
Abstract
Aim:
This in vitro study investigates the limit of expansion forces and torque wrench forces developed by five skeletal bone expander designs (MICRO 2/4 expanders™) for clinical application.
Material and Methods:
A total of 30 skeletal expanders were placed in artificial bone blocks and mechanically tested, simulating maxillary expansion. Differences in jackscrew (Dentaurum™ [D], Superscrew™ [S] and Powerscrew™ [P]), number of orthodontic mini-implants (OMIs; two or four) and their placement inclinations (parallel 0° or 10° inclination) form five designs (D4/10°, S4/0°, S4/10°, P4/10° and P2/10°). Expansion forces and torque wrench values were registered, and radiographs were made initially and after 4 mm of expansion. Stress-strain curves were obtained after successive activations and the statistical analysis was performed as appropriate.
Results:
Plastic deformations in the OMIs and jackscrew occurred around the activation numbers 11–13, with torque wrench values in the range of 500–700 cN. The maximum expansion forces in expanders with four OMIs varied from 93.0 (D4/10°) to 166.6 N (P4/10°) whereas two OMI expanders (P2/10°) registered forces of 79.4 N. Radiographs revealed during loads bending forces (S4/00°, S4/10°) with jackscrew and OMIs deformation in a convex shape, and shear forces (P4/10°, P2/10°) demonstrated only OMIs deformation in a concave shape, providing 15% more expansive force. The jackscrew D4/10° did not have any deformation, but its wire key did not allow reliable activations from activation number 10 and compared to S4/10° and P4/10°, these expanders provided greater expansion forces (P = 0.000 and P = 0.032, respectively).
Conclusion:
The different results obtained in stability and expansion forces indicate that if the activations are carried out under extreme conditions, they may have clinical importance with deformations and non-working expansion mechanics. Jackscrew designs play an important role in expansive forces and expander stability. Torque wrench values can be used clinically as a tool to asses the expansion forces and to avoid deformations.
Keywords
Introduction
Transverse maxillary deficiencies are common orthodontic issues observed by professionals. It is estimated that 9.4% of adult orthodontic patients have a transverse maxillary deficiency in combination with a posterior crossbite (Betts et al., 1995; Timms, 1999).
A normal transverse skeletal relationship between basal bones is fundamental to achieving a satisfactory and stable occlusion. Therefore, to correct a maxillary transverse deficiency, palatal expanders are needed (Andrucioli and Matsumoto, 2020).
Since Haas popularised this technique in the early 1960s, rapid palatal expanders are the most popular devices of choice, characterised by safety, predictability and efficiency (Bishara et al., 1987; Haas, 1965). The rapid process of activation reduces dental movements (side effects) thus enabling skeletal expansion (Haas, 1970). Surprisingly, only 30% of the expander opening seems to result in suture opening, whereas one-third reflects alveolar bending and another 30% dental movement (Baratieri et al., 2014; Gamba et al., 2008).
During activations of traditional tooth-borne rapid palatal expansion devices (with or without acrylic plates), heavy transverse forces are generated in a short period of time, causing disruption of the intersutural tissue thus producing midpalatal suture opening (Haas, 1970; Lione et al., 2008; Wertz, 1970). On many occasions, these expansion forces in-vivo are in the range of 75–120 N (Isaacson and Ingram, 1964; Sander et al., 2006; Zimring and Isaacson, 1965), measured at the level of the hyrax screw of the connecting stainless-steel wire arms at the buccal crowns. In vitro skeletal hybrid expanders, before plastic deformation, demonstrated expansion force values from 67 ± 13 N to 183 ± 48 N when tested on the mini-implant’s reinforced bone-anchored wire arms (de la Iglesia et al., 2018). With these forces, the opening of the palatal suture in adolescents or young adults can be frequently unsuccessful (Isaacson and Ingram, 1964; Sander et al., 2006; Zimring and Isaacson, 1965). Therefore, conventional expanders, under high loads, deform prematurely or create excessive molar tipping or mucosa soreness before reaching midpalatal suture opening (Carlson et al., 2016; Lin et al., 2015; Winsauer et al., 2017). If these expansion forces are not able to open the suture, surgically assisted rapid palatal expansion (SARPE) is suggested. In addition, scientific papers do not provide information of the amount of force at the level of the midpalatal suture and the limit of plastic deformation.
Pure bone-borne maxillary expanders (MICRO4 expander™, Dresden expander™ and BAME expander™) (Hartono et al., 2018; Lagravère et al., 2013, 2020) are solely anchored on orthodontic mini-implants (OMIs) and placed in the anterior-middle palate. These bone anchored expanders seem to improve the aforementioned drawbacks and provide greater expansion forces to facilitate midpalatal suture opening even in adult patients so as to avoid SARPE; however, studies are lacking to demonstrate this, which is what this study aims to look at. Nonetheless, it has been observed that skeletal expanders also suffer deformation during surgery, especially at the level of the expansion screw (jackscrew) and at the level of the OMIs (Brunetto et al., 2017; Winsauer et al., 2021).
The solid construction and design of the skeletal expanders, by increasing the diameters of the OMIs, jackscrew and wire arms to counteract forces and moments, provide greater stability and expansion forces (Walter et al., 2017). Therefore, this study aims to investigate Micro4 expanders, to gain a better understanding of their structural stability and activation before reaching deformation and breakage. This is supported by several reports (de la Iglesia et al., 2018; Walter et al., 2017) but has not yet been methodically investigated.
There are also questions related to the magnitude of force required for suture opening when applied to the clinical settings.
