
Abstract
In 2020, we experienced the largest disruption to normal life recorded in recent years with the COVID-19 global pandemic. Creative thinking was required to ensure patient care was maintained. In this article, we share a service evaluation and experiences dealing with the crisis through using a virtual office approach with video conferencing to manage emergency consultations, treatment reviews, new patient and multidisciplinary clinics in a hospital orthodontic unit.
Introduction
COVID-19 was declared a global pandemic on 11 March 2020 by the World Health Organization (WHO, 2020). On 25 March, the Chief Dental Officer for England advised that ‘all routine, non-urgent dental care including orthodontics should be stopped’ (NHS England, 2020). This instruction was guided by evidence that aerosol-generating procedures performed in the dental setting result in the production of airborne particles which could contribute to the transmission of COVID-19, and also to limit movement of people (British Orthodontic Society [BOS], 2020a, Harrel and Mollinari, 2004).
Connecting remotely with patients is not a new concept, the term ‘teledentistry’ was used as early as 1997 and was defined as the use of video conferencing to diagnose and provide advice about treatment over a distance (Jampani et al., 2011). Currently, the term e-dentistry has been used. In 2002, 58% of UK orthodontic consultants were interested in providing an electronic diagnostic service for general dental practitioners (GDPs) (Stephens and Cook, 2002). E-dentistry has been shown to be effective and a randomised controlled trial on a store-and-forward system of emailed clinical photographs concluded that decisions on accepting referrals based on this information were similar to that of face-to-face (F2F) appointments (Mandall et al., 2005a). Multiple studies have outlined that e-dentistry is a useful tool for reaching out to rural communities, such as the Scottish Highlands and Islands, where access to specialist care is limited (Berndt et al., 2008, Scuffham and Steed, 2002).
Two distinct approaches to e-dentistry have been described: to store and forward images or text; or to use real-time communications such as video consultations (Irving et al., 2018). In recent years, the development of high-quality consumer cameras and fast Internet has allowed video calls to become routine. Despite technological advances, many barriers halted widespread use and continued development of e-dentistry (Table 1).
Barriers to the uptake of teledentistry in the UK before the COVID-19 crisis.
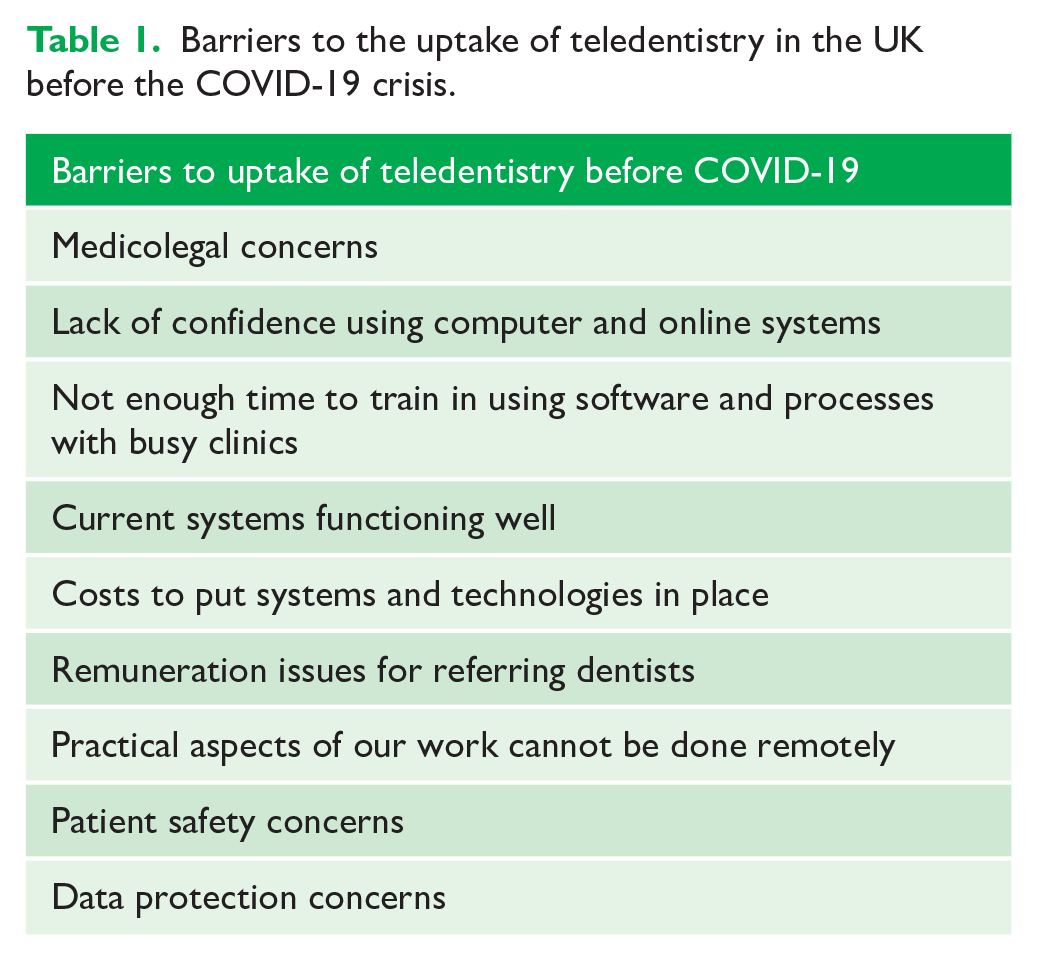
The COVID-19 crisis created a sudden obstacle to F2F treatment and e-dentistry offered an option to maintain patient care. The Information Commissioners Office (ICO) released guidance regarding remote working due to COVID-19 and compliance with data protection regulations were relaxed (ICO, 2020). Often, large organisations such as the NHS adapt slowly to innovation; however, the impending crisis accelerated the development of novel solutions. This article discusses a service evaluation of remote e-dentistry clinics set up by a hospital orthodontic department during the pandemic and aimed to determine which e-dentistry services were most effective and to consider how e-dentistry services could be effectively incorporated into future provision of orthodontic care.
