
Abstract
Dental transpositions are rare anomalies, which may present to the general dental practitioner or orthodontist. Transpositions occur less frequently in the mandible compared with the maxilla, with the most common mandibular transposition involving the mandibular lateral incisor and canine. The degree of displacement can vary from a relatively minor deviation to complete transposition of the mandibular lateral incisor with the adjacent canine tooth. Due to their highly visible position at the front of the mouth, treatment, ideally involving alignment of these teeth, is important for aesthetic, social and functional purposes. This case series reports six cases with mandibular lateral incisor-canine transposition. They demonstrate the variety in presentation and subsequent management of the ectopic teeth. The importance of early diagnosis in combination with interceptive treatment is discussed, to reduce the burden of potentially lengthy orthodontic treatment at a later date.
Keywords
Introduction
Dental eruption has been defined as the movement of a tooth from its original position of development to a functional position within the oral cavity (Massler and Schour, 1941). Although dental eruption is usually an uneventful process, on occasion, changes in the normal pathway of tooth eruption may occur, leading to transposition. A transposition may be defined as the positional interchange of two adjacent teeth or the development or eruption of a tooth into a position ordinarily occupied by a non-adjacent tooth (Peck and Peck, 1995). This is a form of ectopic eruption, leading to a tooth developing in an aberrant position. The degree of transposition can vary from being incomplete, with the root still in its usual position, to being complete, with both the crown and root involved.
Transpositions are coded using three elements: the jaw of occurrence; the tooth that is transposed; and the site of transposition (Favot et al., 1986). Therefore, Mn.I2.C would represent the transposition of the mandibular lateral incisor to the canine position.
This paper discusses the aetiology of this condition, and how early assessment and diagnosis, in combination with interceptive treatment, may reduce the burden of orthodontic treatment required later.
In addition, this paper reports six cases with mandibular lateral incisor-canine transposition (Mn.I2.C) and describes the orthodontic management and implications when treating this rare developmental anomaly.
Aetiology
Transpositions of maxillary teeth are more common compared to mandibular teeth (Ely et al., 2006). The maxillary canine-first premolar (Mx.C.P1) and maxillary canine-lateral incisor (Mx.C.I2) are the most frequently encountered in the maxilla. In the mandible, lateral incisor-canine transposition (Mn.I2.C) is the most common. However, this type of transposition is still extremely rare, with a reported prevalence of only 0.03% (Peck et al., 1998). Though the precise aetiology of a Mn.I2.C transposition remains largely unknown, literature reports various possible causative local factors (De Paula et al., 2011; Plunkett et al., 1998; Shargill and Littlewood, 2020):
Crowding
Supernumerary teeth
Spacing
Premature loss of the adjacent primary tooth
Retention of the corresponding primary tooth
History of trauma to the area
Digit-sucking habit
In addition, there also appears to be a genetic basis, with a multifactorial inheritance pattern, as it is frequently associated with other dental anomalies, such as impaction and hypodontia (Ely et al., 2006).
Assessment
The mandibular lateral incisor normally erupts when the patients is aged 7–8 years. Therefore, the optimal time to assess for the development and path of eruption of the mandibular lateral incisors is in the early mixed dentition phase, when the patient is aged 6–8 years. Any primary tooth that is unduly firm, or retained past the period of time normally expected for exfoliation, should raise suspicions to the clinician of absence or ectopic positioning of the corresponding permanent tooth.
Radiographic investigation may be necessary to determine the presence and position of a potentially ectopic mandibular later incisor. The radiograph of choice is often a dental panoramic tomograph (DPT), which can also confirm the presence and position of nearby unerupted teeth and assess for any potential anomalies or pathology. On occasions, the ectopic tooth can be found as an incidental finding on alternative radiographs. For example, the bitewing radiograph taken for Case 1 to assess for interproximal caries also highlighted the presence of an ectopic left mandibular lateral incisor, which had migrated towards the furcation of the left mandibular first primary molar.
Presentation and treatment
Mn.I2.C transposition often presents with distal tipping and rotation of the lateral incisor as it erupts into the position normally occupied by the ipsilateral canine and premolar (Cases 1–6). In the early stages of a transposition, at approximately 8–9 years of age, there may only be an incomplete transposition, with the roots of the lateral incisors and canine still occupying their normal positions. At this stage, interceptive removal of the corresponding primary incisor +/– canine may lead to spontaneous improvement in the lateral incisor position. The decision can then be made later for the need for interceptive or comprehensive orthodontic treatment with fixed appliances.
