
Abstract
Objectives:
To evaluate the characteristics and content of YouTube™ videos created by patients undergoing orthodontic fixed appliance treatment and to assess the content accuracy of these videos.
Design:
A mixed-methods quantitative and qualitative study.
Data source:
YouTube™ webpage.
Methods:
The term ‘braces’ was used to search for relevant videos on the YouTube™ webpage between 18 August and 30 August 2020, with no limits imposed regarding how long the video had been available on YouTube™. Videos were included if they were made by patients and were predominantly about patients’ experiences during treatment with labial fixed appliances. The main themes/subthemes of the included videos were identified. A checklist was then developed to assess accuracy of the video content for two of the main themes and the videos were assessed against the checklist.
Results:
The video search identified 350 videos, of which 64 were selected as potentially eligible; 41 were subsequently excluded as they related primarily to the bond up/debond experience or had minimal information about orthodontics. This meant that 23 videos were ultimately included for analysis. Six main themes were identified in the videos: problems with fixed appliances, effects of fixed appliances, oral hygiene maintenance, dietary advice, treatment duration/appointment frequency and auxiliaries used with fixed appliances. From the 23 videos, 20 were assessed against the checklist for content accuracy related to two selected themes: oral hygiene maintenance and dietary advice. The majority of videos had low content accuracy scores, indicating that important and relevant content was generally missing.
Conclusion:
Several included videos focused on oral hygiene maintenance and dietary advice associated with fixed appliances; however, the content was incomplete and not always accurate. This is concerning to the profession, and it is therefore recommended that clinicians consider collaborating with patients to produce videos that are patient-centred and that also contain accurate information.
Introduction
Effective information provision for patients is important for several reasons, including to support good patient compliance. High-quality information regarding the material risks and benefits of treatment helps patients to better understand their role and the commitment for successful treatment (Smailhodzic et al., 2016; Tang and Newcomb, 1998). There has been a significant transformation in the provision of patient information from the traditional didactic approach by orthodontists to patients to the inclusion of peer-to-peer information exchange among orthodontic patients (Al-Silwadi et al., 2015; Papadimitriou et al., 2019). Many orthodontic patients share YouTube™ videos with other patients, providing so-called peer-to-peer information exchange (Papadimitriou et al., 2019). Orthodontic patients appear to be more active in sharing their own treatment experiences via YouTube™ than orthodontists are in providing patient information via this popular platform (Guo et al., 2020; Knösel and Jung, 2011; Livas et al., 2018). Patients may find peer-to-peer learning via YouTube™ videos effective because they are able to relate more readily to each other than to professionals (Rupert et al., 2014; Smailhodzic et al., 2016).
The quality of YouTube™ videos relating to orthodontics has been found to range from poor to good (Grewal et al., 2019; Hegarty et al., 2017; Lena and Dindaroglŭ, 2018). These assessments also appear to be affected by heterogenous search strategies and assessment tools used in the literature (Grewal et al., 2019; Hegarty et al., 2017; Ustdal and Guney, 2020). However, there are limited publications that have compared YouTube™ video content with the information provided in professionally developed orthodontic resources; therefore, there is a lack of evidence supporting the recommendation of the YouTube™ videos created by patients for patients.
The aims of this study were to evaluate the characteristics and content of YouTube™ videos created by patients and that related to patients’ treatment experiences with orthodontic fixed appliances. Also to assess the accuracy of the content of these patient-created YouTube™ videos, by assessing them against the information provided in accepted orthodontic resources utilised by professionals.
Methods
This study was conducted in two parts:
Part 1: the development of inclusion and exclusion criteria, video search and selection, data collection and identification of the themes in the included videos.
Part 2: the development of an assessment checklist to assess content accuracy of the videos, followed by identification of the videos for inclusion in this assessment and subsequent data analysis.
Part 1
Development of inclusion and exclusion criteria
Inclusion and exclusion criteria were pre-developed based on the professional opinion of two experienced orthodontic researchers (MOS, SJC) (Appendix 1). These selection criteria were then pilot-tested by conducting a YouTube™ video search on 18 August 2020 using the search term ‘braces’. This term was most commonly used by those looking for online information related to orthodontics on Google Trends (Google, 2006). The pilot video search was undertaken using the following settings to minimise selection bias:
The browser history and cookies were deleted before commencing the search.
Private browsing mode was used to search for videos on the YouTube™ webpage (https://www.youtube.com/) under the default YouTube™ setting, where videos were sorted according to the relevance of search subject.
The location was set as the United Kingdom as that was where the researchers resided. No further search filter was applied.
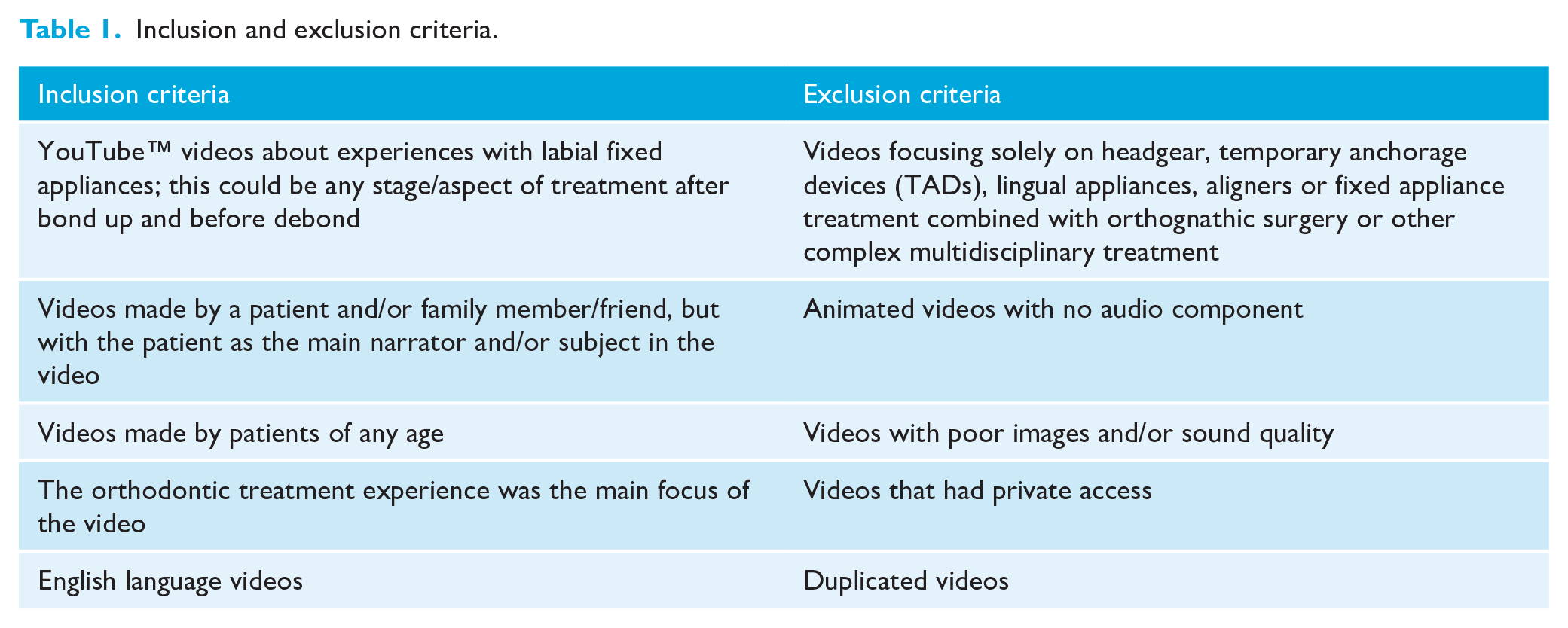
In order for videos to be eligible for inclusion, the patient had to be the main ‘narrator’ and/or subject to ensure that the treatment experience was definitely their own. Only English language videos were included because English was the only language that all the researchers spoke. The exclusion criteria were videos with only animation and no audio, and/or poor images/sound quality, and/or private access, because these videos could not provide useful information about patients’ treatment experiences.
The pilot video search identified 100 videos, of which the first 30 videos were independently screened for eligibility by all three researchers (IL, MOS, SJC). The three researchers showed high levels of agreement regarding whether they could be included: 3 out of 30 were included, 24 were excluded and 3 were debated further because of differences in interpretation.
After discussion, the inclusion/exclusion criteria were modified to allow enhanced interpretation and a more focused sample. The modifications were:
Videos had to specifically include information about patient experiences during treatment with labial fixed appliances. Videos that focused primarily on bond up or debond were excluded.
Videos that focused purely on lingual fixed appliances or aligners were also excluded.
The final inclusion and exclusion criteria developed for this study are summarised in Table 1.
Inclusion and exclusion criteria.
Video search
A final YouTube™ search was conducted on 30 August 2020 by IL (postgraduate orthodontic student) to identify the first 350 videos, using the same settings as in the pilot study. This number of videos was deemed sufficient for selection because 90% of Internet users only use the results in the first three pages of a search (iProspect, 2006).
Video selection
Before the final video selection, a calibration exercise was undertaken by IL and SJC, using 20 videos randomly selected from the 350 identified videos. Inter-examiner reliability in video selection was tested using Cohen’s kappa.
The videos identified by the search were then screened for eligibility. All videos considered eligible or potentially eligible were watched and final videos for selection were included based on the inclusion and exclusion criteria shown in Table 1. This process was undertaken independently by IL and SJC and the results then compared. Any disagreement was resolved by discussing with the third researcher (MOS). The process of video selection is summarised in Figure 1.
