
Abstract
Correcting severe tooth rotations can be challenging. There are many ways to de-rotate teeth with fixed or removable appliances. Mechanically, the best and most effective way is one that produces a two-force couple system to rotate a tooth around its centre of rotation (longitudinal axis). The aim of this article was to introduce a simple and efficient technique using a closed coil to correct localised tooth rotations in the early alignment stage, utilising a simple two-force couple system. Furthermore, some of the biomechanical principles concerning de-rotation will be revisited.
Introduction
The fourth key of Andrews’ six keys to normal occlusion is the absence of tooth rotations (Andrews, 1972). Tooth rotation can be defined as an observable (at least 20°) mesiolingual or distolingual intra-alveolar displacement of the tooth around its longitudinal axis (Proffit et al., 2006). The severity of rotations can be very subjective, although some authors attempted to classify the rotation into three groups: < 45°; 45°–90°; and > 90° (Gupta et al., 2011). The prevalence of rotated teeth in the untreated population is in the range of 2%–5% (Shpack et al., 2007). Rotations can be caused by a variety of reasons. The aetiology can be described in relation to the stage of tooth development (Parisay et al., 2014):
Rotation of permanent teeth due to pre-eruptive disturbances (injury to the primary dentition, the presence of an adjacent pathology such as cyst, tumour, odontoma and supernumerary tooth).
Rotation due to post-eruptive disturbances (habitual factors such as digit sucking, mechanical, local factors such as retained primary predecessor, or environmental factors in the form of localised crowding or spacing arising from dentoalveolar disproportion). Other environmental factors that can be associated with tooth rotation are path of tooth eruption and functional effects produced by tongue and lips.
Aims
The aim of this article was to introduce a simple, efficient and cost-effective technique using a closed coil, to correct localised tooth rotations in the early alignment stage.
This technique was initially presented at the Training Grades Group meeting of the British Orthodontic Society and subsequently at the British Orthodontic Conference in 2019.
Indications and considerations
The proposed technique is indicated in situations where orthodontic brackets cannot be bonded on the facial axis (FA) point from the outset due to the severity of rotation. Therefore, if a bracket is bonded, it will be in the incorrect position initially and will need to be repositioned at a later visit, once the rotated tooth has sufficiently de-rotated. Moreover, if a bracket can be bonded on the FA point, it would likely be difficult to fully engage the aligning archwire due to the minimal inter-bracket distance (Figure 1).

The LL5 is severely rotated to the extent that bonding an orthodontic bracket on the FA point can be challenging or impossible. Even if the bracket is successfully bonded in the correct position, full archwire engagement would not be possible.
Partial ligation of the archwire will not be effective in de-rotating a tooth given that superelasticity of the nickel titanium archwire only takes effect after significant deflection of the archwire (⩾ 2 mm). Superelasticity is the martensite-austenite phase transformations of the archwire, generated by mechanical stress (pseudoelasticity) or heat (thermoelasticity). It only exists when both phases of the alloy are present. Tonner and Waters (1994) showed that the superelastic wires have to be deflected at least 2 mm before exhibiting plateau behaviour. For example, the archwire is only partially ligated on the LL5 in Figure 1. This amount of deflection in the nickel titanium archwire is not sufficient enough to utilise the desirable pseudoelastic property; thus, the elastic behaviour (springback) and resultant tooth movement is minimal.
Another factor to consider when correcting tooth rotations is the space availability or deficiency. Rotated posterior teeth occupy more space and so correcting the rotation of these teeth would create space. On the contrary, correcting anterior tooth rotations requires space as these teeth occupy less space when rotated when compared to normally placed anterior teeth. This should be taken into account when carrying out space analysis at the treatment planning stage (Figure 2).
