
Abstract

We recently published the findings of a Journal of Orthodontics reader survey and, reassuringly, while you cannot please all of the people all of the time, the feedback was generally good (Jennings et al., 2021). Among the themes that did emerge, was a feeling that the Journal is quite academic and does not necessarily report in subject areas of direct interest to the whole orthodontic team. In particular, there was a suggestion that primary care orthodontics is not sufficiently represented in the articles that are published. With this in mind, I recently asked Guy Deeming if he would be interested in writing a column for the Journal, relating to wider issues in orthodontics with some emphasis on primary care. I am delighted to say that after a little bit of arm-twisting he has agreed. When we started discussing possible subject areas, the issue of direct-to-consumer (DTC) orthodontics came up (Figure 1), and given that this is likely to affect all orthodontic providers over the coming years, we thought it might be a suitable domain to put down some combined thoughts to start things off. A regular column for the Journal of Orthodontics focussing on issues in primary care orthodontics might ostensibly represent something of a challenge. However, in the current climate the challenge is not necessarily finding something to write about, but more finding subject matter that will still be relevant when the article actually appears in print! The rate of change in the post-COVID landscape of primary (and indeed, secondary) care orthodontics is so rapid that it feels unprecedented in the history of our specialty.
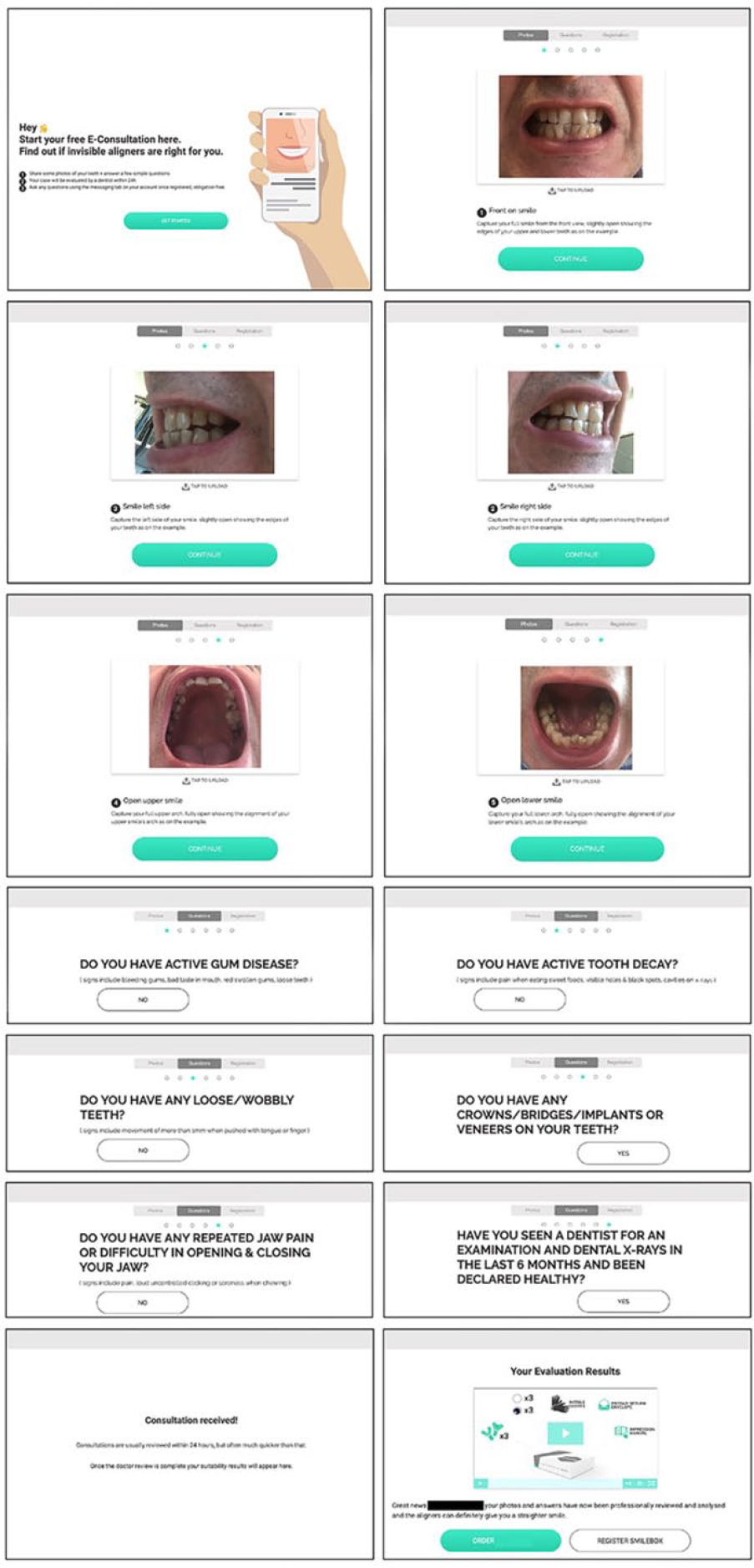
One of your correspondents was able to gain acceptance for a course of direct-to-consumer orthodontics following an examination based upon very simple photographs.
Suitable stimulus for a subject came in May from an unlikely source, when the General Dental Council (GDC) published their guidance for the general public in relation to treatment with ‘Aligners or braces sent directly to your home’ (GDC, 2021). The orthodontic profession will have read, absorbed and digested this publication very rapidly on release, with a combination of hope and trepidation, we are sure. Primarily, hope that it may provide some recourse in the face of a seemingly unstoppable wave of DTC orthodontic treatments. However, we were actually not so surprised that the GDC stance was not the regulatory broadside that might stop this trend in its tracks. Why might this be? Well, most significantly the DTC aligner manufacturers are seemingly playing to different rules than GDC registrants, and hence the GDC statement, rather than a David versus Goliath victory, may be nothing more than a small