
Abstract
Objective:
To examine the diagnostic value of orthopantomograms (OPG) in the identification of root resorption of lateral incisors, secondary to an impacted canine, as confirmed by a cone-beam computed tomography (CBCT) scan.
Design:
Retrospective observational cohort study.
Setting:
South Wales secondary care setting: Royal Gwent Hospital, Newport and Nevill Hall Hospital, Abergavenny.
Methods:
A total of 40 consecutive patients with impacted canines between January 2018 and December 2019 were selected. For each patient, one consultant orthodontist examined the OPG in isolation to detect the presence and extent of resorption of lateral incisors. The CBCT report was then studied to confirm the presence and extent of pathology. Sensitivity, specificity, accuracy, positive predictive values and negative predictive values were calculated.
Results:
In total, 19 maxillary right canines, 18 maxillary left canines, one mandibular right canine and two mandibular left canines were examined. Impactions were more prevalent in the maxilla (92.5%) with higher predilection towards female patients (65%). There was higher prevalence of root resorption in the maxillary right quadrant (57.1%), in concordance with other studies. OPGs were found to have a sensitivity of 81.0% and a specificity of 10.5%, with an accuracy value of 47.5%. Positive and negative predictive values were found to be 50.0% and 33.3%, respectively. The extent of root resorption was incorrectly estimated from the OPG in 84% of cases. Correct estimation occurred in 16% of cases, with overestimation and underestimation occurring in equal proportion (42%).
Conclusion:
This study demonstrates the limitations of plain film radiographs and the merits of using CBCT in the accurate diagnosis of resorption of lateral incisors with an associated impacted canine. It also gives an indication into the location prevalence of resorption in a small cohort of patients. This preliminary study establishes the basis for future, larger-scale studies where outcomes can be generalisable at a population level.
Keywords
Introduction
Orthopantomograms (OPGs) have traditionally been used as a diagnostic tool for the presence and location of impacted canines and associated pathologies. However, the introduction of cone-beam computed tomography (CBCT) in 1998 represented a true paradigm shift in dental and maxillofacial imaging. CBCT imaging is capable of providing accurate, submillimetre-resolution images that enable three-dimensional (3D) visualisation of the oral and maxillofacial complex (Shukla et al., 2017).
Dental CBCT utilises a cone or pyramid-shaped beam using largely flat-panel detectors for 3D image reconstruction with high spatial resolution (Kiljunen et al., 2015). CBCT images contain isotropic volume elements (0.075–0.4mm isotropic voxel), which have equal dimensions in all planes. Therefore, CBCT can provide multiple orthogonal images in coronal, sagittal and axial views to allow detailed visualisation of anatomical structures. This offers many clinical advantages to conventional, two-dimensional (2D) plain film imaging with ongoing technological advances and innovation promising the potential to yield further clinical benefits.
Currently, CBCT is utilised in a variety of dental applications and specialties such as endodontics, periodontics, implantology and orthodontics (Abdelkarim, 2019).
Within orthodontics specifically, CBCT has a variety of uses, including:
• Localisation and assessment of retained or impacted teeth and associated pathology, e.g. root resorption
• Assessment of morphological anomalies, e.g. dilaceration, macrodontia, etc.
• Assessment and planning of complex orthognathic cases
• Assessment of the temporomandibular joint complex
• Assessment of patients with cleft palate (Garib et al., 2014; Machado, 2015)
In the assessment of the impacted dentition, CBCT is used to help evaluate the prognosis of alignment as well as potential resorption of adjacent teeth and the diagnosis of developmental pathology, such as supernumeraries and cystic changes. The most common pathological consequence of ectopic canines appears to be resorption of the adjacent lateral incisors. Ericson and Kurol (1987) determined that 12.5% of incisors associated with an impacted canine had some degree of root resorption when assessed with 2D plain film images. However, more recent work using CBCT found 38% of incisors had some degree of root resorption (Ericson and Kurol, 2000b). This value was as high as 66.7% in other CBCT studies, suggesting a historic precedent for the underestimation of disease using plain films (Walker et al., 2005).
The clinical management of an affected lateral incisor depends on a number of factors, including the following: the overall malocclusion; space requirements in the arch; position and prognosis of the associated ectopic canine; and the extent of resorption of the adjacent lateral incisor. A comprehensive CBCT report can, among other things, be invaluable in providing information regarding the extent of any associated pathology to the adjacent incisors, which is a fundamental component of the decision-making process (Wong and Khan, 2016b).
However, although CBCT involves a lower radiation dose and yields higher spatial resolution than conventional CT, this type of imaging involves a higher effective exposure dose than alternative imaging modalities in dentistry. It is therefore essential that all exposures are clinically justified. The diagnostic benefit must exceed the individual detriment that radiation exposure may cause. This is particularly true in growing patients more susceptible to stochastic biological effects (Roberts et al., 2014).
Plain film radiographs, specifically OPGs), have a lower effective dose and have been shown to have some use in detecting resorption; however, studies have found this type of imaging to be unreliable for root assessment (Nardi et al., 2017; Sosars et al., 2020; Wong and Khan, 2016a). When examining for dental root fractures, a study by Wang et al. (2011) determined CBCT scans to be significantly more accurate (91.9%) than plain film radiographs (48.1%). Similarly, a study by Dudic et al. (2009) studying 275 teeth found that resorption was detected in 69% of the dentition when assessed by CBCT, but only 44% when assessed by an OPG. Reasons for this include image magnification, distortion and superimposition of anatomical structures over the region of interest. When using plain film radiographs alone, even cases of severe resorption can remain undiagnosed (Alqerban et al., 2011; Ericson and Kurol, 2000a; Jawad et al., 2016).