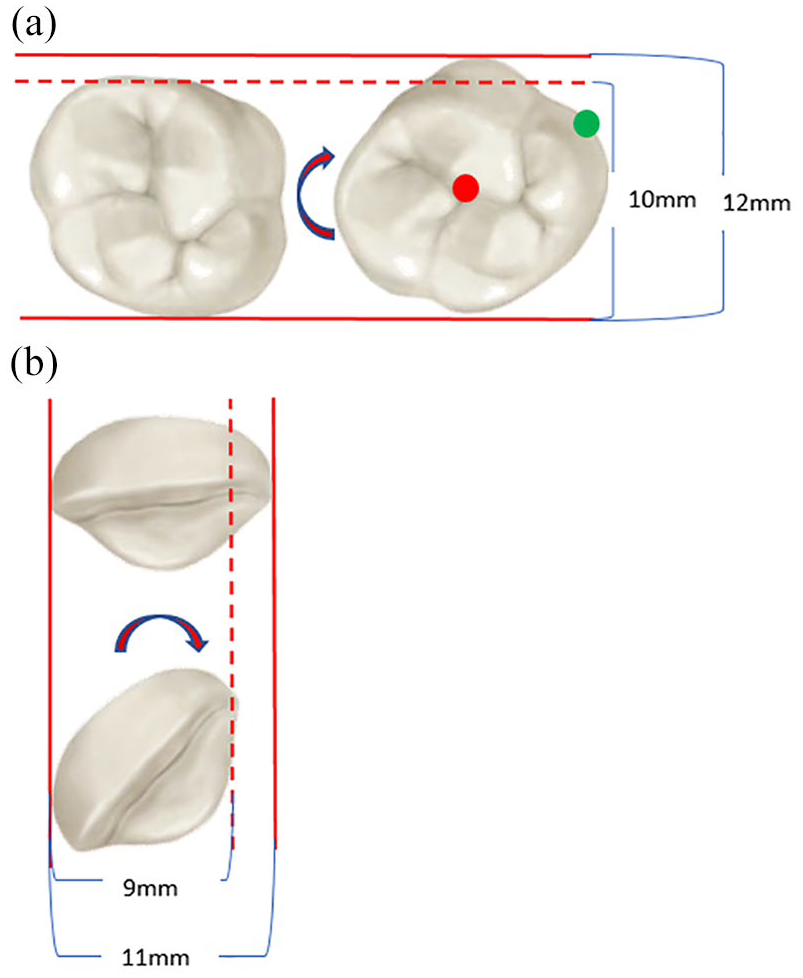
Rotated UR6 (right) occupies more space than if it was normally placed (a). De-rotation creates space (left). The same principle applies to all other posterior teeth, both maxillary and mandibular. On the other hand, de-rotating a rotated anterior tooth (UR1 in this case) requires space (b). Again, the same principle applies to all other anterior teeth, both maxillary and mandibular. Rotation around the long axis (red dot) will produce a true rotation, whereas if the tooth is rotated around any other point (for example, the green dot), tipping will be produced as well as rotational movement.
Technique
This technique involves bonding a suitable length (approximately 5 mm) of closed ‘dead’ coil on the labial/buccal surface of the tooth to be de-rotated (Figure 3). The technique can be applied by following these simple steps:
Prepare the labial/buccal surface for composite bonding. Acid etch, rinse with water, dry and apply bonding agent.
Hold the closed coil in position with a small round wire through the inner lumen (this prevents blockage of the coil with composite).
Add a thin layer of composite (flowable composite is preferable for ease of manipulation), just enough to cover the closed coil and then light cure to initiate polymerisation setting reaction.
Remove the round wire from the closed coil.
‘Thread’ the initial aligning archwire (round nickel titanium) through the closed coil and ligate the remaining teeth as normal.
From frontal view: the closed coil should be parallel and on same horizontal level as the bracket slots on either side to minimise unwanted second-order tip and first-order in–out vertical movement (Figure 4).
From occlusal view: the coil should be approximately on the mid-buccal of the tooth for maximum de-rotation effect (Figure 3).
On the second visit, the closed coil can be removed (with a bracket remover or a composite de-bond bur and handpiece). A bracket can then be bonded on the FA point to continue the alignment stage.