The aims of this in vitro study were (1) to quantify the proportional relation between the activation force and the resulting expansive force of five pure bone-borne maxillary expanders placed in two artificial bone blocks simulating the palatal position; and (2) to determine the rigidity before reaching plastic deformation.
Materials and methods
All tested pure bone-borne maxillary expanders (MICRO expanders™, Mini-Implant Collar Retained Orthodontic expanders) are currently in daily clinical use (Winsauer et al., 2013). The present study aimed to understand their characteristics and mechanical properties better (Figure 1a). The MICRO4 expander™ placed the OMIs in the palate positions M4 (anterior palate half-way between the midpatalal suture and palatal cusp of the first premolar) and M5 (middle-posterior palate half-way between the midpalatal suture and palatal cusp of the second premolar) since this position seems to provide adequate bone height (Winsauer et al., 2014).
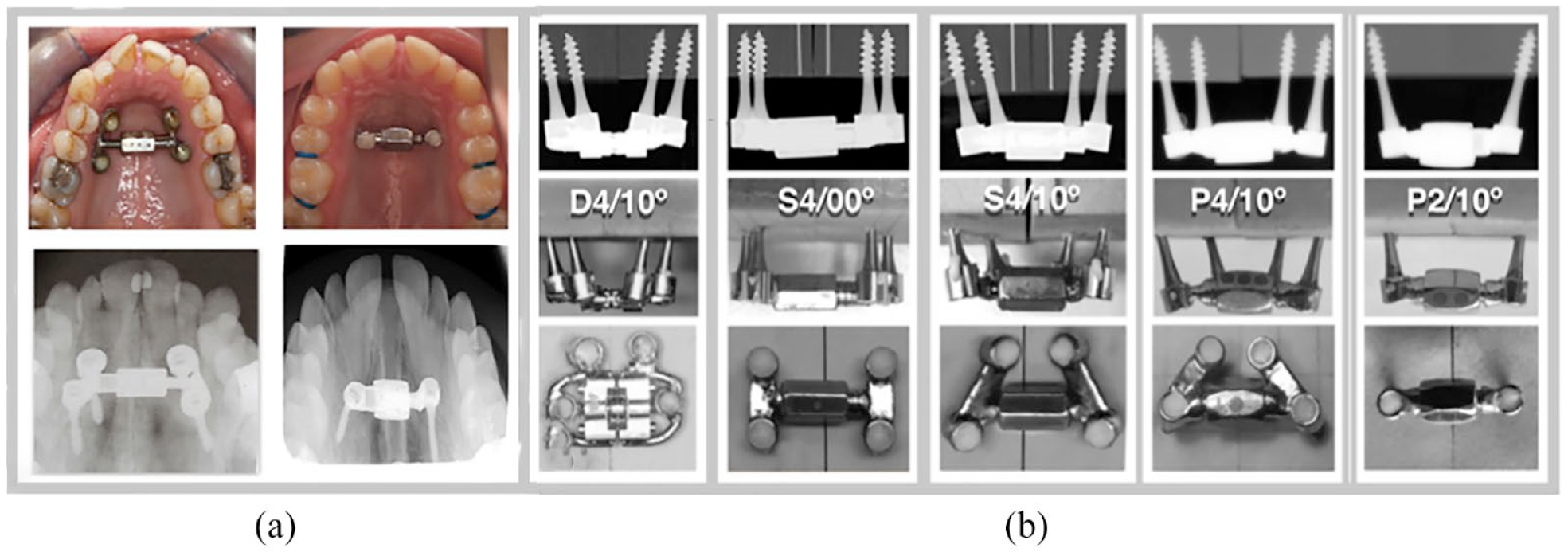
(a) Micro4/2 expander in clinical use and (b) in vitro investigation of skeletal expanders distributed in five groups according to jackscrew trademark, number of orthodontic mini-implants and their inclination with their radiographs before loading.
Five differently designed pure bone-borne MICRO-expanders™ were tested in vitro in terms of stability and magnitude of expansion force with regard to the numbers of OMIs, their insertion inclination and types of jackscrews used. All OMIs (Jeil Medical™ Company, Seoul, Republic of Korea) were 2.5 mm in diameter and 14 mm in length (Figure 1b). The placement of the OMIs in artificial bone blocks was similar to that on the palate, in the clinical position M4-M5. For each tested sample, the name was chosen according to the type of jackscrew (S = Superscrew, P = Powerscrew, D = Dentaurum), the number of supporting OMIs and their inclination (e.g. P4/10°). The study tested four expanders each anchored on four OMIs (MICRO4 expander, D4/10°, S4/00°, S4/10° and P4/10°) and one expander anchored on two OMIs (MICRO2 expander, P2/10°) (Figure 1b). In this in vitro test, the OMIs were placed in double blocks made of artificial bone (Sawbones™ 35 pcf, EEUU) at a depth of 8 mm simulating the average bone depth and density in the anterior palate of adult patients (Devlin et al., 1998). For each design, six tests were made and studied mechanically (30 samples in total).
In four expanders, the OMIs were placed at inclinations of 10° outward from the vertical whereas in the S4/00° expander the OMIs were placed strictly parallel at 0° (Figure 1b). Three different jackscrews were used: the cylindrical double action telescopic SuperScrew (IL, USA) with a 2.5-mm diameter threaded rod for S4/00° and S4/10°. The cylindrical double action telescopic PowerScrew (Tiger Dental, Bregenz, Austria) with a hardened threaded rod of 3.0 mm diameter for P4/10° and P2/10°, and a flat double action spindle screw (Dentaurum, Ispringen, Germany; ref: 602-808-10) for D4/10° (Figure 1b).