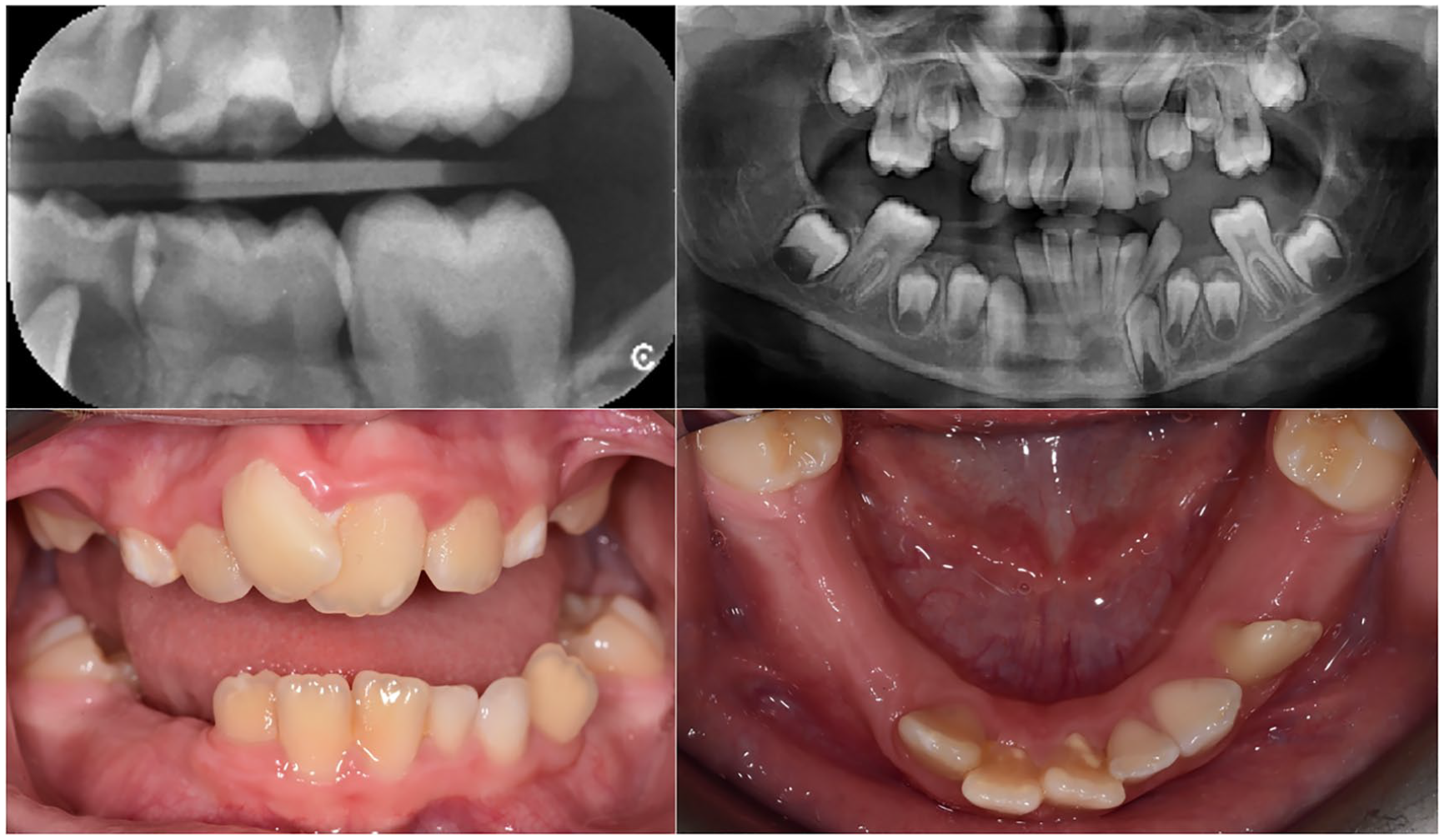
A 9-year-old male patient with poor oral hygiene and a displaced LL2 referred for an orthodontic opinion from Special Care Dentistry. The patient had previously undergone a general anaesthetic for extractions of carious teeth without an orthodontic opinion being sought. Note how LL2 is visible on the left bitewing and is causing root resorption to the LLD. Both LLB and LLC are firm with good root lengths. Earlier recognition of this malocclusion, with interceptive removal of these primary teeth may have led to less severe displacement of the LL2.