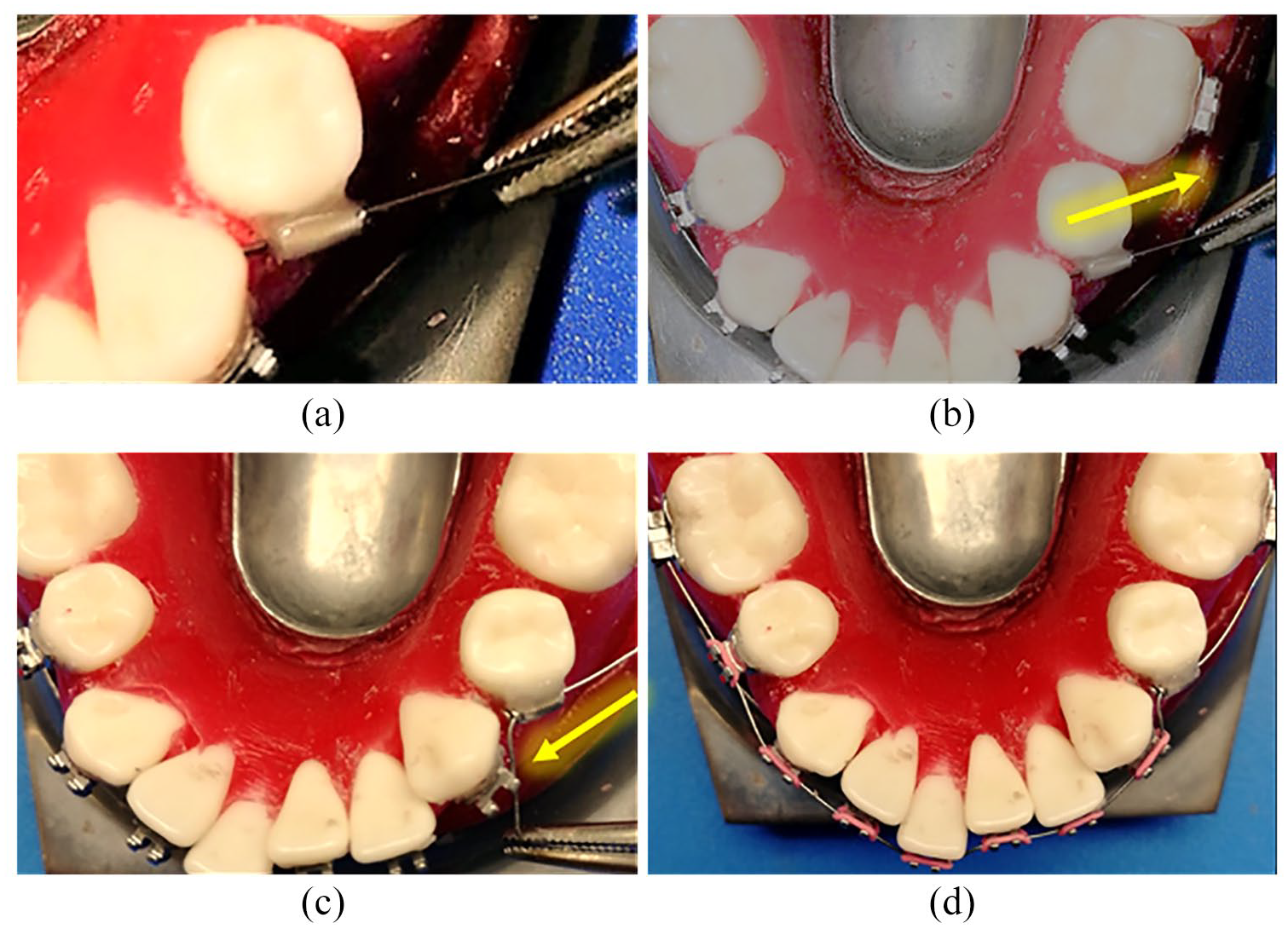
Typodont demonstration of the procedure. After preparing the buccal surface of LL5 for composite bonding, the closed coil is held in position with a round wire inserted through the inner lumen to prevent blockage (a). After light-curing the composite, the wire is simply removed (b). The initial aligning archwire (round nickel titanium) is then ‘threaded’ through (c). The remaining teeth are then ligated in the normal manner (d).

The closed coil on the buccal of LL5 is approximately parallel and on same horizontal level as the bracket slots on either side to minimise unwanted second-order tip and/or first-order in–out vertical movement.
Biomechanical considerations
In orthodontic terms, when more than one force vector is applied to a tooth, the forces are combined to determine the single overall net force. Forces produce either translation (bodily movement), rotation or indeed a combination of these movements depending on the relationship of the line of action of the force to the centre of resistance of the tooth in question. To rotate (or de-rotate) a tooth, a moment of the force (measured in newton-meters) is required, which is equal to the force magnitude multiplied by the perpendicular distance from the line of action to the centre of rotation (M=F d), where ‘M’ is the moment of force, ‘F’ is the applied force and ‘d’ is the distance from the line of force to the centre of rotation (Figure 5). There are two types of rotations in orthodontics: centric (rotation around the long axis, this produces true rotational movement); and eccentric (rotation around any other centre of rotation other than the long axis, this produces tipping as well as rotation of the tooth) (Figure 2). To produce centric rotation, a couple force system is required. The only force system that can produce pure rotation (a moment with no net force) is a couple force system. A couple force system is produced when equal and opposite forces act in the same plane of space and parallel to each other to produce moment of force. The couple force system concept can be utilised to de-rotate teeth. The technique described in this article produces a two-force couple system which is beneficial in producing maximum de-rotation effect (Figure 5).