For each expander design, five tests (30 tests in total) were carried out in the Galdabini Universal testing machine™ (Quasar 50 kNl Cardano al Campo, Italy). During each activation, the resulting expansion force of the hyrax was measured in a static position until plastic deformation was reached. Occlusal radiographs were taken initially and after 4 mm of the activation to analyse the mechanical properties with regard to deformation behavior.
Jackscrew activation
To turn the hexnut for opening the Superscrew™ and Powerscrew™, the manufacturers provide an 8-cm-long wrench (Figure 2a and b). One activation (=30°) turns the hexnut from one side to the next, thus opening the jackscrew 0.18 mm per activation (6 turns = 1 mm, respectively). The Dentaurum jackscrew™ (hyrax medium 10) with a leadscrew parallel with two guiding pins, is activated by turning the perforated cylinder seated in the centre of the leadscrew from one hole to the next (=90°), corresponding to 0.20 mm of expansion (5 turns = 1 mm). The activation was done with a 4-cm-long 0.036-inch stainless-steel wire key provided by the manufacturer. A stainless-steel tube was used to enlarge this wire key to a total length of 8 cm in order to obtain an identical comparison setup.
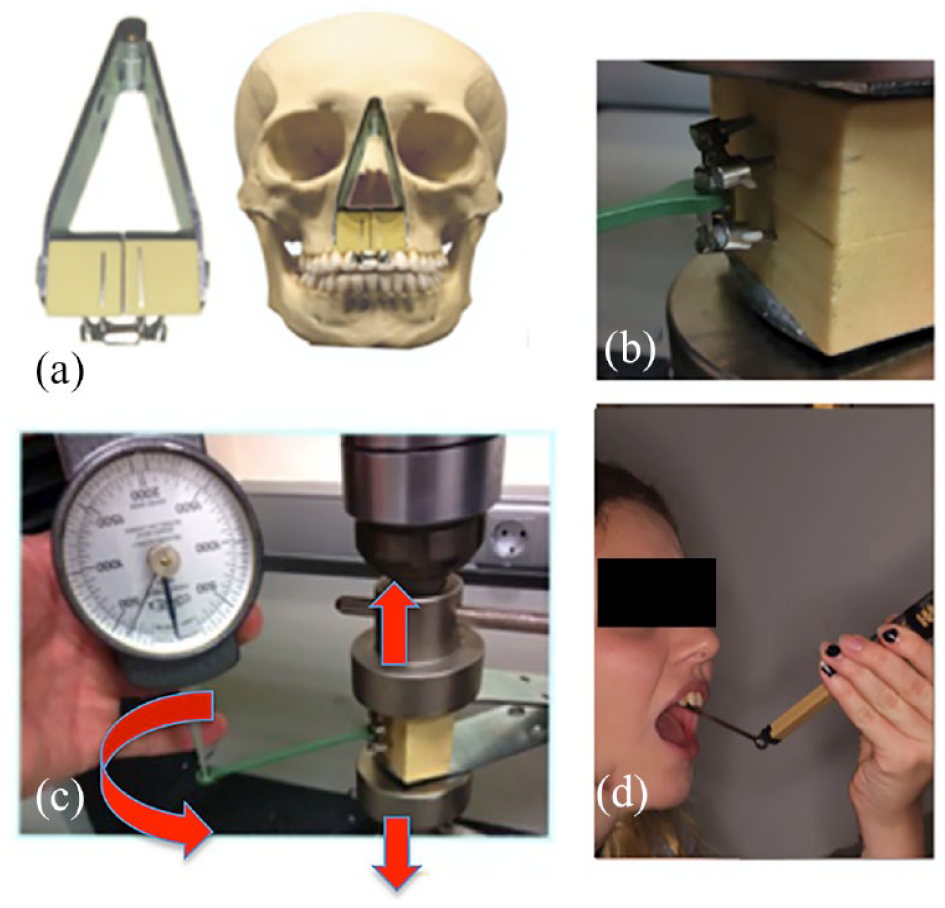
Settings of the expanders in the testing machine: (a) expander fixed at the end of a 9-cm hinge joint simulating the opening of the maxillary complex in the skull; (b) activation of the expander placed in artificial bone blocks with a wrench placed in the hexnut of the jackscrew; (c) Correx scale placed on the activation wrench for force measurement; and (d) in-vivo activation of the expander done by a patient with spring scale. This allowed reading the force magnitude during each activation (force controled activations).
The expanders were placed in double blocks of artificial bone with a density similar to the maxilla bone of an adult patient (de la Iglesia et al., 2018; Walter et al., 2017), and then fixed at the end of the leaves of a metal hinge joint construction, simulating the maxilla complex during midpalatal suture opening (MacGinnis et al., 2014) (Figure 2a). These fixed expanders assured standardised openings and unwanted rotations of the bone blocks. The distance of 9 cm—arbitrary according to the standard adult anatomy skull model (3B Scientfic, Anatomy Stuff Company, UK)—between the axle of the hinge and the expander mimiced the anatomical skull situation of the palate in relation to the frontonasal suture. During the opening of the palatal suture, the maxilla was separated in a certain inclination, in what is called an inverted V-shape opening, in a similar way to a hinge with the axis located in the nasal bones (Serpe et al., 2014; Yoon et al., 2019). The chosen distance between the nasal bones and the expander located in the maxilla was obtained from an adult skull model and it has also been used in computed tomography scans of dried adult skulls in finite element studies (Cantarella et al., 2017; Holberg and Rudzki-Janson, 2006). Therefore, the setting mimiced the mechanical behavior of expanders during the opening procedure (Serpe et al., 2014).
