
Abstract
• Summary: This article uses the concept of citizenship to explore the recent mental health statutes within England and Wales and within Scotland. It argues that differences in the content, and practice context, herald a parting of the ways in mental health social work in the United Kingdom.
• Findings: The author focuses on three key differences: the reciprocity principle, the grounds for compulsory treatment and the place of social work within compulsory intervention to demonstrate how the statutes have led to more limited legal, procedural and social rights in England and Wales than in Scotland. The result for social work is that the practice context created in England and Wales may become more risk averse and that social work services may have a more residual role within statutory mental health work. The differences described in this article may also reflect increasing post-devolution divergence in the provision of social work services across the four countries that make up the United Kingdom.
• Applications: Further research is needed to explore if these divergences, within mental health law and policy, are in practice supporting or limiting citizenship.
Introduction
This article argues that the Mental Health (Care and Treatment) (Scotland) Act 2003 (MHSA03) and the Mental Health Act 2007 (MHA07) represent a significant parting of the ways in terms of mental health social work within the United Kingdom. Scotland is viewed as having taken a rights-based approach (Northern Ireland Assembly, 2008). In comparison, the MHA07 seems to have adopted a safety-first approach with fewer safeguards for the person subject to compulsory intervention (Pilgrim, 2007). There are many differences between the two statutes and this article will discuss the following three in depth: the principle of reciprocity; the grounds for compulsory treatment; and the place of social work in compulsory intervention. The concept of citizenship will be employed to argue that whilst the legal rights clearly vary, there is also an impact on the social and procedural rights of people defined as having a ‘mental disorder’: the legal term within both statutes. The result for social work is that the practice context created in England and Wales may become more risk averse and that social work services may have a more residual role within statutory mental health work.
This type of variance, in law and practice, is not uncommon across wider Europe because countries have developed at different paces and under different influences (Prior, 2007). What is uncommon is that this variance is now within the UK, where countries had followed a similar pattern of reform in mental health law and policies for the previous 50 years. Additionally, Wales and England developed their own Codes of Practice on the MHA07 (Department of Health, 2008; Welsh Assembly, 2008a) and these have resulted in other variations such as a different list of principles (Barber, Brown, & Martin, 2009). However, this article will concentrate on the key differences between the statutes and is therefore a comparison between the bills passed by the Westminster and Scottish Parliaments.
The article first introduces the concept of citizenship as a lens with which to view the changes for mental health social work. Second, the article briefly discusses the development of the social work role alongside mental health services prior to these new statutes. Third, it sets the wider context of devolved government and the political perspectives that led to different climates of change. Fourth, the emerging practice contexts will be considered with reference to the statutes’ stated principles and their grounds for compulsory treatment. Finally, the resulting changes for the role of social work services will be discussed in relation to independence and accountability.
Citizenship
The concept of citizenship has been central to the disability movement (Oliver, 1996), and has started to be used by mental health organizations, and within literature (Barnes & Bowl, 2001; Sayce, 2000), to demonstrate the way in which groups of people continue to be excluded from mainstream society. Marshall (1950) is credited with re-introducing the notion of citizenship and making it relevant to modern welfare states. There are three domains of citizenship rights: civil, political and social. First, civil, or legal rights, describe how the state might protect privacy and liberty such as ensuring the right to a fair trial. Second, political rights allow participation in the decision-making of the country by the right to vote, to peaceful protest and to organize into trade unions or pressure groups. Social rights, as envisaged by Marshall, underpinned the state’s collective responsibility for the welfare of all citizens and he saw social services as being pivotal to this (Harris, 1999). As such, social rights ‘help to define the extent and quality of a citizen’s substantive welfare entitlements and are also the focus of wider welfare debates and struggles’ (Dwyer, 2004, p. 6). Such struggles and debates are many. For example, how much should the state provide for people’s welfare and how much are individuals responsible for looking after themselves? Also, to what extent should perceived socially unacceptable behaviour be tackled by use of the law?