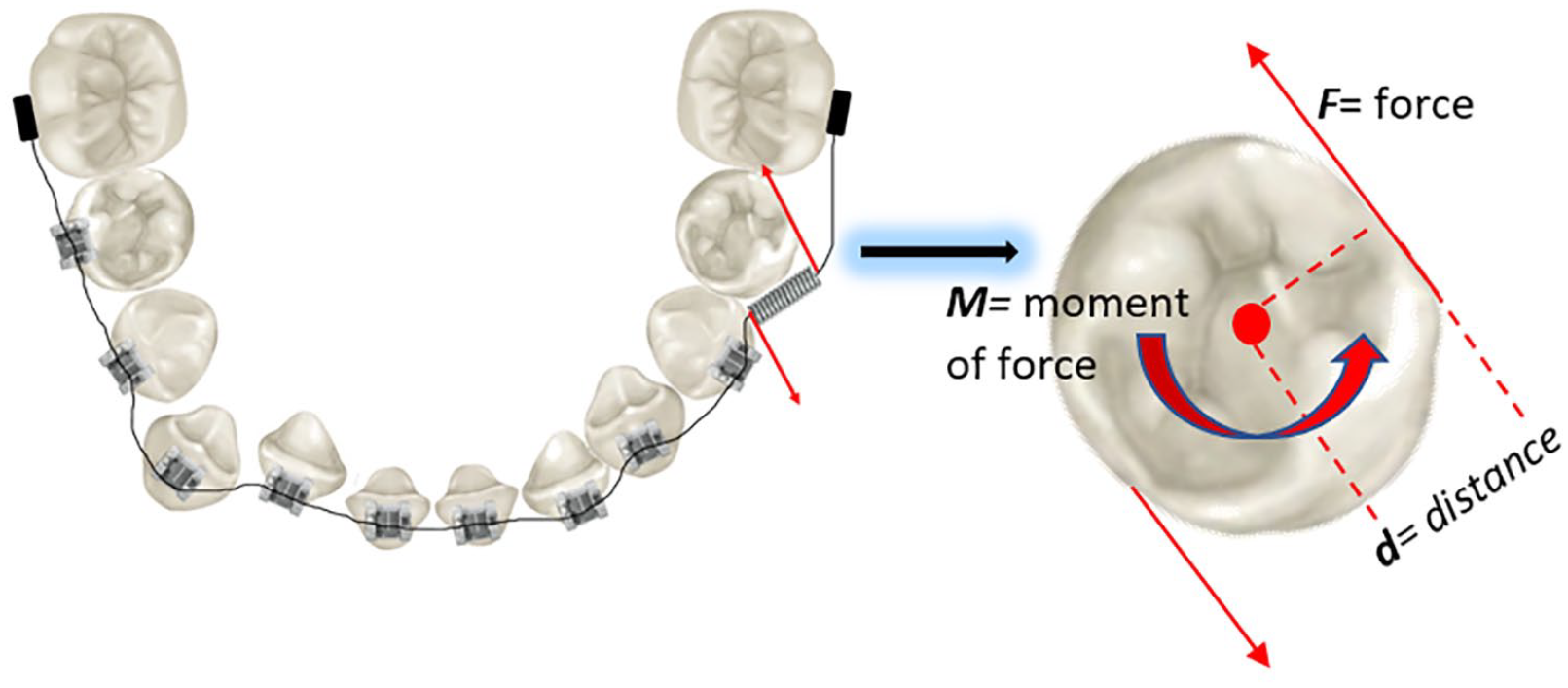
Couple force system is produced with the proposed technique, which is effective in de-rotating the tooth around its longitudinal axis.