The double blocks were fixed in the testing machine to allow static lateral displacement during manual activations (Byloff and Mossaz, 2004) (Figure 2b). In this testing machine the expansion force was measured while simultaneously registering the force at the end of the wrench with a Correx scale (Correx Waage, Dentaurum, Ispringen, Germany), activating it every 25–30 s (Figure 2c). This in vitro procedure, with a calibrated torque wrench, mimiced the procedure of the patient (in vivo) performing activations in the mouth (Figure 2d).
Statistical analysis
Scatter plots showing the relationship between torque wrench force (cN) and expansion force (N) were constructed for every type of expander, establishing a linearity range (elastic limit) of this relationship according to investigator experience and visual results of the plots in the stress-strain curves.
To assess the relationship between these two variables (torque wrench force and expansion force), a linear mixed model was used, with expansion force as a dependent variable, torque wrench force as an independent variable and the experimental measures repeated as random factors. The slope and its 95% confidence intervals, were shown for each type of expander, as well the expansion force for every 100-cN force increase of torque wrench.
The relationship between the expansion force and the number of activations was also shown with scatter plots. The comparisons of expansion force with the activation force between the different expanders, were undertaken with a non-parametric Mann–Whitney U test.
All the measurements were processed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). P values <0.05 were considered statistically significant.
Results
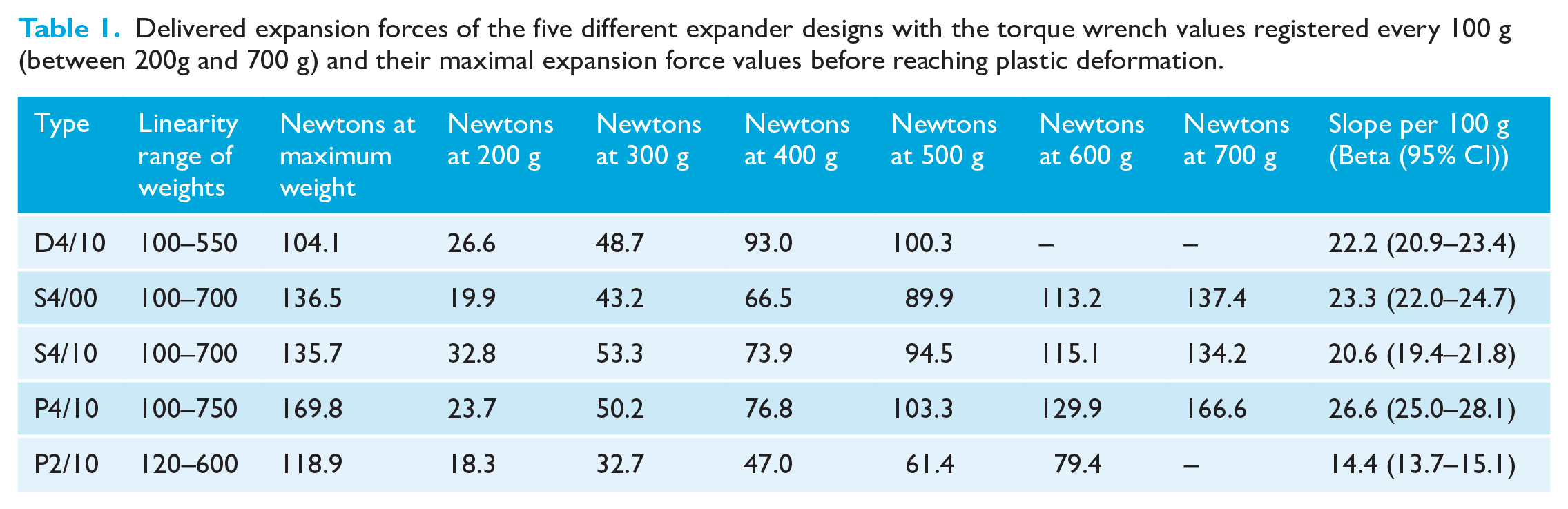
The expansion forces measured in the five expander designs are shown in Table 1 and Figure 3. The pure bone-borne expander types S4/00°, S4/10° and P4/10° showed maximum expansion forces above 130 N. Maximum expansion forces of approximately 166 N were observed in the P4/10° expander design, while the lowest value of 79.4 N was observed in the P2/10° expander design. All these values were within the limit of the elastic deformation just before reaching the plastic deformation, which is shown in the highest part of the linearity range (Figure 3).
Delivered expansion forces of the five different expander designs with the torque wrench values registered every 100 g (between 200g and 700 g) and their maximal expansion force values before reaching plastic deformation.