Materials and methods
Before the UK government announced the lockdown and routine dental activity ceased, the authors considered delivering care remotely. A secure virtual clinical system, Attend Anywhere (AA), already used by NHS Scotland, was available. Other video consultation software is available; however, AA was Trust-approved, readily accessible and already had training available via YouTube videos. Remote access to our dental electronic referral system (DeRS) was arranged by Rego Vantage, which allowed viewing of referrals with attached images from the referrer. Remote access to AA and DeRS software were implemented within two days.
Electronic records are preferred in an e-dentistry service; however, these were not available at the Trust. A digital workflow was established using home computers for remote access to the CITRIX desktop or a virtual professional network. This allowed access to the Patient Administration System (PAS) to make further appointments and code clinics, and to the Picture Archiving and Communication System (PACS) to view digital images. One author (EC) did not have remote CITRIX access; therefore, before e-dentistry clinics, digital images were sent securely and outcomes were communicated to the administration team via NHS mail to be entered into PAS. EC used a 14” laptop (ASUS) for AA and NHS Mail; this was linked to a 27” monitor to view digital images concurrently during the consultation. The second author (NGT) used an iMac (27”) for AA, DeRS and NHS Mail, and a Trust laptop (Dell) linked to a 24” HP monitor to access PAS/PACS. Correspondence with secretaries via secure NHS mail ensured patients could still receive correspondence after their appointments. Personal mobile phones (141 was used to withhold personal phone numbers) were used as a backup for telephone communication if there were connection issues with AA; they were not used for video calls.
Initially, only emergency consultations were conducted. However, the AA software proved to be successful and within days new patient (NP) clinics, treatment reviews and multidisciplinary team (MDT) clinics were also set up. The e-dentistry model used a combination of the two approaches described for e-dentistry: real-time video consultations with the patient, alongside the adjunct of digital records to aid the consultation and decision making (Irving et al., 2018).
Emergency consultations