pot-shot brushed away without a scratch. So, what to make of the GDC’s work – is it all bad? The answer is no, we do not think so; and neither do we think the shortcomings and weaknesses therein are necessarily the fault of the GDC. The advice is good, excellent even; but the sad truth is that it seems very unlikely that the GDC message will get into the line of sight of those who may benefit most. Even if there were meaningful penetration, with features on Jeremy Vine and in the Daily Mail, when up against DTC companies underpinned by multibillion-dollar equity and eye-watering marketing budgets, it will be an almost impossible challenge. Even more so, when the companies in question are focussed on establishing market share and brand awareness with scant regard for profit. Although perhaps the biggest barrier is whether ‘consumers’ considering these options really want to be ‘advised’ at all. The uneasy truth is that there may be a reason that these companies exist and reasons why consumers are looking to them to solve their problems. A point worth returning to.
The GDC release is clear and sensible in its language, focussing on the three main domains of ‘Who is treating you’, ‘Valid consent’ and ‘Is the treatment safe?’ These headers have deliberately been put in a reverse order to the original statement from the GDC, as the message within the ‘Who is treating you’ section is the most potent to date, in one specific area. There it is stated that DTC services do fall within the legal practice of dentistry and therefore those engaged in the delivery of these services (in any capacity) are subject to the same professional standards as other registrants. So far so good, because by implication this also means that should any aspect of a DTC service be carried out by a non-registrant, then these individuals would then be at risk of prosecution within the 1984 Dentist Act for the illegal practice of dentistry.
This is double-edged because one of the key aspects of DTC provision is the self-administration of impressions and the dispatch of aligners from manufacturing facilities outside of the UK and therefore GDC jurisdiction, direct to patient (or should we continue with consumer?) homes. It is hard to see how the clarity offered by the GDC will have any impact on this route to treatment fulfilment. Where the GDC statement may have more bite is with the numerous high-street scanning/smile-shops/smile-centres/spas that have popped up in town centres over the last 24 months. One suspects and hopes that our regulators will now be looking very closely at these clinics, who is working in them, and the correct application of all the multiple standards and governance requirements that guide and regulate our own clinical practice.
