
Abstract
The importance of psychological support for orthognathic patients has taken an increasing precedence over recent years and is embedded in orthognathic commissioning guidelines. Furthermore, attention towards mental health-related conditions and their management is of prime importance and continues to be a key area of focus within healthcare settings. With this in mind, this paper aims to outline our experience of establishing a need for and subsequently securing funding to establish a clinical psychology service within an existing orthognathic service in the NHS. The information outlined may be of benefit to orthognathic teams seeking to secure such psychological support within their respective units.
Introduction
Orthognathic surgery is a complex multidisciplinary treatment undertaken to correct dentofacial deformity for approximately 3000 patients annually in the United Kingdom (British Orthodontic Society, 2014). This treatment is planned on multidisciplinary clinics by orthodontists and maxillofacial surgeons working closely together for the benefit of the patient. Orthognathic surgical treatment is often undertaken over three years or more and it is important that the patient’s motivation and emotional resilience are assessed at the outset by a mental health professional to try to align the patient’s and clinician’s treatment goals.
The importance of clinical psychology in supporting patients in complex decision-making within other fields of elective surgical treatment such as bariatric surgery is evident in National Institute for Health and Care Excellence (NICE) guidance (Stegenga et al., 2014). They assess the psychological needs and expectations of the patient at the initial stages of the treatment pathway, which is critical to optimising the chances of a successful outcome. The same should apply to orthognathic patients, and the psychologist adds value by increasing the psychological awareness of other members of the multidisciplinary team. The patient is pivotal within the team and the aim was for them to view the psychological services as being an integral component of the management pathway. The role of the clinical psychologist within the multidisciplinary team (MDT) will be to offer a more holistic approach to the patient assessment and care and to support patients in making decisions about their care.
There is an increasing awareness within the public of the importance of mental health in addition to physical health. In 2011, the Department of Health published a framework for the Government’s strategy on mental health illustrating the role the commissioners would play called No Health Without Mental Health (HM Government, 2011). It listed six objectives and, arguably, the most important of these was that ‘fewer people would experience stigma and discrimination’ in seeking mental health support. Patients have welcomed the addition of a mental health professional within the MDT and they are seen as a huge asset to the treatment planning process and communication between the patient and the team.
It is well recognised that we are judged on our appearance and that people who are perceived to be more attractive are treated more positively than people that are deemed unattractive, even by those who know them (Langlois et al., 2000). Orthognathic patients often report having experienced significant distress in relation to their dental or facial appearance and have experienced bullying or discrimination as a result.
The model for oral health-related quality of life has five aspects to it: oral health; function; dentofacial appearance; social/emotional aspects; and environment (Sischo and Broder, 2011). A malocclusion impact questionnaire has been developed to measure the impact of malocclusion on oral health-related quality of life in young people (Patel et al., 2016). Three main themes emerged from the adolescent group interviewed: appearance concerns; social interactions; and oral health and function. These themes mirror the common concerns expressed by orthognathic patients at initial presentation. Patients presenting with craniofacial abnormalities at the Eastman Dental Hospital identified experiencing negative emotional issues including anxiety, depression and self-harm affecting their quality of life (Visram et al., 2018).
Patients can have many different motivations for seeking orthognathic treatment, including functional problems, facial or dental aesthetic concerns, emotional difficulties (history of bullying and low self-esteem) and to prevent future oral health-related problems (Pabari et al., 2011; Williams et al., 2005). The gold standard for a MDT caring for such patients should include an orthodontist, a maxillofacial surgeon and a psychologist to provide holistic care.
Why did we need a mental health professional as part of the team?
Mental health professionals can come from a background of clinical psychology or psychiatry but are more often clinical psychologists. They are an integral part of the team who not only can explore treatment expectations and support patients in their decision-making but also prepare patients for their treatment journey and in doing so enhance treatment outcomes.
A mental health professional’s primary role is to work with the orthognathic team to determine the best approach for each individual patient’s needs and if an approach other than surgery is more appropriate or if support is required preceding surgical treatment then they can support the team. They are also skilled in assessing and managing patients in psychological distress or where there are concerns about their mental health. This will include more common mental health issues such as anxiety and depression up to conditions of a higher complexity such as body dysmorphic disorder or schizophrenia. Psychologists will triage those patients to other mental health services such as the Improving Access to Psychological Therapies programme (IAPT) or secondary mental health services. The IAPT programme began in 2008 to improve the access to services for adult patients with anxiety and depression in England. This was a step forward, however, as stated in the National Health Service England (NHSE) publication Five Year Forward View for Mental Health the waiting times for IAPT were lengthy with many patients never having access to more advanced therapies with a clinical psychologist (NHS England Mental Health Taskforce, 2016). As a result, strategic investment in mental health services ensued with an emphasis on integrating physical and mental health wellbeing in healthcare delivery.