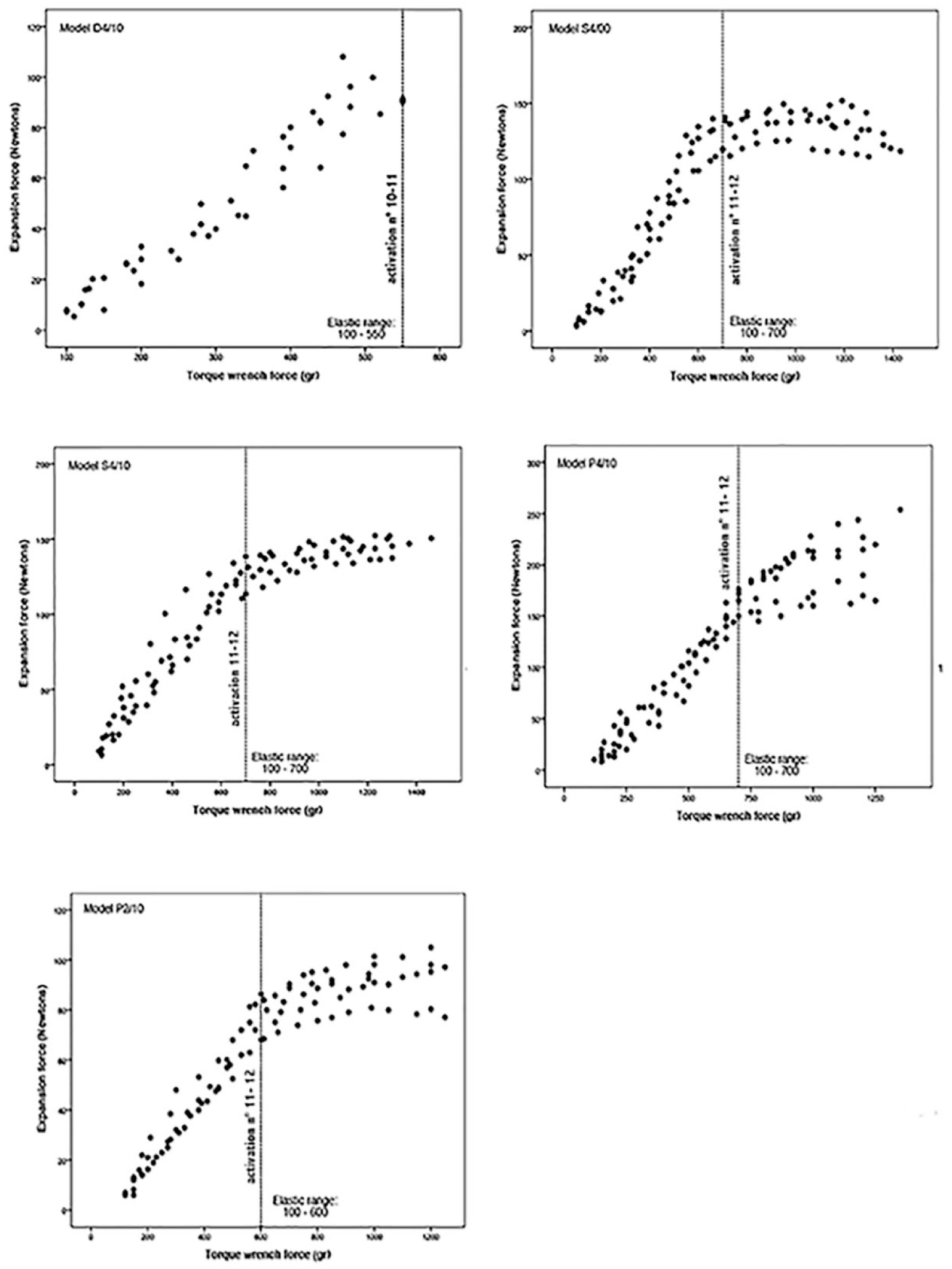
Stress-strain curves and results of the maximum delivered expansion forces in relation to the limit of the elastic deformation, which is shown at the highest part of the linearity, range for each expander types (between the activation numbers 11 and 12).
The maximum torque wrench values were measured within the elastic deformation range of 500–700 cN. Slopes between the expansion force and torque wrench were in the range of 14.4–26.6 cN.
In relation to the successive activations of the expanders (every 25–30 s), the x-radiographs revealed deformations in different parts of the expander designs (Figure 4). The S4/00° and S4/10° expanders started to deform between activation 12 and 13 (activation 12 = 2 mm of expansion) (Figure 3). The deformations after 4 mm of expansion are located mainly in the OMI shaft and the threaded rod of the jackscrew expander in a convex shape. The linear range value before plastic deformation of these two types of expander corresponds to a torque wrench of around 700 cN (Figure 3). Both show similar mechanical behavior initially; however, after activation 11, statistically significant differences were seen with more jackscrew deformation in the S4/00° design (Table 2).
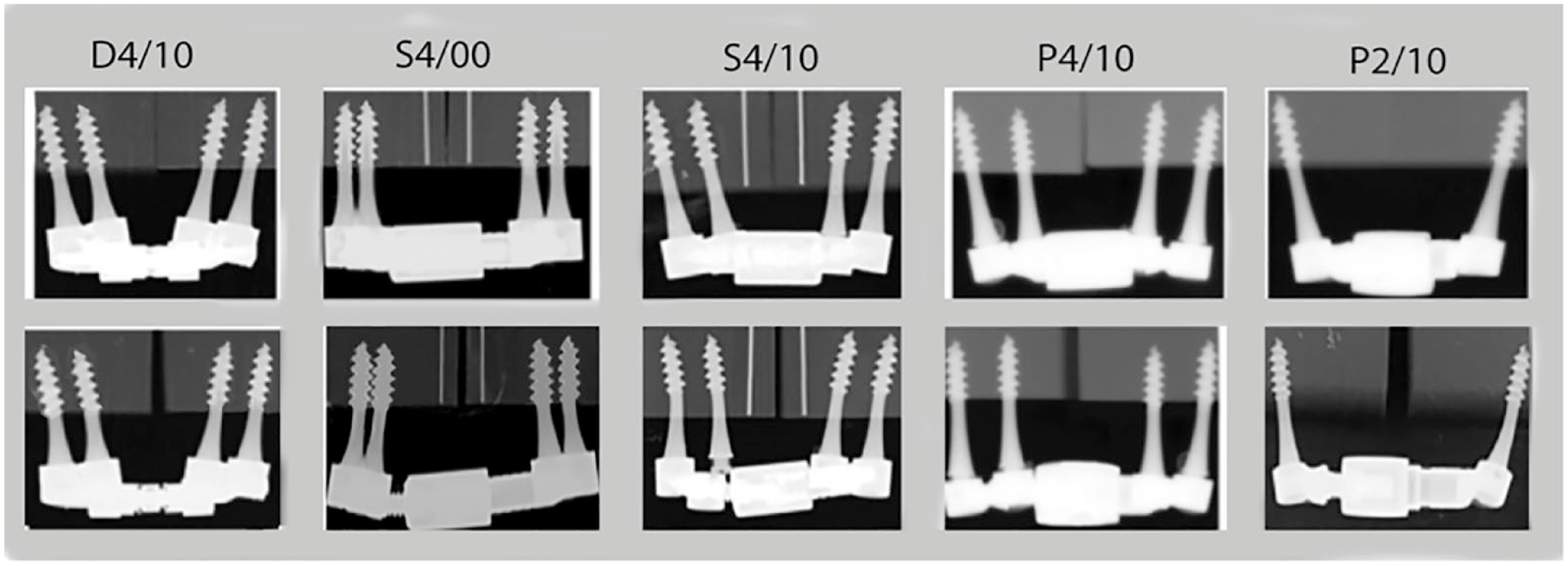
Radiographs of the skeletal expander after 4 mm of expansion with deformation located in the orthodontic mini-implants and jackscrew.
