
Abstract
Adult orthodontics is now mainstream, made all the more acceptable by the advent of removable aligners. These patients may also coincidentally suffer from snoring and obstructive sleep apnoea (OSA), for which the indefinite wearing of a mandibular advancement device (MAD) during sleep may be required. Indefinite removable nocturnal orthodontic retention is now established practice.
This case report describes a cast chrome cobalt MAD and its application in the management of a patient who, having very successfully managed his snoring and mild OSA with a removable cast chrome cobalt MAD, wished to continue this management while undergoing active orthodontic treatment using removable aligners. He also wished to wear a chrome cobalt MAD to incorporate orthodontic retention and inter occlusal splinting as part of his MAD on completion of his active orthodontic treatment.
Keywords
Introduction
Adult orthodontics is now common practice, made all the more tolerable by the advent of cosmetically acceptable appliances such as removable aligners. Over the last two decades, there has been a dramatic increase in demand for treatment by adults. This demand is likely to continue and escalate with time and increased public awareness.
Following the completion of orthodontic treatment, the commitment to indefinite retention is advocated, often including the wearing of removable retainers at night (Little et al., 1988; McGuinness, 2008).
Within the adult population, one in three is thought to suffer from snoring and one in ten of these have obstructive sleep apnoea (OSA). In their survey, Lugaresi et al. (1983) found that 24% and 13% of men and women, respectively, were habitual snorers and this increased to 60% and 40%, respectively, at the ages of 60–65 years. It is therefore no surprise that adults seeking orthodontic treatment may suffer from snoring and OSA for which indefinite wearing of a mandibular advancement device (MAD) during sleep may be required.
Active orthodontic treatment, by its very nature, is protracted, often taking many months to complete. Continuous changes in tooth relations may mitigate against the wearing of conventional bulky MADs. On the one hand, the patient may wish to wear the orthodontic aligners to achieve orthodontic changes especially during the hours of sleep, while on the other they may be dependent on wearing a MAD for control of the sleep-related breathing disorder. The two requirements would appear incompatible. Similarly, having completed orthodontic treatment, the patient is faced with the choice and dilemma of wearing removable retainers or MADs during the hours of sleep.
This case report describes the management of a patient who, having very successfully managed his snoring and mild OSA with a removable cast chrome cobalt MAD, wished to continue this management while undergoing active orthodontic treatment using removable aligners. He also wished to wear a chrome cobalt MAD to incorporate orthodontic retention and inter occlusal splinting as part of his MAD on completion of his active orthodontic treatment.
Case report
A 51-year-old man was referred by an ear nose and throat specialist for non-surgical management of his problematic snoring and mild OSA. The pre-treatment Epworth Scale, described by Johns (1993), was 5 with an apnoea hypopnoea index (AHI) and a body mass index within normal limits. He had an unremarkable medical history, was a non-smoker and a social drinker.
His noise levels were intolerable to the sleeping partner resulting in separate bedroom sleeping arrangements. His main concern was resolving the intolerable snoring and mild OSA.
He initially presented with a class one incisor relationship on a class one skeletal base with imbrication and mild crowding in the upper and lower labial segments with otherwise acceptably aligned arches. There was evidence of tooth wear and possible jaw parafunction; the patient was not concerned with his malocclusion at this time. After a full examination and clinical records, a cast chrome cobalt MAD (Somnowell®) was fitted (Figure 1).
Somnowell® chrome cobalt mandibular advancement device.
Follow-up reports and survey results registered at two months after fitting the device showed cessation of snoring and a reduction in the Epworth Scale from 5 to 1 with the sleeping partner returning to the shared bedroom. This was considered a successful outcome in the management of his presenting concerns.
Approximately three years later, the patient reappeared and advised that he had commenced a course of orthodontic treatment with an orthodontic provider by means of removable aligners. The patient was concerned that during this active orthodontic treatment, he had been unable to wear his MAD and the snoring and OSA had returned with unacceptable consequences to him and his sleeping partner who were now sleeping separately again.
He therefore requested the provision of a MAD to be worn in conjunction with the ongoing orthodontic aligners. This posed the challenge of how to maintain jaw advancement using a customised and close fitting cast metal device during sleep while at the same time enabling ongoing dental tooth alignment. The potential bulk of a device being worn over a series of aligners and retention issues of such a MAD were a concern.
The initial advice was that the orthodontic treatment should be completed and then a replacement MAD be made. This was unacceptable to the patient and his sleeping partner. It was therefore agreed to provide a MAD to be worn during and in conjunction with active orthodontic treatment. The patient was informed of the need to have a further device after completion of orthodontic treatment.