Approximately 40% of the patients referred to the orthodontic department of the Royal Gwent Hospital, Newport and Nevill Hall Hospital, Abergavenny present with ectopic canines. As part of a multidisciplinary approach to treatment in secondary care, CBCTs are taken in addition to plain films for a number of reasons, particularly where radiographs are inconclusive with regard to pathology or resorption of adjacent teeth or where accurate localisation is required for surgical purposes, prognosis for alignment or treatment planning. Between January 2018 to December 2019, approximately 54% of canine referrals to the department required CBCT imaging, reflecting the complexity of cases received in secondary care. Most commonly, a 5-cm standard resolution scan is performed, with an average effective dose of 140 µsv. This allows for accurate diagnosis and treatment planning, specifically determining whether to expose or extract ectopic canines and whether to accept or extract dentition affected by pathology.
The aim of the present retrospective observational cohort study was to examine whether the presence and extent of resorption could have been detected from an initial OPG before a CBCT scan was performed, therefore determining whether an OPG alone is an adequate diagnostic tool.
Materials and methods
As this was a retrospective study, in line with guidance from the Royal College of Radiologists, no formal ethical approval was required. The collected data were anonymised, and all steps were taken to ensure that the study was conducted ethically.
Where a condition is thought to have a prevalence of 90%, the minimum sample size required for both screening and diagnostic studies is estimated at 22 and 34, respectively (Bujang and Adnan, 2016). The prevalence of lateral incisor resorption secondary to canine impaction is in the range of 27% (Liu et al., 2008) to 66.7% (Walker et al., 2005). Therefore, a sample size of 40 was deemed to be suitable for the purpose of this preliminary study.
Forty consecutive patients between January 2018 to December 2019 were selected from the CBCT list of two consultant orthodontists for inclusion in the study. Cases that did not involve impacted canines were excluded as well as cases involving patients aged > 18 years. The indication for CBCT referral in these cases was not limited to the diagnosis of root resorption and, as such, this ensured reasonable variation in the case mix. The patients were anonymised and assigned a number from 1 to 40.
All patients were referred to the orthodontic department of either the Royal Gwent Hospital, Newport or Nevill Hall Hospital, Abergavenny. In all cases, the patient had an initial digital OPG radiograph and were diagnosed with one or more maxillary and/or mandibular ectopic canines. Supplementary images used to carry out parallax view analysis were discarded for the purpose of this study in order to evaluate the diagnostic merits of an OPG radiograph in isolation.
All patients had been subsequently referred to the University Hospital Wales, Cardiff for a CBCT scan. The report was used to confirm the presence and extent of resorption of the adjacent lateral incisors. All 40 scans were of diagnostic quality and were reported by a single consultant dental and oral maxillofacial radiologist (the CBCT assessor).
For each of the cases, one consultant orthodontist (the OPG assessor) examined the OPG radiograph in isolation to diagnose the presence and extent of resorption of the adjacent lateral incisor. The risk of recall bias was mitigated by sampling from cases referred over six months before data collection. Owing to the differing indications for CBCT referral, the assessor was not expected to assume there was root resorption in the included cases. A single consultant was used as the OPG assessor to reduce inconsistencies related to inter-examiner variability. A retrospective intra-examiner reliability study was carried out to measure variability and assess test validity by measuring agreement levels between two separate scoring episodes. The assessor was found to have an 85% level of agreement between the scoring episodes, suggesting a high degree of reproducibility and reliability, where 60%–79% is considered moderate agreement and 80%–90% is considered a strong level of agreement (McHugh, 2012).
During data collection, all OPG radiographs were assessed digitally with the same computer monitor. Standardised lighting was used to replicate the clinical environment as best as possible. To reduce the effects of confounding variables resulting from cases with multiple ectopic canines, one canine was selected at random using a computer randomiser. The diagnosis was recorded using the following four categories based on the Malmgren Index:
• No resorption – no radiographic evidence of change (index score 0 and 1)
• Mild resorption – < 2 mm of root length loss (index score 2)
• Moderate resorption – > 2 mm but less than one-third root length loss (index score 3)
• Severe resorption – more than one-third root length loss (index score 4) (Levander and Malmgren, 1988)
The findings of the CBCT scan were recorded by detailing the extent of resorption as reported by the CBCT assessor. This was divided into the following four categories:
• No resorption – intact root surfaces, mild loss of cementum only
• Mild resorption – up to half of the dentine thickness lost
• Moderate resorption – more than half of the dentine thickness lost; no pulpal involvement
• Severe resorption – pulpal involvement (Ericson and Kurol, 2000a)
The presence of disease was recorded as a dichotomous measure, that is, present or absent. The extent of disease was recorded on a 4-point scale as outlined above, that is, nil, mild, moderate or severe. This was in line with the study by Leeds Dental Institute (Jawad et al., 2016). The same data collection sheet, designed for use in Microsoft Excel, was used to record the data for all cases, including the extent to which resorption was either overestimated, underestimated or correctly estimated. The results were tabulated (Table 2) and further analysed and presented graphically (Figures 1 and 2).