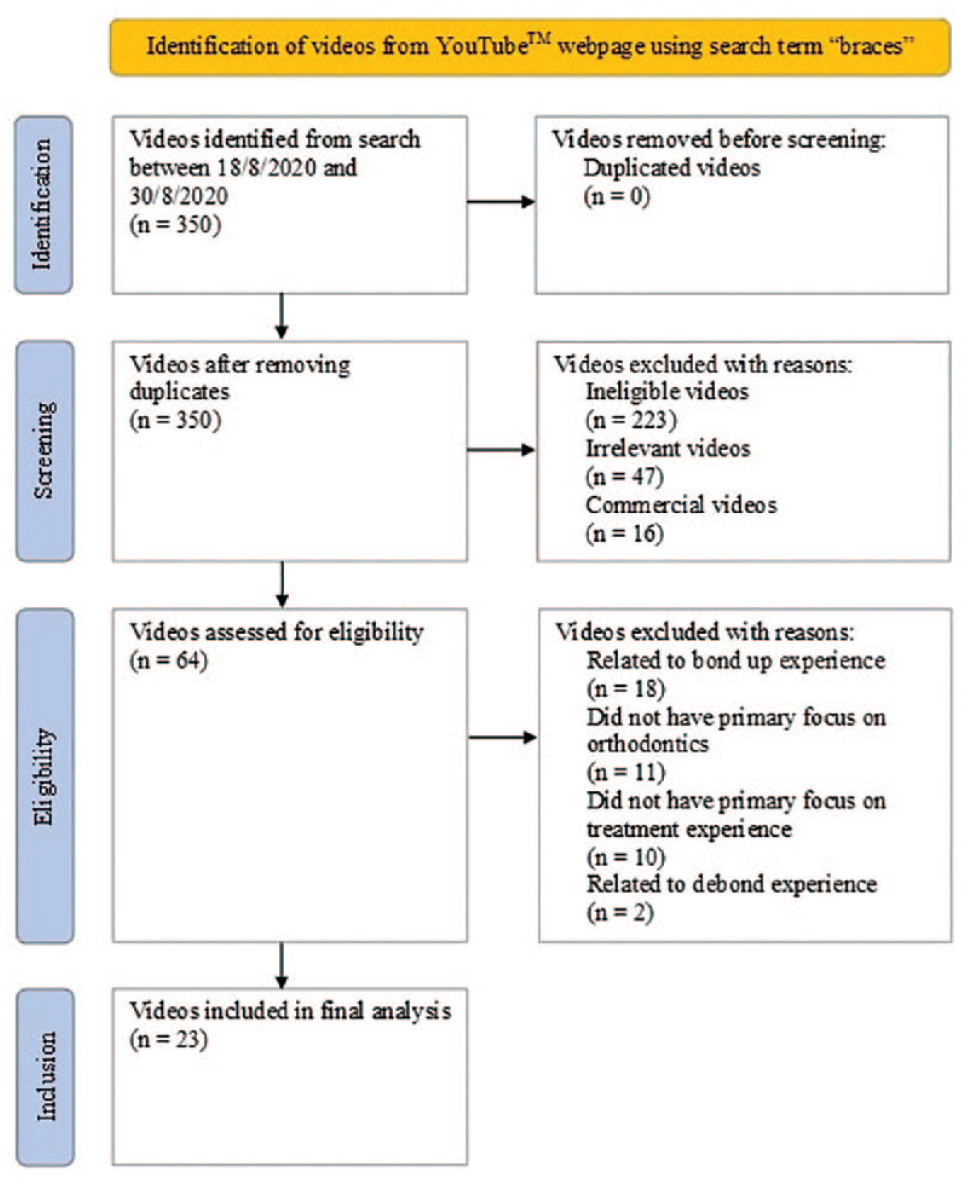
PRISMA flow diagram for video selection in Part 1 of the study.
Data collection
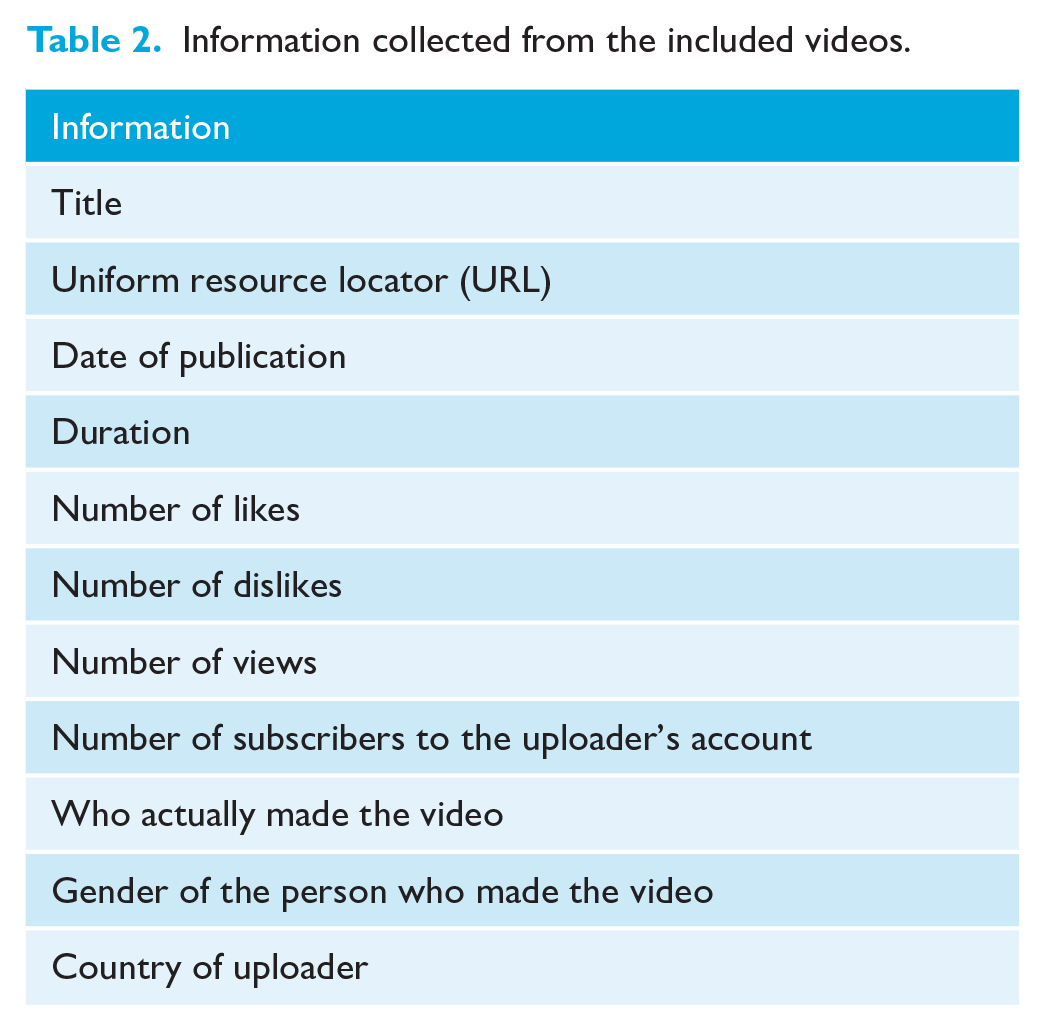
The included videos were then watched again by IL to extract information regarding the characteristics of the videos. This information included title, uniform resource locator (URL), date of publication, number of likes and dislikes, number of views, number of subscribers to the uploader’s account, who actually made the video, gender of the person who made the video and country of uploader (Table 2). All the information collected was recorded in a Microsoft Excel sheet.
Information collected from the included videos.
Identification of the themes in the included videos
One of the researchers (IL) analysed the included videos using a basic descriptive analysis to identify the main themes and subthemes. The researcher also attended a Qualitative Data analysis course before commencing the study to familiarise themselves with the techniques employed. The videos were watched in full to obtain an overview of the video focus, and they were then progressively categorised into different themes based on the main content. Each theme was independent and did not overlap with another. However, a video that had a variety of content could be categorised into more than one theme. Each theme was then further categorised into subthemes to describe the content more thoroughly. The themes and subthemes identified were then reviewed by all three researchers and any disagreement was resolved by discussion.
Part 2
Development of an assessment checklist to assess content accuracy of the videos
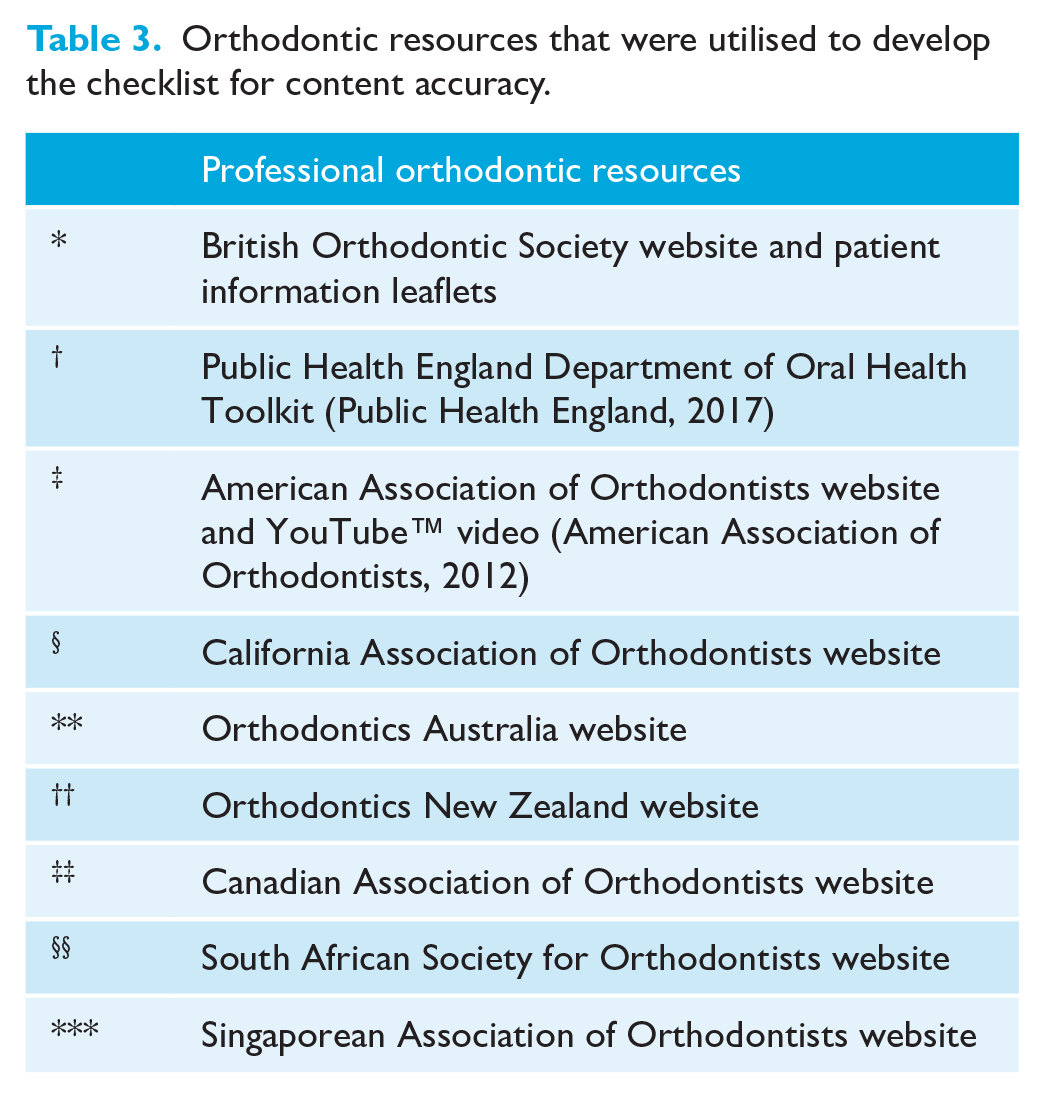
A checklist was developed to assess the content accuracy of the included videos. The three researchers reviewed website information and information leaflets in the English language provided by major orthodontic societies. The orthodontic resources used in the development of this checklist are shown in Table 3. There was extensive information provided regarding oral hygiene maintenance and dietary advice associated with fixed appliances on the websites and in the professional information leaflets reviewed; therefore, these two areas were selected for the assessment of content accuracy in Part 2. The checklist which was developed consisted of 19 items related to oral hygiene maintenance and 10 items related to dietary advice (Table 4).