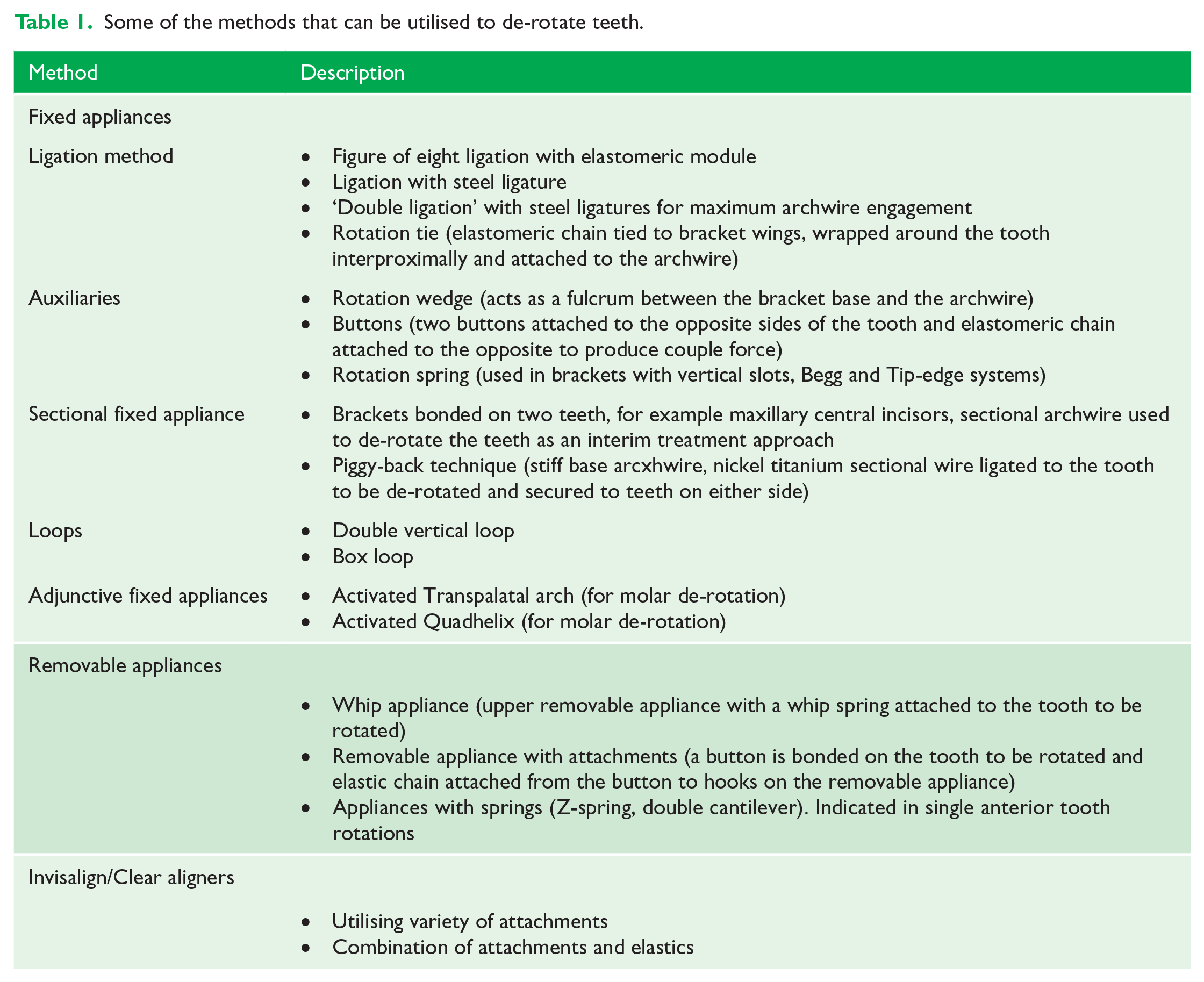
Applying the biomechanical principles above, there are variety of methods that can be utilised to correct tooth rotations (Table 1).
Some of the methods that can be utilised to de-rotate teeth.
Clinical cases
Cases 1 and 2 demonstrate the use of the technique to de-rotate the severely rotated LL5s (Figures 6 and 7). In both cases, the closed coil was bonded on the buccal surfaces of the LL5s initially, from the outset. The remaining teeth were bonded with conventional orthodontic brackets. Initial aligning archwires (0.014” nickel titanium) were ligated. After two visits, the closed coils were removed with bracket removing pliers and conventional brackets were bonded on the FA points and rectangular nickel titanium archwires were ligated fully to continue the alignment and levelling stage.