Statistical analysis, between activations 9 and 13, of the five types of expander designs in relation to their mechanical expansion forces behavior.
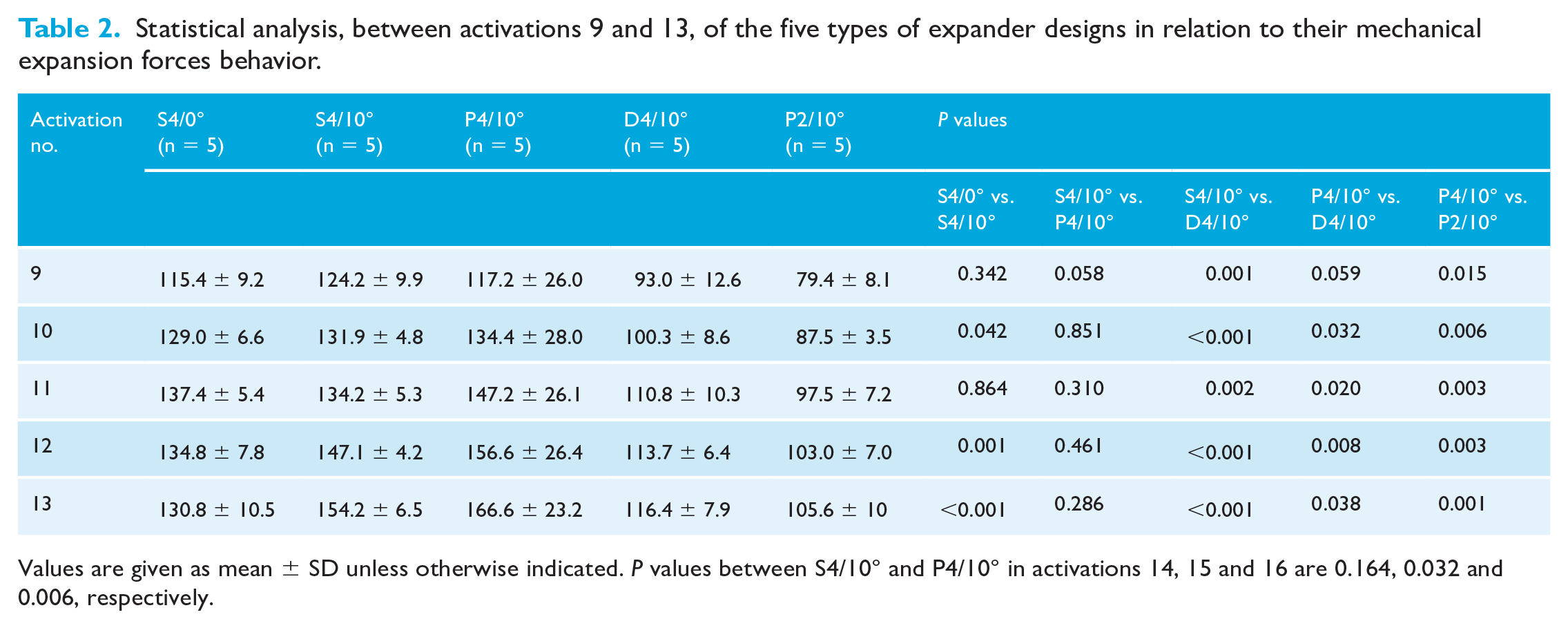
Values are given as mean ± SD unless otherwise indicated. P values between S4/10° and P4/10° in activations 14, 15 and 16 are 0.164, 0.032 and 0.006, respectively.
Expanders D4/10° and P2/10° start to deform with a torque wrench value of approximately 600 cN, corresponding to the activations between 10 and 12 (close to 2 mm of expansion) and with expansion forces of approximately100 N and 79 N, respectively (Figure 3). Radiographs showed, in the P4/10° and P2/10° designs, concave deformations only in the OMI shaft but not in the jackscrew.
Between the expander designs S4/10° and P4/10°, the expansion forces demonstrated similar results, but changed dramatically after activations 13 with highly statistically significant differences (P = 0.033, activation 13; P = 0.026, activation 14; and P = 0.025, activation 15) (Table 2 and Figure 3).
