
Abstract
Introduction:
Soft tissue injuries are known complications of orthodontic treatment. Most of the injuries are mild, but severe complications can arise from deeper penetration or dislodgement of brackets and other foreign bodies into the surrounding tissues of the oropharynx and infratemporal fossa.
Patient concerns:
The patient, accompanied by his parents, presented to the Children’s Emergency Department with the concern of gradual limitation of mouth opening and eventual trismus, which occurred over a span of 2 weeks.
Clinical findings:
The patient presented with trismus and slight discomfort at the left cheek region. He reported a history of gradual limitation to his mouth opening 2 weeks prior. He was wearing upper and lower fixed orthodontic appliances and the left distal end of the maxillary archwire was found to have migrated into the left infratemporal fossa.
Primary diagnoses:
Left medial pterygoid muscle inflammation, or bleeding and haematoma formation, or infection within the infratemporal region.
Interventions:
The maxillary archwire was removed in the Children’s Emergency Department and a computed tomography (CT) scan performed subsequently confirmed the diagnosis of left medial pterygoid muscle inflammation. The patient was started on an intravenous (IV) antibiotic and a 2-day course of IV dexamethasone to reduce the muscle inflammation.
Outcome:
By the second day, the patient was able to achieve a mouth opening of 6 mm, and by the second week, the mouth opening had returned to normal.
Conclusion:
The potential risk of soft tissue injury and complications from orthodontic treatment is generally mild and limited. Soft tissue injuries can be avoided with careful management by the operator with the proper precautions taken. Clinicians should be familiar with the surrounding soft tissue anatomy and be aware of the potential for more severe complications and provide management or referral to the appropriate specialty accordingly.
Introduction
Soft tissue trauma is a known complication that can occur during fixed orthodontic treatment. Laceration and/or penetration of the gingivae and mucosa, causing ulceration or tissue hyperplasia, can occur during treatment and between appointments. This can be caused by the exposed distal ends of archwires, long unsupported stretches of the archwire in direct contact with the buccal mucosa, exposed brackets and hooks (Abdulrazzaq et al., 2018; Travess et al., 2004). Migration of the orthodontic archwire resulting in soft tissue penetration injury is also one of the possible complications of orthodontic treatment. Here, we present a case report of a patient who experienced gradual limitation of mouth opening and eventual trismus due to the penetration of the orthodontic archwire into the infratemporal fossa and the resultant impingement and inflammation of the medial pterygoid muscle.
Case report
A 15-year-old male Chinese patient with global developmental delay, dyslexia and a background of recurrent blocked ears, tinnitus and allergic rhinitis on follow-up with Otolaryngology and no known drug allergy presented to the Children’s Emergency Department with the complaint of being unable to open his mouth. His vital signs (oxygen saturation, heart rate, respiratory rate and blood pressure) were normal and he was afebrile. He was also experiencing some discomfort in the left cheek region, with a pain score of 2 out of 10 using the numerical rating scale (NRS). The patient reported that he had started experiencing gradual limitation of mouth opening over the past 2 weeks while he was on an overseas holiday. There was no history of trauma to the facial and oral regions before this. It eventually culminated in him being unable to open his mouth, necessitating the visit to the Emergency Department. Written consent was obtained from the patient’s primary caregiver for the use of case information and clinical photos for the purpose of this publication.
Clinical findings
On examination, the patient was alert, comfortable and did not exhibit any malaise. He was not in respiratory distress, and there were no obvious signs of facial swelling. His left cheek region was slightly tender to palpation.
Intra-orally, the patient was noted to have fixed upper and lower orthodontic appliances, with the right end of the maxillary archwire terminating at the upper right first premolar bracket. The left end of the archwire could not be fully visualised due to the trismus and overlying buccal mucosa. His maximum mouth opening was approximately 2 mm (Figure 1).