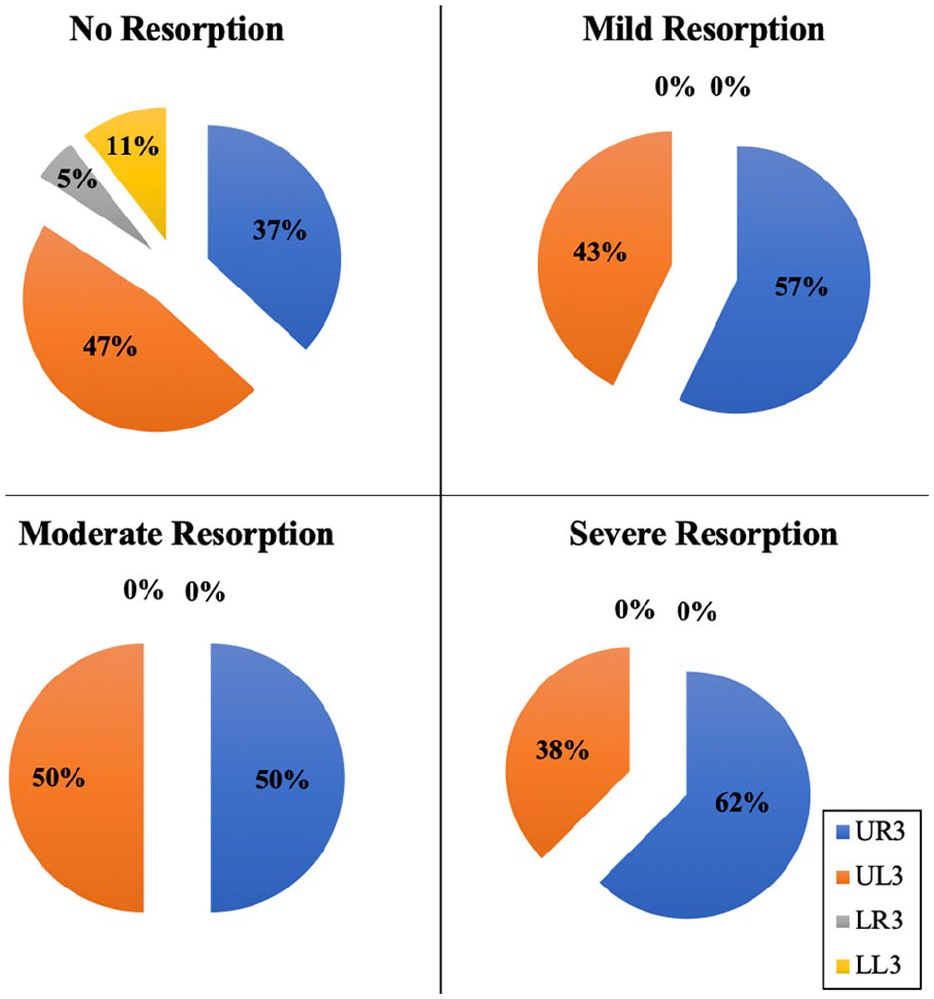
Extent of resorption when analysed for each individual tooth notation.
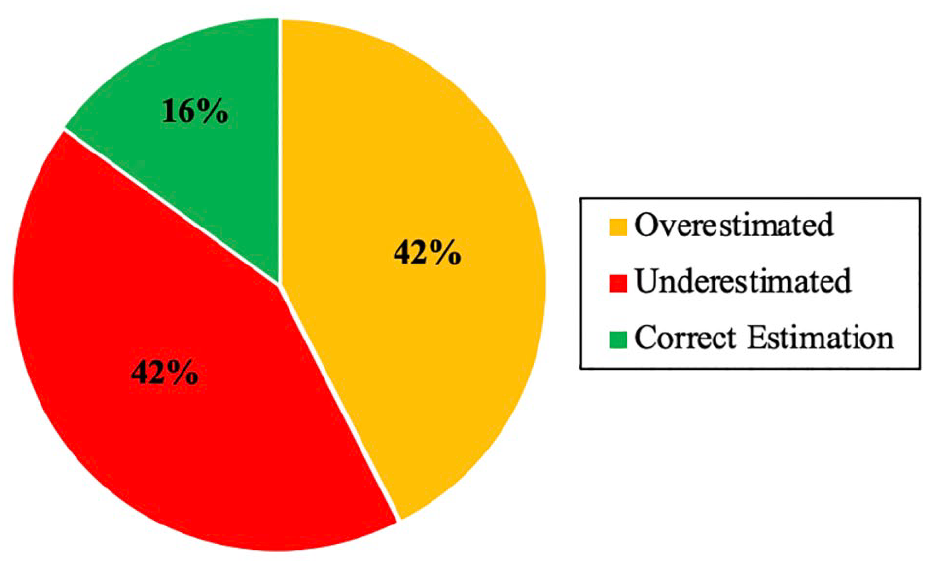
Accuracy of resorption estimated between the OPG radiograph and the CBCT report.
For the purpose of statistical analysis, the presence of disease (i.e. a positive diagnosis) relates to the presence of root resorption as seen in an OPG radiograph. A negative diagnosis relates to the absence of root resorption. The outcome of the CBCT scan was considered the gold standard used to confirm the validity of the diagnosis. The number of true/false positives (TP/FP) and true/false negatives (TN/FN) were recorded and tabulated for further statistical analysis. The following outcome measures were calculated as follows:
• Sensitivity (Sn); the diagnostic ability to identify the presence of disease (TP)
• Specificity (Sp); the diagnostic ability to rule out the presence of disease (TN)
• Diagnostic accuracy (Ac); the proportion of true results (both TPs and TNs) among the total number of cases examined
• Positive predictive value (PPV); the probability of disease following a positive result
• Negative predictive value (NPV); the probability of the absence of disease following a negative result
Results
The demographic and clinical profile of the sample set can be seen in Table 1. Of the 40 patients included in the study, 26 were female (65%) and 14 were male (35%), demonstrating a F:M ratio of approximately 2:1. The mean age of the cohort was 14.3 ± 1.9 years (age range = 10–17 years) at the time the CBCT scan was completed. The mean duration from OPG to CBCT for all cases was six weeks.
Demographic profile of study sample.