Before COVID-19, patients telephoned the department to arrange a F2F emergency appointment. A new protocol was developed for patients with problems during lockdown (Figure 1). A generic departmental NHS email address allowed patients to contact the department in the event that staff were not on site to answer the telephone. The email address was communicated to patients through the answerphone message and Trust website. Patients were encouraged to take photos themselves to aid diagnosis and to send the photos via the secure email address (BOS, 2020b). The inbox was checked daily by secretaries working remotely. An emergency rota was organised, with one clinician responsible for emergencies each day.
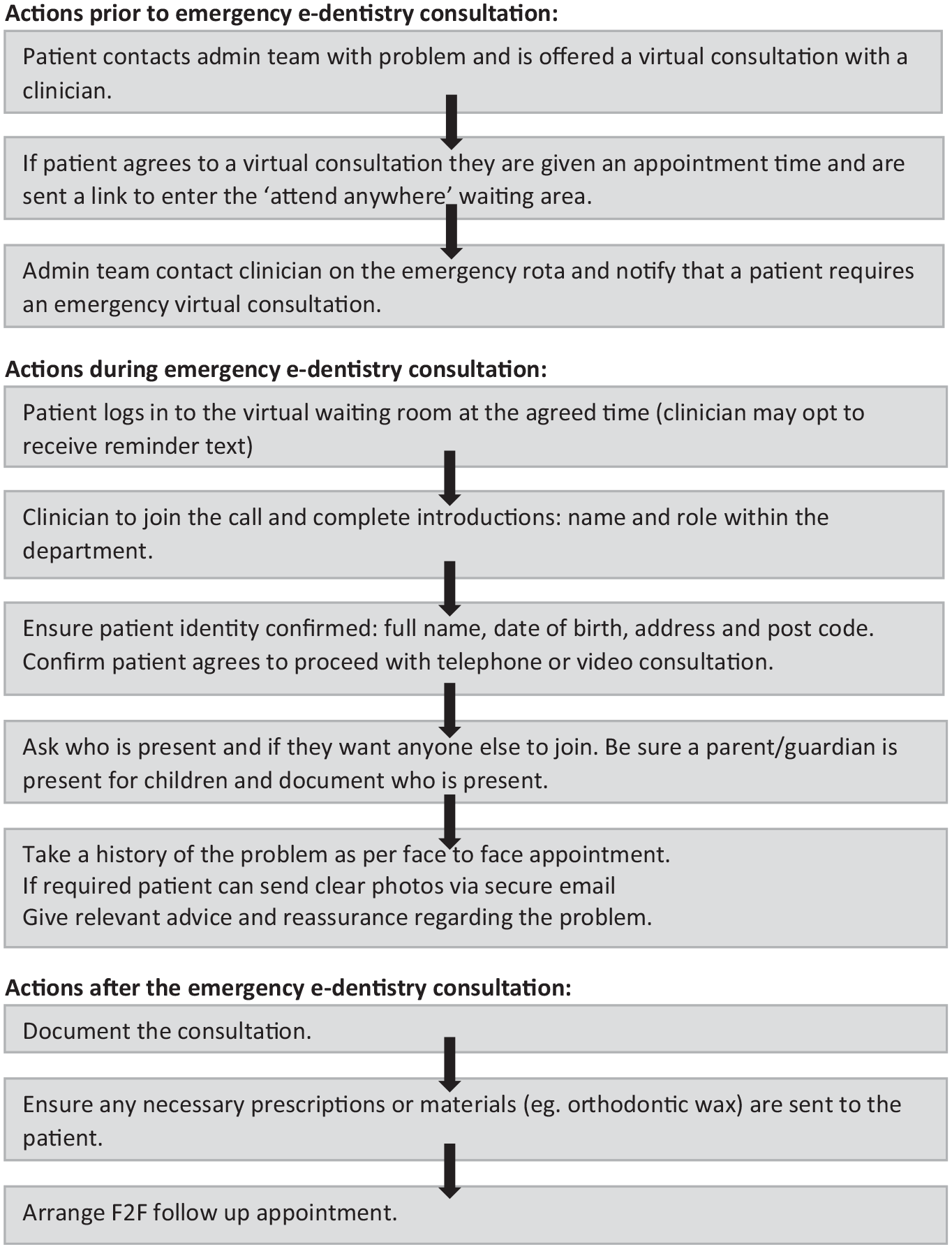
The process for an emergency e-dentistry consultation during the COVID-19 crisis.
New patient and multidisciplinary team clinics
NP and MDT Clinics continued remotely throughout the COVID-19 crisis, if comprehensive referral records (including photographs and radiographs) were available. The protocol developed for managing these clinics remotely is shown in Figure 2. If additional diagnostics or a clinical examination was required, a F2F appointment was arranged for a post-COVID-19 clinic. It was always explained to the patient that the opinion given at the video consultation may be revised after a F2F examination and this was documented on the correspondence. Inappropriate referrals were triaged and returned to the referrer.
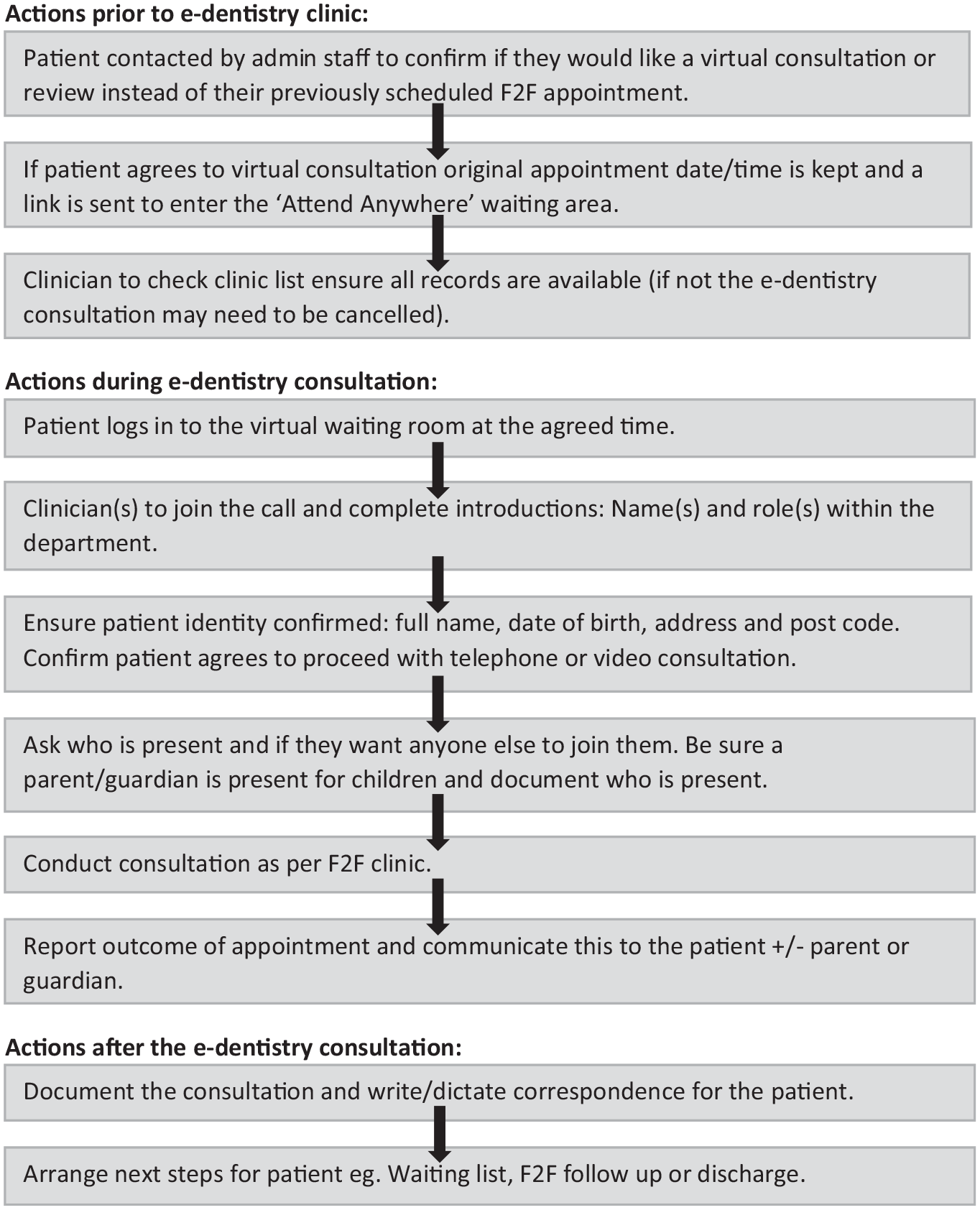
The process for a treatment review/new patient/multidisciplinary team e-dentistry consultation during the COVID-19 crisis.
Treatment review clinics
Treatment review clinics supported patients, reassured them that help was available and advised about the new emergency protocols (Figure 1). Oral hygiene and diet advice were given to maintain dental health. However, fixed appliance care is clearly limited with e-dentistry.
Service evaluation
Data were collected prospectively for the first 300 cases seen between 24 March and 19 May 2020 on the fully remote e-dentistry clinics for two clinicians, one consultant and one senior registrar. All patients who requested emergency advice during the crisis and those who had F2F clinics (NP, MDT, growth/eruption reviews, retainer reviews and treatment reviews) planned before COVID-19 were instead invited for an AA consultation and were included in this service evaluation. Seven other clinicians within the department also provided e-dentistry and telephone services during the crisis but did not have the facilities to work fully remotely using AA; therefore, these data were excluded.