Orthodontic resources that were utilised to develop the checklist for content accuracy.
Checklist for the accuracy of video content.
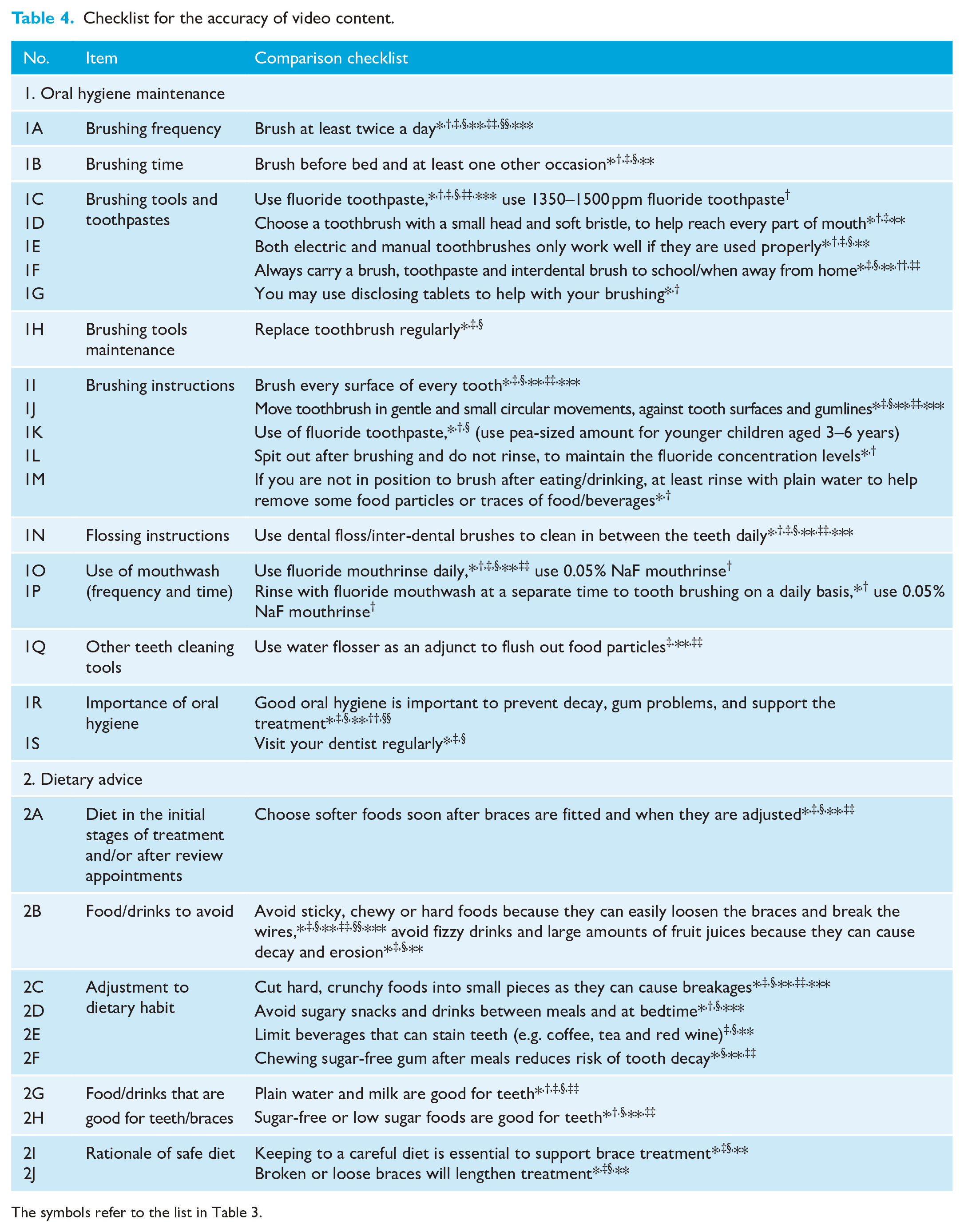
The symbols refer to the list in Table 3.
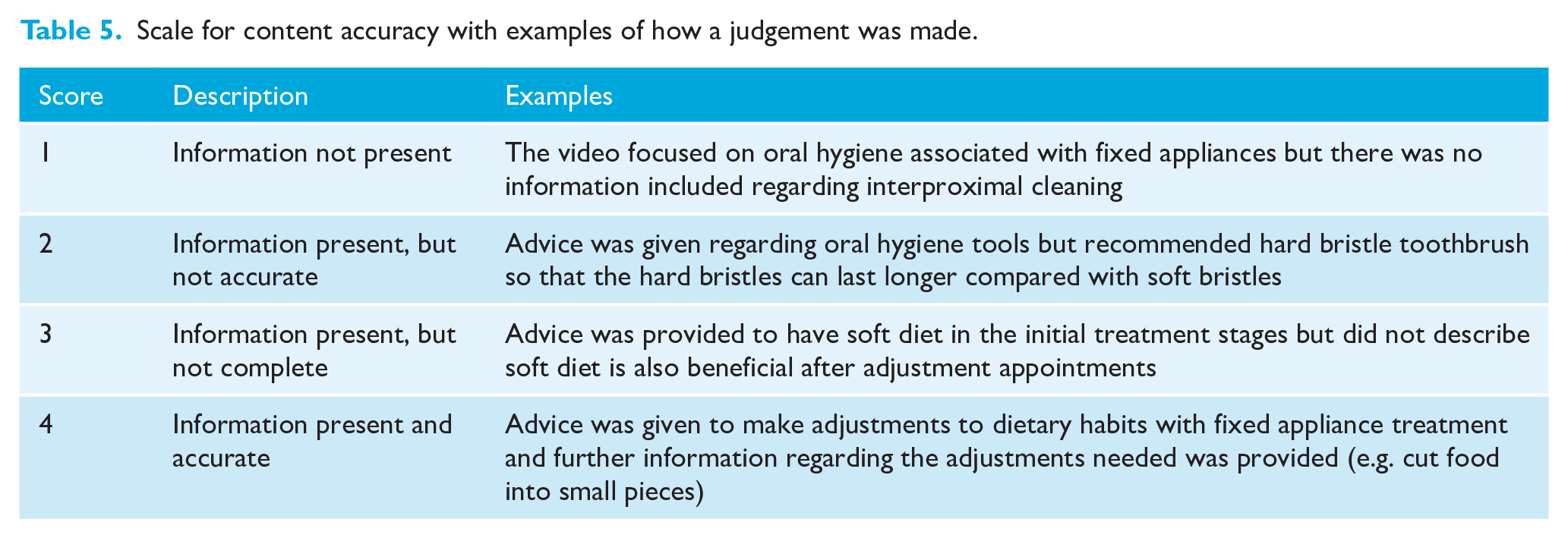
A 4-point scale was adapted from previous similar research to assess the accuracy of video content (Sharif and Alkadhimi, 2019; Smyth et al., 2020). A score of 1 indicated that the relevant information was not present, a score of 2 indicated that information was present but not accurate, a score of 3 referred to information being present but not complete and a score of 4 referred to the information being present and accurate. Table 5 shows these scores, with examples to illustrate how judgements were made.
Scale for content accuracy with examples of how a judgement was made.
The checklist and content accuracy scale were pilot-tested for feasibility with five videos randomly selected from those identified for inclusion in Part 1 of the study. This was undertaken by all three researchers; any disagreement was resolved by discussion and it was decided to include a not applicable (N/A) option for videos that did not focus on a particular aspect in order to prevent items being underscored.
Inclusion of videos for assessment of content accuracy
The checklist developed was used in the assessment of video content accuracy. Videos were included in this assessment if they focused on at least one of the themes identified. Determination of which videos should be included was by one researcher (IL) and reviewed by the other two researchers (MOS, SJC). Any disagreement was resolved by discussion. Figure 2 summarises this process.
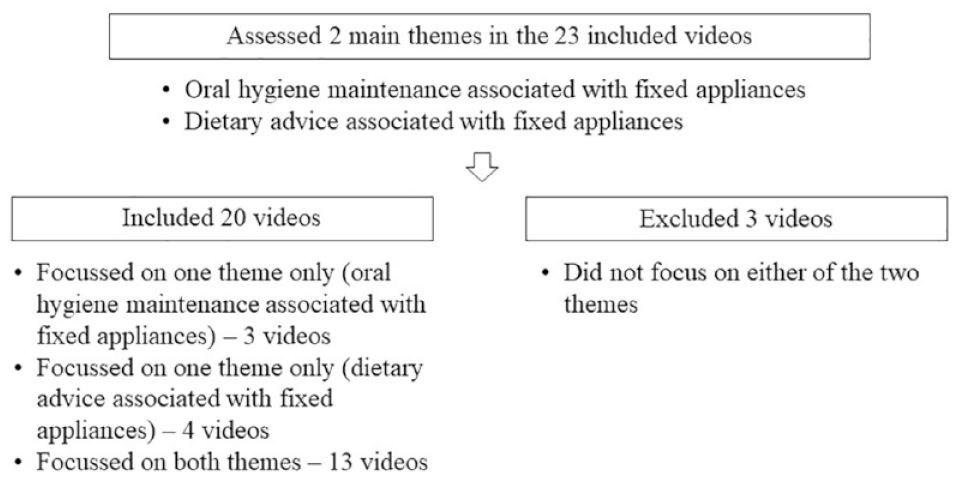
Inclusion of videos for assessment of content accuracy in Part 2 of the study.
