
Abstract
Objective:
To review a series of clinical studies demonstrating the clinical efficiency of aligners with bite ramps in the treatment of severe deep bite.
Materials and Methods:
In order to predictably manage the correction of deep bite with aligners, precision bite ramps on maxillary incisors have been used while posterior extrusion and anterior intrusion in the lower jaw with lateral attachments and proper levelling of the curve of Spee have been planned. Transverse correction and controlled upper and lower incisors proclination completed the treatment plan.
Results:
Full deep bite correction with normal overbite was obtained in nine months of treatment by a combination of anterior intrusion and posterior torque correction, distal tipping and relative extrusion.
Conclusion:
The use of bite ramps represents a valid option for the successful treatment of deep bite with aligners creating proper space for lateral sector extrusion and supporting lower anterior intrusion and controlled proclination.
Introduction
Deep bite features are constituted by a mix of dental and skeletal conditions that can influence the severity of the malocclusion (Danz et al., 2014; Nielsen, 1991). Dental conditions are represented by over-eruption of maxillary and mandibular incisors, vertical inclination of both incisors on respective basal bone and loss of posterior vertical dimension, while skeletal conditions are represented by growth pattern and gonial angle. When the skeletal conditions are predominant, the percentage of success with an orthodontic-only approach often limits the results to dental movements. When dental conditions predominate, the orthodontic approach based on a combination of anterior teeth intrusion and posterior extrusion in order to level the curve of Spee ensures proper malocclusion correction (Baldridge, 1969; Braun et al., 1996; De Praeter et al., 2002).
In case of severe deep bite, this approach cannot work properly if not associated with posterior extrusion. The correction of moderate deep bite condition, on the other hand, producing incisor inclination and vertical posterior over-eruption can be successful. Moreover, when performing anterior intrusion of the upper incisors, specific attention in respect of the smile arc should be observed (Kale Varlık et al., 2013; Sarver, 2001).
The use of aligner treatment induced the observation that molar extrusion seems to be prevented during dental movement by full day use of the aligners. The so-called bite effect is represented by the consideration that teeth are moved within the aligners and the occlusal forces exerted 24 h per day aim to avoid vertical extrusion of posterior teeth. This reactive intrusion force can be considered biomechanically favourable when treating vertical excess in openbite patients, but, on the other hand, when treating vertical reduction in deep bite patients, this bite effect can represent a strict limitation because it circumscribes the dental correction to the anterior part of the arch (incisors inclination, intrusion of upper and lower teeth) (Giancotti et al., 2008, 2014; Miller and Derakhshan, 2002; Rossini et al., 2015). The introduction of bite ramps embedded into the aligners have changed the approach to the deep bite treatment increasing treatment predictability and avoiding the need for digital plan over-engineering. The aim of this clinical report was to assess the outcome of deep bite malocclusion treated in young adult patients with aligners and bite ramps, following a specific 3D digital setup plan.
Digital plan setup
To properly correct deep bite malocclusion with aligners, the Invisalign® system has introduced a feature called precision bite ramps, a feature embedded into the aligners that allows the user to plan a sort of anterior customised bite turbos available on the lingual surface of the upper anterior teeth (centrals and laterals) or on the upper canines. This feature does not require composite filling as in traditional attachments; it is a lingual extension of the aligner (maximum palatal extension = 3 mm) that creates premature anterior contacts and posterior disocclusion. The ramps are planned to move, stage by stage, in a more occlusal direction, creating the necessary posterior occlusal space that permits lateral and posterior teeth to extrude relatively. They need to be combined with two other features: extrusion attachments on lateral teeth and lower incisors pressure areas, a sort of lingual pressure point, designed to exert intrusion forces following the long axis of the incisors more effectively. In this way the levelling of the lower curve of Spee will be more reliable combining two reciprocal movements in two different parts of the arch, fulfilling anterior intrusion and posterior extrusion as indicated in the literature (Liu and Hu, 2018; Simon et al., 2014) (Figure 1).

Bite ramps clinical and digital aspect: 3D curve of Spee levelling with occlusal contacts distribution.
When planning the digital setup (clincheck®), careful levelling of the curve of Spee in the three dimensions of the space needs to be addressed, in particular:
On the vertical plane, the lower second molars represent a reference point, so they do not need to be extruded, while extrusion should be planned on the first molars, second premolars and (sometimes) first premolars (depending on the severity of the curve). The intrusion should be achieved simultaneously from canine to canine creating a normal overbite (Zhao, 2019).
On the sagittal plane, distal tipping of the second and first molars will support the curve of Spee levelling in combination with reciprocal mesial tipping of premolars and canines. This movement is synergic and distal tipping will favourably partially extrude the molars.
On the transverse plane, the uprighting of premolars and molars reaching a torque close to zero degrees will create a relative extrusion of lateral sectors contributing to the generation of levelling of the curve of Spee and the premature posterior occlusal contacts (Kim and Gianelly, 2003).
This amount of posterior extrusion planned in 3D will create, on the digital plan, heavy occlusal contacts on the working cusps and these premature contacts will lead on the clinical side to a proper intercuspation without losing the occlusal contacts during treatment, generating mandibular clockwise rotation. Finally, in order to favour mandible rotation and proper intercuspation, Class II elastics with vertical component directly connected to the aligners will be helpful to achieve the real and relative extrusion.