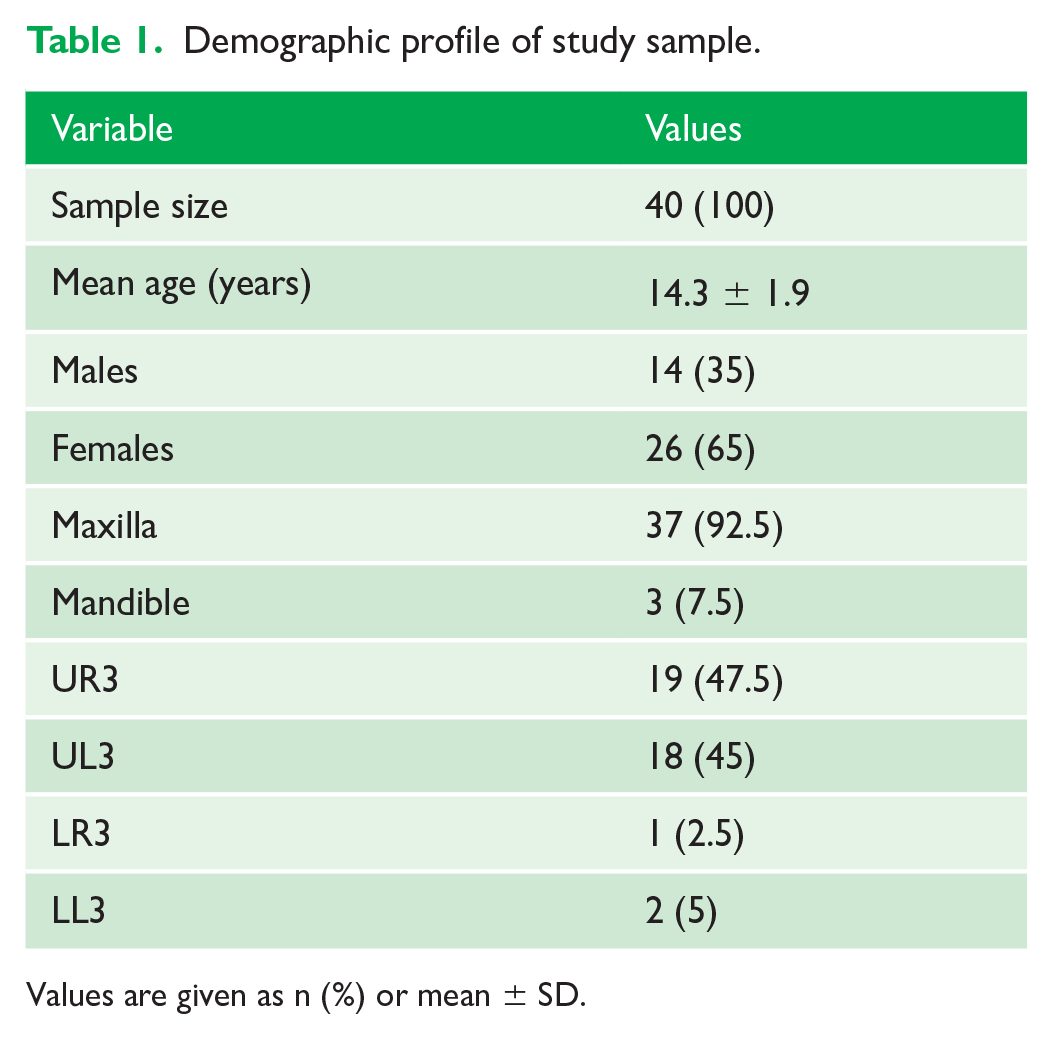
Values are given as n (%) or mean ± SD.
This study sample shows a higher prevalence of impaction in the maxillary arch, with 92.5% (n = 37) of impactions in the maxilla and 7.5% (n = 3) in the mandible. Of the 40 canines included, there were 19 maxillary right canines (47.5%), 18 maxillary left canines (45%), two mandibular left canines (5%) and one mandibular right canine (2.5%).
Tables 2-4 show the extent to which an OPG can identify the presence or absence of disease (root resorption) as validated by a confirmatory gold standard (CBCT scan). The data revealed that OPG analysis alone resulted in 17 diagnoses (42.5%) being FPs and 4 (10.0%) FNs. The data also showed that 17 diagnoses (42.5%) were TPs and 2 (5.0%) were TNs. Sensitivity of the OPG radiograph as a diagnostic tool was found to be 81.0% with a specificity of 10.5%. Accuracy was found to be 47.5%. These results are in concordance with the PPV and NPV of 50.0% and 33.3%, respectively.
Record of resorption determined from the initial OPG radiograph and the subsequent CBCT report in relation to an ectopic canine. False/true positive, false/true negative.
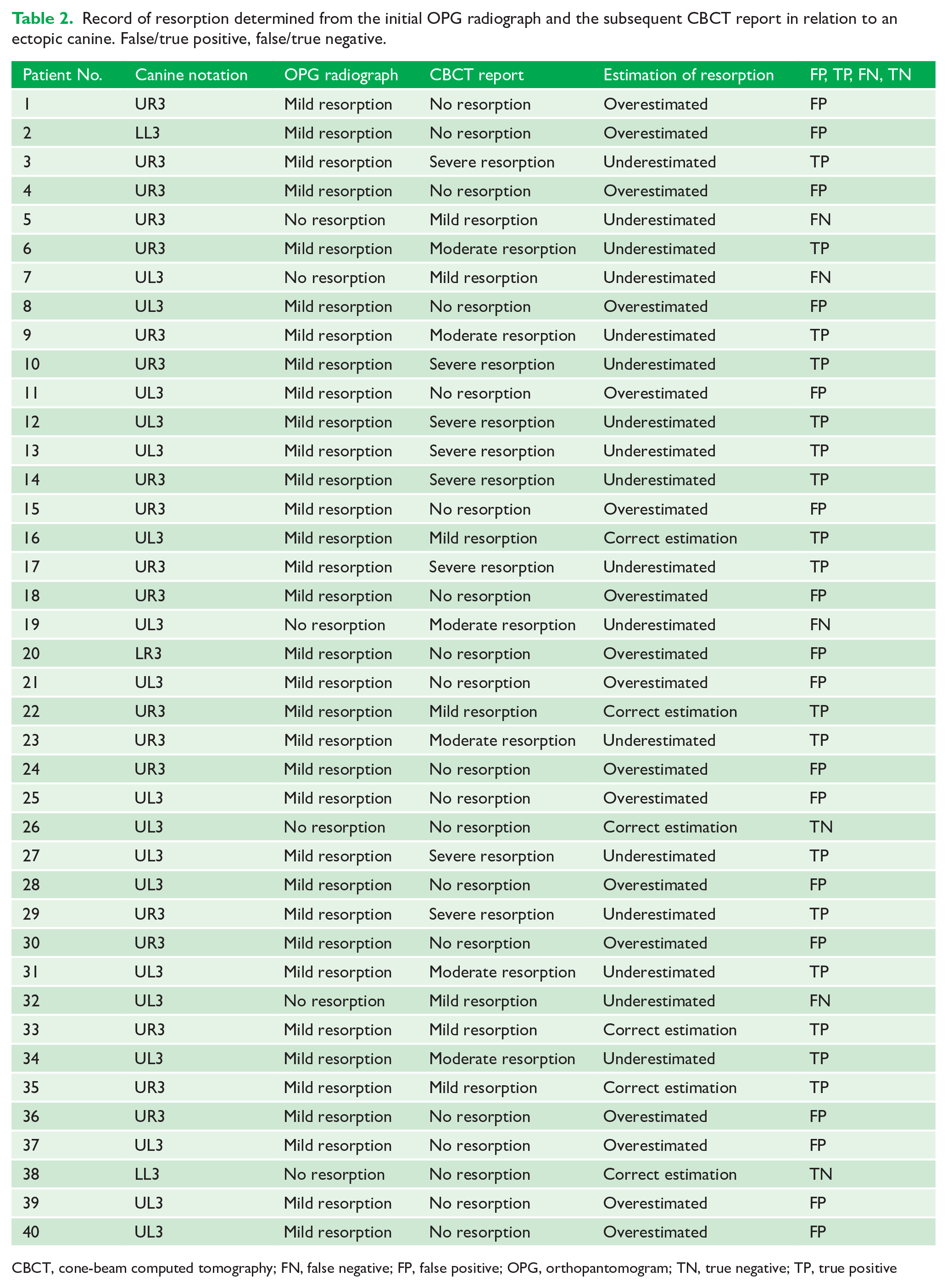
CBCT, cone-beam computed tomography; FN, false negative; FP, false positive; OPG, orthopantomogram; TN, true negative; TP, true positive
Statistical analyses and primary outcome measures.