Assessment of video content accuracy
Before assessment of the content accuracy of the videos, a calibration exercise was undertaken by two of the researchers (IL, MOS) and inter-examiner reliability was tested using Cohen’s kappa. Intra-examiner reliability was also measured by one of the researchers (IL) re-scoring the same calibration videos 2 weeks after the first scoring.
The videos included in Part 2 of the study were then assessed against the checklist developed for content accuracy. The videos were individually scored for each item on the checklist (item score) and scores were recorded in a Microsoft Excel sheet (Appendix 2).
Data analysis
The frequency of the content score per item on the checklist were calculated using Microsoft Excel (Microsoft 365).
Results
Part 1
Outcome of video search and selection for eligibility
The YouTube™ video search aimed to identify 350 videos using the search term ‘braces’. Of these, 64 videos were selected as potentially eligible, and after further assessment, 23 videos were included. In total, 41 videos were excluded, as they either related to the bond up (n = 18) or debond experience (n = 2) or did not have a primary focus on orthodontics (n = 11) or on the treatment experience (n = 10). There was a perfect agreement between the two researchers in the video selection with a Cohen’s kappa statistic of 1.00.
Characteristics of included videos
Table 6 shows the characteristics of the included videos. All of the included videos (n = 23) were published between 2015 and 2020. The video duration ranged from 2 min 7 s to 28 min 58 s. The highest number of views recorded for the videos was over 11 million, whereas the lowest was 770. The most viewed video (video 3) had the highest number of likes (84,000) and dislikes (5100) and was posted by the YouTube™ account that had the highest number of subscribers (3.4 million). In contrast, the video with the lowest number of views (video 23) had the lowest number of likes (43) and dislikes (0) and was posted by a YouTube™ account that had 10,200 subscribers.
Characteristics of the 23 included videos in Part 1 of the study.
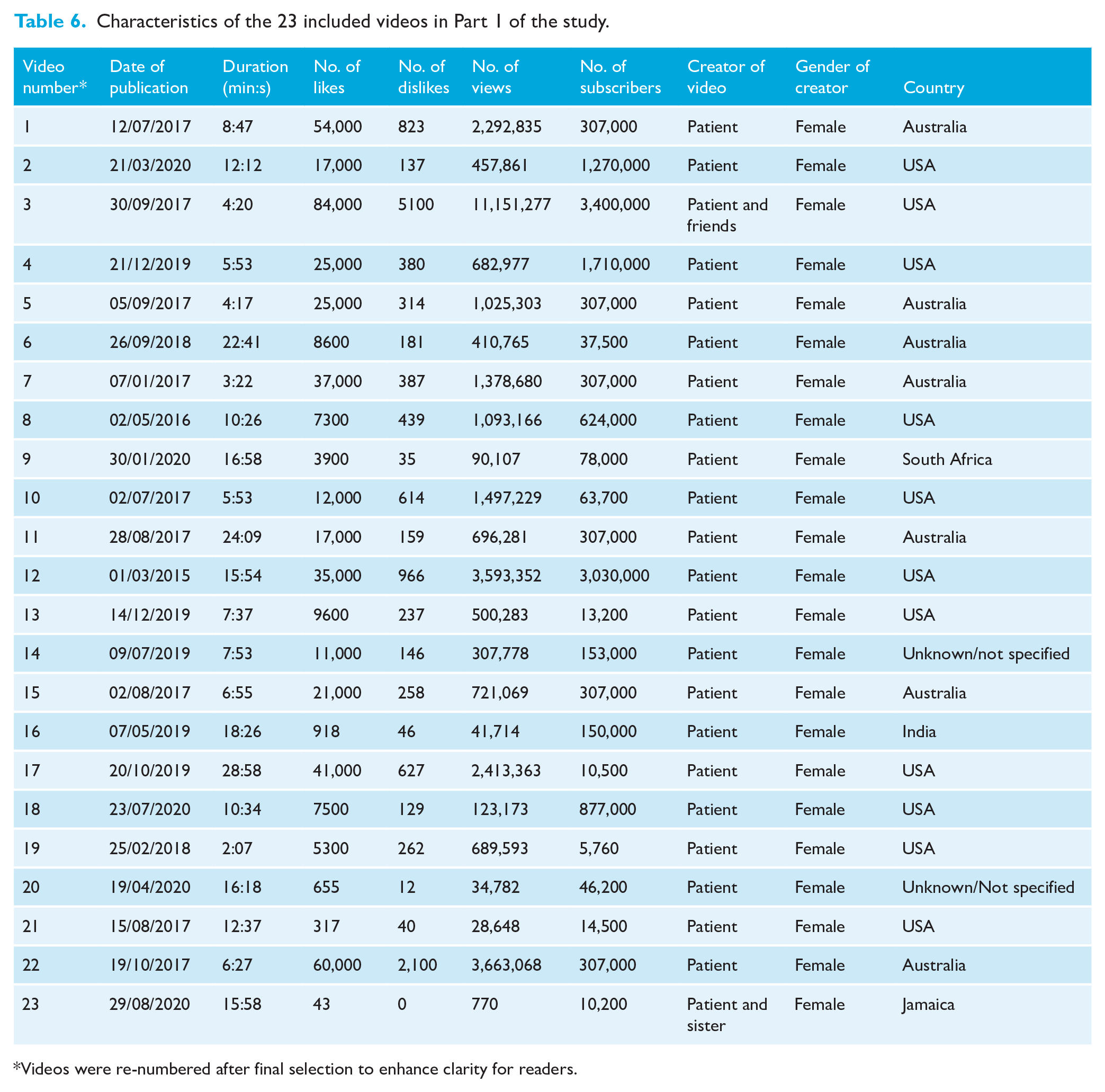
Videos were re-numbered after final selection to enhance clarity for readers.
The majority of videos (21/23) were made by the patient alone, one video was made by the patient and a family member, and one video was made by the patient and their friends. Interestingly, all the patients in the videos were female. The geographic location where the videos were made was mainly the USA (n = 11), followed by Australia (n = 7), South Africa (n = 1), Jamaica (n = 1) and India (n = 1). Two videos did not specify the geographical location in which they were made.
Identification of the themes in the included videos
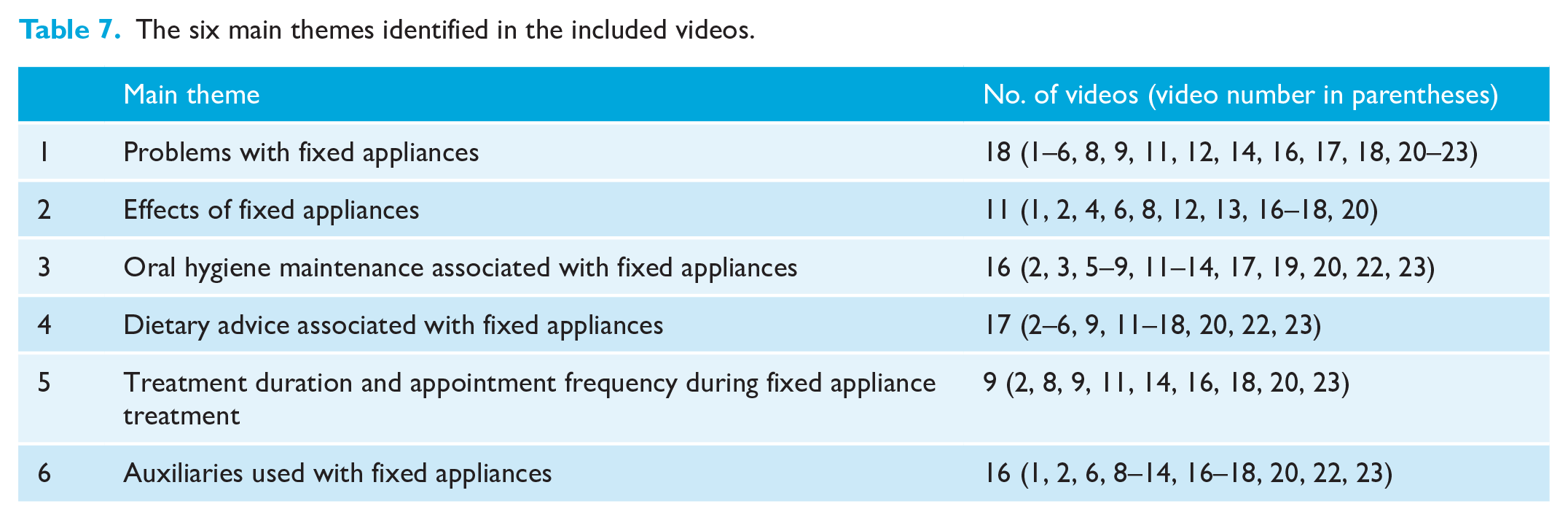
There were six main themes identified in the included videos: (1) problems with fixed appliances; (2) effects of fixed appliances; (3) oral hygiene maintenance associated with fixed appliances; (4) dietary advice associated with fixed appliances; (5) treatment duration and appointment frequency during fixed appliance treatment; and (6) auxiliaries used with fixed appliances (Table 7). Each main theme was divided into subthemes to further describe their content. Tables 8–13 give examples of quotes from the videos for each theme/subtheme, with the video number in brackets after each quote.
The six main themes identified in the included videos.
