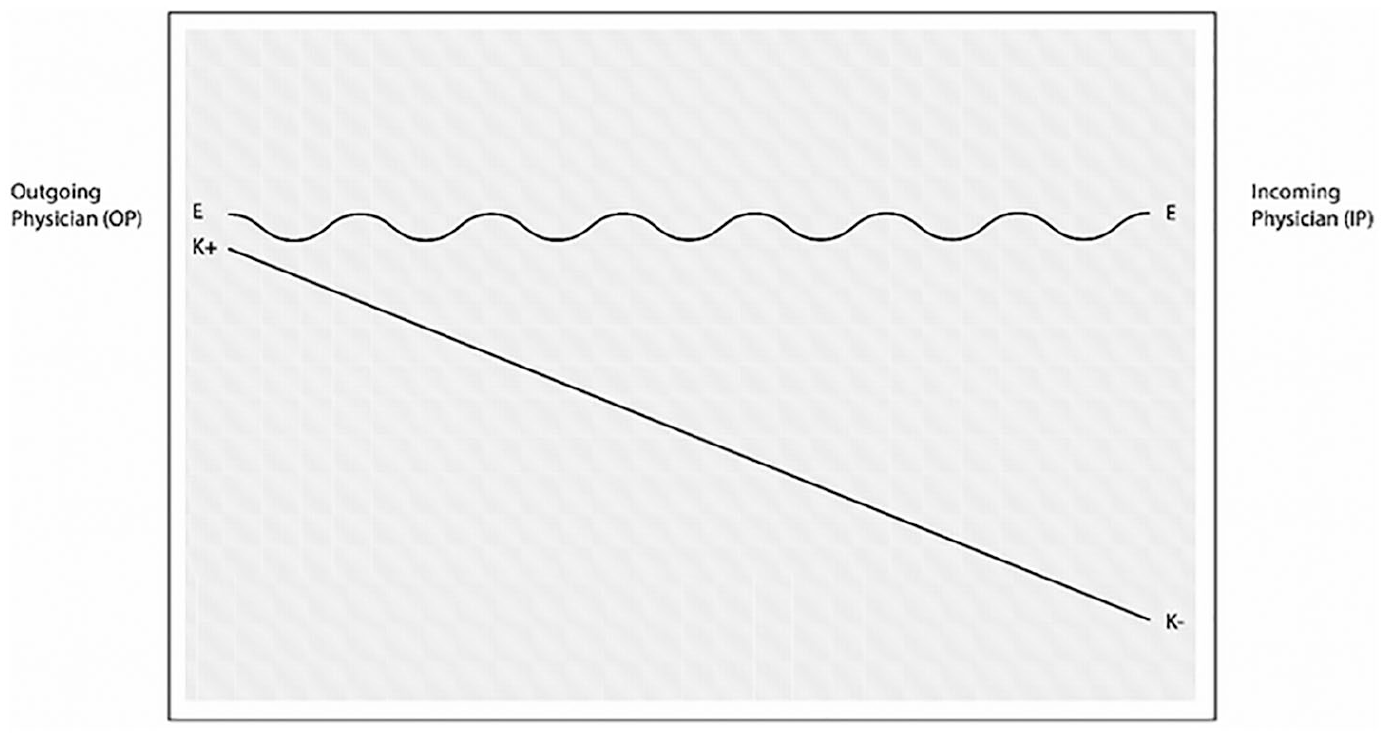
The OP’s orientation toward the IP’s epistemic and expert status.
An important observation that should be mentioned here, is the dual character of expertise when the OP displays his clinical reasoning to the IP. On the one hand, the OP shows an orientation to the IP’s similar reasoning skills, thereby addressing the IP’s expert status. On the other hand, by explicitly formulating his reasoning, the OP also renders his reasoning open for correction by the IP, thus constructing expertise as part of the interaction. Hence the representation of the balance as a wave form.
An interesting point of discussion is that in our simulated set-up, only resident physicians took part in the handovers and not experienced staff members. Not only is a handover a moment of information transfer between medical staff, but also it is used as a teaching opportunity where resident physicians learn by doing and get feedback from their supervisors and experienced staff members. In our simulated handovers, we found that we are dealing with an orientation to a steep knowledge gradient with respect to the patient and a shallower or even horizontal expertise gradient. However, we can imagine that when a handover is conducted between two participants of different educational levels, the expertise gradient might be interpreted differently. When one of the OPs in our data states a type of reasoning like ‘The patient has . . . so we gave him . . .’, we are more likely to interpret this as an orientation to the expertise they share: the horizontal expertise gradient or equal E situation. In contrast, when a more experienced physician in the role of supervisor would make the same remark, it could very well be interpreted in a way where the OP is in an E+ position while the IP is in an E− position. In other words, orientations to participants’ professional backgrounds and expert statuses can possibly be responsible for different sense-making processes.
In Figure 1 above, the line indicating the OP’s orientation to the IP’s expert status is represented as a horizontal wave line. Partly because of the non-authentic character of our data, the handover participants more or less have the same professional background, therefore we see, in our data, a strong orientation to an equal expert status. However, we do not want to claim that expertise is a phenomenon that is equal or horizontal per se. Other participants or settings could cause for more competition in this area.
Another issue, related to the previous paragraph, is how our analyses can be extended to authentic ICU shift-handovers. Real-life handovers differ from the handovers in our simulated set-up in various ways (e.g. more participants, multiple patients, duration, work pressure). Let us start of by stating that we do not want to make any significant claims about real-life handovers. Our findings are predominantly associated with the transfer of information between professionals and about expertise as a domain of epistemics. Dealing with a simulated environment means we have to be careful to make assumptions about real-life handovers. Yet, however different these interactions may be from authentic handovers, they are fully authentic as information transfer activities between professionals and since our findings are related to how information is transferred, they may still be valuable for training purposes.
Finally, we want to conclude this paper on a practical note. Recent studies on handover interaction try to answer the question how the OP and IP can increase shared understanding (Cohen et al., 2012; Manser and Foster, 2011). One of the factors that seems to cause problems, is that the OP’s have misguided assumptions regarding the IP’s expertise and understanding of disease processes which produces critical information omissions (Berger et al., 2012). Additionally, different experience levels between the handover participants has led to failures on the side of the OP regarding assessing the IP’s level of expertise and to OP’s inability to adjust the handover to the IP’s information needs (Berger et al., 2012). A first step in changing such misconceptions of the other’s expertise is to show how these conceptions take form in their mutual interaction. Our analysis has shown how participants’ orientations to expertise are made observable for each other and for us as analysts.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.