With the patient’s consent, contact was made with the dentist providing the aligner treatment who advised that ongoing tooth movements were confined to the labial segments in both jaws and that the cuspids and teeth in the buccal segments were not being moved.
Records which comprised impressions, a postured bite and face bow transfer registration were taken with the patient wearing the current aligners, typically 0.75 mm in thickness.
The cast stone models were mounted on a semi-adjustable articulator and surveyed. The appliance design in the maxillary arch consisted of a major connector palatal plate. Clasps were placed in the buccal segment only and there was no labial bow (Figure 2). The fixing points for the fixed linkage Herbst piston rods were positioned buccal to the upper first permanent molars. The lower fixing points on the mandibular device were located disto buccally to the lower cuspid teeth.
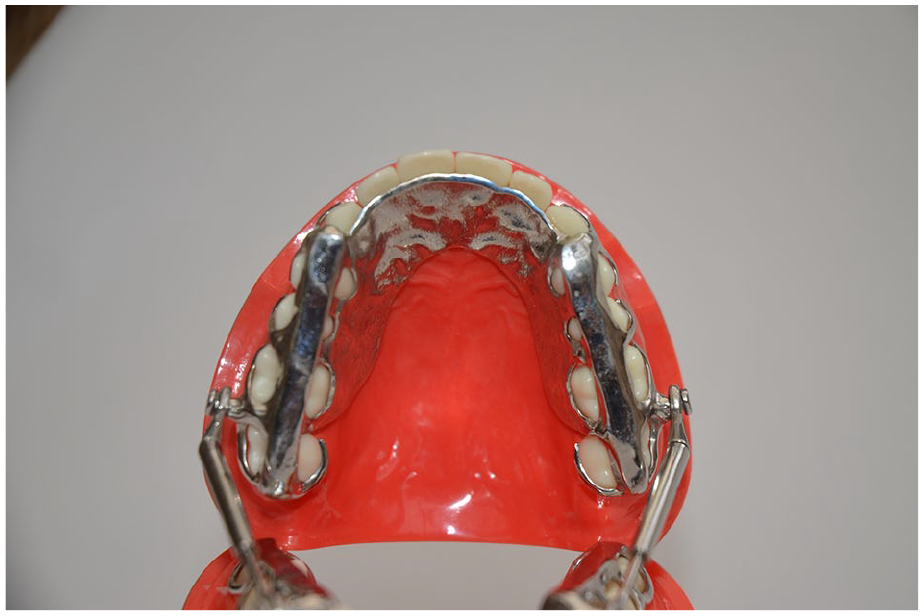
Palatal view of the maxillary device.
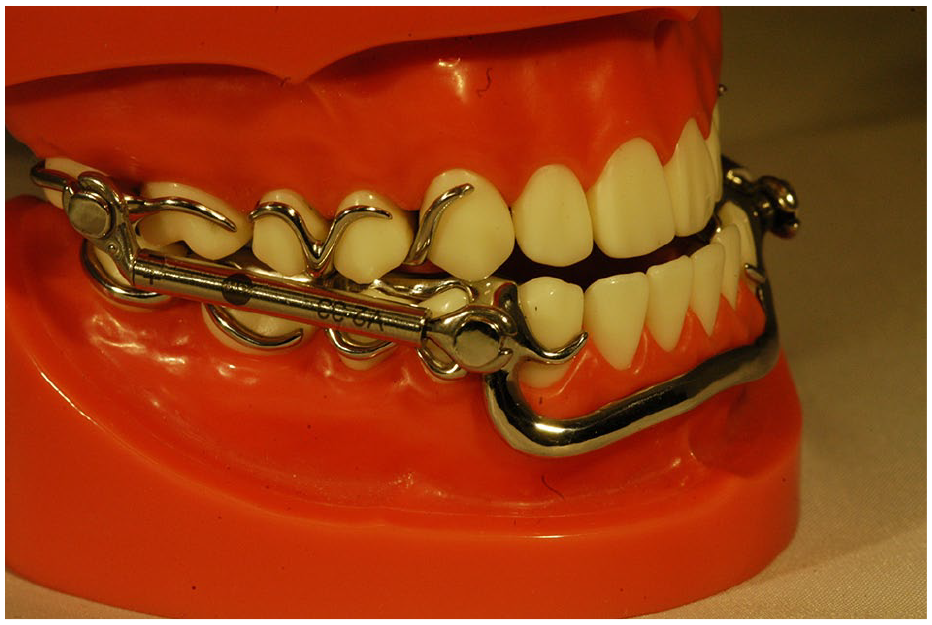
In the lower arch, the major connector was the Somnowell® labial bar placed below the outer margin of the tooth aligner in the labiomental sulcus. No lingual bar or plate was used. In this way, the MAD was kept clear of the aligner and incisor teeth in the labial segments while covering the teeth in the buccal segments. The lower device was retained by clasps in the buccal segments and the connecting occlusal plates (Figure 3). The advantages and benefits of wearing cast chrome cobalt oral devices for extended or indefinite wear have previously been described (Ash et al., 2015).