Patient demographics (age and gender) were recorded. Each e-dentistry consultation had an outcome recorded as follows: follow-up as normal; added to waiting list; MDT review appointment booked; declined e-dentistry consultation; discharged; F2F required for next appointment; or did not attend (DNA). It was also recorded if patients sent additional photographs taken themselves to aid the e-dentistry consultation.
Whether the outcome was satisfactory or not was also recorded. A satisfactory outcome for the e-dentistry consultation was defined as an outcome that would have been no different to that of a F2F appointment. This includes the categories of follow-up as normal and added to waiting list. An unsatisfactory outcome was recorded if additional diagnostics or clinical examination was required or a F2F appointment was arranged for the post-COVID-19 clinic. Data were recorded and analysed using a Microsoft Excel database.
Results
The results include the first 300 fully remote e-dentistry consultations provided by two clinicians. One clinician (senior registrar) carried out treatment reviews and emergency consultations, and one clinician (consultant) also conducted NP, review and MDT clinics.
The average patient age was 14.7 years (age range = 6–64 years), 51% were female and 49% were male. Of the patients, 97% accepted an e-dentistry consultation while a small number (3%) declined (Table 3). The usual departmental did not attend (DNA) rate and the e-dentistry DNA rate was 9%. Overall, the e-dentistry system was well received by patients and parents/guardians, who felt supported by the guidance and reassurance from clinicians.
The clinics with the most satisfactory outcomes were retainer reviews, growth/eruption reviews and MDT consultations (Table 2). All emergency consultations and the majority of treatment reviews had an unsatisfactory outcome. NP or MDT consultations required a full set of records for a satisfactory outcome. Records were easily accessed remotely but were not always comprehensive and further imaging was indicated for these cases; this was more common for NP clinics.
Percentage of satisfactory outcomes by e-dentistry clinic type.