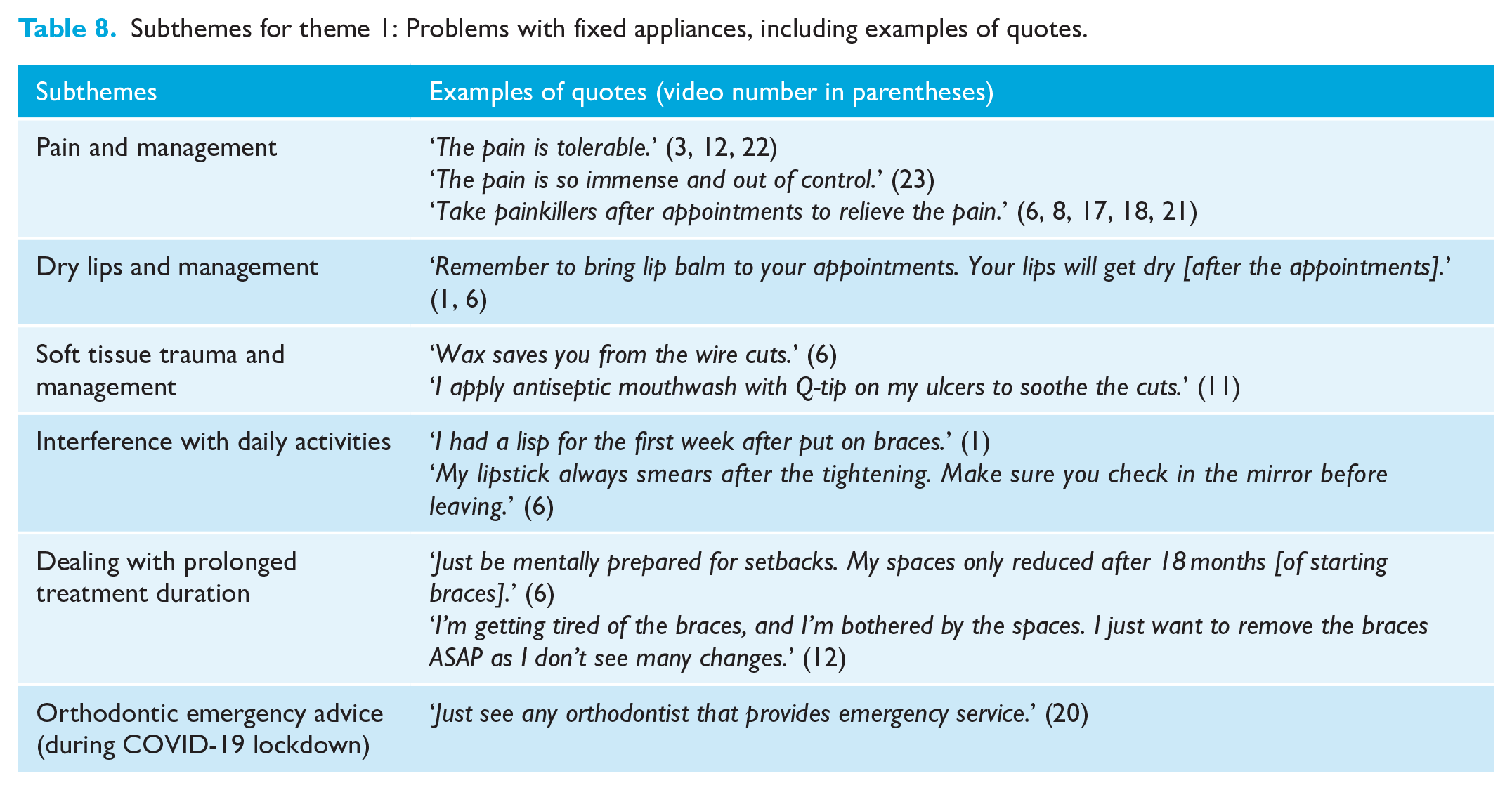
Subthemes for theme 1: Problems with fixed appliances, including examples of quotes.
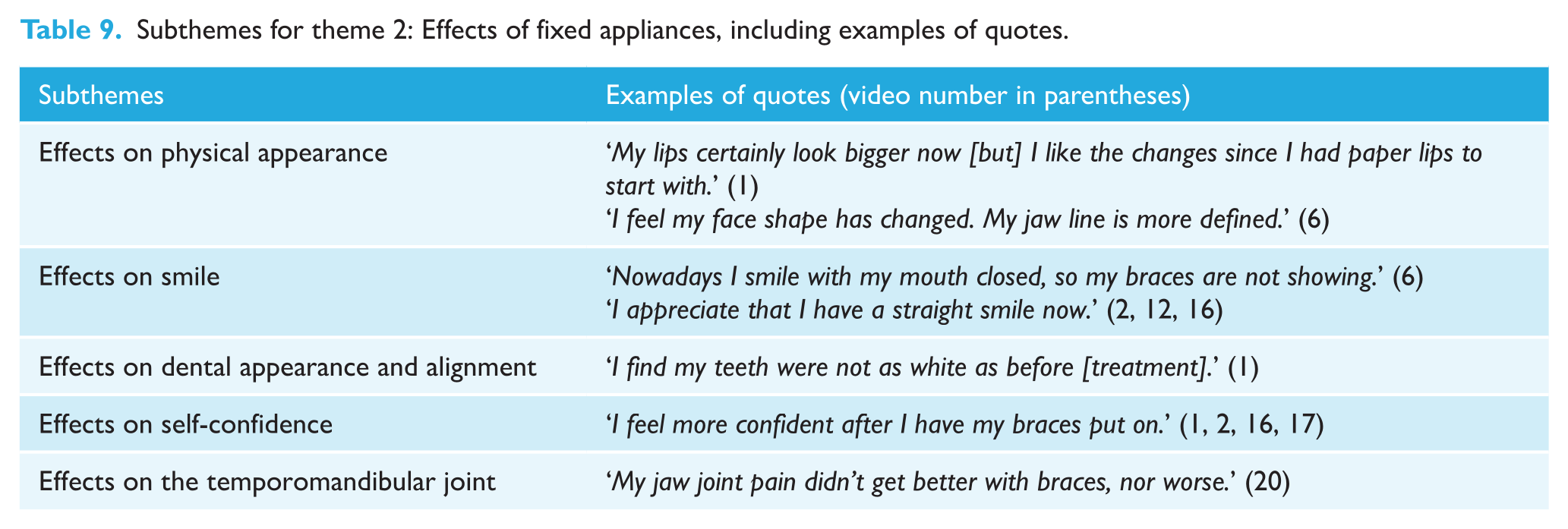
Subthemes for theme 2: Effects of fixed appliances, including examples of quotes.
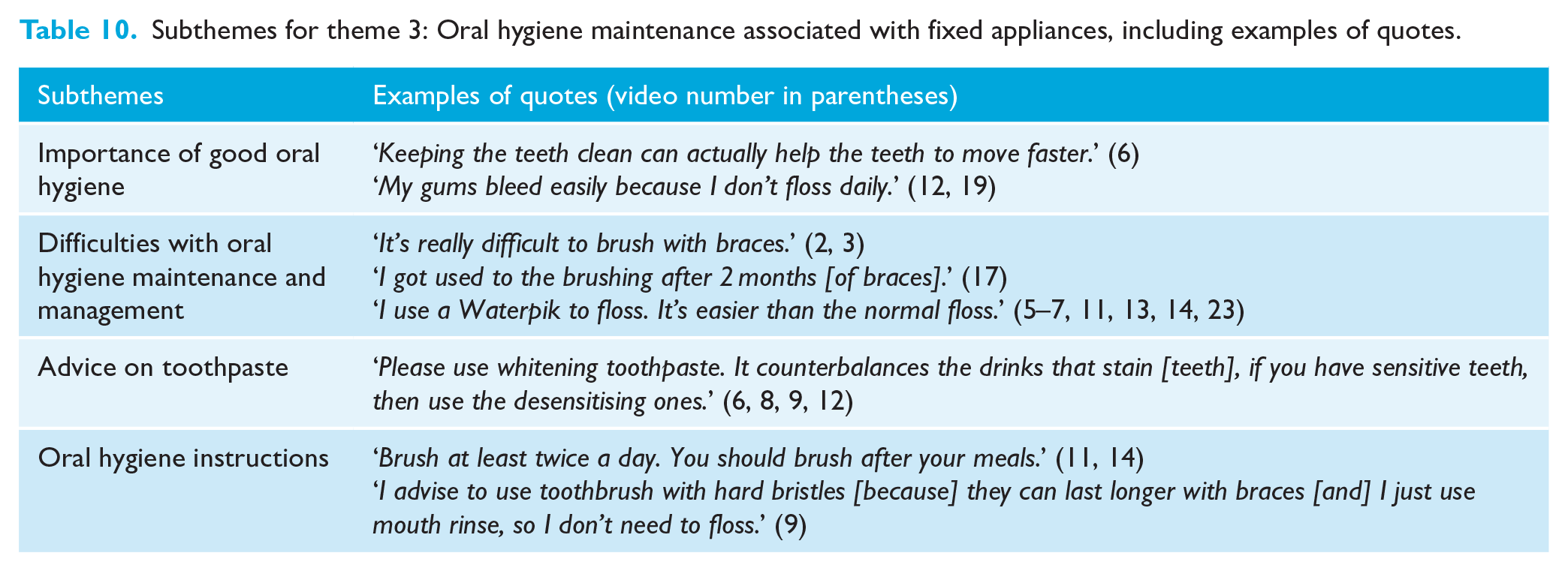
Subthemes for theme 3: Oral hygiene maintenance associated with fixed appliances, including examples of quotes.