Occlusal view of the mandibular device with major connector in the labiomental sulcus.
The patient successfully wore the MAD while continuing to progress through the sequence of aligners until the orthodontic treatment was concluded. The next stage was to provide a mainly tooth-borne metal MAD which could provide orthodontic retention, distribute occlusal bite forces fairly evenly over the teeth in the buccal segments and attempt to protect the teeth from the damaging effects of nocturnal bruxism.
Further post-orthodontic treatment records were taken, which included working impressions without the vacuum formed retainers, a forward postured bite and facebow transfer registration. A replacement chrome cobalt Somnowell® device was constructed with the addition of buccal segment, occlusally balanced grind plates. In this device, close fitting cast chrome cobalt labial bows and a palatal plate to follow the palatal contour of all the upper teeth were included (Figure 4). The new device was designed to work as a MAD to hold the lower jaw forward temporarily during sleep, to provide nocturnal removable orthodontic tooth retention and provide balance buccal grinding plates to reduce the damaging effects of nocturnal bruxism and jaw parafunction by means of an inter occlusal barrier.

Somnowell® chrome cobalt mandibular advancement device with buccal grinding plates and labial bows.
Discussion
The benefit of aligner treatment is that tooth movements can be localised, leaving tooth segments unaltered; this is advantageous in constructing a customised, close-fitting, chrome cobalt device to be worn over the aligners.
The fit of the MAD used during the active orthodontics over the aligners was far from ideal. This is not surprising since the design had to be modified to fit over the 0.75-mm aligner material, with each successive aligner being slightly different. The patient also reported that the combined devices, i.e. aligners plus MAD, were a little bulky but tolerable.
A recognised risk of wearing MADs is class two intra-arch forces leading to forward pressure being applied to the lower anterior teeth possibly leading to incisor crowding, tooth imbrication and possible changes in jaw relations, these devices being derived from functional orthodontic appliances. It is postulated, yet unproven, that the Somnowell® major connector located in the labio-mental sulcus might resist the forward class two forces of the MAD by virtue of the Somnowell® bar sitting just behind the inner fibres of the mentalis muscle. Placing the lower major connector in this position has the added advantage of not encroaching on the tongue space in the oral vault, i.e. lingual and palatal sulci.
The balanced opposing buccal grinding plates are thought to confer additional strength to the device as well as distributing the opposing occlusal forces over the teeth. These also allow the patient to brux onto metal in preference to direct inter-occlusal contact between the teeth the intention is that the metal will act as a barrier to this parafunction and be damaged in preference to tooth structure.
It is recognised that the introduction of any device or prosthesis into the mouth may alter the balance of forces on the teeth, possibly giving rise to unwanted teeth and jaw movements. MADs are no exception to these unwanted side effects. It is hoped that the addition of the close-fitting labial bows, multiple clasps and the occlusally balanced buccal grinding plates within the Somnowell® MAD might limit these challenges but careful monitoring of any patient wearing these appliances is paramount.
Conclusion
The advent of removable aligners has made orthodontic treatment much more acceptable, especially for adults, some of whom may have sleep-related breathing disorders. However, the dependence on wearing a removable MAD for the management of their sleep-related breathing disorder has precluded these patients from such orthodontic treatment. This case has shown that the properties conferred by the cast chrome cobalt skeletal designed MAD can be worn in conjunction with orthodontic tooth aligners. In addition, the post-treatment MAD can include tooth-retention features, satisfying the patient with their mandibular advancement needs, and post-orthodontic tooth retention. The benefits of the aligners and of the chrome cobalt devices were found to be mutually beneficial in this case.
Footnotes
Acknowledgements
The author thanks Professor Parmjit Singh for his guidance and support. Somnowell® is a registered copyright and covered by patent.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect, to the research, authorship, and/or publication of this article: Simon Ash is the inventor of the Somnowell Chrome Cobalt mandibular advancement device.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.