There are many positive service and financial benefits to having a psychologist within the orthognathic team:
Meet commissioning guidance and the gold standard of working practice;
Integrated approach to healthcare provision seen in other elective surgical specialties (in the Department of Health, NICE and Royal College guidance) and with other psychology services, e.g. IAPT, secondary mental health;
Increased patient satisfaction with the outcome of surgery by improving communication and managing patient expectations/aligning clinician and patient objectives from the outset;
Reduced number of unattended appointments or cancelled surgery by improving the engagement of the patient with the treatment process and early screening of patients to assess their emotional resilience;
Increase the research profile of the service and potential for improving the service through audit and clinical governance;
Enhance registrar training and the personal development, awareness and education of all the team members.
Initial pilot phase (2004–2006)
The initial pilot phase began when the orthodontic and maxillofacial team jointly approached their local clinical psychology team at North East London Foundation Trust (NELFT) to discuss working collaboratively. The idea was to demonstrate a demand for the service if one was to be established. The clinical psychologist would be present on the joint clinics and see patients for consultation where support would be beneficial. There were numerous business cases drafted with little progress due to financial constraints and relatively low perceived need of such a service.
Political background to the second pilot phase (2014–2017)
The turning point came in April 2012 when there was a merger of five hospital sites to create Barts Health NHS Trust, which included both Whipps Cross University Hospital and the Royal London Hospital. The Orthodontic and Maxillofacial departments at Whipps Cross became networked though this merger to the Royal London Dental Hospital.
During this time, the Primary Care Trusts were assessing money spent on elective surgical procedures within the NHS, including orthognathic surgery, and classifying procedures as high or low priority for funding by commissioners. While there was a renewed interest in orthognathic surgery, it was from a financial perspective and perceived value for money as opposed to any understanding of the improvement to a patients quality of life that is achieved with this treatment.
The ‘Commissioning Guide: Orthognathic Procedures’, jointly published in 2013 by the British Association of Oral and Maxillofacial Surgeons and the Royal College of Surgeons, outlined the evidence for the effectiveness of orthognathic treatment and stated that patients were at risk of suffering ongoing psychological disadvantage resulting from their malocclusions which could not be treated without orthognathic surgery (Royal College of Surgeons of England, 2013).
A group of consultant orthodontists within the British Orthodontic Society developed the Index of Functional Treatment Need (IOFTN) (Ireland et al., 2014) to help address the shortfalls within the Index of Orthodontic Treatment Need (IOTN) with regard to functional problems of orthognathic patients. This would be used to help justify the patient selection process for orthognathic surgery in times when it was felt that future funding for orthognathic surgery may have been at risk. It is recognised that the IOFTN is limited to assessing functional aspects of the malocclusion which is only one part of the assessment process of orthognathic patients. This limitation highlights the important role of the psychology service in a more holistic assessment of the patient’s needs and the need for these mental health professionals within the MDT.
A national orthognathic audit was undertaken during 2017–2018 of acceptance criteria for treatment and information provided to patients before their treatment (Ireland et al., 2019). A total of 69 hospitals submitted evidence, including Whipps Cross. The audit concluded that the majority of the orthognathic cases recorded fulfilled the criteria for acceptance for NHS-funded orthognathic treatment, with 91.07% of patients having an IOFTN score of a 4 or 5 and 88.73% having an IOTN score of 4 or 5. The audit therefore suggested that any suggestion of a prior approval process would not be a good use of NHS resources.
The second pilot phase began at Whipps Cross in collaboration with NELFT and ran from 2014 to 2017 during this complex political climate and a time of renewed interest in mental health within the NHS and the nationwide provision of orthognathic surgery.
Second pilot phase: Data collection (2014–2017)
A second pilot ran in 2014 identified 78 new patients seen on the orthognathic clinic in the first 12 months requiring at least 1–3 appointments depending on the level of psychological support required. These patients were previously seen on the new patient clinic and for a records appointment before attending their first appointment on the MDT clinic. Of these new patients, 27 (34.6%) were aged under 18 years. Five patients required more in-depth psychological support and each of these required up to 10 sessions with the psychologist. We found there were patients attending the MDT clinic who has never had the opportunity to see a clinical psychologist before and had concerns that could go on to affect their satisfaction with the process. Some of the concerns raised were: disproportionate effects on their social functioning due to their feelings about their malocclusion; conflict within their families with regard to the decision whether to proceed with treatment; and use of extreme language in describing themselves and low self-esteem. A further five patients required some additional postoperative psychological support and were seen as postoperative review patients. Six patients were deemed to be in significant psychological distress at the time of their attendance on the joint clinic, and sessions were arranged as soon as possible after the clinic. These patients were at various stages of their treatment and there are concerns regarding the impact that depression, self-harm and eating disorders were having on their wellbeing and functioning.