The jackscrew of the D4/10° expander design showed great stability during the activation process compared to the S4/00° and S4/10° designs, without deformation in the radiographs that were also not observed in the 2.5-mm diameter of the OMIs (Figure 4). It only allows around 10–11 activations because of the early deformation of the 1.5-mm-diameter stainless-steel key. Expander designs P4/10 and S4/10° had differences in mechanical behavior in comparison with the D4/10° design, with statistical differences after activation 9 (Table 2).
Discussion
About the study
The literature about investigations concerning the expansion forces of pure bone-borne expanders during activation phases and its limits related to plastic deformations is scarce (Camporesi et al., 2013; Muchitsch et al., 2011). Therefore, this in vitro study analysed the expansion force capability and plastic deformations of the pure bone-borne maxillary MICRO expanders™ utilising two or four OMIs at an insertion depth of 8 mm (Winsauer et al., 2013). It simulated the placement of these expanders in the anterior palate with the OMIs in the M4 and M5 positions (Winsauer et al., 2013), since it is a described position to perform midpalatal suture opening of the maxillary bone.
Because the rigidity of hyrax wire arms is associated with weaker expander constructions they are also subject to early plastic deformations that occur during their activations (Muchitsch et al., 2011). The expanders analysed in this study (without wire arms) provided greater stability and therefore a greater ability to produce expansion forces. However, in this study, plastic deformation was also observed in the mini-implants and jackscrews and therefore limited their expansion force.
The in vitro expansion force values, registered in the five analysed expander designs, were in the range of 79.4–166.6 N before reaching plastic deformation. For better mechanical understanding and clinical usefulness (Isaacson and Ingram, 1964), the stress-strain curves recorded during expansion forces, torque spanner values obtained and radiographs made in this study were carried out in a similar way to other in vitro and in vivo expander studies (de la Iglesia et al., 2018; Walter et al., 2017; Winsauer et al., 2021). Since OMIs and jackscrew deformations have also been clinically observed (Brunetto et al., 2017; Winsauer et al., 2021), a better understanding of how they occur justified this study.
Force delivered values
The study provides an activation force/delivered expansion force curve. It showed that the greater the stiffness of the expander (S4/10° vs. P4/10°, see the activation screw/force curve) (Table 2, Figure 4), the greater the developed expansion force. Activations 12 and 13, in particular, corresponded to a jackscrew opening of approximately 2 mm, but mechanical diferences were seen when further activations were applied (p = .164, p = .0032, p = .0006) (Table 2). This is explained due to the early jackscrew plastic deformation with a smaller treaded rod diameter (S4/10°), which was not capable of counteracting forces and moments. Consequently, a convex plastic deformation in the jackscrew and in the OMIs (S4/00° and S4/10°) seen in the radiographs are in concordance with other studies (de la Iglesia et al., 2018; Walter et al., 2017) and were not capable of exceeding expansion forces of 135 N (Table 2, Figure 4). With similar results, in a tooth expanders investigation, by changing the height of the jackscrew on the palate, the expansion forces were in the range of 80–160 N (Camporesi et al., 2013), demonstrating the importance of the generated moments during the expansion forces. In the present study, the moments generated by the 9-mm distance cantilever arm of the jackscrew to the artificial bone surface (7 mm transgingivally of the smooth extraosseous OMI part + 2 mm of abutment height of the cantilever arm) was in accordance to the clinical expander placement in regular use (Winsauer et al., 2013).
The computing finite element analysis can also measure the expansion forces, highlighting the importance of design and rigidity of all components (jackscrew, wires, abutments and OMIs) (Lin et al., 2015; Muchitsch et al., 2011). It is reported that the skeletal C-expander (acrylic mucosa-borne expander embedded with four OMIs) clinically opens the midpalatal suture in adolescents and young adults successfully. Its jackscrew lies close to the palate, which, in principle, is mechanically more favorable to counteract forces and moments, with registered expansion forces of approximately 80 N (Lin et al., 2015). The smaller implant size of the C-expander (1.8 × 8.5 mm length), in contrast to the Micro4 expander design (2.5 × 14–16 mm length), provided lower expansion forces and can be seen in the study by Boryor et al. (2013), where a smaller implant size can counteract the generated moments less, with similar results of 86 N. These authors observed, in a dried human skull utilising a pure bone-borne expander with four OMIs (1.7 × 8 mm length), that during the activations palatal screw displacements occur (Boryor et al., 2013). Therefore, increasing the diameter of the OMIs and rigidity of all components of the expander design is recommended (Walter et al., 2017). This weakness in mechanical behavior is also confirmed in hybrid expander in vitro studies (de la Iglesia et al., 2018; Walter et al., 2017). By placing two wire arms side by side, the expansion forces vary from 62 to 72 N up to 140 N, changing during load convex OMI deformations produced by bending forces to concave deformations produced by shearing forces. In the present study, radiographs reveal shear forces on OMIs without jackscrew bending after activations 12 and 13 in the expander design P4/10° which was statistically different in comparison to S4/10° (Table 2, >13 activations (*), Figure 3). Shear forces provide approximately 10%–15% more mechanical strength than the bending forces (Walter et al., 2017).
The pure bone-borne expander design with two OMIs (P2/10°) can be used successfully in children for midpalatal suture opening (Hansen et al., 2007). The registered 79 N in the study confirmed that these values are well below those needed for success in young adolescents (Isaacson and Ingram, 1964). In a 13.4-year-old female patient, Isaacson and Ingram (1964) reported in vivo expansion forces up to 100 N, and other studies reported forces in adolescents up to 120–154.7 N (Sander et al., 2006; Zimring and Isaacson 1965). Seeing this result, the relevance of the skeletal expander stability lies in the clinical demand, where adult patients showed greater resistance to expansion (Cantarella et al., 2017; Holberg et al., 2007).