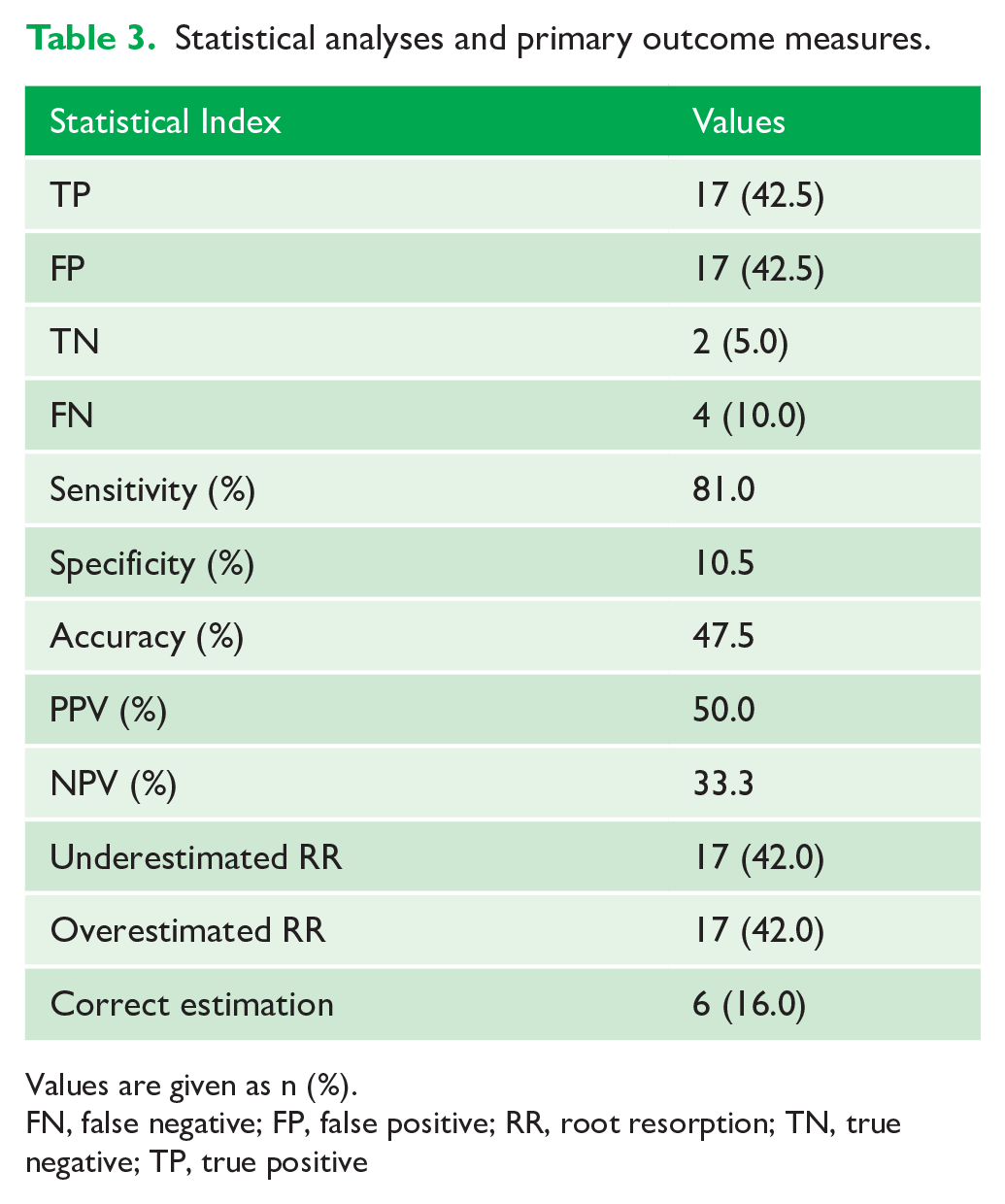
Values are given as n (%).
FN, false negative; FP, false positive; RR, root resorption; TN, true negative; TP, true positive
Contingency table (2×2) showing TPs, FPs, TNs, and FNs for OPG in relation to CBCT imaging for the diagnosis of resorption.