A waiting list for orthognathic patients soon built up, demonstrating a need for such a service; wherever possible, local services such as IAPT were utilised if appropriate. There were a few patients who caused concern and advice was sought from other units who had existing support structures in place.
Pilot presentation to NHSE in September 2017
In light of the increased emphasis on mental health awareness and wellbeing with the healthcare setting, an opportunity arose to present our initial findings to a panel of commissioners at NHSE and to pitch for support in establishing a psychology service at Barts Health NHS Trust.
During this time there was a pilot running in the south-east of England to seek prior approval for orthognathic surgery (among other surgical interventions) from NHSE. Within the application form, there was a section asking for confirmation of psychosocial assessment that ‘orthognathic surgery was in the patients best interest’. It became obvious to the team that clinical psychology needed to be integrated within the orthognathic service to ensure equity of care for patients when comparing ourselves with other teaching hospitals in London.
Historical data from two pilots as well as more up-to-date statistics were presented at the meeting together with projected finances needed to run the service. The risks and benefits to the patients and the service were summarised as listed below.
Risks included:
The risk of the patients not having the full team of orthodontists, surgeons and clinical psychologists available to comprehensively assess and support them
Increasing frequency of patients presenting with psychological problems and vulnerability of the clinicians not trained to manage their complex needs or conditions remaining undiagnosed
Increased cost of referrals to external tertiary centres/third party organisations
Negative effects on the lack of seamless provision of care
Benefits included:
Assessment only model – early signposting to psychological support at the point of initial attendance on the orthognathic clinic for patients with complex needs
Assessment and treatment model – improving access to both assessment and treatment providing a steam-lined psychological service which is evidence based
NHSE agreed to fund a service for a provisional one year for the orthognathic service at Barts Health NHS Trust. Money would be paid by NHSE directly to NELFT and Barts Health would cross-charge for services provided. We were allocated with a fixed amount of funding and in turn had to present evidence on a quarterly basis before a decision would be made on funding the service indefinitely. The evidence of service utilisation and clinical outcome measures would be presented to a mixed group of clinical and managerial representatives from NHSE, NELFT and the Barts Health.
Structure of the psychology service (March 2018)
Three clinical psychologists were appointed (one band 8a and two band 7s) with the band 8a based at the Royal London and the two band 7 psychologists being responsible for the Royal London and Whipps Cross units, respectively. All were appointed in two interview days with the same interviewing team consisting of one consultant orthodontist from Barts Health, two consultant psychologists from NELFT and one representative from Medical Staffing. The band 8a would coordinate the service while each of the band 7s would be based at two hospital sites to provide continuity of care for the patients and build solid working relationships with the orthodontic and maxillofacial consultants. There would also be two assistant clinical psychologists who would be assigned to one of the band 7s to help with the initial screening assessments and analyse the data from these clinics. The band 8a psychologist would be supported by a consultant psychologist from NELFT who had previously worked at Whipps Cross during the initial pilot.
Referral pathway
Figure 1 illustrates the referral pathway that was developed for the service. The majority of patients would enter the pathway from their first attendance on the joint clinic where they would be initially assessed by the orthognathic team. Other patients may also be seen by the psychology team on the joint clinic further along their treatment journey (i.e. being seen at the end of preoperative orthodontic treatment for confirmation of their surgical treatment plan or immediate or long-term postoperative review). Patients may also be seen by direct referral to the psychologist using a referral form (Figure 2) completed by the orthodontist or the surgeon and emailed directly to the psychologist.