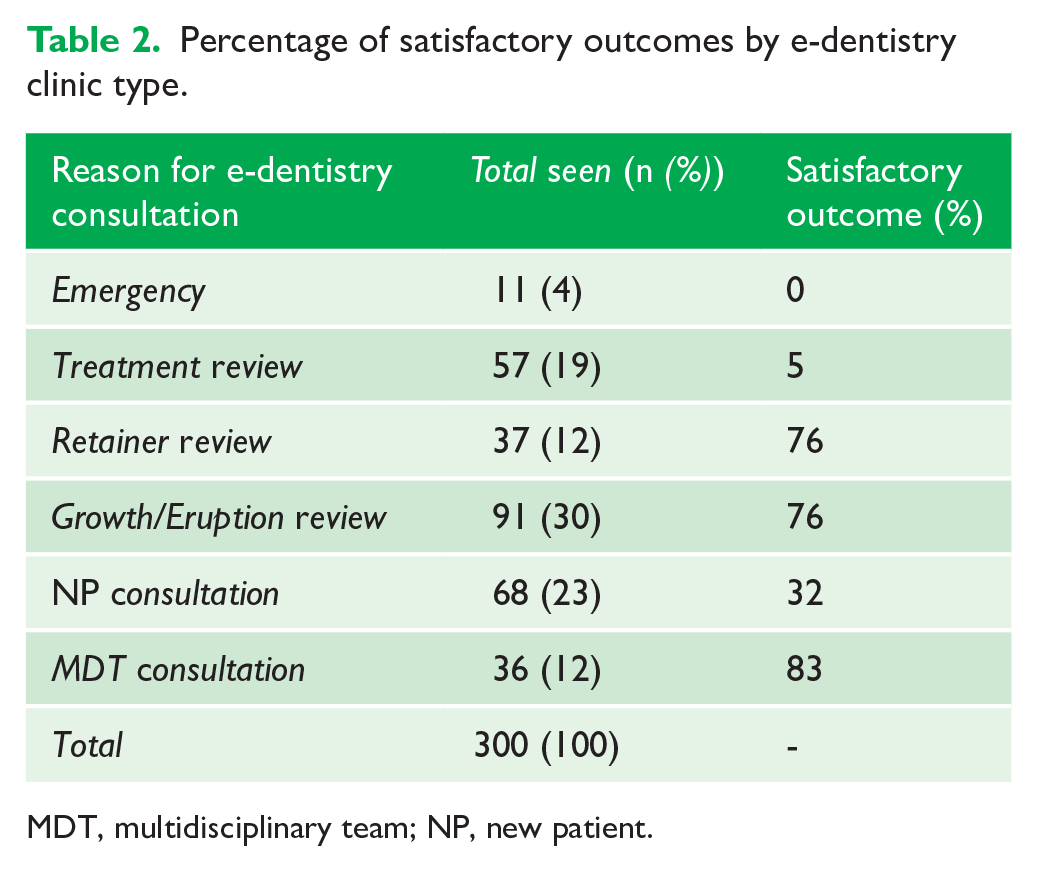
MDT, multidisciplinary team; NP, new patient.
Of the patients, 42% were either seen for follow-up as would have been planned if the consultation had been F2F or added to treatment waiting lists (Table 3). A F2F appointment was required for the next consultation for 37% of patients, due to either need for practical treatment or incomplete records to enable decision making (Table 3). Only 3% were added to treatment waiting lists and a small number of patients (2%) were discharged. Of the patients, 8% successfully provided additional photographs to aid the outcome of the e-dentistry consultation.
E-dentistry consultations and outcomes clinics during the COVID-19 crisis.
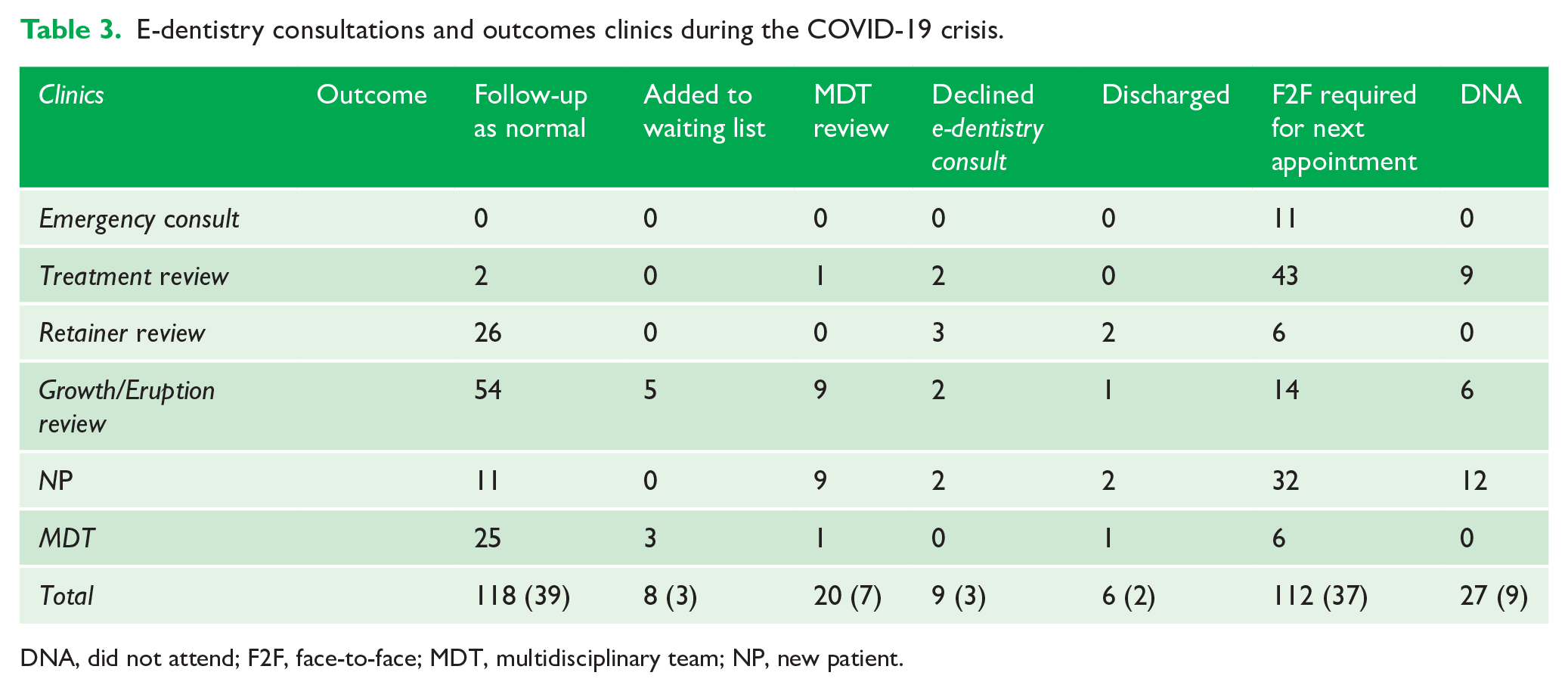
DNA, did not attend; F2F, face-to-face; MDT, multidisciplinary team; NP, new patient.
Discussion
Creating a remote e-dentistry service during the COVID-19 crisis required teamwork and management support. Access to resources already available decreased disruption to patient care and enabled some continuation of patient flow. The satisfactory outcomes from e-dentistry consultations helped save valuable F2F appointments after COVID-19. While urgent concerns were successfully managed for the interim period, practical treatment was essential and a F2F follow-up was always required. This was also the case for treatment reviews; the satisfactory outcomes seen were for those with functional or removable appliances as they were able to continue active treatment. Therefore, the outcomes from e-dentistry clinics will vary for clinicians depending on the type of treatments within their caseload.