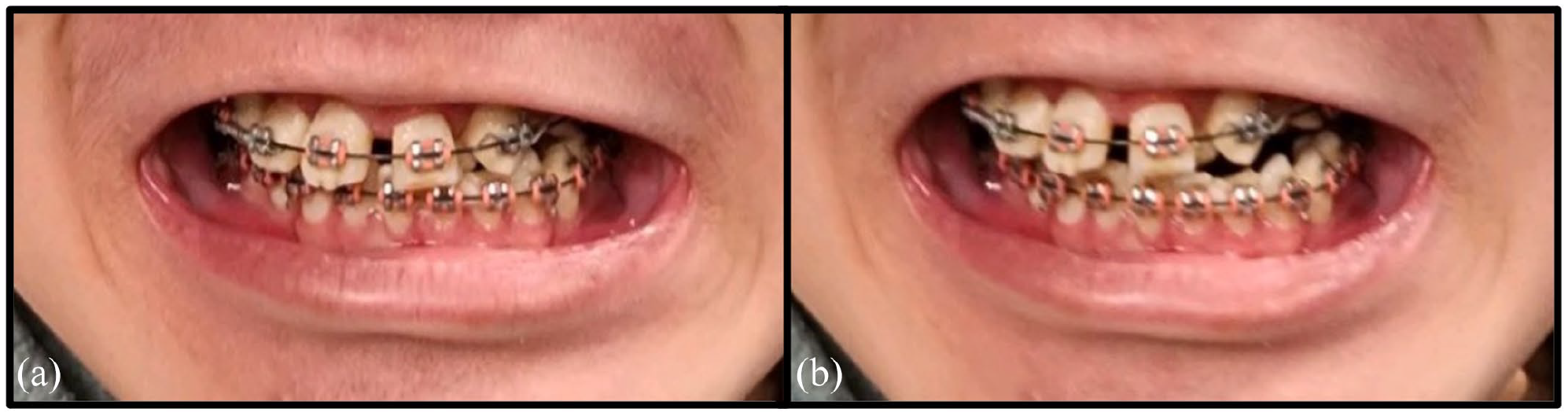
(a) Occlusion at maximum intercuspation and (b) at maximum mouth opening.
Diagnostic assessment
Plain skull radiographs were taken, which revealed the migration and penetration of about 3.5 cm of the maxillary archwire into the left infratemporal fossa (Figure 2).
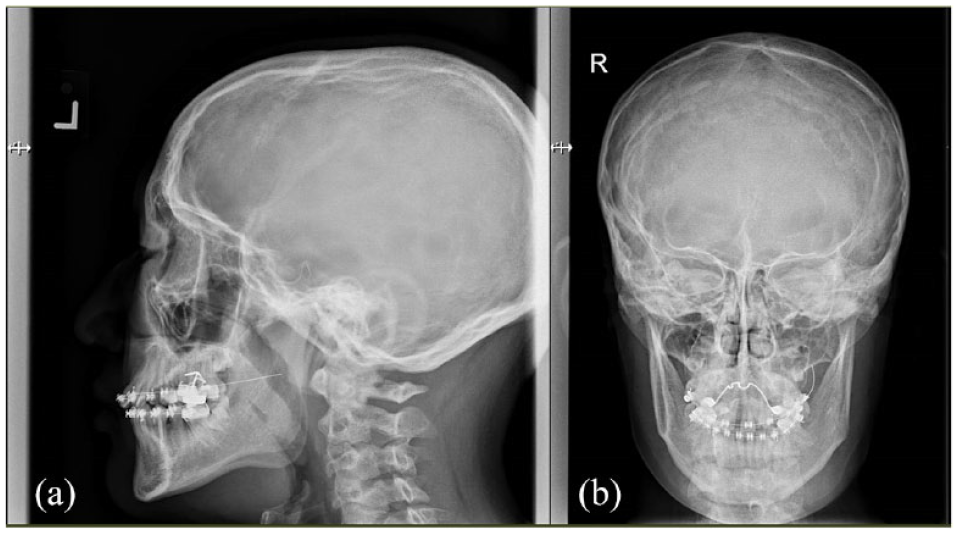
(a) Lateral view and (b) posteroanterior view.