An 11-year-old female patient presented in the late mixed dentition with a displaced LR2. As the transposition was incomplete, orthodontic treatment was undertaken with fixed appliances to align this tooth. The patient’s compliance was not ideal throughout treatment, leading to acceptance of an undertorqued LR2.
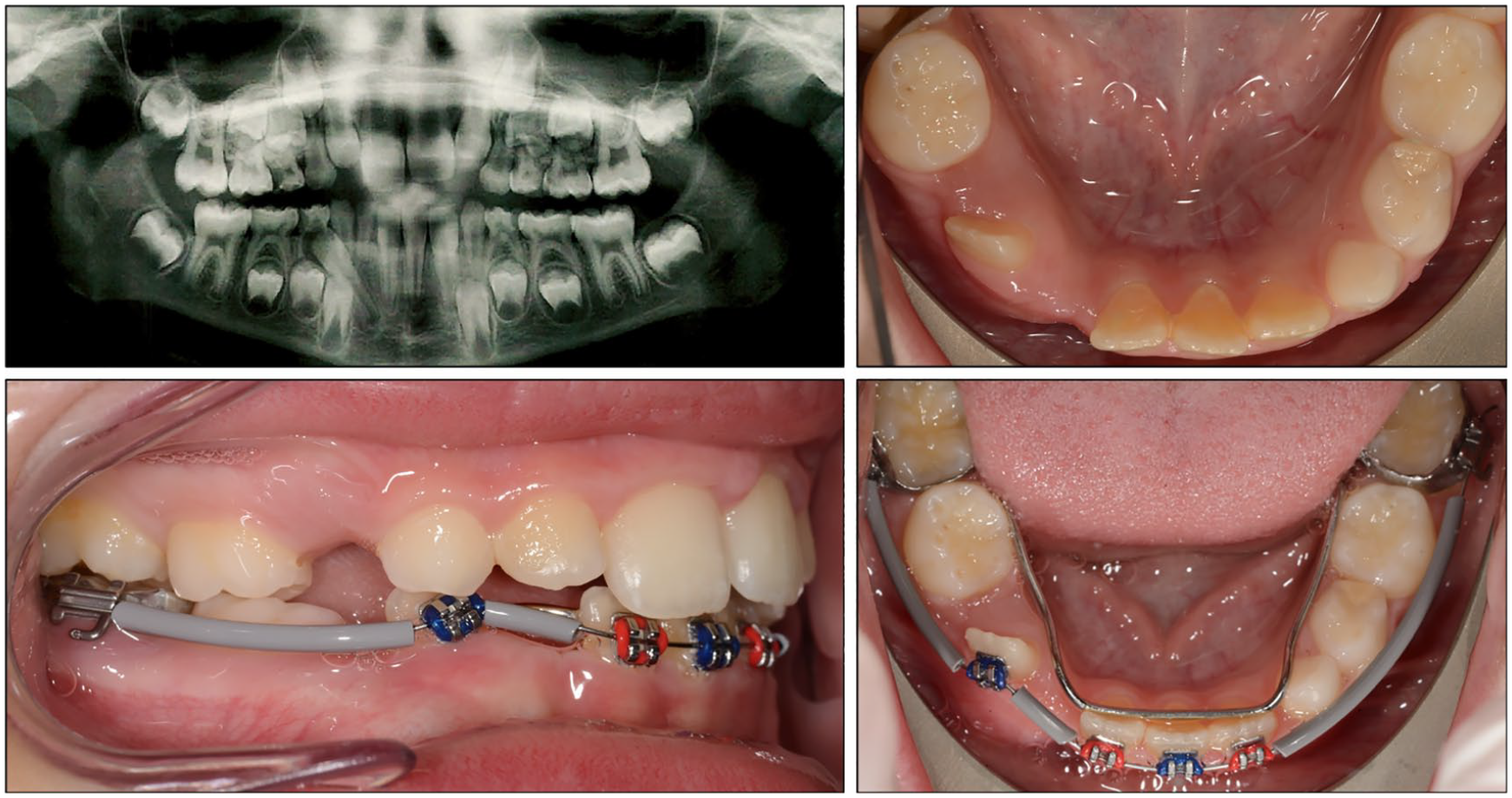
An 8-year-old male patient presented in the mixed dentition with a displaced LR2. Note how the LRB and LRC are still present on the pre-treatment OPG and the ectopic LR2 is causing root resorption to the LRD. Interceptive orthodontic treatment was undertaken with fixed appliances to align the LR2 after removal of the LRB, LRC and LRD. Anchorage was reinforced with a lingual arch and long spans of unsupported archwire protected with elastomeric bumper sleeve tubing.