Satisfactory outcomes for NP or MDT e-dentistry consultations required good quality patient records. MDT patients had often previously attended the department for initial assessment and thus full records were available. Fewer satisfactory outcomes were observed for NP clinics as referrers do not always have facilities for the necessary imaging, such as lateral cephalometrics or cone beam computed tomography scans. Success of a future e-dentistry service would rely on comprehensive referrals and support from referrers. Research in 2005 found that GDPs generally supported e-dentistry for NP orthodontic referrals; however, they were concerned about the costs, increased surgery time and appropriate remuneration (Mandall et al., 2005b). However, the majority of referrals to the department are tertiary referrals from orthodontists who often have the facilities to take comprehensive records. Communication with referrers is required to address referral issues and requirements, alongside robust triaging, to aid a successful referral process for e-dentistry clinics moving forward.
To incorporate e-dentistry services into future orthodontic practice requires appropriate selection of patients to ensure efficiency and increase satisfactory outcomes. The data from the service evaluation help develop a targeted approach to booking e-dentistry clinics, to include the most effective clinic types: retainer reviews; some removable appliance reviews; growth/eruption reviews; and MDT consultations. If comprehensive records are not available for NP or MDT consultations, a F2F appointment would be more appropriate. Emergency consultations and fixed appliance reviews that demand practical treatment must remain as F2F consultations. Carefully identifying specific consultations will help ensure the most effective use of e-dentistry and F2F clinical time.