Due to the extent of the archwire penetration into the infratemporal fossa as well as the trismus, a computed tomography (CT) scan of the facial region was ordered. However, before the scan could be performed, the archwire was prematurely removed without any local anaesthetics by the junior dental officer attending to the case in the Emergency Department. Removal of the archwire did not resolve the trismus.
The patient was admitted to the hospital with differential diagnoses of left medial pterygoid muscle inflammation, bleeding and haematoma formation within the infratemporal fossa affecting the pterygoid muscles, or an infection affecting those same muscles within the fossa.
A CT scan was performed of the facial region, which revealed an enlarged left medial pterygoid muscle with adjacent mild fat stranding which was suggestive of an infective/inflammatory aetiology. There was no discrete intramuscular or neck collection/haematoma identified (Figure 3).
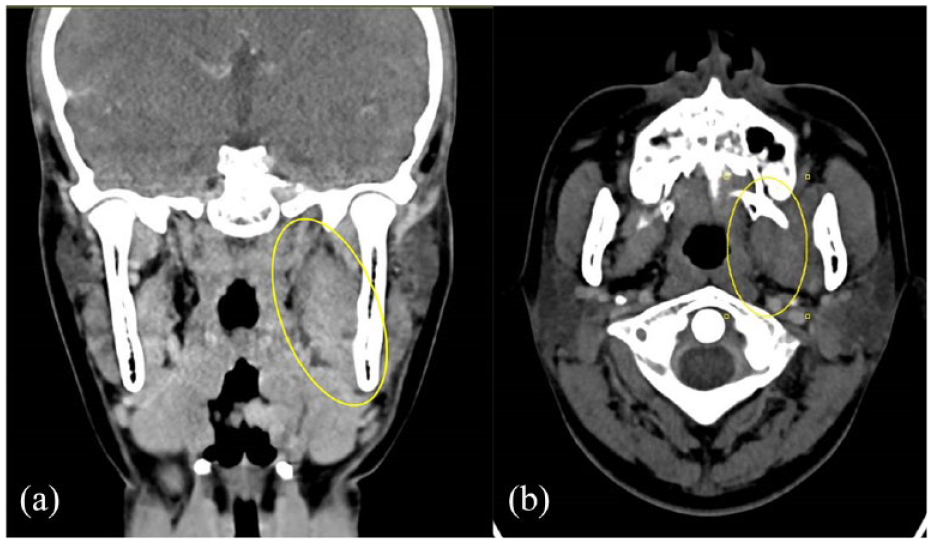
(a) Coronal view showing enlarged left medial pterygoid muscle and (b) transverse view showing enlarged left medial pterygoid muscle.
The CT scan findings confirmed the diagnosis of left medial pterygoid muscle inflammation due to the presence of the archwire foreign body, which resulted in the trismus.
Therapeutic intervention
The patient was started on intravenous (IV) augmentin antibiotic (1200 mg every 8 h) on admission, and upon confirmation of the diagnosis, he was placed on a 2-day course of IV dexamethasone (4 mg twice a day) to aid in the resolution of the inflammation and swelling.
Follow-up and outcomes
By the second day of admission, the patient’s maximum mouth opening had increased to approximately 6 mm and after completion of the 2-day course of IV dexamethasone, the patient was discharged with a 5-day course of oral antibiotics. On follow-up 2 weeks after discharge, the patient’s maximum mouth opening and range of motion had returned to normal (Figure 4). The sequence of events is illustrated in chronological order in Figure 5.

Normal mouth opening 2 weeks after discharge.