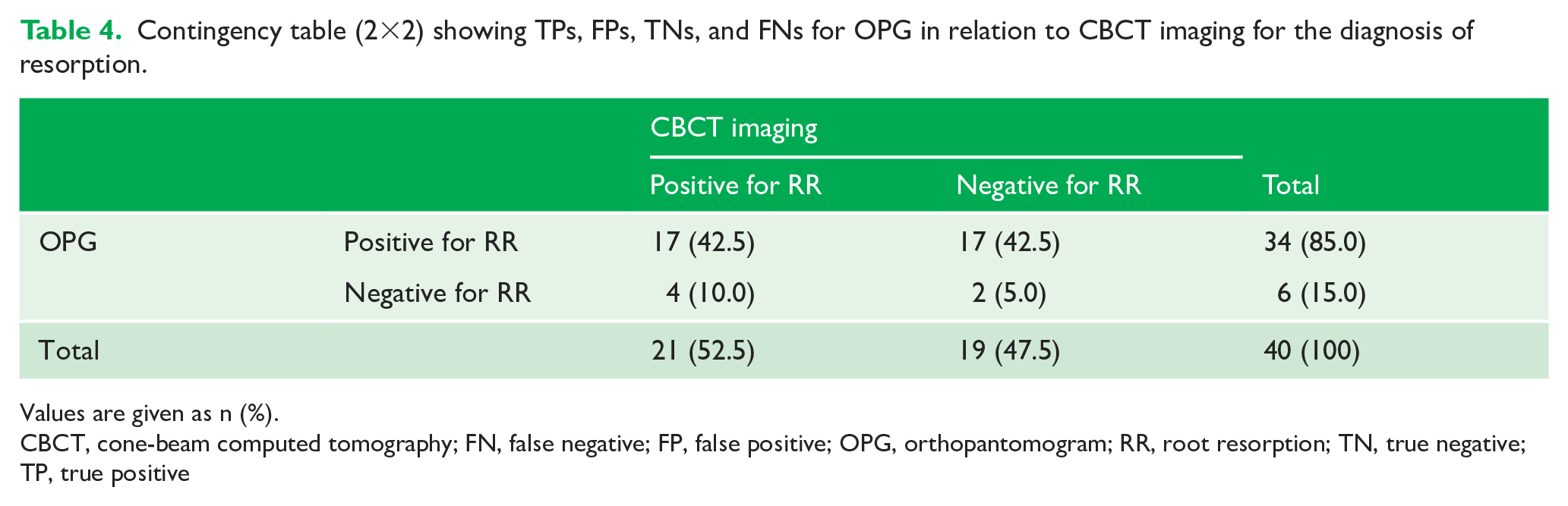
Values are given as n (%).
CBCT, cone-beam computed tomography; FN, false negative; FP, false positive; OPG, orthopantomogram; RR, root resorption; TN, true negative; TP, true positive
With respect to the ability to diagnose the extent of disease, Table 2 shows the reported degree of agreement between the initial OPG radiograph and the subsequent CBCT report in relation to the ectopic canine of that case. For each case, the accuracy of resorption estimated was identified and recorded as overestimated, underestimated or correct estimation. In 34 cases (84%), the extent of root resorption was incorrectly estimated from the OPG radiograph, with overestimation and underestimation occurring in equal proportion (n = 17, 42%).
While not a primary outcome of the study, the data reveal the extent of canine-induced resorption when analysed for each individual tooth notation. In this study sample, there was a higher prevalence of root resorption related to the maxillary right quadrant. Of the 40 cases, 21 lateral incisors were found to have resorption (52.5%), of which 12 involved the maxillary right canine (63% of UR3s) and nine involved the maxillary left canine (50% of UL3s). No resorption was detected by CBCT scans in the three cases involving impacted mandibular canines.
Discussion
Despite modern advances, CBCT scans continue to deliver a higher effective radiation dose per cubic centimetre than any imaging modality in dentistry. Nevertheless, it has been demonstrated that there are merits to using CBCT over plain film radiographs alone. This study has identified the limitations of panoramic radiographs in diagnosing the presence and extent of root resorption secondary to impacted canines. This study also gives an indication into the location prevalence of root resorption in a small cohort of patients.
The demographic profile of the sample was broadly representative of patients referred to the orthodontic department at both hospital sites. The sex distribution (65% girls, 35% boys) also correlates closely with previous findings where a study by Sajnani and King (2012) sampled 533 impacted canines and found that 61.4% of patients were female and 38.6% were male.
With respect to age, the sampling methodology was expected to yield a wide sample variance. However, while the cohort age was in the range of 10–17 years at the time the CBCT scan was completed, the mean age was 14.3 ± 1.9 years, showing that the sample cohort was relatively homogenous. The mean age closely reflects the average age at which impaction diagnoses are usually confirmed in the secondary care setting.
As this cohort of patients was limited to those which involved impacted canines and where CBCT was required, it is recognised that there was a potential risk of selection bias manifesting in an over-representation of FPs and an under-representation of TNs. However, given the multidisciplinary nature of the department, the indication for CBCT referral in these cases was not limited to the diagnosis of root resorption and, as such, there was heterogeneity in the case mix therefore mitigating the risk of excessive bias. A single OPG assessor was utilised to avoid bias attributed to inter-examiner reliability. An intra-examiner reliability study revealed a high level of agreement. Although case selection was limited to patients seen in excess of six months before data collection, some degree of ascertainment bias is acknowledged.
The data revealed that OPG analysis alone resulted in 17 diagnoses (42.5%) being FPs and 4 (10.0%) being FNs. When looking at OPG radiographs in isolation, we found that 34 of the 40 cases (85%) were deemed to have mild resorption of the adjacent lateral incisor. Subsequently, the CBCT report then confirmed some degree of resorption in only 50% of these cases. Conversely, in 6 of the 40 cases (15%), resorption could not be determined from the OPG radiograph alone. The CBCT scan then detected resorption in 4 (67%) of these cases. However, while a diagnostic deficiency has been identified, the overall sample size and the small number of cases with no resorption detected on the OPG means this relationship should be interpreted with care. Nevertheless, Ericson and Kurol (2000a) suggest that deficiencies in panoramic radiographs are likely due to distortion artefacts as various anatomical structures are projected into the field of view. Overlying structures can overlap the lateral incisor roots and the subsequent artefact may appear radiographically as resorption.