Citizenship is therefore a fluid and contested concept that changes through time and by political ideology as demonstrated by the current and previous UK-wide governments (Dwyer, 2004; Lister, 2003). The Conservative government (1979–1997), with its neo-liberal ideology, developed a much narrower view of citizenship that socially excluded many in society (Harris, 1999). It created a version of individualized citizenship around consumerism and choice, alongside the rolling back of the state and the introduction of the market and managerialism into health and social care services (Harris, 1999; Rummery, 2002). It was a conditional status based on responsibilities, as well as rights, to contribute to and comply with the government’s expectations of employment and social behaviour, with a more limited safety net for those who could not work. This model of citizenship supported negative civil and legal rights and weakened positive social rights (Dwyer, 2004; Rummery, 2002).
The Labour UK-wide government (1997–2010) distanced itself from this individualized approach and talked more of mutual responsibility though ‘the principle of conditionality [was] also being applied in an increasingly wide range of UK welfare policy areas, including education and health’ (Dwyer, 2004, p. 74). Part of this conditionality was that groups in society such as people defined as having a mental disorder, young people involved in anti-social behaviour, or asylum seekers, were facing increasing direct intervention to reduce their perceived harmful impact on the public. In so doing the government was feeding as well as responding to public concerns about harm and safety (McLaughlin, 2008).
This reduction in social rights has led academics to consider the idea of procedural rights for people who use public services (Harris, 1999; Rummery, 2002). These are the right to request an assessment, to have a worker who correctly follows policy and to redress where services fall below the standard expected. They are viewed as perhaps more claimable than social rights ‘because it is unlikely that there could be a substantive right to receive a particular form and amount of state social work services in the light of uncertainty over resources’ (Harris, 1999, p. 930). Rummery (2002) explored how community care workers undertook their work, with physically disabled people, in a way that constrained the procedural rights of those referred, by rationing information as well as services (Rummery, 2002). People who use public services may already have limited citizenship due to the situation in which they live; actions, such as these by front-line workers, further disempower them. Whilst budgets and procedures might limit the scope of services, it is incumbent upon workers to support service users to claim their rights and to address procedural injustice (Evans & Harris, 2004).
Some people will need more support to claim their citizenship rights than others due to health, disability or personal circumstances. This is highlighted by the distinction drawn between being a citizen and acting as a citizen. ‘To act as a citizen involves fulfilling the full potential of the status. Those who do not fulfil that potential do not cease to be citizens’ (Lister, 1998, p. 28). This has particular relevance for people defined as having a mental disorder because they may be temporarily, or permanently, unable to act fully as citizens and therefore workers will be responsible for promoting citizenship on their behalf.
Mental health social work
Social work developed alongside the National Health Service (NHS) in the move from institutional to community based care in the second half of the 20th century. Large psychiatric and learning disability hospitals gave way to small in-patient units and increased out-patient services such as day hospitals (Rogers & Pilgrim, 1996). Social workers had been based within these institutions long before the creation of social work departments by the respective statutes within the UK in the 1960s (Sheldon & Macdonald, 2009). The establishment of social work departments formalized their place within the welfare state, albeit younger and less socially acceptable than the NHS, and gave them a clear mandate to support wider social rights (Harris, 1999).
The social work role was to offer advice, support and counselling on a range of personal and practical matters to those in hospital and to support their return into the community. They were, until the 1980s, the only mental health professionals, except psychiatrists, who worked across the boundary between hospital and home; providing an important link between patients, their families, communities and wider welfare systems.
The social worker’s distinct role in hospital detention was established by the Mental Health Act 1959 and the Mental Health (Scotland) Act 1960, and confirmed in the respective mental health statutes of the 1980s, through the creation of Approved Social Workers (ASW) in England, Northern Ireland and Wales, and Approved Mental Health Officers (MHO) in Scotland (Rogers & Pilgrim, 1996; Sheldon & Macdonald, 2009). The ASW/MHO role was to act as a check and balance to the medical power and standpoint of the doctors in compulsory detention procedures (Pritchard, 2006). Social workers were seen as having a socially orientated perspective of mental health, familiarity with legal frameworks and knowledge about community resources that might be used to avoid hospitalization or reduce its length. Their legal tasks were to give or refuse consent to emergency and short-term detention orders, apply for long-term orders, prepare social circumstances reports and participate in reviews. Their wider support role continued and there was evidence from research that this had better long-term outcomes for service users than the intervention of nurses in the community (Shepherd, 1990, cited in Rogers & Pilgrim, 1996).