To recapitulate, in order to have a predictable clinical outcome for overbite correction, it is fundamental to plan in the 3D setup software (clincheck®):
anterior intrusion (in lower jaw when smile arc is correct);
posterior extrusion;
3D curve of Spee levelling as described above;
posterior and lateral teeth thick attachments (rectangular shape, horizontal orientation, gingival beveled);
bite tamps on upper incisors (in case of lower anterior intrusion);
pressure area on lower incisors;
controlled upper and lower incisors proclination;
heavy posterior occlusal contacts;
Class II elastics with vertical component directly connected to the aligners.
Case report 1
History and assessment
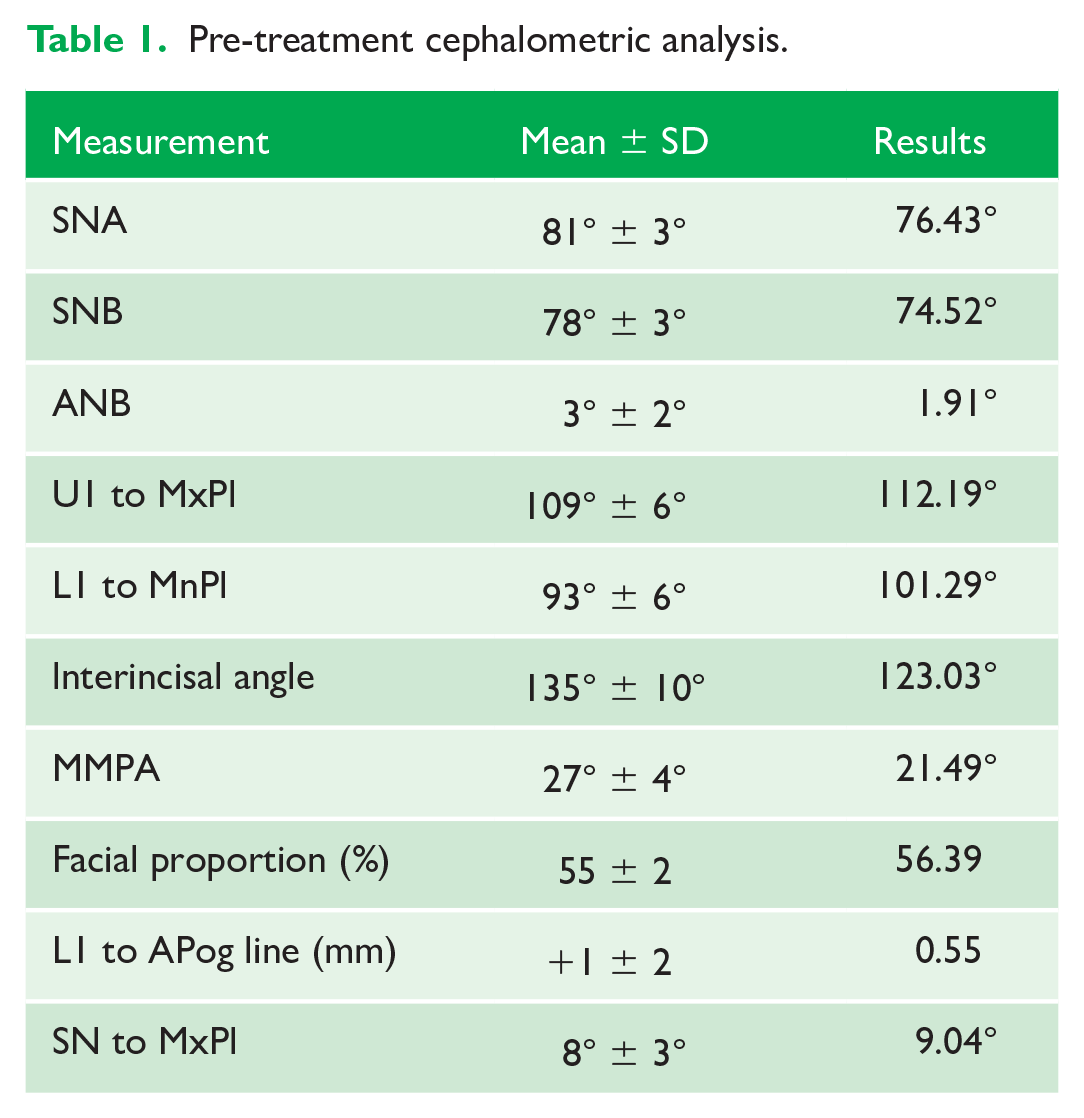
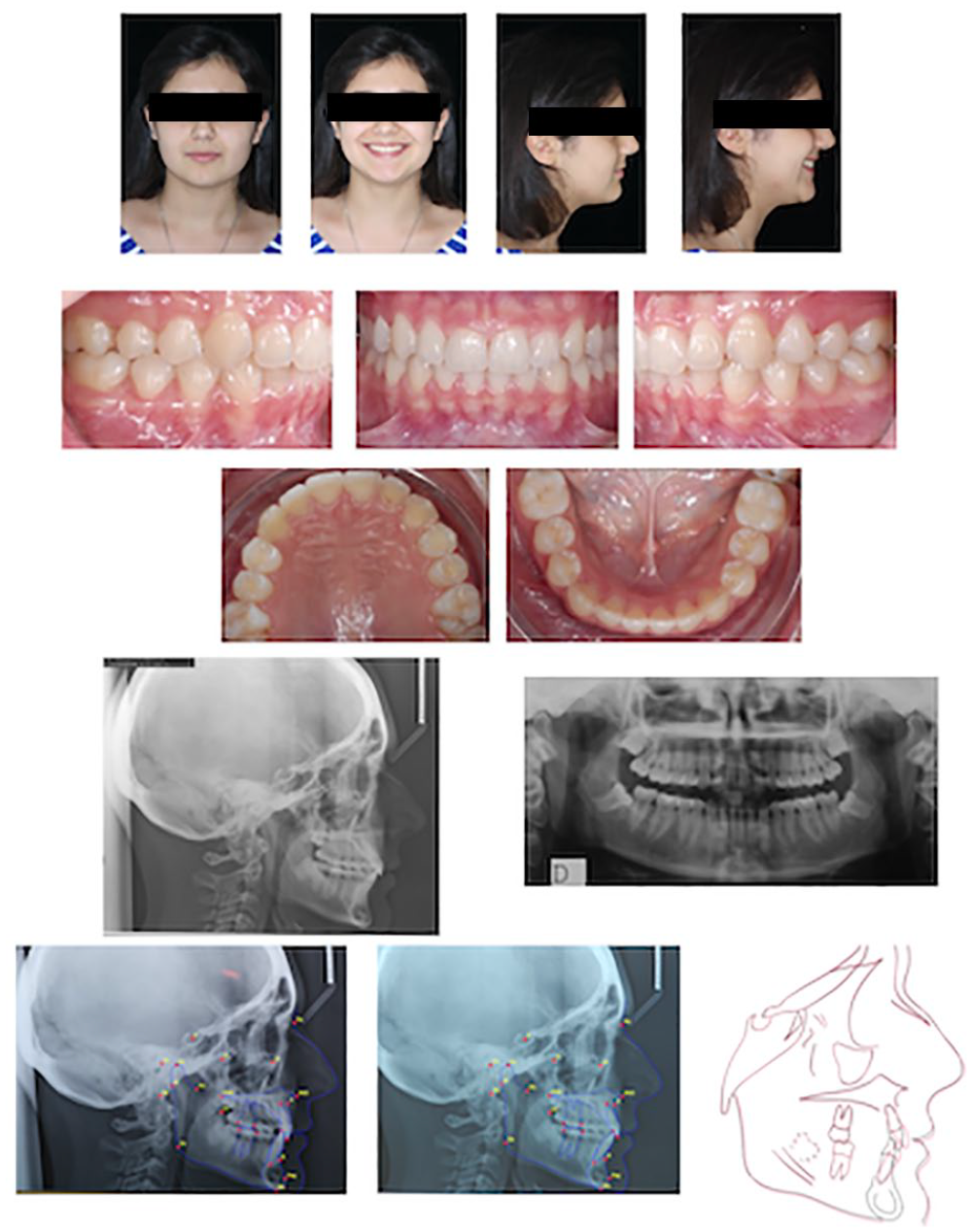
A 16-year-old female patient presented with the chief complaint of re-establishing anterior alignment in both arches. Facial analysis showed a short face with a flat profile but a proper chin projection, while clinical examination revealed a skeletal (ANB = 1.47°) and dental Class I malocclusion with severe deep bite (100%), deep curve of Spee, negative upper central incisors torque (1-SN = 91.19°) with proclined lateral incisor, and severe mandibular and maxillary tooth-size arch-length discrepancies in a Class I molar and canine relationship (Figure 2). The deep bite components are fully represented in this patient since negative incisor inclination (IMPA = 88.24°), over-eruption of lower teeth and hypodivergent pattern (FMA = 20.85°) with decreased gonial angle (115.10°) can be detected. Lateral cephalogram analysis indicated a reduced lower anterior facial height combined with hypodivergent pattern (Table 1). The only treatment option suggested was an orthodontic treatment approached with aligners for deep bite correction with all the features described above (bite ramps, pressure area, 3D curve of Spee levelling, Class II elastics, heavy occlusal contacts).

Pre-treatment records.
Pre-treatment cephalometric analysis.