In the present study, all the samples in the radiographs showed jackscrew or mini-implant deformation with the exception of D4/10° due to the fact that the stainless-steel spanner was not capable of providing more activations. Nonetheless, a similar jackscrew design in the Moon expander design (miniscrew-assisted rapid palatal expander) with four palatal OMIs is capable of clinically separating the midpalatal suture in young adults ( Carlson et al., 2016; Winsauer et al., 2013) due to a more rigid wrench during its activations.
Torque wrench values
In orthodontics, the use of torque wrench is limited to mini-implant placement (Motoyoshi et al., 2010). Palatal expanders used in most cases have a short stainless-steel wire (0.036-inch) activation key of 4 cm that bends easily during activations under high expansion resistance. A rigid stainless-steel 8-cm-long torque wrench key has been used routinely in some palatal expanders (Winsauer et al., 2013), thus providing a spring scale in adult patients to allow a simple visual reading of the activation force applied to the spanner key (Winsauer et al., 2021) (Figure 2d). This allows the patient to know, during the activation process, the force that is being applied in the hexnut of the jackscrew as an indirect measurement of mechanical strength (Winsauer et al., 2021), with values in the in vitro study in the range of 500–700 g (Figure 4, Table 2) before reaching plastic deformation observed in the stress-strain curve. Therefore, in clinical practice it is recommended to use a limited torque wrench force of 500 cN with a protocol (Force Control Poly Cyclic [FCPC] protocol) (Winsauer et al., 2021) to avoid possible deformation of the expander. The information and instructions, together with written consent and explanation, can be provided to patients during activation. The assessment of the linearity range (elastic limit) and the yield point were estimated values carried out in other hybrid expander studies (Walter et al., 2017). It was conducted by two observers twice and, in case of any doubt, a third observer also assessed. In concordance with other in vitro studies (de la Iglesia et al., 2018; Walter et al., 2017), the plastic deformation started after 2 mm of static load, which corresponds in the present study to around activations 12 and 13. These are approximate values, and in clinical situations they can vary considerably, taking into account that they were tested under ideal conditions. Parameters such as inclined mini-implants (Cho et al., 2013), different implant diameters (Walter et al., 2013), different insertion depths (Marcé-Nogué et al., 2013), lower bone density (Samrit et al., 2012) or expanders placed at different distances from the palate (Lin et al., 2015) can significantly vary the stress-strain curves and their elastic limits in lower values.
Inclination of insertion and clinical implications
Different inclinations of insertion can affect the stability of OMIs (Cho et al., 2013) with very oblique insertion angles (>30°) resulting in reduced stability in a lateral loading (Wilmes et al., 2008). When the loading direction changes from 90° to 45°, the reduction of the OMI stability decreases by approximately 40% (Petrey et al., 2010). The influence of a difference in OMI inclination of 10°, between S4/00° and S4/10°, shows highly statistically significnat differences in the mechanical behavior after activations 12 and 13, respectively (P = 0.001, P = 0.000) (Table 2). This was observed in the radiographs, suggesting OMI shaft and jackscrew deformation. According to other studies, a change in inclination of <10° in the angle had negligible effects in their stability, and is in concordance with our study before reaching 2 mm of expansion (Wilmes et al., 2008). Nonetheless, a very narrow palatal vault requires a greater inclination of OMI placement, which could compromise their stability when a lateral load is applied.
Limitations of the study
The present in vivo study was tested under ideal conditions, both with the insertion depth of the OMIs and with high-density artificial bone blocks (30 pcf), which are different from the maxillary bone in vivo. The inclinations, the insertion depths of OMIs, bone density, bi-cortical anchorage and stability may therefore, differ considerably clinically (Winsauer et al., 2013) and the expansion force values and deformation obtained may be lower in clinical situations. The activation speed and rate every 25–30 s was done manually, and makes the slope of the loading curves somewhat different; therefore, the results must be considered to be a simulation and evaluated with caution. Differences in the slope of the strain-stress curves of the five tested expanders were <10% and the results must be considered as guide values. Instead, the results obtained from the limits of the plastic deformation were not dependent on the speed and manner of applying the activation rates, and therefore may be considered more reliable. Since the values recorded by the dynamometer were obtained under ideal test conditions, clinically these measurements may be much more difficult for the patient to obtain due to the uncomfortable visual measurement on the dynamometer during the process of torque spanner activations (Winsauer et al., 2021). Therefore, it is recommended that a calibrated torque spanner sensor, provided by the manufacturers, with a torque limitation is used to prevent the expander deformation observed clinically (Brunetto et al., 2017; Winsauer et al., 2021).
The linearity range, proposed by the authors, has been made with an observational criterion of the obtained graphics and these values may vary considerably especially in the P2/10° where the limit of plastic deformation was very difficult to see. In addition, OMI displacement during orthopedic loads are observed clinically, but were not seen in this study, with expansion forces that can vary considerably in clinical situations.
Conclusion
Pure bone-borne expanders, without dental anchorage analysed in this study, were able to develop forces up to 150 N in ideal conditions. These values were higher than those reported in traditional tooth-borne expanders. This requires greater rigidity in the expander design. The activation spanner key and rigidity of the jackscrew, play an important role to exert greater expansion forces. This in vitro study does not support the claim that the registered expansion forces from these expanders are capable of opening the midpalatal suture without dental tipping, in clinical situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.