The next phase in the development of mental health social work, from the late 1980s onwards, had two particular characteristics: the creation of inter-professional community mental health teams (CMHTs), and the introduction of community care reforms under the NHS and Community Care Act 1990. CMHTs arose due to the recognition that a range of professions should be working together to support people in their own communities (Onyett, 2003). It was thought also that formally organized teams would improve communication, response times to referrals and support offered by professionals with a complementary range of skills and knowledge (Ovretveit, 1993). The ways in which social workers linked into these teams varied, from full-time placement to attendance at team meetings only, though they continued to be employed and managed by the local authority.
The NHS and Community Care Act 1990 introduced the purchaser–provider split into what was seen as inefficient state-run services by the then Conservative government, which, as noted above, was influenced by neo-liberal ideology and its principles of marketization and managerialism (Means, Richards, & Smith, 2008). The role of the social worker for all adult care services started to be defined as one of care manager, open to other professionals within local authorities, with a focus on assessment and the brokering of services from independent providers that were stimulated by the wider community care reforms (Lewis & Glennerster, 1996).
Social work’s traditional role of supporting and networking with wider agencies could potentially be brokered from the independent sector or carried out by other professions. These developments have led some commentators to state ‘mental health social work’ is now a rarely used term in the inter-professional community care context of today (Wilson, Ruch, Lymbery, & Cooper et al., 2009). However, such comments overlook the differences within the UK that this article highlights and to which it now turns.
Climates of change
On the surface the reasons for the reviews of mental health law were the same: the outdated focus on hospital as the site of treatment, limited rights for patients and the need to make the legislation more compatible with the Human Rights Act 1998. Yet the announcements of the reviews of mental health law in 1998 by the respective ministers for health struck very different tones. In Scotland, Sam Galbraith spoke of the need to modernize the law to reflect the fact that most people with mental distress lived successfully in the community but that when there was a need to intervene there should be improved safeguards for the individuals involved (Scottish Executive, 1998). On the other hand, Frank Dobson’s press release began with the view that community care had failed to offer the required protection to society (Department of Health, 1998). Whilst he also went on to talk of modernization, the real priority was clear: the government wanted more control over those deemed as a risk to society (Pilgrim, 2007).
The respective review processes similarly demonstrated that the Westminster government was focused on the outcome rather than the process of the review. It established an Expert Committee that was given 10 months to do its work; severely limiting its ability to consult widely (Department of Health, 1999). In contrast, Scotland established a Commission, which was given twice that length of time. It undertook full consultation exercises and commissioned research to assist its work (Scottish Executive, 2001). A comparison between the review reports demonstrates they made similar recommendations. Whilst the Scottish Parliament adopted the recommendations, the Westminster government did not and its large majority in Parliament allowed it to pursue its safety-first agenda.
Whilst some service user groups were unhappy with the proposal of community based treatment orders, they supported the proposal for improved rights and processes and the bill had a relatively smooth passage through the Scottish Parliament in 2003 (Pilgrim, 2007). The Westminster government took a further four years before legislation was finally passed. The first bill adopted those recommendations that supported the government’s desire to more easily detain people and disregarded those that significantly increased rights for people who may become subject to the statute. This raised so much concern that an alliance of organizations was formed to oppose the bill, there was also dissent within the Labour Party and objections across both Houses of Parliament. The protracted and ultimately doomed passage of this first bill has been well documented elsewhere (Fennell, 2007; Pilgrim, 2007). In 2006 the government withdrew it and proceeded to amend the existing statute, the Mental Health Act 1983, with comparatively less opposition.