When considering diagnostic validity, this study shows OPG radiographs have a high sensitivity (81.0%) and low specificity (10.5%) in detecting root resorption. Sensitivity and specificity are a measure of the diagnostic capability of a test when compared to a gold standard or confirmatory test, in this case a CBCT scan. The factors contributing to sensitivity and specificity are not influenced by the prior probability, or prevalence, of disease (Chavarria-Bolanos et al., 2017).
A number of studies are in agreement that OPG sensitivity is higher than specificity, including in vitro studies by Alqerban et al. (2009) (78% sensitivity, 38% specificity) and Schroder et al. (2018) (78.2% sensitivity, 59.5% specificity). This suggests an increased probability that patients who are disease free are potentially being incorrectly informed of the presence of pathology from positive OPG findings. However, other studies contradict these findings, showing higher specificity than sensitivity (34.2% sensitivity, 95.8% specificity) (Nardi et al., 2017). This may be explained by the fact that Nardi et al. (2017) looked at teeth throughout the dental arch and, in fact, recognised that sensitivity significantly increased in the incisor region. Studies which incorporated the buccal segment dentition yielded significantly lower sensitivity values, owing to the multi-root morphology of the teeth and the proximity of the maxillary sinus. The low specificity found in our study may also be attributed to the small sample size, which consequently may exaggerate the percentage incidence of true/false positives/negatives.
The limitations of OPGs alone are also reflected in the predictive value of the diagnostic test. The study reveals that a PPV of 50.0% and a NPV of 33.3% are broadly in agreement with the findings of Nardi et al. (2017), who found a PPV of 89.1% and a NPV of 59.3%. While the magnitudes differ considerably, there is agreement between the two studies in terms of the relationship between the two values, where diseases of increasing prevalence are expected to result in tests with the NPV lower than the PPV. Our study suggests, in keeping with sensitivity and specificity, that in the presence of a positive diagnostic test (i.e. root resorption identified on an OPG), it is possible to expect the presence of disease, although this can only be confirmed with 50.0% certainty. Whereas a negative diagnostic test (i.e. no root resorption identified on an OPG) offers a slightly lower level of assurance of the absence of disease. From the findings of various studies, the trend of higher PPV values compared to NPV appears to be as true for root resorption as it is for root fractures (Wang et al., 2011) and periapical pathology (Estrela et al., 2008; Nardi et al., 2017). With all the above outcome measures considered, diagnostic accuracy of OPGs in identifying root resorption was estimated to be 47.5%. This value is in line with the plain film accuracy found by Estrela et al. (2008) (42%) and Wang et al. (2011) (48.1%).
In one particular instance, moderate resorption was determined from the CBCT report with more than half dentine surface loss, despite only mild resorption noted from the OPG radiograph. Researchers, including Alamadi et al. (2017) and Lund et al. (2012) explain how slanted surface root resorption, found in up to 15% of palatal root surfaces, is often missed on OPG radiographs and can only be evaluated on tomographic images, such as CBCT. An example of this can be seen in Figure 3. The premise behind this error is underpinned by the idea that the line of site of plain films can only detect tooth surface loss in the axial plane or in the mesiodistal aspects. Dudic et al. (2009) describes resorption as a 3D phenomenon. Buccolingual or buccopalatal surface loss will largely remain undetected on plain films, which is particularly problematic in the maxilla given that the majority of impacted canines are palatally ectopic and therefore cause palatal resorption.
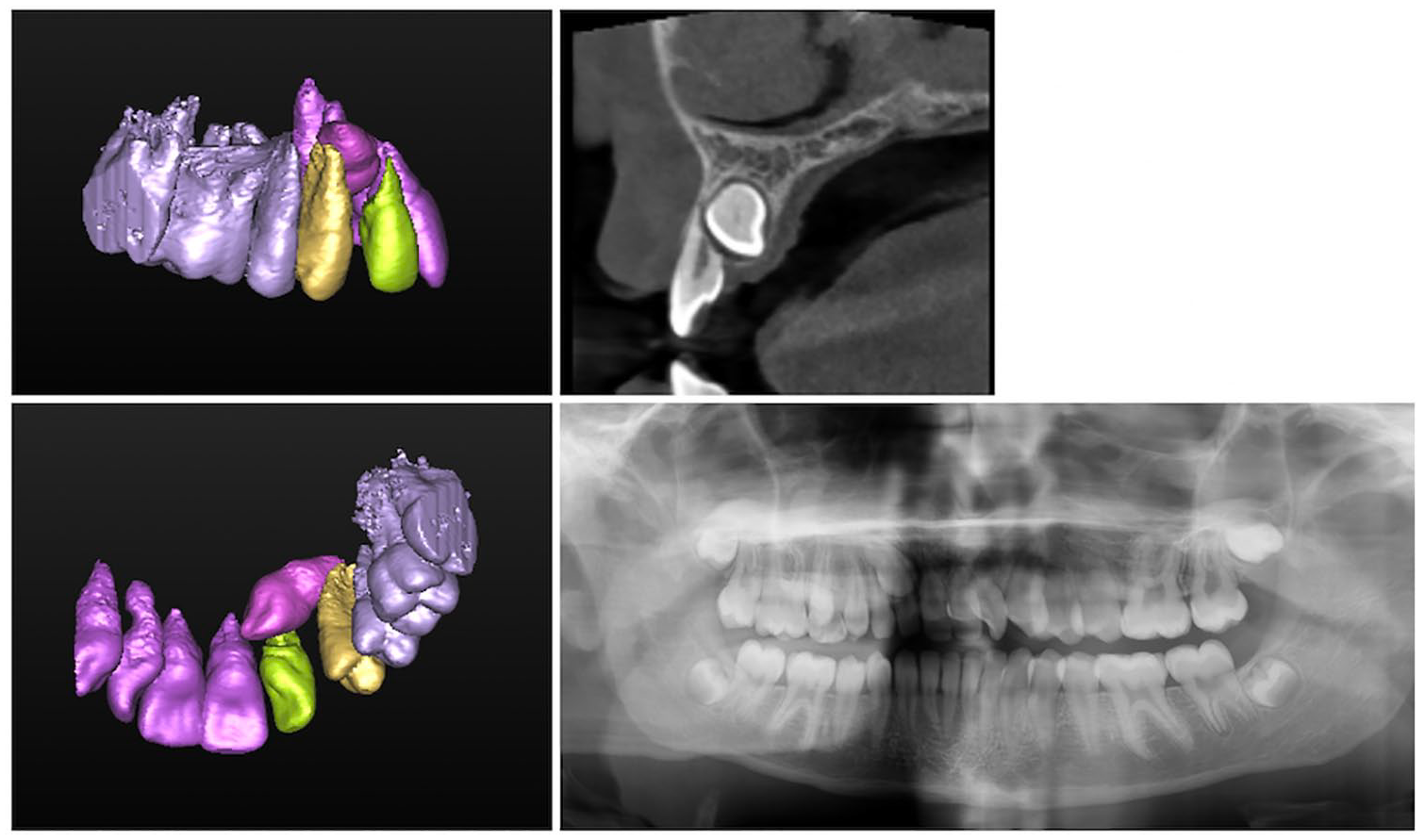
CBCT and plain film radiographs, where OPT was reported as showing no evidence of resorption. CBCT report identifies significant resorption of the upper right lateral incisor root with 5 mm of the root remaining buccally and 1.6 mm root remaining palatally. CBCT, cone-beam computed tomography; OPT, orthopantomogram.