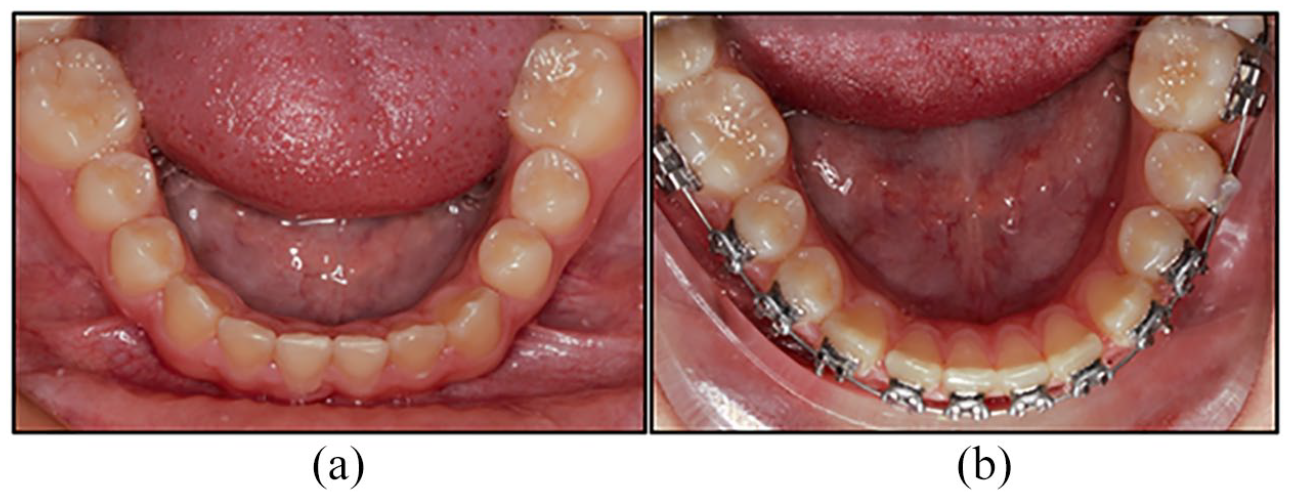
Case 1. An example of utilising the closed coil technique on a mesiolingually rotated LL5 (a). Note the improvement of LL5 rotation after one visit (b). At the following visit, the closed coil was removed and a bracket was bonded on the FA point.
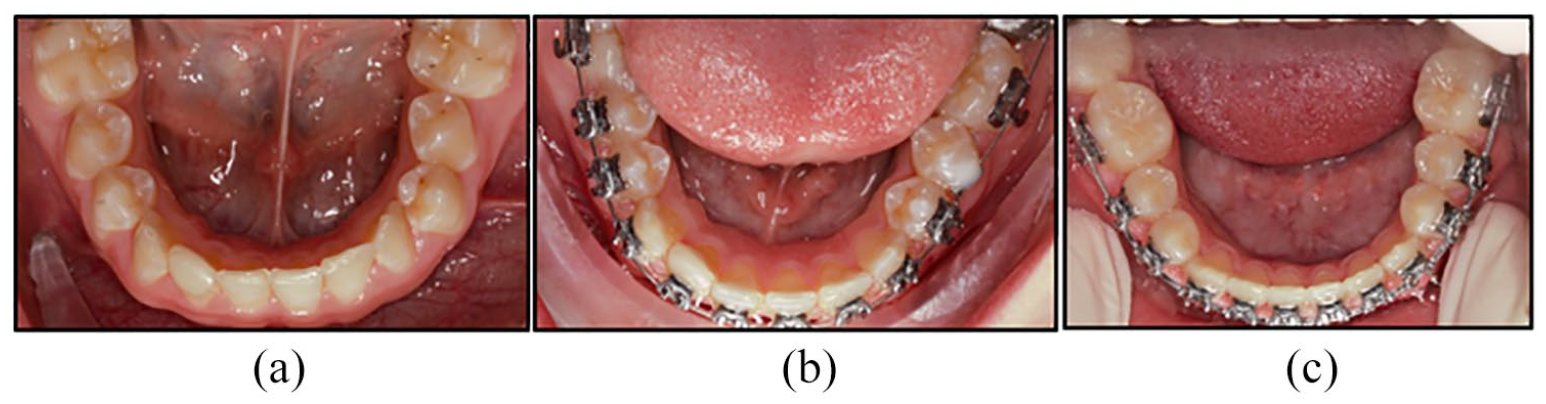
Case 2. Another example of a mesiolingually rotated LL5 (a). After one visit (b), the LL5 has de-rotated enough to allow for conventional bracket placement. At the third visit, the closed coil was removed from the LL5 with bracket remover and a bracket was bonded on the FA point with engagement of 0.017” × 0.025” nickel titanium archwire.