A 9-year-old male patient presented in the mixed dentition with a displaced LR2 and a congenitally absent UL5. Following removal of the LRB and LRC interceptive orthodontic treatment was undertaken with fixed appliances to align the LR2. At a later stage, the LR3 became impacted, with this tooth being subsequently removed.
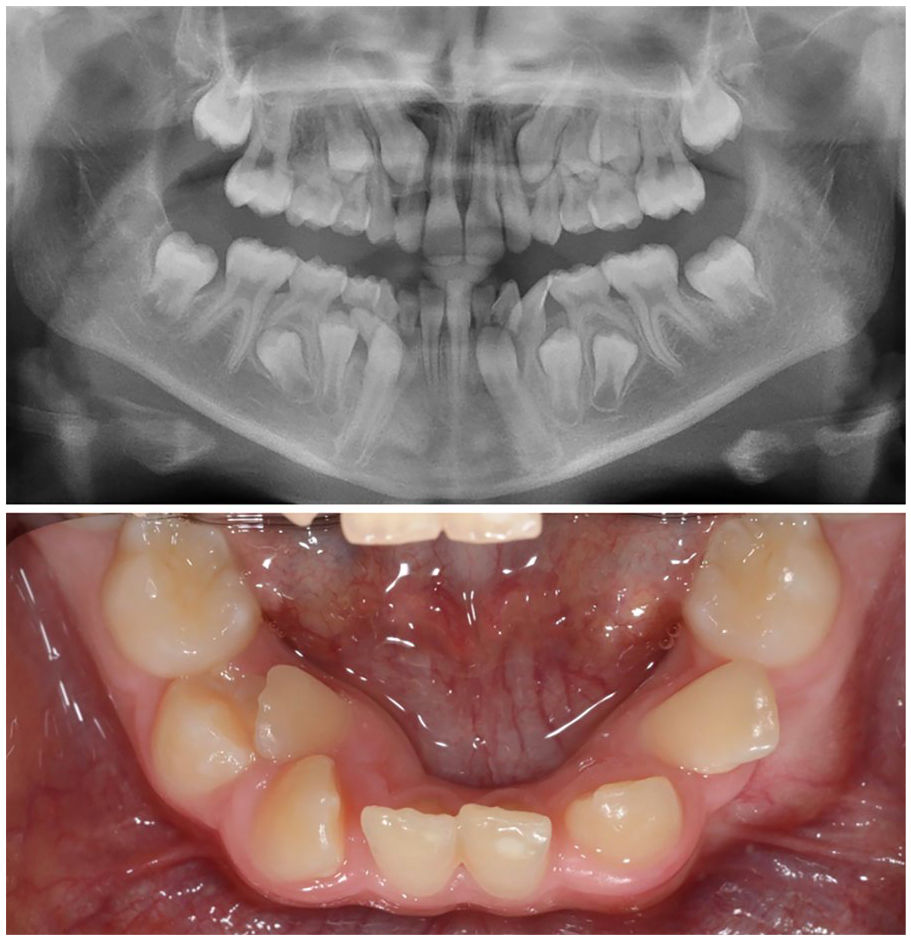
A 10-year-old female patient presented in the mixed dentition with mandibular crowding, ectopically erupted LR2 and LL2, ectopically displaced LR5 and LL5, impacted UR3 and developmental absence of UR5. Due to the degree of crowding within the mandibular arch and the extent of the displacement of the mandibular lateral incisors (complete transposition with the adjacent mandibular canines), the mandibular lateral incisors were planned for extraction.

A 10-year-old female patient presented in the mixed dentition with an ectopically erupted LR2, a developmentally absent LL2 and poor oral hygiene. The decision for extraction of the LR2 was undertaken as the level of oral hygiene was unsuitable for the fixed appliance therapy and to preserve symmetry in the mandibular arch.