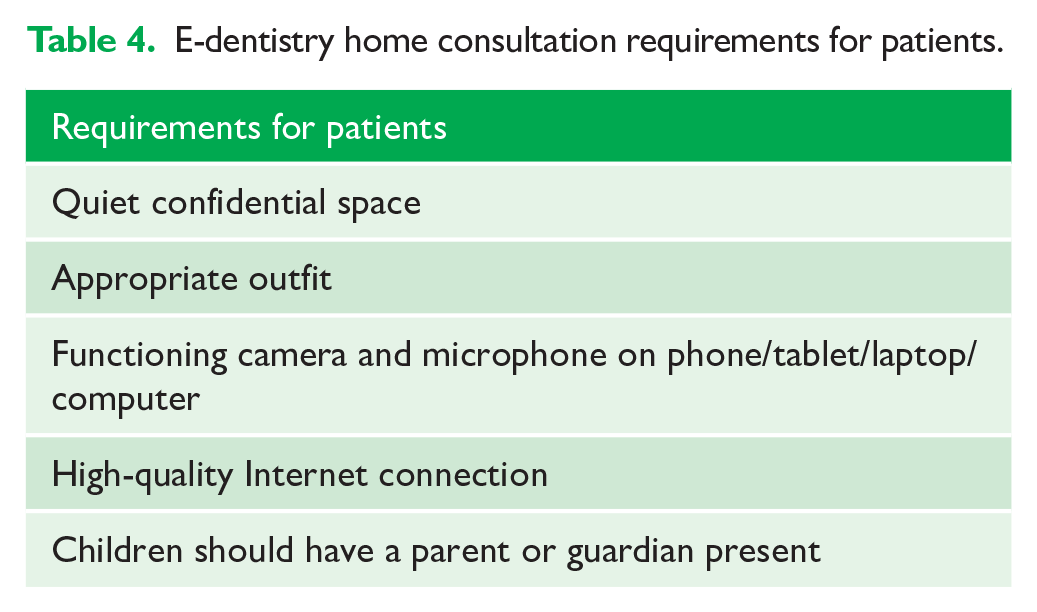
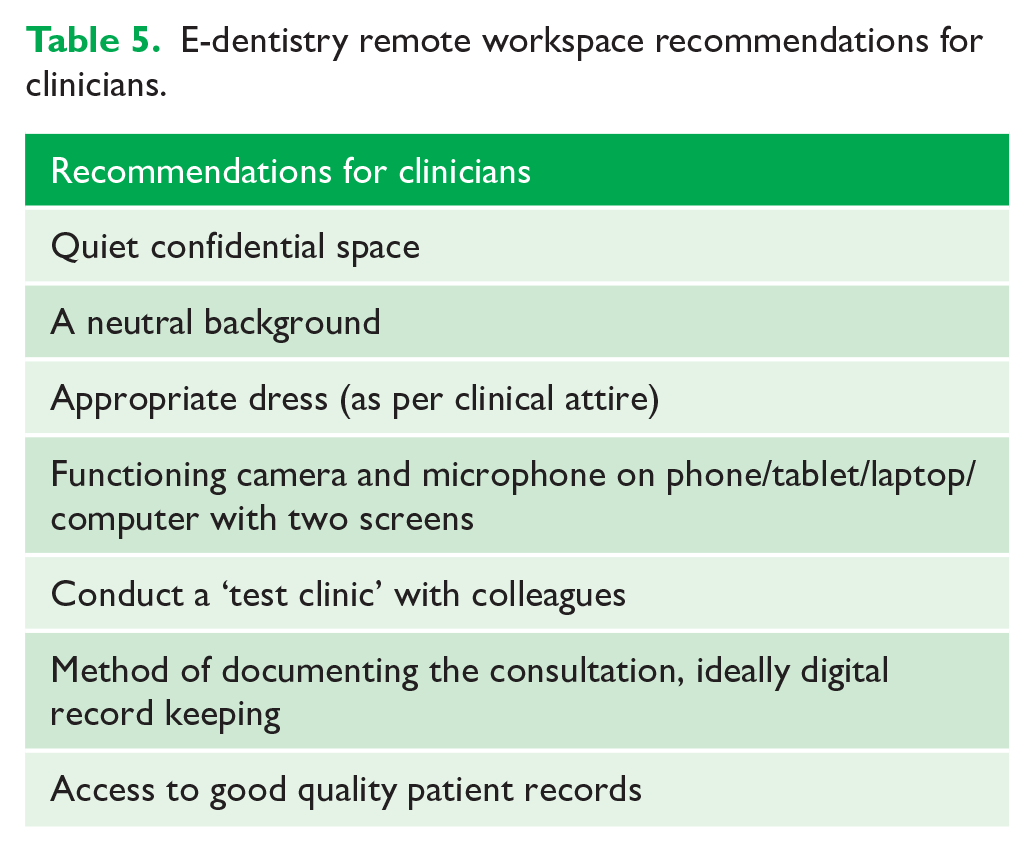
The authors found several practical factors influenced the running of e-dentistry clinics (Tables 4 and 5). It is important to maintain identical standards and a professional approach that would apply to a F2F consultation (Dental Protection, 2015). A quiet space, including a neutral background, free from interruptions is essential to maintain information governance standards. Two screens help view multiple programmes, such as the patient consultation and digital records simultaneously. It is also important to note that not all personal computers (e.g. Apple) can support remote access to Trust applications unless they can run in a browser, as they are often designed for use on a PC. Fully digital patient records would streamline data transmission for e-dentistry clinics; additional administration for clinicians and administrative staff was required to ensure availability of all records in this study. A good quality Internet connection is essential and the majority of the UK households (93%) had access to the Internet in 2019, with 84% of adults using the Internet via a mobile phone, smartphone, laptop, tablet or handheld device (Office for National Statistics, 2019).
E-dentistry home consultation requirements for patients.
E-dentistry remote workspace recommendations for clinicians.
The present study did not evaluate the quality and connectivity of each e-dentistry consultation. There were some notable connection outages during the service evaluation as the use of AA software grew more popular throughout the crisis. Initially AA was hosted by NHS Scotland (Grampian) and became exhausted by the increased utilisation; therefore, a transfer to new servers in England was arranged in March 2020. AA lost connectivity again on 19 May and 10 June 2020, due to the server’s inability to service a further increase in demand. The AA team communicated well with clinicians throughout these incidents and worked swiftly to correct the problems; no major disruptions to the clinics were experienced. Two of the remote e-dentistry clinics were affected by this outage and patients affected were telephoned to inform them of the issues and appointments were held at a later time than planned.