Case 3 demonstrates a modification of the described technique (Figure 8). Due to the severity of displacement and rotation of the LR3, the tooth was picked up with ‘piggy-back’ mechanics, to prevent distortion to the archform. A closed coil was bonded on the labial surface of the LR3 and 0.014” nickel titanium archwire was ‘threaded’ through the closed coil and ligated to the brackets on either side over a main base arch wire (0.018” stainless steel) to maintain archform and prevent uncontrolled tooth movements.
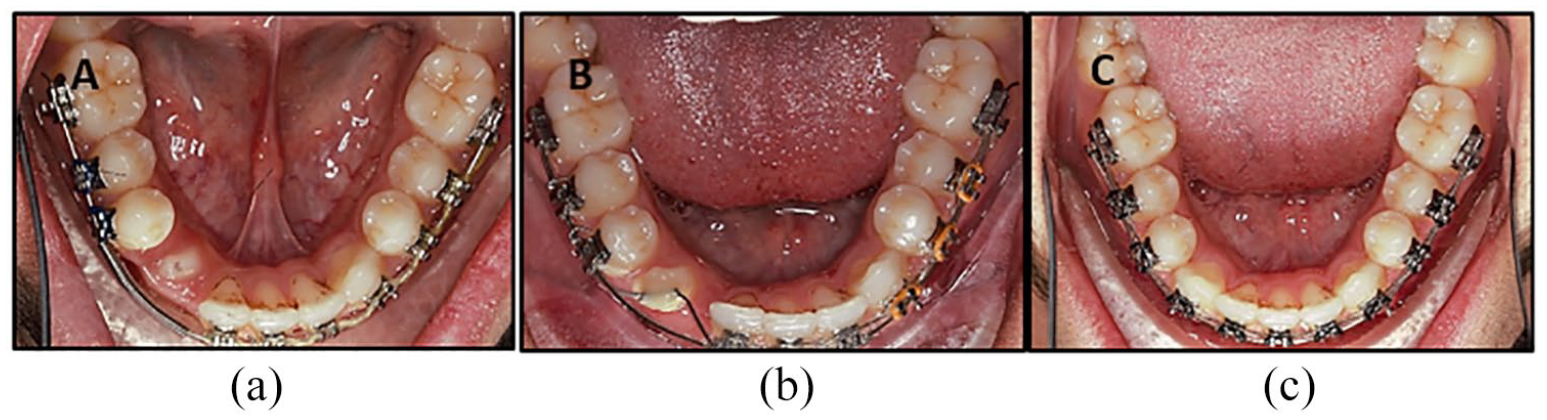
Case 3. LR3 was picked up with ‘piggy-back’ mechanics. A closed coil was bonded on the labial of LR3 and 0.014” nickel titanium archwire was threaded through the closed coil and ligated to brackets on either side over a main base archwire (0.018” stainless steel).
Ideal clinical scenario for maximum benefit
For this technique to be as effective and simple as possible, the following factors should be considered:
No more than one tooth to be corrected at a time (de-rotated). Otherwise this procedure can be more technique sensitive.
The technique is most effective when utilised in cases where it is not possible to bond a bracket on the FA point at the first appointment at initial bonding due to the severity of the rotation.
Cost-effectiveness
One of the major advantages of the proposed technique is the cost-effectiveness, if utilised in the right clinical scenario. Below are the average prices of the closed coil and alternatives (the prices are average market values in the United Kingdom as of March 2020).
Conventional metal bracket: approximately £2.
Self-ligating bracket: approximately £9.
Closed coil: approximately £10 (supplied as a 5-m spool), Therefore, a 5-mm piece of closed coil costs approximately £0.01.