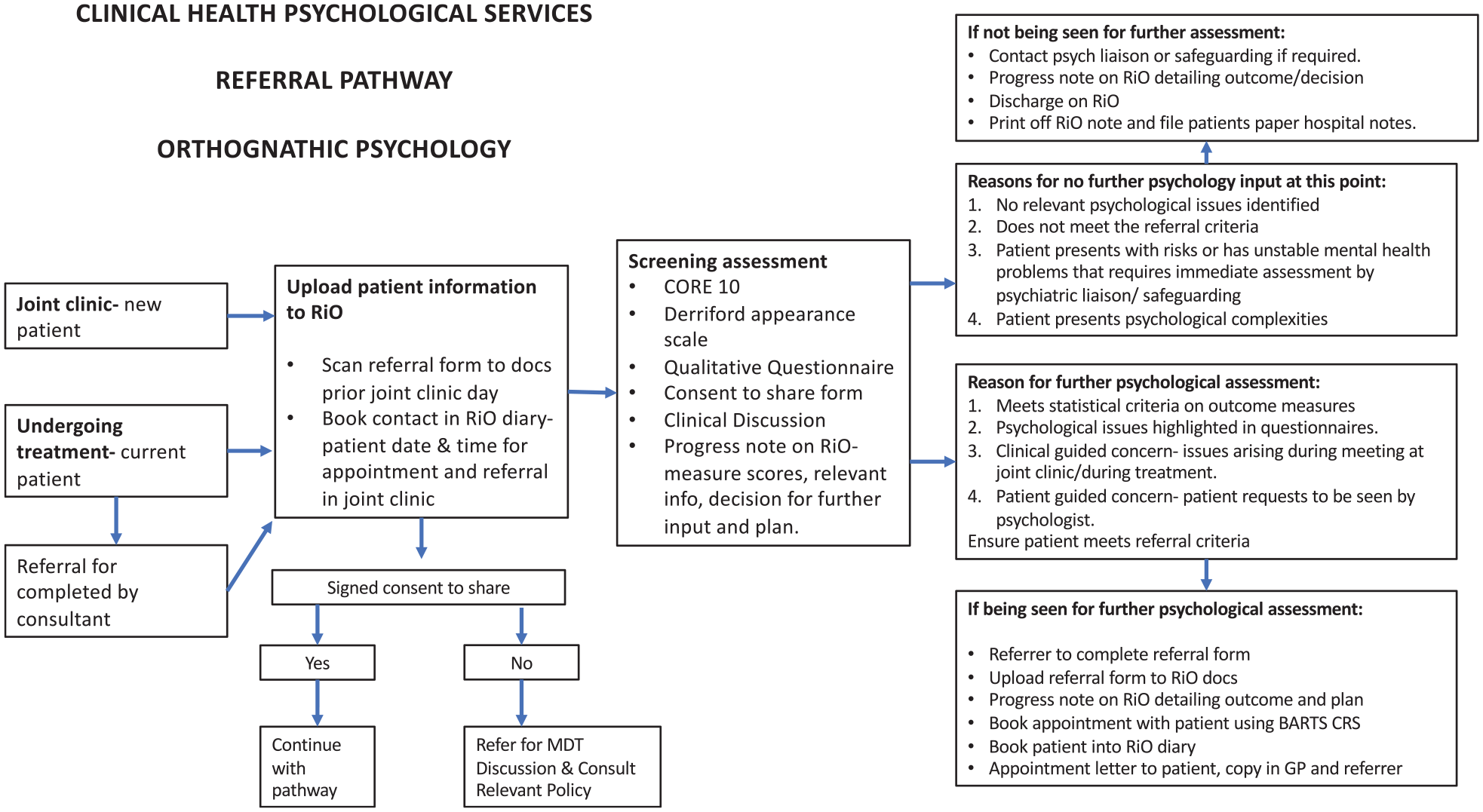
Referral pathway for orthognathic psychology service.
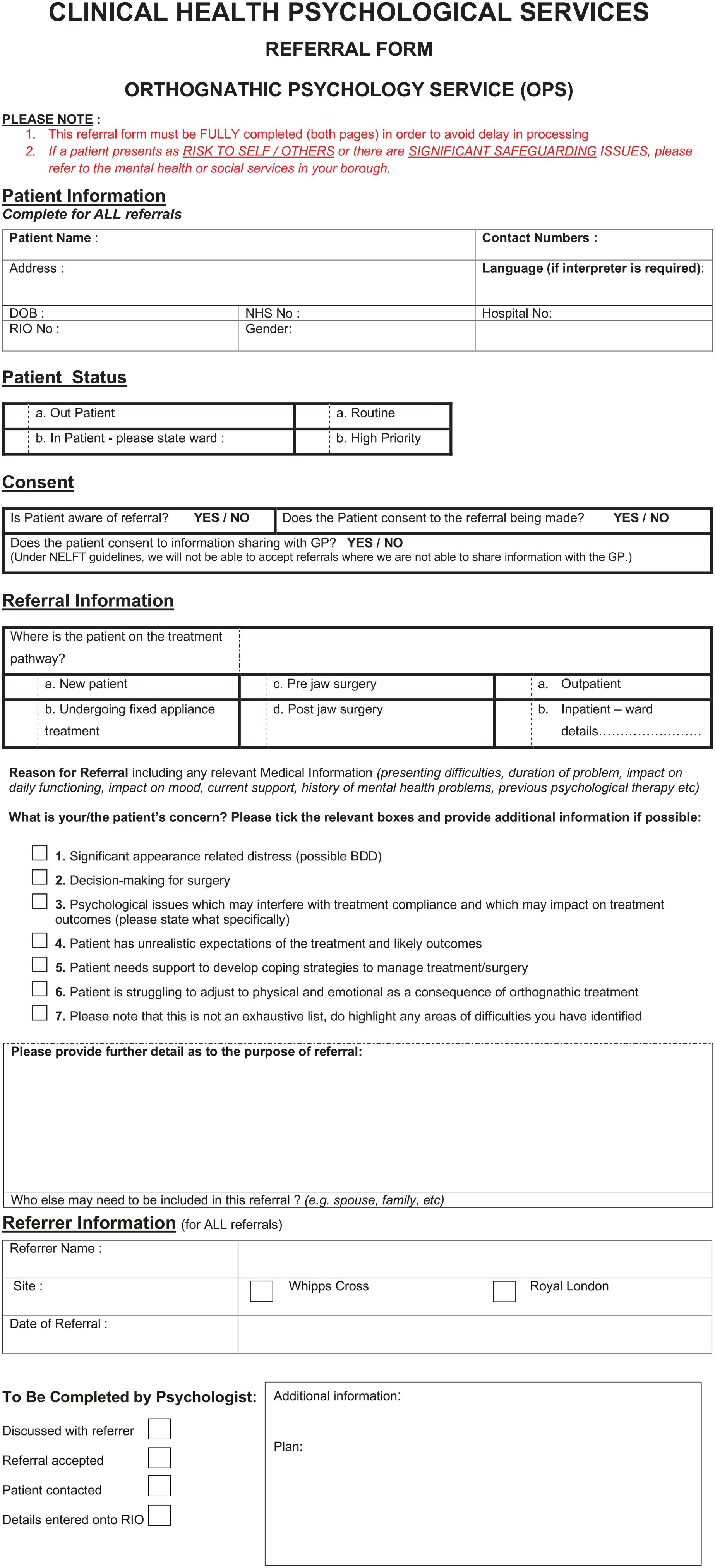
Orthognathic Psychology Service (OPS) referral form.