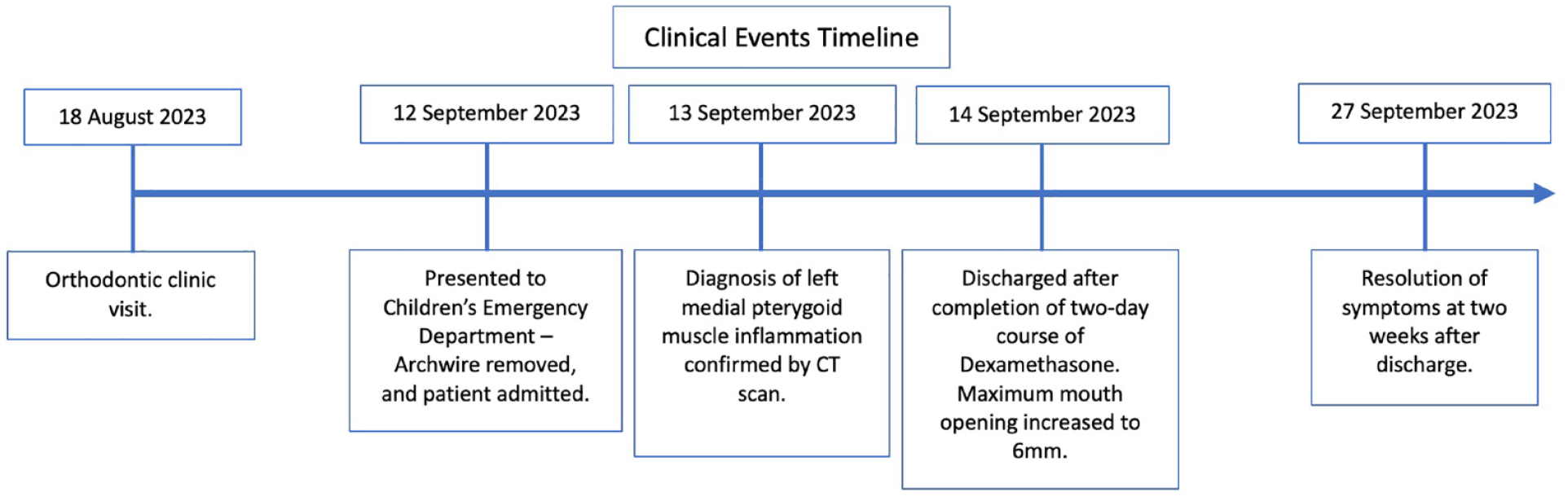
Clinical events timeline.
Discussion
Applied anatomy
The infratemporal fossa is an irregularly shaped cavity that is one of the most anatomically complex regions in the head and neck (Casale and Bordoni, 2023). The fossa is located inferior-medially to the zygomatic arch and is bounded by the posterolateral surface of the maxillary sinus, the ramus of the mandible, the medial pterygoid and tensor veli palatini muscles, styloid process and the tympanic part of the temporal bone (Casale and Bordoni, 2023; Vishteh et al., 1999).
Within the fossa, the maxillary artery with its associated branches, including the middle meningeal and accessory meningeal arteries, courses through. The venous pterygoid plexus that is connected to the cavernous sinus is also present. The carotid neurovascular bundle is also considered as part of the posterior boundary of the fossa (Casale and Bordoni, 2023).
The mandibular branch of the trigeminal nerve passes through the foramen ovale to enter the fossa. The mandibular nerve provides motor supply to the muscles of mastication and also provides sensory innervation to the buccal membrane in the oral cavity, the lower teeth, and the lower lip and chin. The auriculotemporal branch of the mandibular nerve is a sensory nerve to various regions on the lateral portion of the head (Casale and Bordoni, 2023). In addition, within the fossa are the lingual and chorda tympani nerves, which supplies general sensation and taste sensation to the anterior tongue. Autonomic nerves within the fossa pass from the otic ganglion to the glossopharyngeal nerve, and postsynaptic parasympathetic axons are able to innervate the parotid gland via the auriculotemporal nerve (Guo et al., 2015; Joo et al., 2013).
Anatomical implications to clinical practice
As evident from the intimate relationship of the neurovasculature within the infratemporal fossa, as well as the close proximity to vital structures like the cavernous sinus and the cranial base, the clinician will be able to appreciate the risk of injury or infection to the contents of the fossa. The presence of an infective process or bleeding and/or haematoma formation can easily result in trismus due to the involvement of the muscles of mastication within the fossa, and associated alteration to sensory and motor function may also present. Further, the spread of infection can involve the cavernous sinus or the cranial contents. Deeper penetrating injuries can result in injury to the carotid bundle, which has the potential to result in a life-threatening bleed.