Relapse and retention considerations
Correction of rotations is considered to be one of the less stable orthodontic movements; therefore, rotational relapse should be prevented accordingly. Reitan (1967) demonstrated that reorganisation of the gingival and periodontal tissues occurs after orthodontic tooth movement. The tissues of the periodontal apparatus remodel and undergo reorganisation to the new position of the tooth. While collagen fibres in the periodontal ligament take 3–4 months to remodel, the gingival fibres take slightly longer, approximately six months. The collagen transeptal fibres (supra crestal) can take up to one year to remodel. The latter fibres are thought to be the main cause for rotational relapse. This has important implications in terms of teeth that have been de-rotated as part of the overall treatment (Alkadhimi and Sharif, 2019).
The following are some of the principles that should be considered when correcting rotations in order to reduce rotational relapse and improve stability:
Overcorrection: Particularly in severe cases, overcorrection is advised if some degree of rotation relapse is anticipated, for example in patients that are expected to be less compliant with retainer wear.
Early correction: This is indicated for two reasons: (1) to allow the transeptal fibres enough time to remodel, as described above; and (2) the transeptal fibres do not develop until the cemento-enamel junction of the developing tooth overpasses the alveolar process. Therefore, early correction allows development of the transeptal fibres in a normal anatomic relationship (Kusters et al., 1991).
Accepting the rotation: In certain clinical scenarios, accepting rotations might be the preferred option, for instance a premolar that is rotated 180° around its long axis is best accepted to avoid any future rotational relapse.
Circumferential supracrestal fibrotomy (CSF): CSF, or pericision, was first described by Edwards (1970) to reduce post-retention relapse of de-rotated teeth. Edwards originally described the procedure as beneficial in teeth that have been rotated by > 30° during treatment (Edwards, 1970). CSF can be undertaken in the conventional way with a surgical scalpel to transect the gingival fibres or by using laser. Ideally, this procedure should be carried out a few weeks before removal of the fixed orthodontic appliances so that the tooth/teeth remain in the corrected position during the healing phase. In 1988, Edwards reported on the findings from a prospective study, in which it was shown that the incisors in the CSF group has less rotational relapse after 4–6 years into the retention phase (Edwards, 1988). Importantly, there was no loss of epithelial attachment in the CSF group when compared to the control group. Although the above findings seemed promising, there is still a need for high-quality clinical trials to investigate the long-term effects. A Cochrane systematic review in 2006 included data from two trials that looked into the effects of CSF (Edwards, 1988; Taner, 2000) and concluded that there was ‘weak unreliable evidence’ that there was a statistically significant increase in stability in both the mandibular and maxillary anterior segments when the CSF was used.
Long-term retention: As with most orthodontic tooth movements, prevention of rotational relapse relies on continuous retainer wear (or maintenance of the fixed retainers). The British Orthodontic Society encourages patients to adhere to life-long orthodontic retention in order to maintain tooth alignment. It is generally accepted that patients should be encouraged to wear retainers, at least on a part-time basis, for as long as they want the teeth to remain well aligned.
Vacuum/pressure formed retainer: When compared to other types of removable retainers (Hawley or Begg), vacuum formed retainers can be more effective at maintaining correction of rotations due to their wraparound effect around individual teeth. Rowland et al. (2007) found that vacuum formed retainers were more effective than Hawley retainers at holding the correction of mandibular and maxillary anterior teeth (mean difference of 0.25–0.56 mm).
Reshaping the interdental contact points: This applies mainly to anterior teeth, mandibular anteriors, in particular. It is believed that broken contact points are risk factors for later crowding and relapse. Interdental stripping producing near parallel sides may therefore be associated with greater stability than triangular teeth (Peck and Peck, 1972). Tuverson (1980) advocated reshaping the contact points to make them larger to improve stability. Nevertheless, recent randomised controlled trials found no significant difference in terms of stability between teeth treated with interdental stripping and other retention strategies (Edman Tynelius et al., 2010, 2013, 2015).
Conclusion
The technique described in this article is simple, cost-effective and versatile and can be utilised for early correction of severe localised rotations in situations where an orthodontic bracket cannot be placed on the FA point from the outset due to severity of rotation. De-rotated teeth have a strong tendency to rotational relapse; therefore, retention is of paramount importance and considerations should be given to overcorrection and long-term retention.
Footnotes
Acknowledgements
The author(s) thank Helen Travess, Giles Kidner, and Aneel Jaisinghani for their advice and guidance.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.