Referral criteria for the service were developed for inclusion and exclusion criteria to demonstrate to the NHSE commissioners that the service would be ring-fenced for suitable orthognathic patients (Table 1). Anyone who fulfilled the inclusion criteria and under the care of the Bart’s Health service could be referred to be seen.
Inclusion and exclusion criteria.
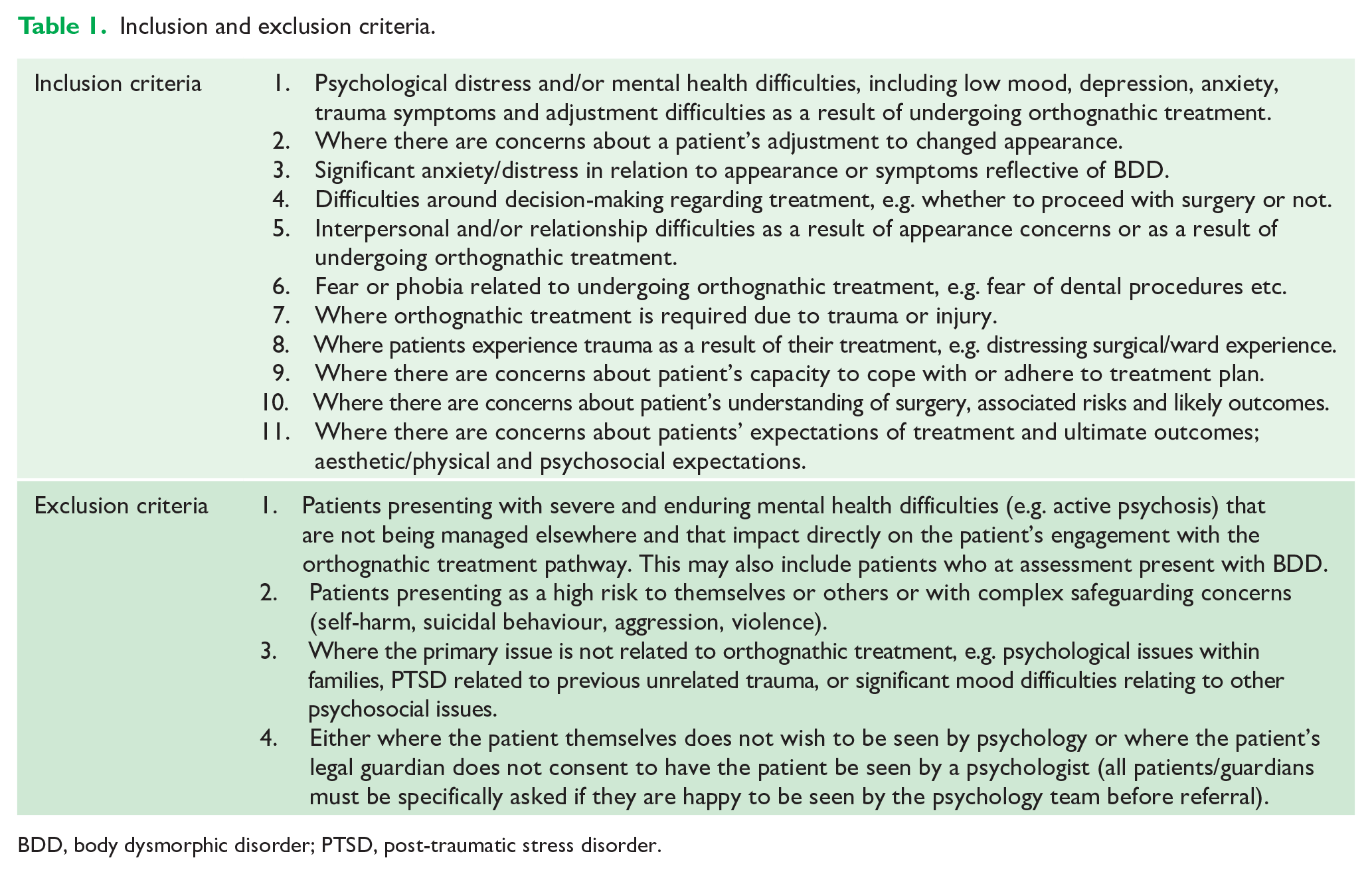
BDD, body dysmorphic disorder; PTSD, post-traumatic stress disorder.