Comparison with other cases
The management of a displaced orthodontic bracket embedded in the medial pterygoid surface during routine orthodontic adjustment has been reported in literature. The force of dislodgement was sufficient to allow the bracket to penetrate the mucosa of the oropharynx and become embedded in the deeper tissues (Wilmott et al., 2016). A similar case of embedded archwire in the buccal mucosa was also reported where it was speculated that the short segment of archwire had been propelled into the buccal mucosa during the clipping of the end of the archwire by the operator (Watanabe et al., 2023). Both these cases required surgical intervention to remove the foreign bodies and were fortunate to not have developed into an infection or damage to the surrounding neurovasculature.
Most recently, a severe complication associated with migrated archwire was reported in the literature, where a young patient developed seizures due to intraparenchymal haemorrhage from the migration of the mandibular archwire through the foramen ovale, terminating in the inferior temporal lobe (Morgan et al., 2023). This case represents the rare but severe consequences that can arise from the penetration of foreign bodies into the infratemporal fossa. Apart from that, this case also illustrates the importance of obtaining proper imaging before the removal of any foreign body within the deeper spaces surrounding the oral cavity like the oropharynx and the infratemporal space. The ability of the scans to identify the affected structures in the deeper tissue will be hindered if the foreign body is removed before imaging. The blind removal of foreign bodies without proper imaging can potentially result in devastating consequences like haemorrhage if the maxillary artery or carotid bundle is involved or cause further nerve/brain injuries.
The patient in the current report suffered only medial pterygoid muscle inflammation, without any injury to the neurovasculature. There was also no airway embarrassment during the period of trismus, and he experienced a relatively quick recovery after the removal of the archwire and a course of steroids and antibiotic therapy.
The patient was undergoing upper left canine retraction into the previously extracted upper left first premolar space. A flat 0.018-inch stainless steel ‘A. J. Wilcock Australian Wire’, adapted to his arch form, was used with 0.022 × 0.028-inch slot brackets. After canine ligation with a stainless-steel ligature, an elastomeric power chain, extending from the upper left canine to the terminal upper left second molar, was placed to retract the canine, along with lacing of the posterior teeth to reinforce anchorage. The rest of the teeth were tied to the archwire with elastomeric modules. It was likely that the wire migrated due to the lack of friction from the small wire gauge and the play in the bracket slot, and the lack of stops along the wire, for example, anterior ‘V-bend’ stops or cuspid loops, that could prevent lateral movements and migration of the wire. The rigidity of the stainless-steel wire also allows it to penetrate the soft tissue and migrate deeper compared to a nickel-titanium (Ni-Ti) wire, which will likely bend instead due to inherent elasticity. This incident occurred over a period of 2 weeks after placement of the archwire, and the authors hypothesised that the continued jaw movement and repeated tensing and relaxing of the musculature gradually pulled the archwire deeper into the tissues.
Methods to prevent migration of wire include:
Patient education to allow the early identification of wire dislodgement or migration. This will prevent the development of more serious complications as patients will know to seek treatment earlier.
Adding stops in the wire mesial and distal to the bracket in the form of cuspid loops, centreline ‘V-bend’ stops, or crimpable or soldered stops/hooks. This allows the archwire to be removed easily, compared to cinching the ends of the archwire (Modi et al., 2020). However, the location of the stops may interfere with tooth movement and the crimpable stops may dislodge.
Cinching the ends of the archwire (Fleming and Seehra, 2010).
Adding tipback or toe-in bends at the upper posterior segment (Takada and Lu, 2017). Clinicians should be aware that tipback bends may alter the overbite.
Conclusion
In summary, the potential risk of soft tissue injury and complications from orthodontic treatment is generally mild and limited. Soft tissue injuries can be avoided by careful management by the operator with the proper precautions taken to avoid accidental dislodgement of brackets and to prevent archwires from migrating into the surrounding soft tissues. Clinicians should be familiar with the surrounding soft tissue anatomy and be aware of the potential for more severe complications arising from injuries and foreign bodies being embedded in the soft tissues and provide management or referral to the appropriate specialty accordingly.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.