Treatment progress
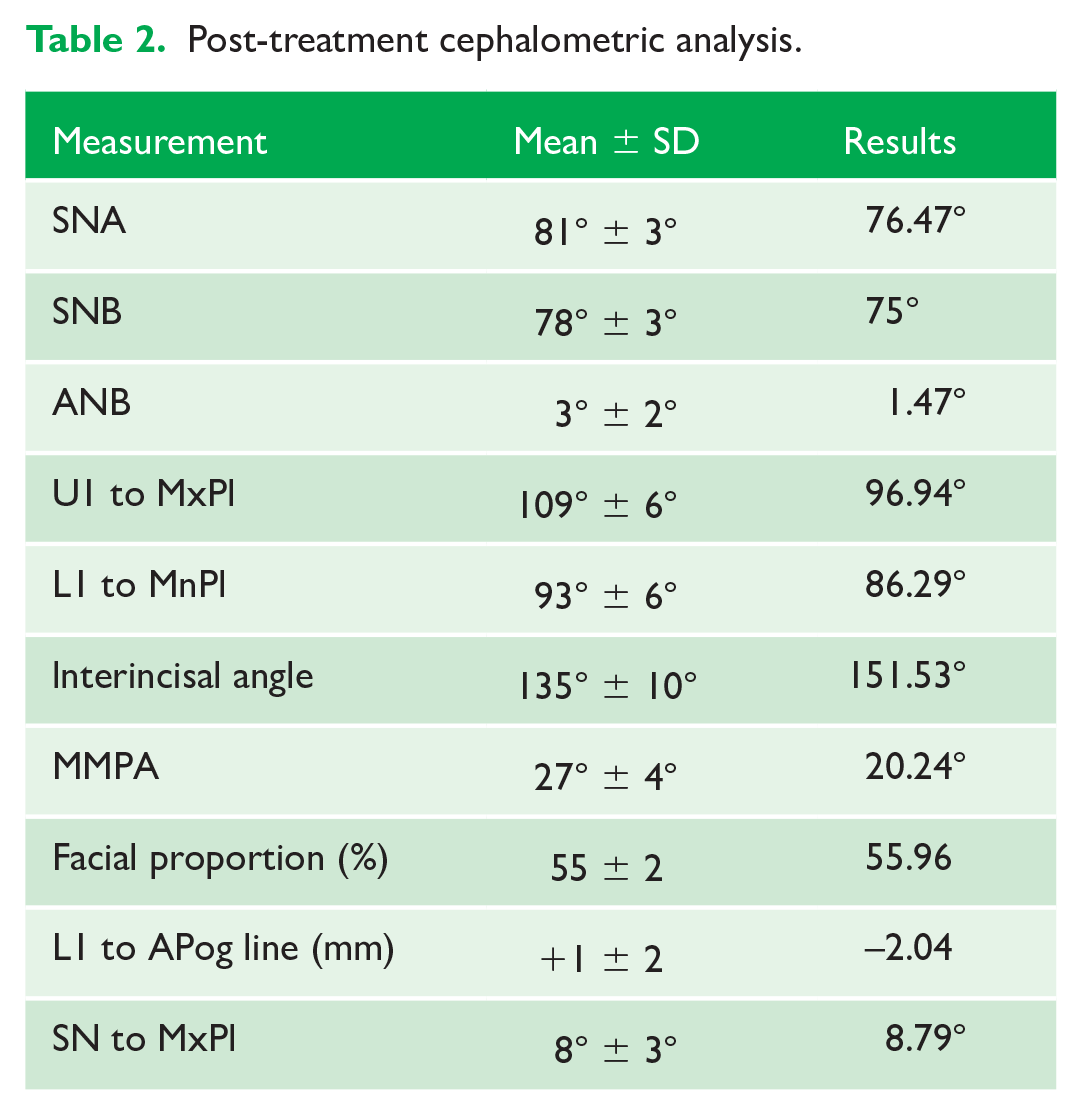
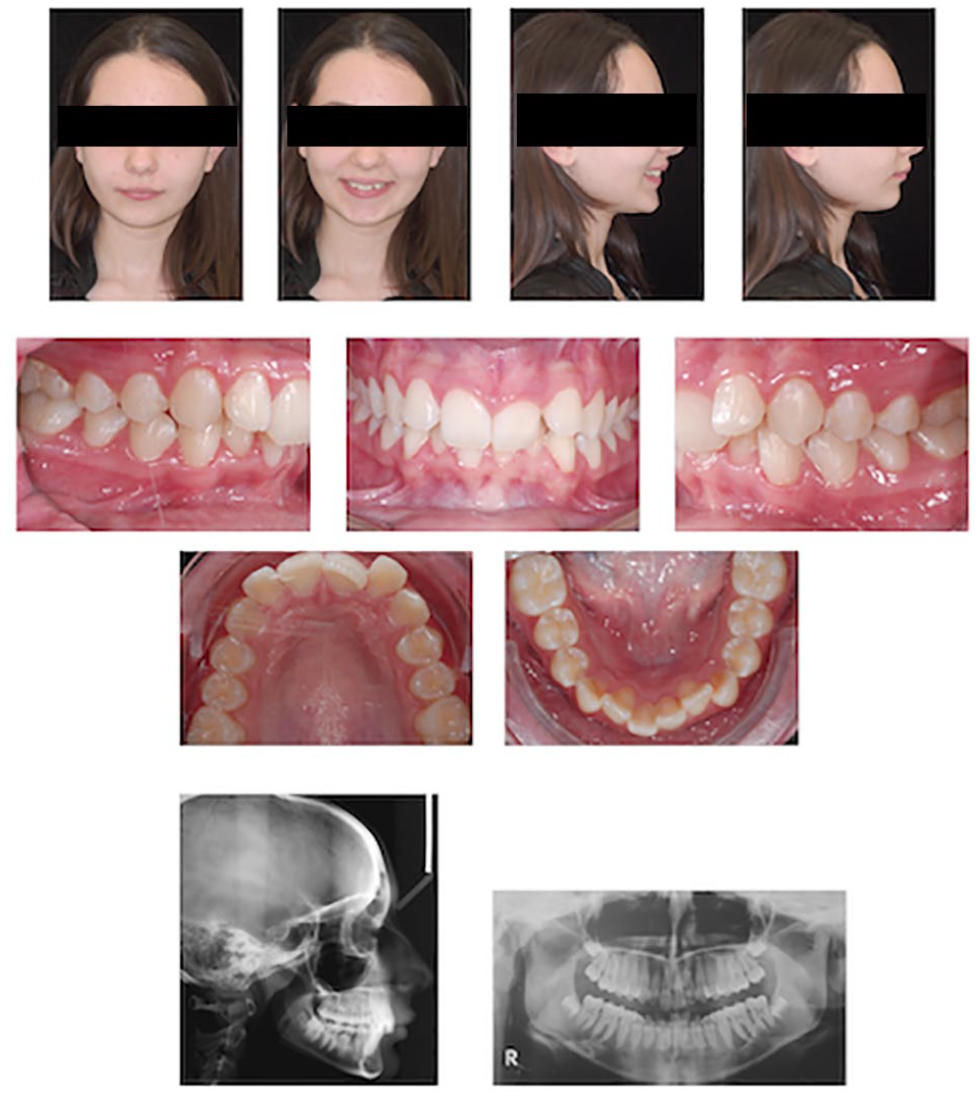
The digital treatment plan (clincheck®) provided 26 aligners in the upper arch and 26 in the lower arch. The treatment objectives were focused on coupled vertical movements of posterior extrusion and anterior intrusion by means of a bite ramp feature providing for posterior disocclusion, anterior intrusion of lower teeth and by means of extrusion attachments needed for lower arch levelling. Upper and lower incisors were proclined in order to level the upper and lower curve of Spee and to support the flat profile and the lips. Class II elastics were planned to support lower proclination and posterior heavy occlusal contacts with relative posterior extrusion. Lateral and posterior upper torque were planned to be close to 0° in order to achieve wider arch design and ideal intercuspation. No digital over-engineering has been planned in the setup. Because of the age of the patient, weekly aligner change was followed for the total treatment time of 6.5 months. At the end of the first stage of aligners (Figure 3), an additional stage was planned to improve molar intercuspation without elastics and with a digital plan of 13 further aligners. This brought the total treatment time to 9.5 months. At the end of the treatment (Figure 4), full Class I canine