With respect to the ability to diagnose the extent of disease, the OPG radiograph predominantly incorrectly estimated the extent of root resorption (n = 34, 84%); with overestimation and underestimation occurring in equal proportion (n = 17, 42%). These results should be interpreted with a degree of caution due to the inevitable margin of error arising from the differing metrics used for the OPG and the CBCT. Nonetheless, it is also possible that the degree of resorption was underestimated due to image distortion or superimposition of anatomical structures over the region of interest. Conversely, pathology may have been overestimated as a consequence of image magnification (Alqerban et al., 2011; Ericson and Kurol, 2000a). Foreshortening may also contribute to the overestimation of apical root surface loss, particularly in lateral incisors abnormally proclined due to crowding. This is a phenomenon unique to plain films where apices lie outside the focal plane as described by Dudic et al. (2009) in a study that concluded that apical root resorption after orthodontic treatment was underestimated by 25% when evaluated on an OPG. Furthermore, Ericson and Kurol (2000a) determined that the diagnostic validity and accuracy for detecting root resorption can be incorrectly estimated due to deficiencies such as blurred images and distortion projection errors as complex maxillofacial structures are projected onto a 2D plane, thus increasing the risk of misinterpretation. Figure 3 shows images for a patient where plain film radiographs underestimated the extent of resorption in a lateral incisor.
Although not a direct outcome measure, our results agree with other studies in showing ectopic canines occur most commonly in the maxilla (n = 37, 92.5%) compared to the mandible (n = 3, 7.5%) and therefore impacted maxillary canines are more likely to cause root resorption (Sajnani, 2015). All three of the observed mandibular canines had no associated incisor root resorption. However, the cohort included in this study did not include sufficient numbers of mandibular canines to be able to make definitive conclusions regarding the prevalence of resorption in mandibular lateral incisors.
Maxillary canines begin development high in the maxilla at approximately four months of age and pass along the distal root surface of the lateral incisor to reach their position in the arch. Therefore, this long and deviational eruption path of approximately 22 mm, described by Becker and Chaushu (2015), has been attributed to the increased prevalence of impactions in the maxilla compared to the mandible. This close relationship also explains the prevalence of resorption seen in lateral incisor roots in contrast to, for example, the adjacent first premolar. The authors found that the risk of impaction is further increased if the adjacent lateral incisor is diminutive or congenitally absent.
Furthermore, in our study sample, there was a higher prevalence of root resorption related to the maxillary right quadrant (57.1%) compared with the maxillary left quadrant (42.9%). Due to the small sample size, it is not possible to determine whether this difference is statistically significant. However, this was in agreement with a study by Liu et al. (2008), which sampled over 200 impacted canines and found that 62.1% were on the right side and 37.9% were on the left. Location predilection (right vs. left) has been attributed to genetic factors in much the same way as in cleft lip and palate, hypodontia (Sajnani and King, 2012) and other studies looking at canine location (Peck et al., 1994).
Limitations
There are a number of limitations recognised and discussed in this study, meaning conclusions should be interpreted with care and in context. While the sample size is similar to that seen in other studies (Alqerban et al., 2009; Bonfanti et al., 2019; Dudic et al., 2009; Jawad et al., 2016; Maddalone et al., 2019; Walker et al., 2005), it is recognised that the small cohort of patients reduces the external validity of the findings, particularly with respect to specificity. Similarly, some degree of selection bias and recall bias is inherently associated with the study design, although measures were taken to reduce their impact. Further, in much the same way as the study conducted in Leeds Dental Institute (Jawad et al., 2016), which measured disease seen in OPG and CBCT scans, our study used two different indices for the recording of resorption. This may have led to a systematic error and may impact on the assessment of severity of disease, although it is not expected to adversely affect the dichotomous measure for presence of disease.
These limitations potentially impact the magnitude of effects seen, particularly specificity which was found to be excessively low. However, the trends observed are likely to be of interest to inform future studies. It is recognised that panoramic radiographs can be beneficial as an initial screening tool when one or more ectopic canines are suspected, particularly given their multi-use function in orthodontic treatment planning. However, their use as a diagnostic tool for root resorption has been shown to be inadequate.
Conclusion
This study identifies the limitations of panoramic radiographs and the merits of using CBCT in diagnosing root resorption secondary to impacted canines. It also gives an indication into the location prevalence of resorption in a small cohort of patients. This preliminary study establishes the basis for future, larger-scale studies where outcomes can be generalisable at a population level.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.