Patients who were deemed as being not suitable for this psychology service would then be referred onwards to a more suitable tertiary or emergency service by the psychology team.
Initial screening process
All new patients presenting on the joint clinic would be screened by the psychology team on arrival using the questionnaires in a pack:
Qualitative questions: motivation for surgery, expectations, previous dental experiences (idea of treatment response) and current/past mental health;
Clinical Outcomes in Routine Evaluation system (CORE-10) – subjective wellbeing, problems/symptoms (anxiety or depression), life functioning (social relationships). and risk and harm (to themselves and others);
Young Person’s Clinical Outcomes in Routine Evaluation system (YP-CORE) – same as CORE-10 but language adapted for patients aged 11–16 years;
Derriford Appearance Scale (DAS24) – adjustment in problems of appearance (intensity of emotional response, frequency of particular behaviours indicating self-consciousness and functional limitation)
Consent to Share Form
CORE-10 is a list of 10 statements in a questionnaire asking how a patient felt over the last week. It was developed from a multidisciplinary group of practitioners from 33 primary care services and all information was categorised into domains and clusters of which 10 were selected to gain a wide assessment while keeping it a quick screening tool (Connell and Barkham, 2007). The CORE-10 is derived from the more complex CORE-OM which is a 34-item assessment widely adopted in the field of psychological therapies. In CORE-10 each question is rated on a scale of ‘not at all’ to ‘most of the time’. It looks at commonly experienced symptoms of anxiety and depression as well as other aspects of social functioning and crucially asks about risk to self with a question asking about plans to end life. The score from the questionnaire is then used to rank the distress level of the patient out of 40 from ‘Healthy’ or ‘Low Level’ distress with a score of 10 or below to ‘Severe Level’ of distress if scoring 25 or above. The YP CORE-10 questionnaire is modified with some of the questions worded in a way to make it more acceptable for a younger age group.
DAS24 is a psychological measure of appearance concerns which has proven validity and reliability in clinical and research settings. The original scale containing 136 items developed from 54 anecdotal accounts of adult plastic surgery patients from Derriford Hospital, Plymouth (Harris, 1982). Refinement of the scale produced the 59-item version (Carr et al., 2000) and finally the short form with 24 items selected to include the broadest range of responses while making the form easier to use (Carr et al., 2005). The questionnaire takes 10 min to complete and is validated on adult patients who speak English with no learning difficulties.
The consent to share form seeks consent for information to be shared between professionals and the general medical practitioner. Those that did not consent would alert the team that perhaps this patient might not be suitable for treatment. The clinical psychology team would record their clinical notes on the software RIO keeping psychology notes separate from orthodontic and surgical notes for patient confidentiality.
Predictors of dissatisfaction
Orthognathic patients have a poorer body and facial image when compared to a non-clinical control group (Cunningham et al., 2000). The majority of patients are happy with the outcome of their surgery; however, there are a small proportion of who are not. This may be due to underlying undiagnosed psychological condition which can worsen if not identified before treatment. There are certain red or amber flags that may indicate that it is not in the patient’s best interest to proceed with treatment (Table 2). These flags indicate to the clinician the degree of concern that a patient may experience dissatisfaction with orthognathic treatment (Ayoub et al., 2013).
Red and amber flags for predictors of dissatisfaction in orthognathic patients.