Before leaving this issue to think about the ‘Why?’, there are two more concerns. The first relates to those registrants who are at risk of regulation by working in these high-street clinics. In particular, it is a concern that orthodontic or dental nurses are potentially being enticed into these environments and unwittingly operating outside their scope of practice and putting their registration at risk. For this to be the case would be a travesty of justice and we would make a plea to the dental nursing organisations to do all they can to ensure their members are fully informed and aware of the GDC stance. The second concern is again another plea – this time to the Care Quality Commission (CQC); because now the GDC has offered clarity, the path is clear for the CQC to carry out its work and ensure that all high-street scanning clinics are operating to the expected levels of safety, indemnity and governance as others providing clinical services. On this second point there has been some progress because the CQC have released a statement clarifying their position in light of the GDC statement, indicating that procedures such as intra-oral scanning, or even a patient taking their own impressions, does fall within the CQC remit as regulated activities (CQC, 2021). How effectively the CQC can enforce their powers in this context will be the next question, particularly with some DTC organisations fulfilling orders from outside the UK and by default, the jurisdiction of both the CQC and GDC.
This article is not intended as an apology for the GDC, far from it; but viewing this statement in the context of the mandate set out in the Dentist Act for the regulator, it is very hard to see how more can be done without a change or amendment to the Act itself, which requires legislation in parliament or an unimaginably deep information campaign. When the marketing spend for DTC companies exceeds the entire GDC budget – there it ends. Or does it? We have all been watching this market develop from the wings, feeling both powerless and frustrated in equal measure at the ‘impertinence’ of patients taking their own impressions in lieu of ‘proper diagnosis, treatment’ and so on. These feelings and this reaction are understandable, but it does not help either the profession or the patients who may suffer harm by the ‘folly’ of their own decisions and at their own hand. Indeed, many patients have a fundamentally different approach to treatment these days, particularly those from the younger generation. This possibly explains how a 15-year-old patient in fixed appliances under the care of one of the authors took herself off to a flat in Lewisham, London during the lockdown and had her tongue pierced by a beautician she had only liaised with through social media. All completely unbeknown to her mother!
This discussion should credit the work of Richard and Daniel Susskind, who have written extensively about the ongoing evolution of a ‘post-professional society’ (Susskind and Susskind, 2015). Equally, we were all full of scorn when in 2017 Michael Gove stated that ‘the people of this country have had enough of experts’. So, what is going on? The hard truth is that patients only become ‘patients’ once actively engaged in the receipt of clinical care. Until that point, the behaviours, interactions and expectations in the foothills of treatment are viewed, considered and managed by an individual alongside their raft of other consumer decisions being made on a daily basis. An entrenched belief that dentistry or orthodontics has entitlements handed down on tablets of stone to avoid being subject to the same set of rules is naïve and anachronistic.
Those considering doubling down on their position that the ‘expert’ in the white coat commands both the platform and ear of the consumer and that the model of orthodontic care, which has worked so well for so long and will continue to do so, should take a moment to review the well-documented death throes of Kodak, Blockbuster or any one of the many other seemingly untouchable corporations who failed to realise that how their customers chose to engage with their products and the world had changed.
And so it is now, in that the regard that was once held for professions and those in authority—doctors, lawyers, dentists—has been eroded. The generations that will define society now look to their peers through YouTube and the hive-mind of the numerous online review sites and forums for advice and validation. The power of the Google review or Facebook ‘like’ far outstripping the clever restaurant review in a broadsheet or entry in the Good Food Guide or TimeOut (pointedly, neither no longer produced in print form). Indeed, should the ‘expert’ deem it necessary to proclaim the people wrong, then they will be the unwitting recipient of the wrath and scorn of the collective consumer voice.