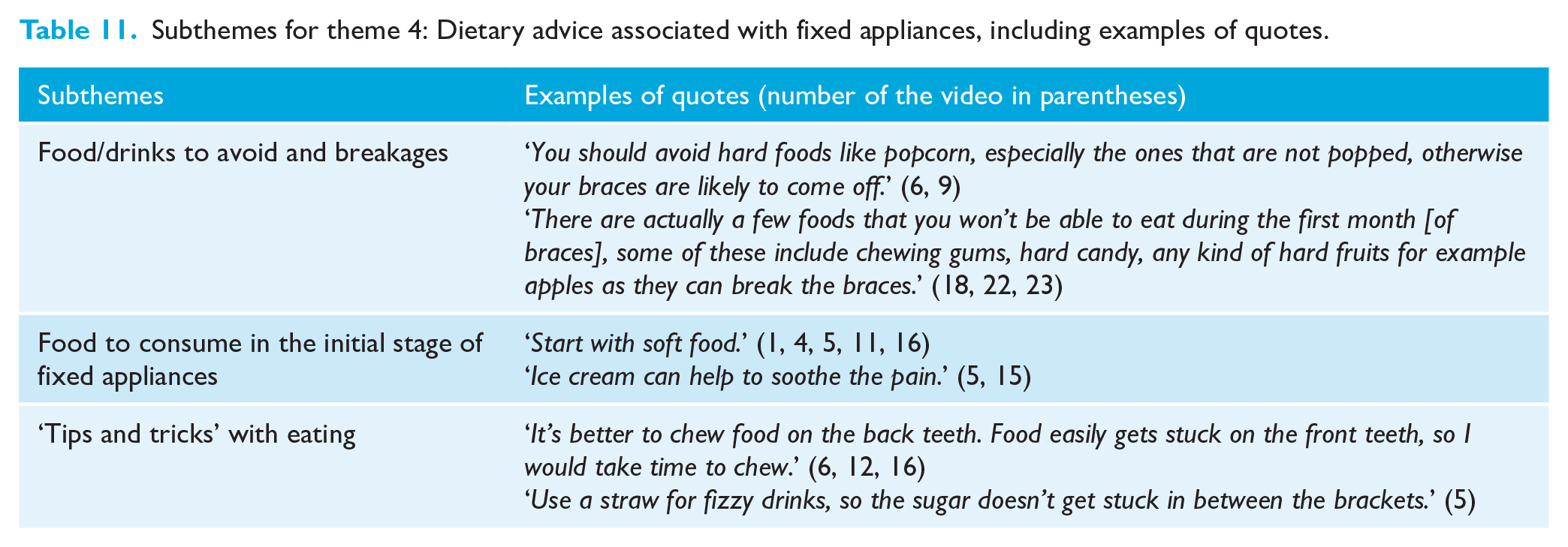
Subthemes for theme 4: Dietary advice associated with fixed appliances, including examples of quotes.
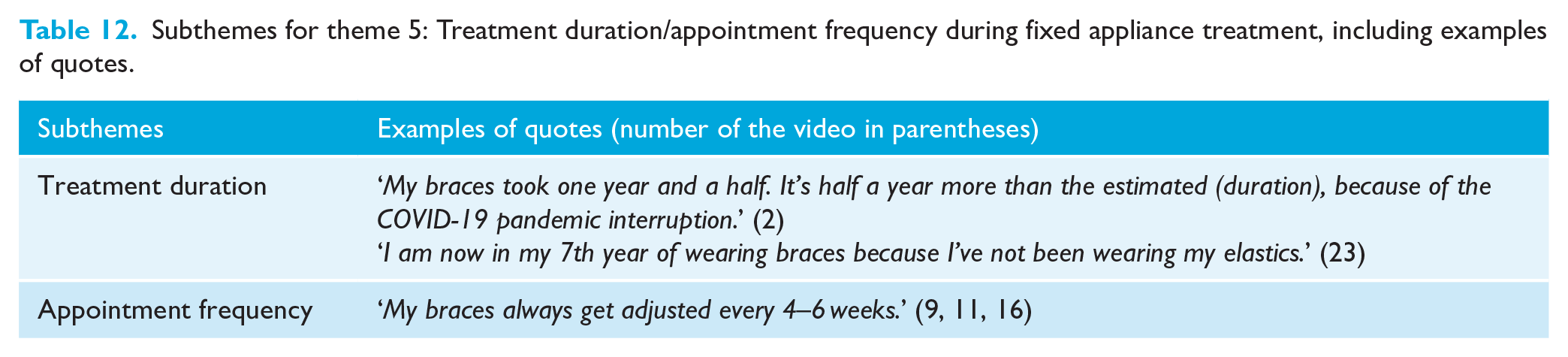
Subthemes for theme 5: Treatment duration/appointment frequency during fixed appliance treatment, including examples of quotes.
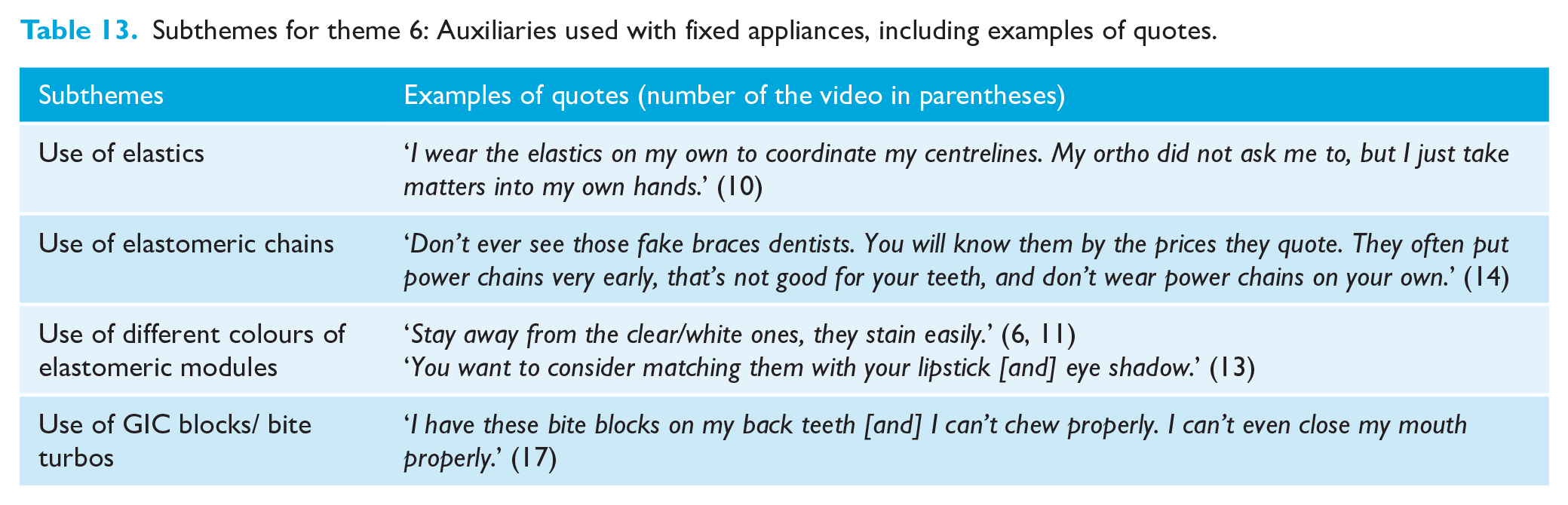
Subthemes for theme 6: Auxiliaries used with fixed appliances, including examples of quotes.
Theme 1: Problems with fixed appliances (Table 8)
There were 18 videos that focused on problems associated with fixed appliances and within this theme there were six subthemes. Patients described how they experienced pain and discomfort, dry lips and intra-oral soft tissue trauma after their fixed appliance adjustments, and often provided advice regarding how to manage these problems. Several patients in the videos also reported fixed appliances interfering with their daily social activities; these included developing a lisp when speaking or singing, developing a ‘teeth-clicking’ habit, lipstick smears and difficulty in mouth opening. Most of the patients encouraged a positive mindset to deal with the treatment; however, one patient clearly had reduced motivation as their treatment progressed.
Theme 2: Effects of fixed appliances (Table 9)
There were 11 videos that focused on the effects of fixed appliances, ranging from changes in physical appearance to effects on self-confidence. It was found that different patients had different perceptions about the changes in their facial appearance, smile, dental appearance and alignment.
Theme 3: Oral hygiene maintenance associated with fixed appliances (Table 10)
There were 16 videos included in this category and these videos included the importance of good oral hygiene, difficulties encountered and oral hygiene advice. It was encouraging to note that although some videos described the challenges in maintaining good oral hygiene, presenters also reassured viewers that the challenges could be overcome with daily practice. A number of videos acknowledged the importance of good oral hygiene in supporting fixed appliances and some patients actually demonstrated oral hygiene techniques.
Theme 4: Dietary advice associated with fixed appliances (Table 11)
There were 17 videos that included dietary advice associated with fixed appliances and this advice was further categorised into three subthemes. Generally, videos advocated avoiding hard foods due to potential fixed appliance breakages. They also recommended a soft diet during the initial stages of fixed appliances to aid adaptation. Some other useful methods to minimise breakages and food impaction were also included.
Theme 5: Treatment duration/appointment frequency during fixed appliance treatment (Table 12)
There were 9 videos that discussed treatment duration and appointment frequency during fixed appliance treatment. Although the descriptions were brief, a small number of the videos further reflected on the possible reasons for extended treatment duration.
Theme 6: Auxiliaries used with fixed appliances (Table 13)
The final theme included 16 videos that discussed the use of auxiliaries with fixed appliances. These included, for example, discussions related to elastics, elastomeric chain, elastomeric modules and bite turbos. The videos often shared information about different auxiliaries in fixed appliances; however, only a small number explained why they were used.
Part 2
Inclusion of videos for assessment of content accuracy
The checklist covered two themes (oral hygiene maintenance and dietary advice associated with fixed appliances); therefore, these two themes were used for the assessment of content accuracy. From the 23 videos included in Part 1 of the study, 20 videos were included in Part 2 of the study because they focused on these two themes: 13 of the 20 videos focused on both themes; three focused only on oral hygiene maintenance; and four focused only on dietary advice (Appendix 2). The remaining three videos were excluded as they did not focus on either of the two themes.
Inter- and intra-reliability in assessment of content accuracy
There was perfect agreement between the two researchers with a Cohen’s kappa statistic of 1.00. A Cohen’s kappa statistic of 1.00 was also achieved for intra-examiner reliability.