However, when the recognition and management of a Mn.I2.C transposition is delayed, this can result in a complete transposition, with the roots of the lateral incisor and canine completely interchanged. At this stage, the only practical treatment options that remain are extraction of one of the involved teeth or acceptance of the complete transposition.
Report of cases
We present six cases with Mn.I2.C transposition. All six cases were assessed and treated at The Royal Surrey NHS Foundation Trust, UK. Three of the patients were female and three were male. Unilateral transposition was displayed by five of these cases, while one case presented with a bilateral transposition. Five of the six cases presented with a transposition affecting the right-hand side of the dentition. For all six cases, the displaced mandibular lateral incisors displayed both a distal inclination and element of rotation.
Discussion
Permanent mandibular incisors develop lingually to their corresponding primary teeth. This lingual eruption usually leads to non-exfoliation of the corresponding primary teeth. However, this is rarely problematic as anterior migration ensues owing to the action of the tongue musculature in concurrence with favourable growth and development. Unfortunately, this was not the pattern of eruption found in our paper, with the mandibular lateral incisors showing a distal direction of eruption relative to their corresponding primary teeth. This was the chief presenting complaint for all six cases, which is unsurprising when considering the importance of lateral incisors for aesthetic, social and functional purposes (Huber et al., 2008).
Although the precise aetiology of ectopic eruption is unknown, it is worth noting how three of the cases we present also suffer from hypodontia (Cases 4–6). Hypodontia is associated with a number of dental anomalies including ectopic eruption, maxillary canine impaction and transpositions, leading to the suggestion that genetics may act as an aetiological factor for Mn.I2.C transposition (Brook, 1984).
It is also interesting to note five of the six cases experienced Mn.I2.C transposition in the right-hand side of the dentition. However, at this moment in time, there appears to be little evidence in the literature regarding a predilection for Mn.I2.C transposition in the right-hand side of the dentition compared with the left-hand side of the dentition. Perhaps of greater significance is how all six cases had retention of the corresponding primary teeth when presenting to our department. It remains uncertain whether the transposition was due to prolonged retention of the corresponding primary teeth or if the prolonged retention of the corresponding primary teeth was due to the ectopic eruption of the corresponding permanent teeth. However, it seems reasonable to suggest that interceptive removal of the primary mandibular lateral incisor +/– canine may have led to less severe displacement of the corresponding permanent mandibular lateral incisor.
In order to preserve the integrity of the dental arch, many clinicians prefer orthodontic alignment of displaced mandibular lateral incisors. Anchorage demands are often high due to the severity with which the lateral incisors can be displaced and the resultant mandibular centre-line shift which needs correcting. The anchorage demands varied for each case, with Cases 3 and 4 requiring a lingual arch to reinforce anchorage, due to the lack of adult teeth available for bonding in the mixed dentition.
While applying orthodontic traction to displaced lateral incisors, care should be taken to avoid root interferences, which may lead to root resorption as well as damage to the supporting tissues. This is particularly difficult owing to the lack of buccal-lingual bone available to accommodate tooth movements in the anterior mandibular region. Adequate labial root torque is essential to reduce the propensity for relapse of the mandibular lateral incisor, however this can also prove challenging, as the relatively small interbracket span in the lower labial segment results in difficulties in producing third order bends in the finishing archwires. To account for this, a full thickness rectangular archwire can be placed to minimise slop and preadjusted edgewise fixed appliances with MBT bracket prescriptions are preferred, owing to the additional labial root torque (–6°) in the mandibular incisor brackets.
While the majority of the mandibular canines within our paper erupted in relatively normal positions, all the ectopic mandibular lateral incisors were severely displaced, exhibiting both a distal inclination and rotation. Although literature states that these findings are common among ectopic mandibular lateral incisors, the reasons for these features remain largely unknown (Taylor and Hamilton, 1971). Despite the uncertain aetiology, these findings remain clinically significant, especially the presence of marked pre-treatment rotations. Derotation of a lateral incisor will necessitate a space requirement within the arch. In addition, once the rotation is fully corrected, long-term retention, supplemented with a bonded retainer, may be required due to the strong relapse tendency (Littlewood et al., 2016).
This inherent relapse potential which can be associated with ectopic mandibular lateral incisors, in combination with the severity with which they are often displaced, may lead clinicians to prefer extraction of these teeth to orthodontic alignment, especially in the presence of crowding. The resulting extraction space can be prosthetically restored or orthodontically closed with the mandibular canine positioned next to the mandibular central incisor. Despite both the mandibular central and lateral incisors being of similar morphology, finishing with a canine–central incisor contact in the mandibular arch can be problematic (Table 1).