Like orthodontists, the London taxi has for decades delivered an efficient service, but now the entire London taxi system is under grave threat from Uber-isation in its purest form. Predictably, the establishment monopoly provider has pressured regulators and lawyers in an attempt to pull the rug from beneath the disrupter. Disruption to the taxi market is still ongoing, with the field now even more crowded with competitors offering further refinements and improvements to the original disruption model, evolving with haste in the light of feedback, consumer engagement and business metrics. Most importantly they are listening, not to the customers they already serve, but to those communities they want to, in order to build and sustain their work. Does this ring warning bells?
All the taxi disruptors have done (as have many before) is to identify the failings of the current monopoly provider in meeting the needs and demands of the community and leverage the benefits of the available technology. Whose fault is that? The disruptor for seeing the opportunity to do better for those they seek to serve, or the existing provider for an assumption that it need not change on the basis of a legacy market position and ‘credibility’. The reality is that travelling in the back of a London taxi is a nice, even pleasurable (albeit expensive) experience, but that in itself may not be enough to sustain the model when burdened by inconvenience and increased cost in the face of a viable alternative that acknowledges and solves these shortcomings. Indeed, who needs to do the Knowledge when you have a SatNav on your smartphone?
So where now? The GDC cannot save the profession from the ‘threat’ of DTC, so perhaps the profession must save itself? We should start to more proactively assert that we have something of value, something meaningful to offer people considering orthodontic treatment. We should also have the confidence that there are a huge number of people who can benefit from our work and will appreciate the value of experience, skill and training, which comes from being a regulated professional. The DTC aligner companies can only show ‘halfway to straight teeth’ for so long – they will need to start showing how the teeth look at the end of treatment.
The answer is not to give up on clinical orthodontics – the treatment on offer is not the problem. Perhaps the solution is to reframe the delivery of care to suit the needs and expectations of the next generation of ‘patients’, making sure the treatment we can offer is more accessible, more empathetic, more convenient and more consumer-centric. Once it is as easy to access professional-led orthodontic treatment under a redrawn model of care as it is to travel the lonely path of ordering aligners online, then there will be no competition.
Herein lies the challenge: how to redefine what is orthodontic care in the context of rapidly changing consumer behaviour and increasing choice in a post-COVID world. It is difficult, but not impossible. Netflix pivoted where Blockbuster failed. But is the quality of the product worse as a consequence? Inarguably not. Did the Hollywood establishment say it would be? Of course they did, as they entrenched their position to defend their world view with a perception that such changes were a threat to their livelihoods. To paraphrase the Susskinds, ‘if technology is threatening the profession then the profession is doing it the wrong way’.
In the end, there has to be an acceptance that we no longer get to make the rules of how people will engage with us. In the eyes of the consumer, the orthodontic establishment no longer has a monopoly on tooth straightening. We know the reality that offering orthodontic care is very different to putting aligners in a box, but consumers either do not know or do not care enough to find out. Whether we like it or not, we are now being disrupted. In an unlikely turn of events, it looks very much like the pandemic may have delivered a shock to the system, with the potential to drive the profession to disrupt itself and reinvent from the inside: to reconsider what is important in a patient journey; to identify opportunities to go virtual; go digital; leverage technology; reduce face-to-face contact.
To finish where we began, the emergence of the DTC model is not the fault of the GDC, nor even the DTC companies. If the DTC concept succeeds at the profession’s expense, it will be our fault by failing to leverage our services in the minds of people who want their teeth straightened and offer care through accessible, convenient and empathetic means. We need to compete with the DTC model while maintaining our core professionalism (Figure 2). To quote the Susskinds for a final time: ‘If we leave it to professionals themselves to reinvent their workplace, are we asking the rabbits to guard the lettuce?’ This is the threat and the opportunity granted to us. DTC and the pandemic have opened a window of opportunity, and we should aim to not prove the Susskinds right.