Content accuracy for the videos that focused on oral hygiene maintenance
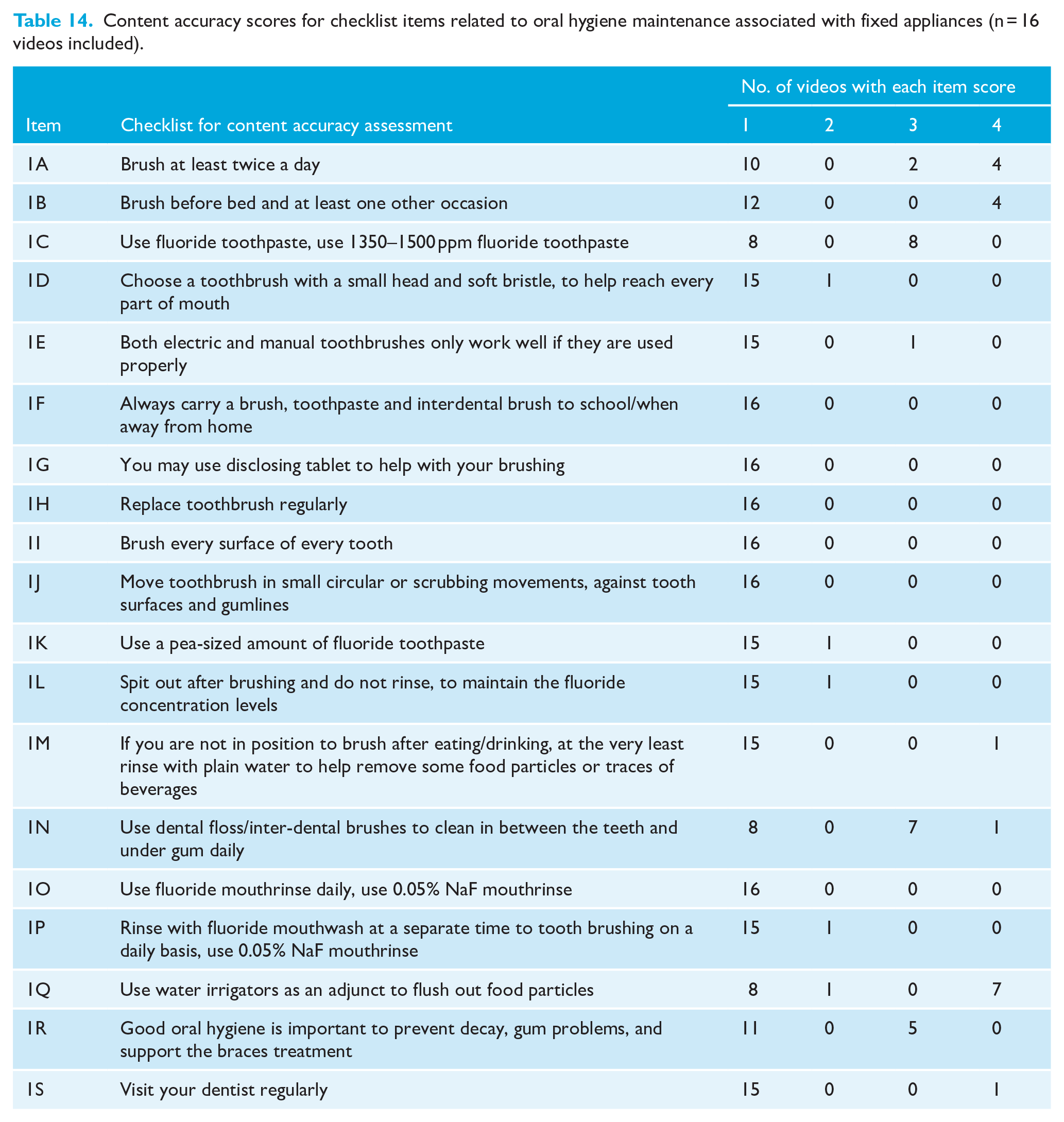
Table 14 shows the content accuracy scores of videos that focused on oral hygiene maintenance associated with fixed appliances (n = 16). The majority of scores on the 19-item checklist related to this theme were 1, indicating that the information was not present. The item that scored most highly and most frequently achieved a score of 4 (information present and accurate) and was related to the use of water flossers/irrigators as adjuncts (item 1Q, n = 7). The items that most frequently scored 3 (information present but not complete) were related to the use of fluoridated toothpaste (item 1C, n = 8), the use of dental floss/interdental brushes for interproximal cleaning (item 1N, n = 7) and also item 1R, which highlighted the importance of good oral hygiene (n = 5). There were only a small number of items that scored 2 (information present but not accurate).
Content accuracy scores for checklist items related to oral hygiene maintenance associated with fixed appliances (n = 16 videos included).
Content accuracy for the videos that focused on dietary advice
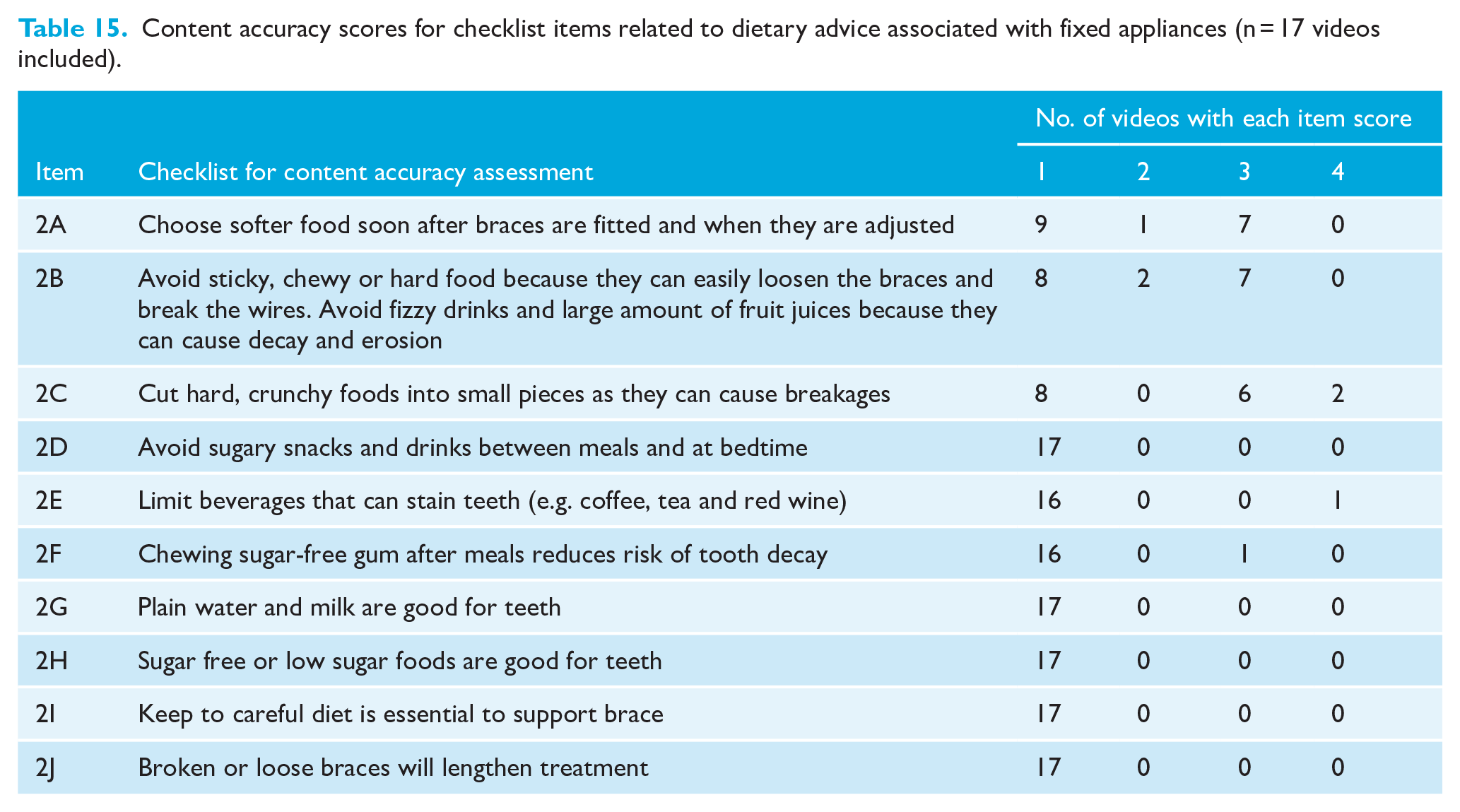
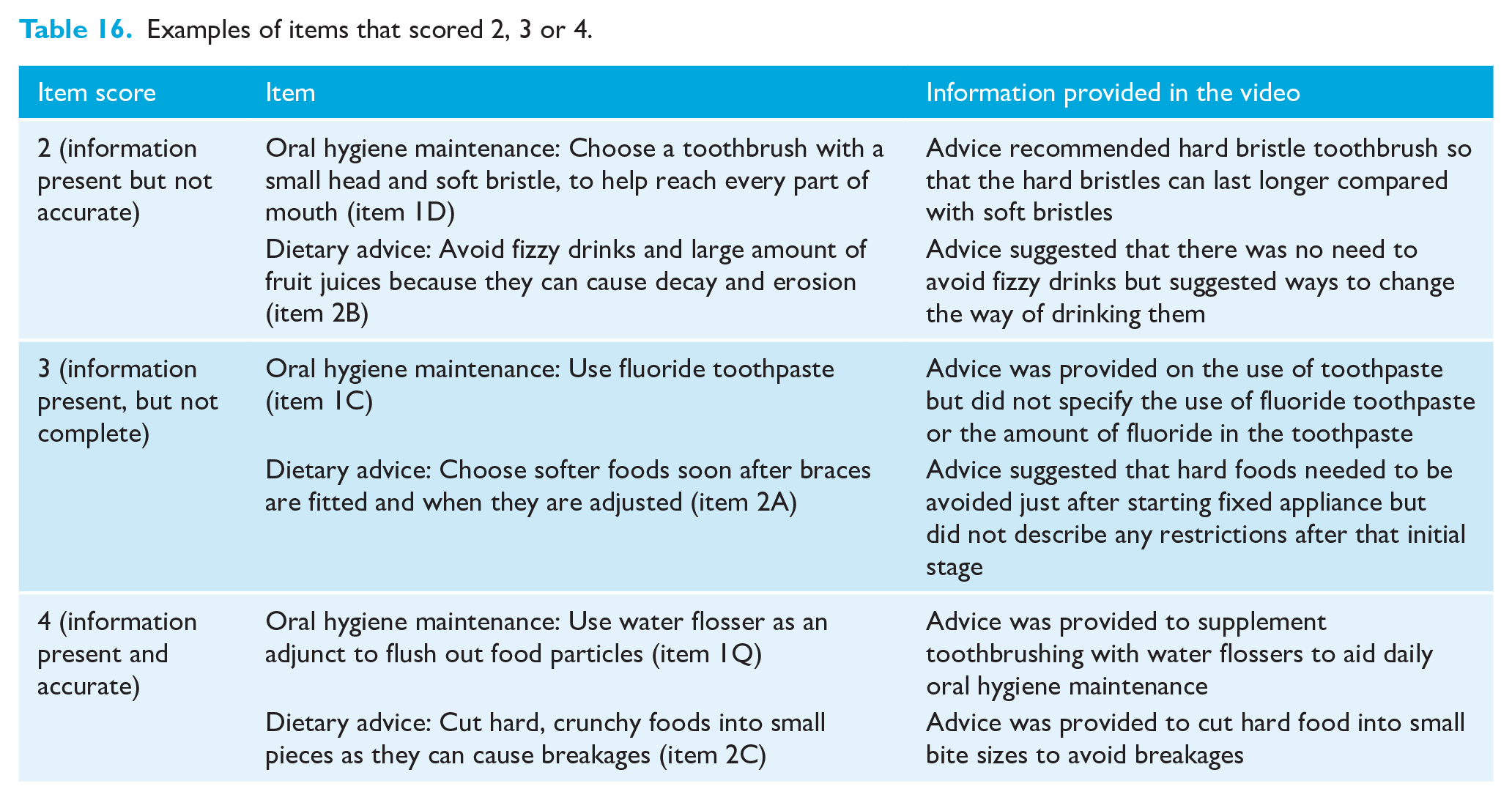
Table 15 shows the content accuracy scores for those videos that focused on dietary advice associated with fixed appliances (n = 17). The majority of the videos scored 1 (information not present) on the 10-item checklist. Items that scored 4 (information present and accurate) were few in number and were related to cutting hard foods into small pieces to avoid breakages (item 2C, n = 2) and avoiding sugary snacks and drinks between meals and at bedtime (item 2E, n = 1). The items that most frequently scored 3 (information present but not complete) were related to choosing softer foods after the braces are fitted and when they are adjusted (item 2A, n = 7) and avoiding sticky/chewy/hard foods and fizzy drinks/large amounts of fruit juice (item 2B, n = 7). There were only a small number of items that scored 2 (information present but not accurate). Table 16 shows examples of items scored 2, 3 and 4.