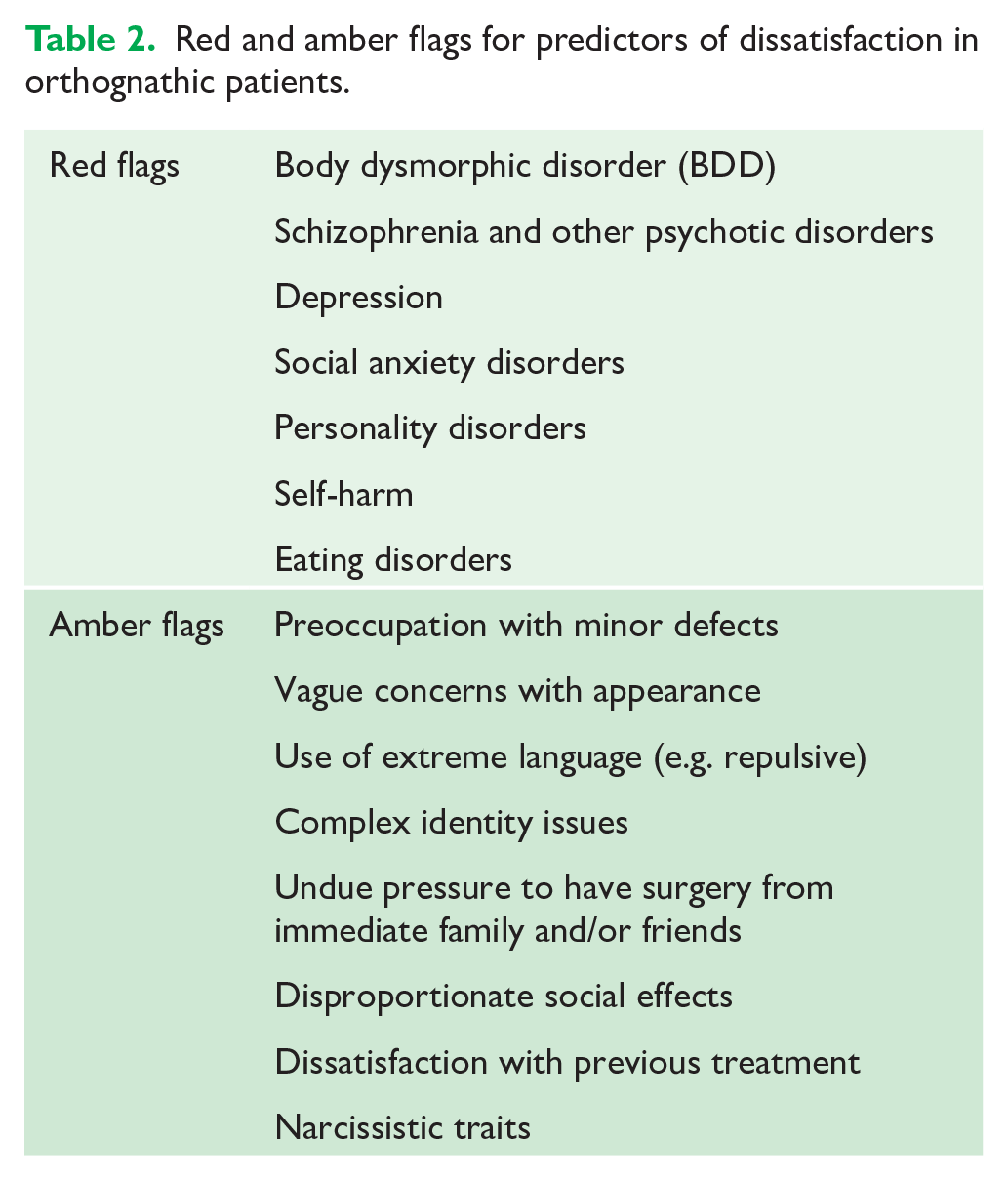
Patients presenting with red flags are unlikely to benefit from orthognathic surgery and have a high risk of dissatisfaction with any treatment provided and should be referred on to specialist mental health services. Amber flag patients need a risk/benefit analysis and careful team discussion to decide if the degree of dentofacial deformity and benefit of surgery could outweigh any psychological concerns provided the patient is offered additional support by the psychology team.
One of the most complex patient group are those presenting with the red flag of Body Dysmorphic Disorder (BDD). BDD is a psychiatric disorder in which ‘the individual has a disproportionate concern about a particular body part’ (Rosten et al., 2018). There are diagnostic criteria such as a ‘preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others’ (American Psychiatric Association, 2013). The weighted prevalence of BDD of adults in the community is estimated to be around 1.9%, while the figure for adult psychiatric inpatients is 7.4% and the prevalence in orthodontic/cosmetic dentistry settings is in the range of 4.2%–7.5% (Veale et al., 2016). The rate of BDD seen by orthodontists was also reported as high as 7.5% of adult patients (Hepburn and Cunningham, 2006). The specific incidence of BDD within orthognathic clinics is quoted as between 10% (Vulink et al., 2008) and 13.1% (Collins et al., 2014). In study of a group of patients with BDD, it was found that 86% of them mentioned the face as one focus of their concern (Veal et al., 1996). The weighted average for BDD in orthognathic patients is quoted as 11.2%, being higher in women (13.2%) compared with men (8.0%) with a ratio between the sexes of 1.65 (Veale et al., 2016).