In 2014, Daniel and Kumar (2014) suggested that a good quality e-dentistry assessment could be carried out using an iPhone4S. Since then, technology has improved; the latest iPhone11 camera is 12 megapixels, compared to 1.2 megapixels for the iPhone4S (Apple, 2020). When required, patients in this study successfully sent photographs to aid the e-dentistry consultation; the British Orthodontic Society instructional videos helped the patients prepare good records of their dentition (BOS, 2020b). In future, patient information packs on the e-dentistry consultation requirements would be a useful resource.
This article evaluated a fully remote e-dentistry service with both patient and clinician(s) delivering a service from their own homes. Previous research has assessed e-dentistry services set up within hospital and general practice settings. A study in the USA investigated an e-dentistry service for patients in areas with limited access to specialist care; GDPs used intraoral cameras to portray high-quality real-time video imaging to specialist clinicians (Berndt et al., 2008). Another study set up specific e-dentistry clinics in rural areas for patients, ensuring the quiet environment and decreased travel commitments for the patient (Friction and Chen, 2009).
It was beyond the scope of this service evaluation to fully examine the cost-effectiveness of this e-dentistry service. The initial set-up costs for the department were low, as the team worked remotely, and the AA software was already available to the Trust. E-dentistry is often thought of as a cost-efficient way of providing services with savings reported as especially beneficial for remote communities whose patients can avoid having to travel long distances for consultations (Berndt et al., 2008; Estai et al., 2018; Scuffham and Steed, 2002). The cost of setting up an e-dentistry clinic was quoted at £25,000 (in 2006–2007); however, this is a very outdated figure (Bradley et al., 2009). Further research into the cost-effectiveness of running current e-dentistry clinics would be ideal to assess the feasibility of providing these clinics after COVID-19.
Patient satisfaction was not assessed by the authors during this service evaluation as the Trust planned a survey for patients across all specialties using AA, which was carried out in June 2020. Unfortunately, it was not possible to extract the data exclusively for the orthodontic patients seen. A total of 547 patients completed a short questionnaire after their AA consultation and 95% of patients felt there were advantages to e-consultation. The top advantages were: saved time (78%); shorter wait for appointment (65%); saved money (56%); and reduced environmental impact (50%). The majority of patients rated their experience of using the video consultation software with the highest score as very good (60%) or good (20%) and felt they could communicate effectively with their clinician. Most patients were able to access the video platform without assistance (89%) and the majority (98%) stated they would be happy to use AA for future appointments. While these data are not fully applicable to the patients included in this service evaluation, it gives insight that there was high satisfaction overall for the use of AA within the Trust. Assessing patient satisfaction would be useful to include in a future service evaluation for e-dentistry orthodontic patients.
This service evaluation is heavily biased to cases selected during the pandemic rather than carrying out a randomised controlled trial. The appointment protocols were set up quickly and specifically to maintain a service that had been prevented from providing F2F consultations. However, useful conclusions are possible from the 300 consecutive consultations and information is presented to identify which cases can be seen effectively using a video-conferenced approach. It was not possible to assess training through e-dentistry clinics as registrars were redeployed for much of the time. E-dentistry clinics and their role in training should be assessed with future research. The authors accept the limitations of this service evaluation; however, they believe that the findings present a good starting point for e-dentistry in the future.
E-dentistry allowed maintenance of the orthodontic service but was limited regarding active treatment as adjustment of appliances and patient interaction is required for the majority of orthodontic care. However, the ability to assess patients in their own homes when active interventions are not required offers convenience, avoids travel, reduces pressure on car parking and improves safety of medically compromised groups, which are important considerations for any clinical service. A change in clinical practice was forced upon the dental profession at very short notice and e-dentistry offered an opportunity to explore different ways to deliver an orthodontic service. E-dentistry has the potential to enhance traditional clinical services.
Conclusions
E-dentistry can deliver good outcomes in selected clinics.
E-dentistry is not the solution to deliver a full service as orthodontic treatment demands practical treatment.
Further investigation is required to establish how targeted case selection for different clinics may improve the effectiveness of e-dentistry.
Supplemental Material
EDentistryMainDocumentFinal – Supplemental material for The effective use of an e-dentistry service during the COVID-19 crisis
Supplemental material, EDentistryMainDocumentFinal for The effective use of an e-dentistry service during the COVID-19 crisis by Elizabeth Crawford and Nigel Taylor in Journal of Orthodontics
Footnotes
Acknowledgements
The authors thank those who helped set up the e-dentistry service: Sharon Osterfield and Richard Civil (Royal Surrey Transformation team) and Mike Singer (CEO Vantage Health). Edward Taylor for helping with excel data analysis. And those who contributed to the running of the e-dentistry service: the nursing team, administration team and secretaries in the Orthodontic Unit at the Royal Surrey County Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.