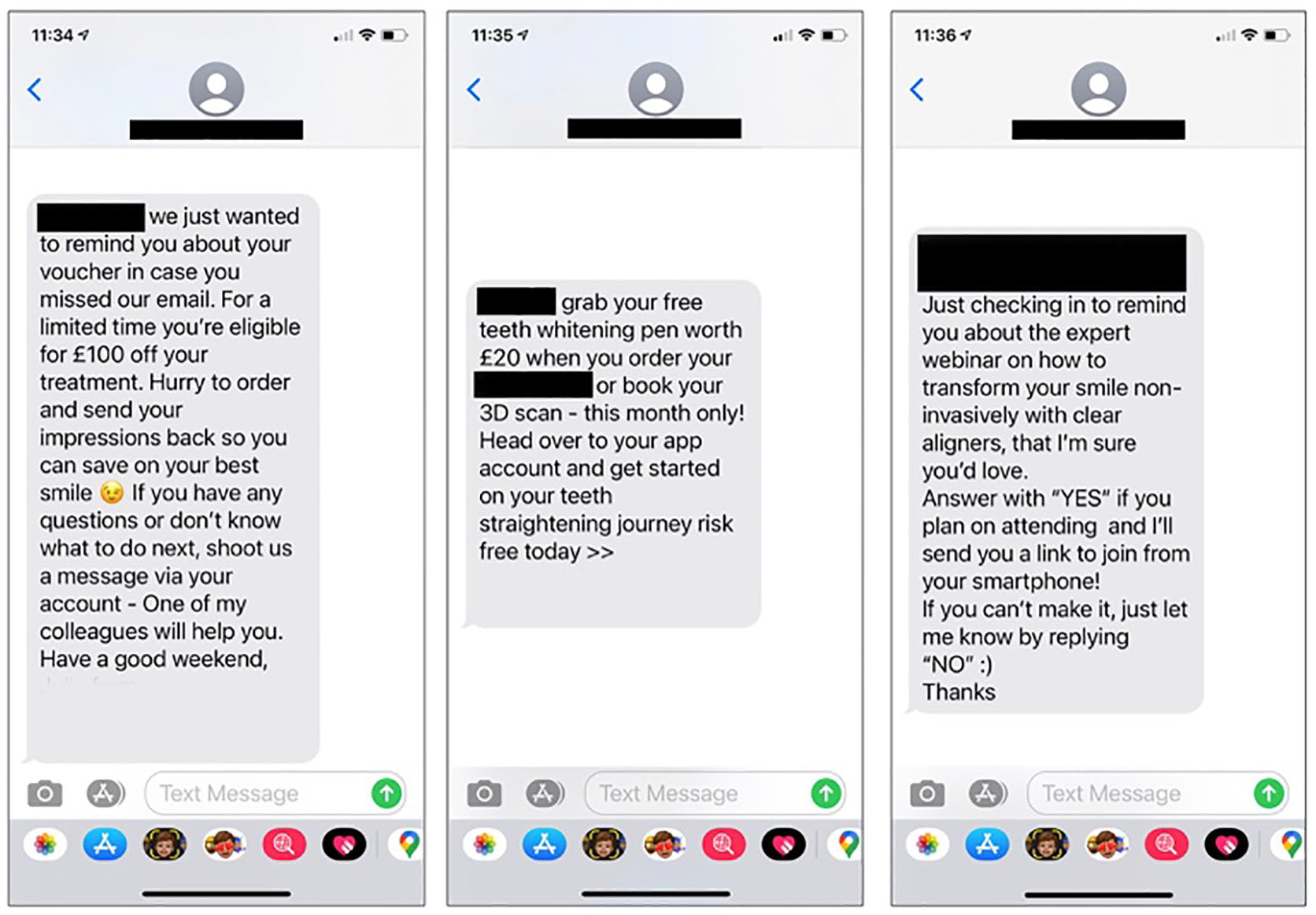
The initial consultation heralds a prolonged period of follow up from the direct-to-consumer orthodontic provider.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.