and molar relationship was obtained, upper and lower incisors inclination (1-SN = 98.79°, IMPA = 98.07°) were fully corrected by means of proclination, the divergency was slightly increased (FMA = 21.71°) because of the relative posterior extrusion and use of Class II elastics (Table 2). A balanced smile arc was reached with an ideal relationship between upper incisors and lower lip, while torque control of lateral and posterior segments generated a broader smile. Reliable superimposition between real clinical conditions and digital setup position was reached without digital overcorrection. The lateral cephalograms general superimposition has shown some interesting changes induced by the orthodontic treatment:
The upper incisor inclination with respect to the maxillary plane changed about 16° (from 96° to 112°) while inclination of the lower incisors with respect to the mandibular plane changed about 15° (from 86° to 101°) with a good interincisal relationship and sufficient symphysis support.
The relative extrusion of upper and lower molars combined with the use of bite ramps generated a slight clockwise rotation of the mandible (MMPA from 20° to 21.5°) which allowed a further improvement of the overbite.
The vertical control and the clockwise rotation of the mandible induced a slight change in the SNB (from 75° to 74°), which is aligned with the overall modifications.
An improvement in profile and lip sustain can be appreciated due to the proclination of the upper and lower incisors.

Progress pictures after six months.
Post-treatment records.
Post-treatment cephalometric analysis.
Case report 2
History and assessment
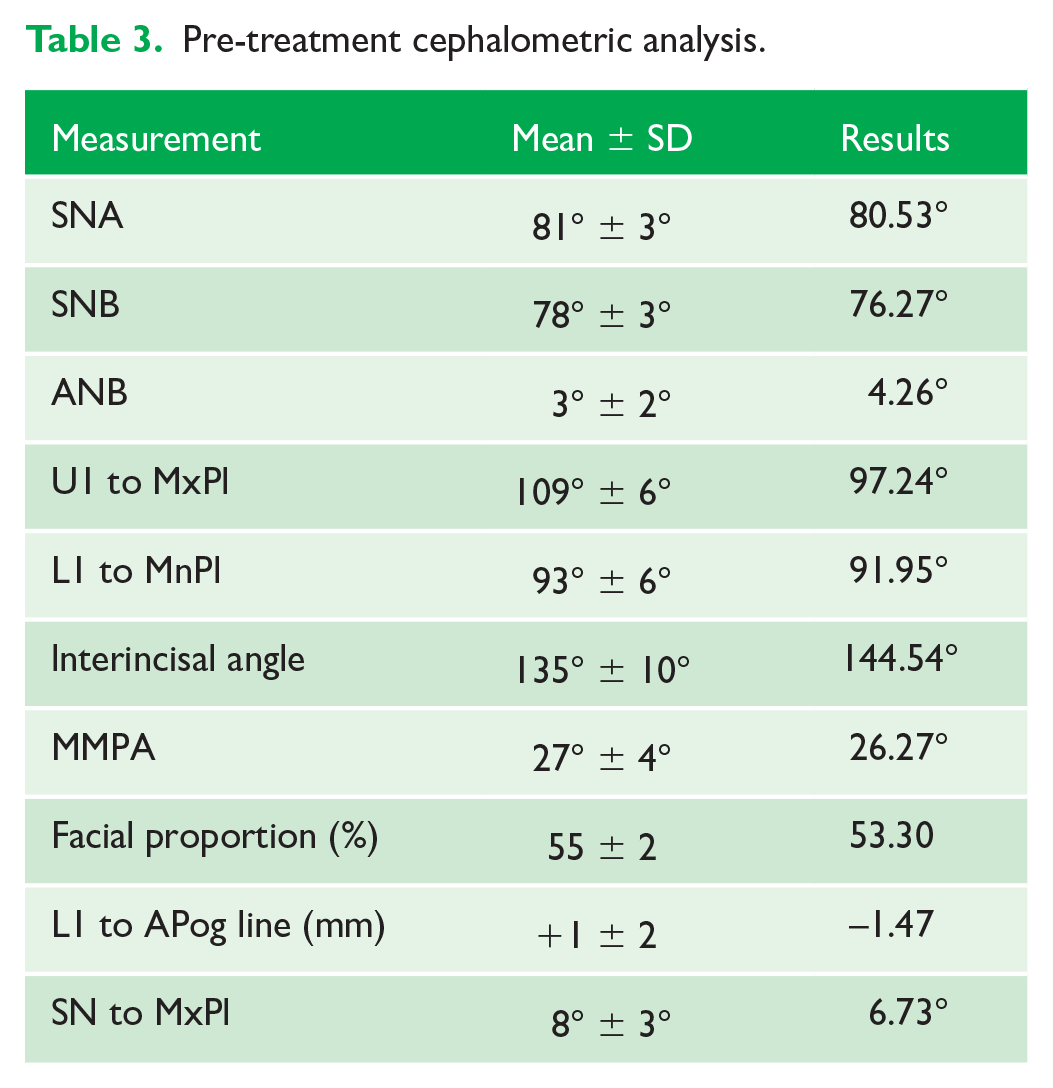
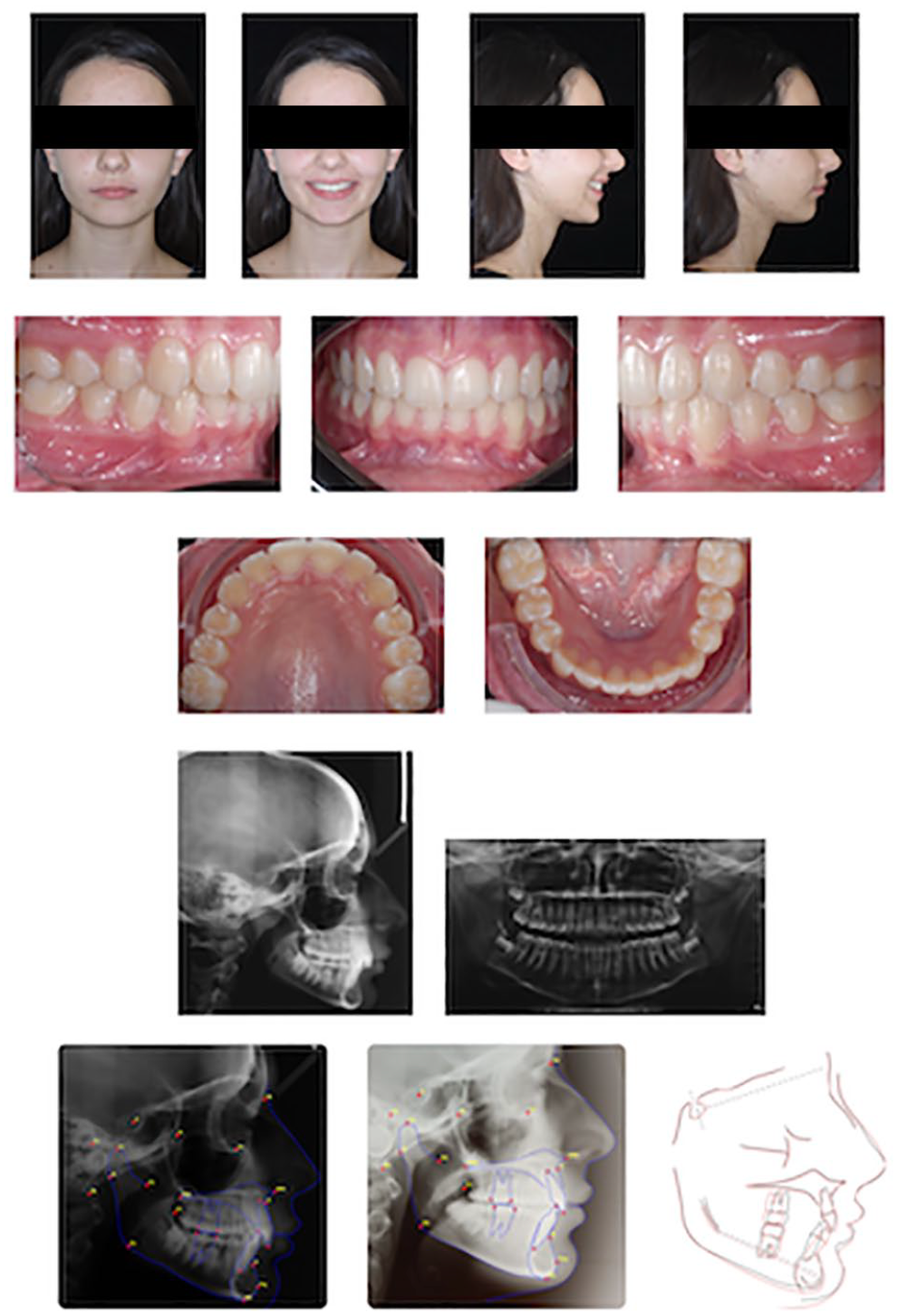
A 12-year-old female patient presented with moderate crowding in both arches with mid Class II malocclusion. Facial analysis revealed a short face with proper nasolabial angle value but reduced chin projection, while clinical examination revealed a skeletal (ANB = 4.26°) and dental mild Class II malocclusion with severe deep bite, deep curve of Spee, negative upper central incisors torque (1-SN = 90.51°) and severe crowding in both the upper and lower arches (Figure 5). The deep bite components are represented with negative incisors inclination (IMPA = 91.95°), hypodivergent pattern (FMA = 21.01°) with a normal gonial angle (123.68°) (Table 3). A mild Class II molar and canine relationship can be detected with severe mesial molars rotation. The treatment option suggested was an orthodontic treatment approached with aligners and precision bite ramps with all the features described above (bite ramps, pressure area, 3D curve of Spee levelling, Class II elastics, heavy occlusal contacts).