Limitations associated with extraction of a mandibular lateral incisor followed by orthodontic space closure.
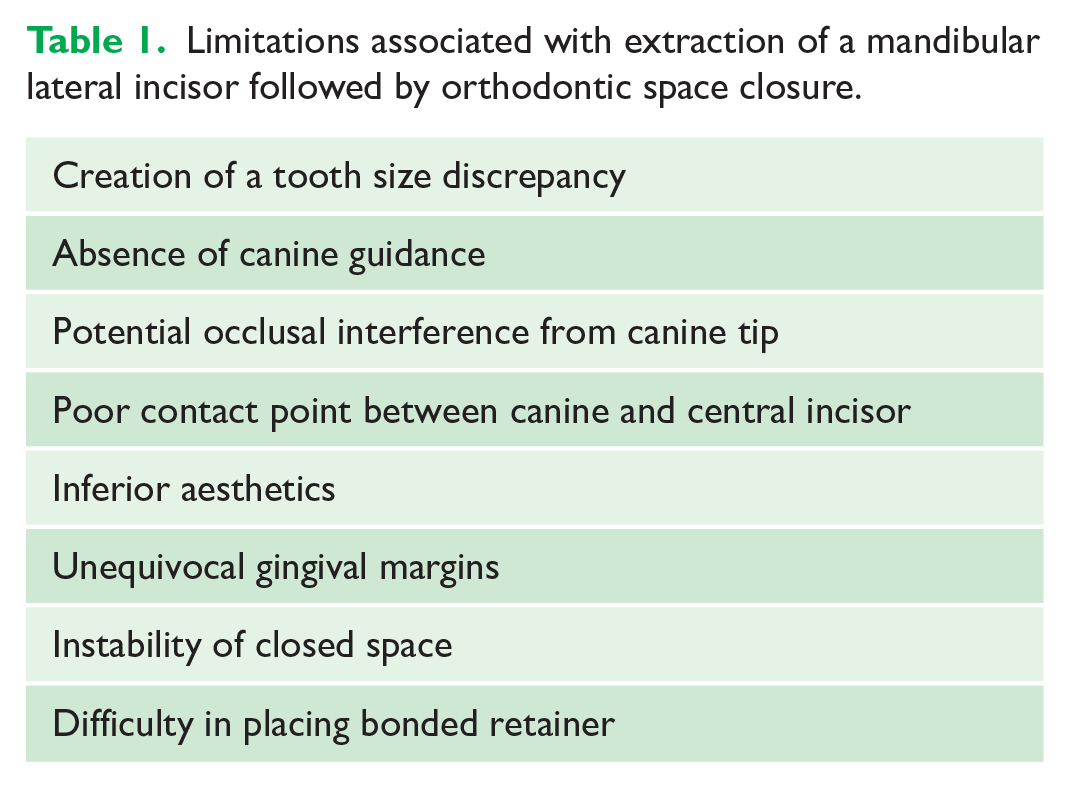
Mandibular lateral incisors tend to have a more fan-shaped appearance compared with mandibular central incisors; therefore, interproximal adjustment may be required to achieve the desired contact between a mandibular canine and central incisor. In addition, the mandibular canine tip can be reduced with occlusal grinding, especially if this tooth has the potential to cause a non-working side interference (Vilhjálmsson et al., 2019). However, owing to the inability to achieve canine guidance on lateral excursion and concern of a resultant tooth size discrepancy, this treatment option is normally reserved for crowded cases necessitating extractions or severe cases where there has been complete transposition of the mandibular lateral incisor with the adjacent canine. Another instance where this approach may be undertaken is for patients who present at an early age, who may not have the required maturity to undertake fixed appliance treatment due to poor compliance and suboptimal oral hygiene (Case 6).
Conclusion
Mn.I2.C transposition, from our case series, appears to have a predilection for the right-hand side of the dentition and show an association with other dental anomalies including hypodontia. Early recognition and intervention for this malocclusion can be beneficial, with interceptive extractions +/– orthodontic management reducing the complexity of any potential further treatment. Although, for a compliant patient, aligning an ectopic mandibular lateral incisor into its correct anatomical position is preferential to produce the best aesthetic and functional results, this approach is not always viable due to compliance, time and biological limitations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.