Conclusions: Turning challenges into opportunities
The service commenced in September 2018 with the time taken from pilot phase being lengthy but ultimately successful. The journey is summarised as a timeline in Figure 3 (adapted from Kingsley, 2020). The additional support provided by the clinical psychologists has been profound for the benefit of patients and the healthcare team involved in delivering orthognathic care.
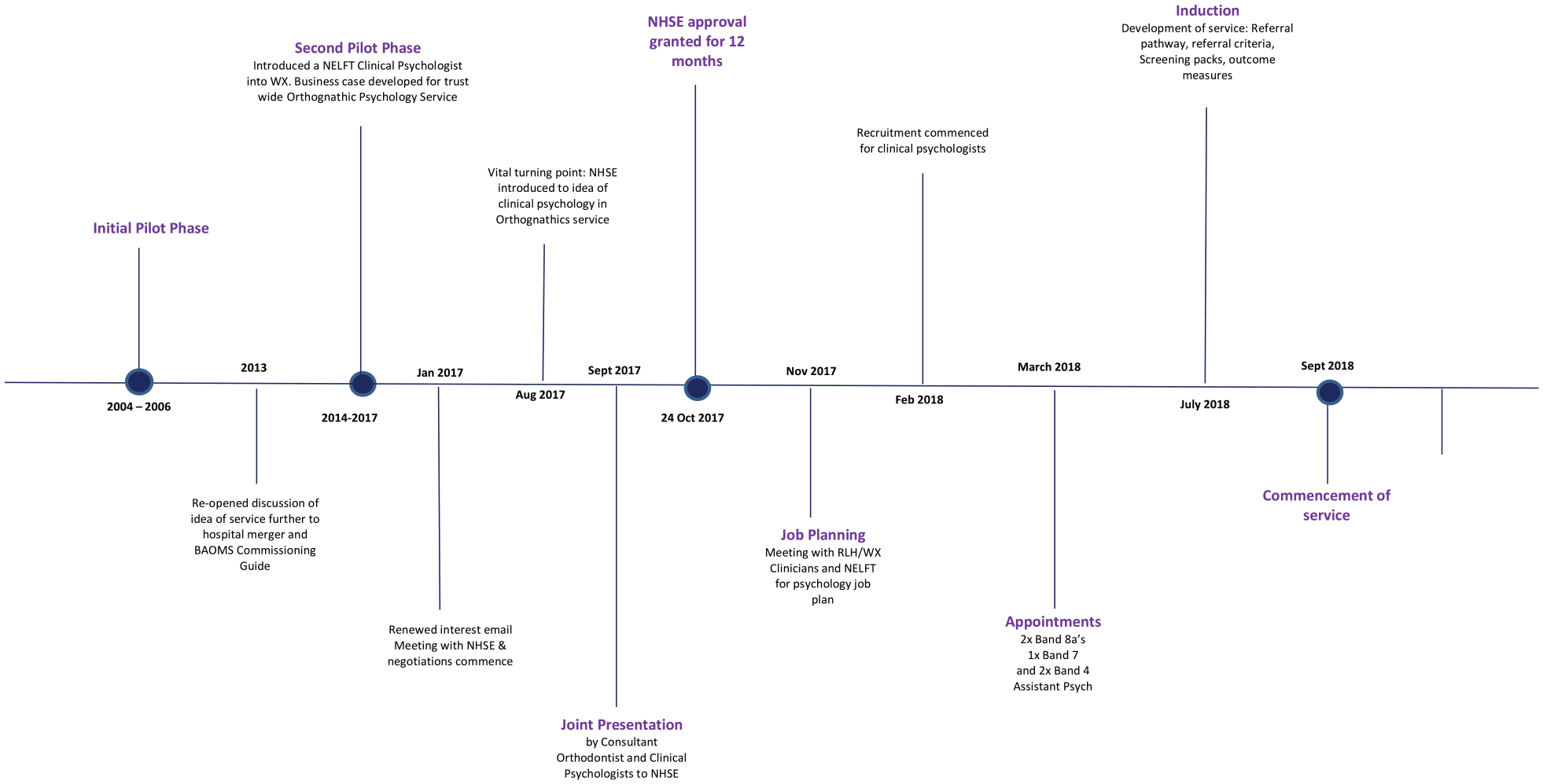
Timeline for establishment of Orthognathic Psychology Service (OPS) 2004–2018.
The biggest challenge faced by the team was convincing the Trust and the commissioning services of the added value offered by the psychology team. There has been a significant shift in attitudes towards the importance of mental health in recent years that will make the path somewhat easier for colleagues also wishing to introduce or further develop their services.
The journey to reach this point has relied on liaising with local mental health services to discuss the potential mutual benefits of collaborative working and resilience within that team to establish the service with the use of well-written and documented business cases. A pilot service to establish initial data collection demonstrating need is recommended.
Footnotes
Acknowledgements
The authors would like to acknowledge Jeremy Wallman and Katherine McNaughton at NHSE without whose support they would not have established the service.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.