Pre-treatment records.
Pre-treatment cephalometric analysis.
Treatment progress
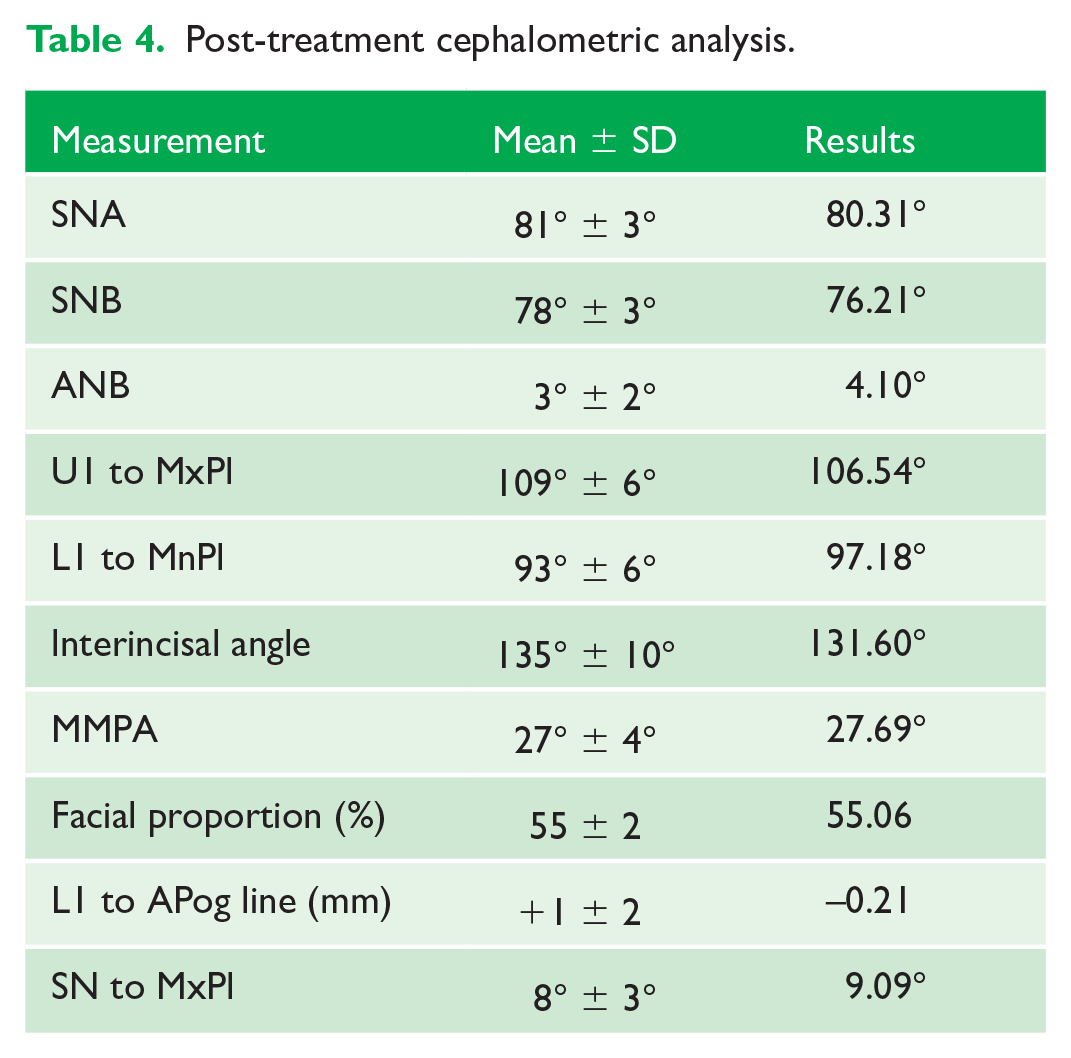
The digital treatment plan (clincheck®) provided 41 aligners in the upper arch and 27 in the lower arch. The digital plan was focused on maxillary molars distal rotation to correct the Class II relationship combined with distalisation. The simultaneous use of precision bite ramps on incisors provided for posterior disocclusion and lower curve of Spee levelling. Upper and lower incisors were proclined in order to support the facial profile, Class II elastics were planned to control posterior anchorage, to support upper molar distal rotation and to favour posterior occlusal contacts. Lateral and posterior upper torque was planned to respect the 0° value in order to achieve wider arch design. Because of the age of the patient, weekly aligner change was followed for the total treatment time of 10.5 months. At the end of the first stage (Figure 6), an additional stage was planned to improve posterior intercuspation with vertical elastics and a digital plan of 15 further aligners. This brought the total treatment time to 14 months (Figure 7). Full Class I canine and molar relationship was achieved with a proper inclination of the upper and lower incisors (1-SN = 97.44°, IMPA = 97.18°). The divergency was slightly increased (FMA = 21.14°) because of the use of bite ramps and the relative posterior extrusion combined with the Class II elastics use (Table 4). Facial aesthetics improved on profile analysis and even more on the frontal smile. Reliable superimposition between real clinical conditions and digital setup position was reached without digital overcorrection. The general superimposition of lateral cephalograms has shown some interesting changes induced by the orthodontic treatment:
The upper incisor inclination with respect to maxillary plane changed about 9° (from 97° to 106°) while inclination of the lower incisors with respect to the mandibular plane changed about 6° (from 91° to 97°) with a good inter-incisal relationship. The amount of proclination was compatible with the thickness and shape of the symphysis.