Content accuracy scores for checklist items related to dietary advice associated with fixed appliances (n = 17 videos included).
Examples of items that scored 2, 3 or 4.
Discussion
Summary of the results
This paper presents the findings of a video search using the search term ‘braces’ on the YouTube™ webpage. The video search was conducted between 18 August and 30 August 2020. In total, 350 videos were identified, of which 23 were eligible for inclusion in Part 1 of the study. These videos included a variety of information related to patients’ treatment experiences and six main themes were identified: problems with fixed appliances; effects of fixed appliances; oral hygiene maintenance; dietary advice associated with fixed appliances; treatment duration and appointment frequency during fixed appliance treatment; and auxiliaries used with fixed appliances.
From the 23 videos, 20 were then assessed against a checklist developed for the assessment of content accuracy in Part 2 of the study and scored using a 4-point scale. The feasibility of using the checklist and scale was confirmed with a pilot study. The majority of videos that focused on oral hygiene maintenance and dietary advice associated with fixed appliances achieved low item scores of 1 (information not present), indicating most of the important information about oral hygiene maintenance and dietary advice was missing.
Comparison with other studies
Characteristics of the included videos
The duration of the videos included in Part 1 of the study was similar to videos from other studies evaluating orthodontic-related YouTube™ videos, ranging from 2 min 7 s to 35 min 22 s (Devanna et al., 2019; Grewal et al., 2019; Hunsaker et al., 2022). However, the videos included in this study had a larger range for number of views, likes and dislikes than some other studies (Devanna et al., 2019; Ustdal and Guney, 2020). A wide range of popular videos with active interaction among users were included in this study; therefore, these videos appear to be a good representation of the popular videos viewed by orthodontic patients.
Video 3 had the highest number of views and subscribers and the popularity of video 3 may be related to its unique presentation in music video format with attractive rap lyrics. This suggests that potentially new and attractive ways to present information for patient education could be considered in future videos.
Interestingly, all of the included videos were made by female orthodontic patients, which is consistent with the study by Guo et al. (2020) where 80% of the YouTube™ videos were uploaded by females. Gender differences have been found in the use of social media, in which females tend to use social media to maintain social relationships with friends and families, whereas males tend to use it for seeking technology-related information (Krasnova et al., 2017). Females have also been found to be more affected by social media than males when choosing their preferred dental practice (Alalawi et al., 2019). These findings could explain why the females in this study were more likely to share their treatment experiences via YouTube™ videos, because they relate more to ‘social media connections’.
Identification of themes in the included videos
There were six main themes identified. Theme 1 focused on problems with fixed appliances and highlighted that most of the presenters dealt well with these problems because they felt that the problems encountered were temporary in nature. These results are comparable with other studies in which orthodontic-related YouTube™ videos portrayed a generally positive attitude towards orthodontic treatment (Hunsaker et al., 2022; Livas et al., 2018).
Theme 2 related to the effects of fixed appliances and showed that although several presenters were concerned about dentofacial changes associated with fixed appliances, some were excited regarding how fixed appliance treatment had enhanced their self-confidence, reflecting the potential psychosocial impacts of orthodontic treatment. This is in agreement with the suggestion by Lew (1993) that improvements in dentofacial appearance and self-confidence are the main factors that encourage individuals to seek orthodontic treatment.
In Theme 3, relating to oral hygiene maintenance associated with fixed appliances, several presenters discussed the benefits of using water flossers to supplement conventional toothbrushing and flossing during fixed appliance treatment. A study by Sharma et al. (2008) suggested that water flossers as an adjunct may be beneficial in the short term in reducing plaque and gingival bleeding, and there is a possibility that this is due to a so-called ‘novelty effect’ (Shin et al., 2019). However, other studies that have investigated the efficacy of water flossers among orthodontic patients found that water flossers did not perform better than conventional toothbrushes (Mazzoleni et al., 2019; Tyler et al., 2023) or orthodontic-specific toothbrushes (Al Hariri et al., 2023). Therefore, the benefits of water flossers as adjunct are open to debate and may be short term.
Theme 4 focused on dietary advice associated with fixed appliances. The dietary advice provided in the videos was generally incomplete. For example, some videos discussed the importance of avoiding hard foods to prevent breakages, but without discussing the avoidance of food and drinks which could actually cause damage to the teeth (e.g. fizzy drinks and fruit juices). Although some videos encouraged a soft diet in the initial treatment stages, they did not describe that the soft diet was also beneficial after adjustment appointments. These findings imply that orthodontic patients generally have some knowledge in this area as it is related to their own experiences, although their knowledge may not be complete.
In Theme 5, presenters covered the treatment duration and appointment frequency during fixed appliance treatment, and the treatment duration experienced by the presenters showed marked variation. This variation may be related to a range of patient-related factors, such as different malocclusions, poor compliance and potential breakages (Skidmore et al., 2006).
Theme 6 focused on auxiliaries used with fixed appliances and some videos provided inaccurate or inappropriate advice related to, for example, unsupervised use of elastics in an attempt to accelerate orthodontic tooth movement.
Content accuracy of the included videos
The content accuracy was generally found to be low for both themes: oral hygiene maintenance and dietary advice associated with fixed appliances. Most of the items had low scores (score 1), indicating that most of the important information that should be routinely delivered to the patients by professionals were not covered in the included videos. Although it would not be feasible for patients to provide the same amount or accuracy of information as professionals, the low content accuracy is a concern especially for videos with high number of views and subscribers as their popularity could potentially disseminate incomplete and/or inaccurate content. Nevertheless, there were a small number of items which scored relatively better with scores of 3 or 4.
Interestingly, item 1Q (use of water flossers as adjunct) had relatively more scores of 4 (information present and accurate) when compared with other items. It is possible that the presenters in the videos were influenced by readily available water flosser posts in social media (Alshaer et al., 2022) or they may have had that advice provided by their orthodontist. The long-term benefit of water flossers as adjuncts in oral hygiene maintenance is debatable (Al Hariri et al., 2023; Tyler et al., 2023), although there is speculation that water flossers may achieve better patient compliance compared with manual flossing (Edlund et al., 2023).
The videos did not always provide accurate or complete information relating to oral hygiene maintenance and dietary advice associated with fixed appliances, and could therefore not be routinely recommended for peer-to-peer learning. Where information was provided, it was often inaccurate or incomplete, even accounting for the fact that patients would not be expected to provide information at the same level of accuracy or completeness as professionals. This finding was comparable with findings of other studies where a significant proportion of the YouTube™ videos on lingual orthodontics (Lena and Dindaroglŭ, 2018) and orthognathic surgery (Hegarty et al., 2017) had low quality content.
Limitations
The video search was conducted between 18 August and 30 August 2020; however, YouTube™ videos are constantly updated, with more than 500 hours’ worth of new video content per minute (Mahajan, 2024), and this potentially results in a discrepancy between the data collected at one time point and new data uploaded. The search filter was not optimised to exclude any video with advertisement or sponsored posts, which may introduce bias in the results; however, commercial videos were manually excluded during the video screening process.
Generalisability
Only English language videos were included in this study and this may restrict the generalisability of the results. However, the included videos were developed internationally even though the video search location setting was programmed to the United Kingdom, suggesting that these videos sharing treatment experiences cover a wide spectrum of cultural backgrounds.
Interpretation
This study does have implications for clinical practice; YouTube™ videos are clearly deemed important from the patients’ perspective, albeit a significant amount of the information provided in the videos is incomplete or lacks accuracy. Nonetheless, our patients’ perspectives are invaluable, and patients are potentially extremely helpful in providing information on YouTube™. Therefore, one of the recommendations from this study would be that clinicians and organisations collaborate with patients to produce educational videos that are patient-centred and contain appropriate and accurate information, to ensure truly useful and effective information provision to patients.
Conclusions
The main findings of this study were:
From the included videos, six main themes were identified: problems with fixed appliances; effects of fixed appliances; oral hygiene maintenance associated with fixed appliances; dietary advice associated with fixed appliances; treatment duration and appointment frequency during fixed appliance treatment; and auxiliaries used with fixed appliances.
When assessing the included videos against a checklist derived from professional orthodontic resources, the accuracy and completeness of the video content relating to oral hygiene maintenance and dietary advice associated with fixed appliances was low.
It is therefore recommended that clinicians collaborate with patients to produce videos that are patient-centred but also contain appropriate and accurate information, to ensure effective information is delivered.
Supplemental Material
sj-docx-1-joo-10.1177_14653125241264827 – Supplemental material for Orthodontic YouTube™ videos made by patients for patients: What are they about and are they accurate?
Supplemental material, sj-docx-1-joo-10.1177_14653125241264827 for Orthodontic YouTube™ videos made by patients for patients: What are they about and are they accurate? by Iris EJ Liew, Mohammad Owaise Sharif and Susan J Cunningham in Journal of Orthodontics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.