An interesting growth of nose and chin can be appreciated in a forward and downward direction.
The relative extrusion of upper and lower molars combined with the use of bite ramps generated a slight clockwise rotation of the mandible (MMPA from 26° to 27°).
The B point maintained its position (SNB 76°) between initial and final Ceph as a result of clockwise rotation of the mandible and related growth.
Distal movement of maxillary molars can be appreciated as a result of the upper distalisation. A slight mesial movement of the lower molars can be detected since it was planned on the digital setup to improve the lateral intercuspation.

Progress after 10 months of treatment.
Post-treatment records.
Post-treatment cephalometric analysis.
Discussion
The curve of Spee and the management of posterior teeth movement represent a crucial point in the treatment of severe deep bite with aligners. To better clarify how differential movements can influence deep bite treatment, some authors (El-Dawlatly et al., 2012) recently classified deep overbite malocclusion features in principal and secondary components.
The principal components are represented by a decreased gonial angle and deep curve of Spee. The secondary components are represented by front teeth inclination, over-eruption of maxillary incisors and vertical growth of the maxilla.
When treating deep bite malocclusion, the intrusion of the mandibular incisors should be combined with the extrusion of the posterior segment by means of relative extrusive movements (torque and tip correction). With this approach it is possible to obtain a significant amount of anterior deep bite correction with a small amount of real posterior extrusion deriving from a proper levelling of the curve of Spee. In particular, with every 1 mm of posterior extrusion the bite opens anteriorly around 2.5 mm (Castroflorio et al., 2013). The described biomechanical features of bite ramps avoid the common teeth intrusion induced by the thickness of the aligners and by the interocclusal contacts. The lower arch levelling with anterior intrusion, associated to posterior relative extrusion or at least with maintenance of vertical position of posterior teeth, will complete the approach. The posterior disocclusion that is maintained stable throughout the treatment by means of bite ramps allows the production of a significant amount of pure posterior extrusion if properly associated with the use of short Class II elastics and heavy posterior occlusal contacts. The slight pure extrusion associated to the relative extrusion planned by means of molar distal tipping and uprighting of the molar and premolar torque (3D curve of Spee levelling) will support the clockwise rotation of the mandible. Moreover, the precision bite ramps will in particular redirect the occlusal force exerted by the muscles creating an anterior prematurity contact that will support the lower intrusion.
Analysing the superimposed lateral cephalograms of both patients it is possible to detect, with the vertical pattern of the patients, how the deep bite was fully corrected, in both cases, by means of a combination of significant proclination of the incisors and slight clockwise mandibular rotation induced by the relative posterior extrusion.
Furthermore, the vertical skeletal relations seem to be influenced by the use of these auxiliary features of the aligners since the cephalometric vertical indicators changed positively. No posterior intrusion and no bite effect were encountered at the end nor during treatment. The overall change of the vertical position of the posterior teeth was minimal but, as described above, the data in the literature support that small amount of posterior real or relative extrusion, induced by the appliance biomechanics, can result in significative deep bite opening due to the mandible clockwise rotation justifying the need of bite ramps as an effective feature in case of deep bite malocclusion. These aligner-embedded features, combined with proper 3D planning of curve of Spee levelling and other features such as extrusion attachment and pressure areas acting on the lower arch, provided better levelling of the curve of Spee and a more predictable result. No papers have been published analysing the use of bite ramps; the only study examining deep bite and aligners was conducted before the introduction of these features (Khosravi et al., 2017). Following this approach, the treatment of deep bite could represent an elective choice for aligner system (Figure 8) avoiding the problems strictly connected to lower occlusal interferences commonly encountered during fixed a appliance approach and achieving an ideal outcome in a shorter treatment time.

Cases 1 and 2: comparisons between clinical result and digital plan.
Conclusion
In conclusion, deep bite treatment with aligners and bite ramps demonstrated to be a reliable and efficient option. Bite ramps represents a fundamental feature to manage the 3D levelling of the curve of Spee, combining anterior intrusion with posterior relative and real extrusion; they still need further investigation since no scientific papers have analysed their use. Occlusal contacts need to be properly designed during the digital setup to achieve a good posterior intercuspation at the end of the treatment. Class II elastics directly connected on the aligners are useful to translate the force on the teeth to achieve proper proclination of the lower incisors and ideal posterior intercuspation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.