Practice contexts
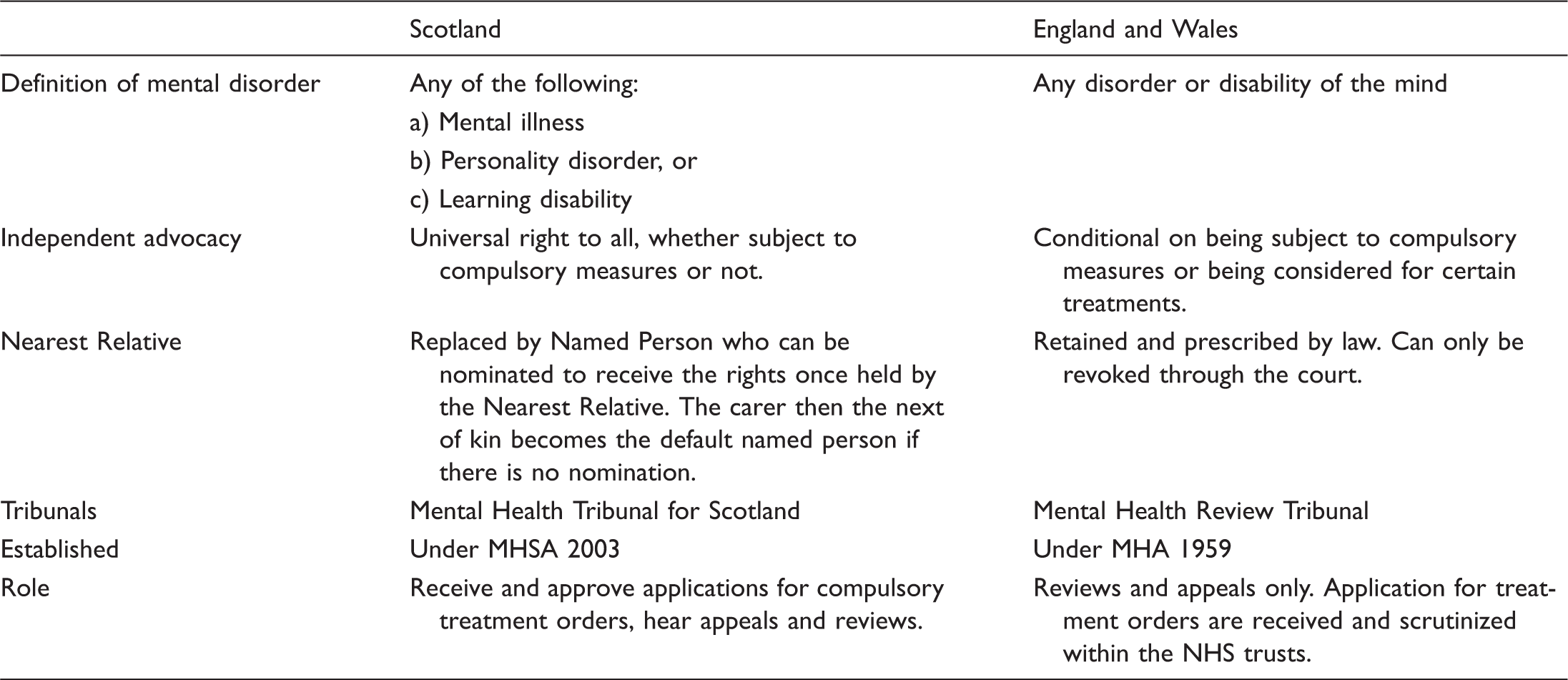
Other key differences between the MHSA 2003 and the MHA2007
Principle of reciprocity
The statement of principles within any statute is intended to be a guide for professionals as to how its measures should be implemented. The principles are listed at the beginning of the MHSA03, whereas the MHA07 leaves the principles to the respective national Codes of Practice (Department of Health, 2008; Welsh Assembly, 2008a). The result is that the values that underpin the context in England and Wales will be ‘a statement of principles which the Secretary of State thinks should ‘‘inform decisions under this Act’’’ (Fennell, 2007, p. 36). This leaves the principles more open to interpretation and review, without recourse to the elected chambers of Westminster where any changes in law have to be considered.
Reciprocity is recorded in Section 6 of the MHSA03 as having ‘regard to the importance of the provision of appropriate services to the person who is, or has been, subject to the certificate or order concerned’. It can be seen as re-creating a wider definition of social rights for people defined as having a mental disorder in Scotland. It acknowledges of some of the negative effects for people of hospitalization and engagement with mental health services in terms of social exclusion (Rogers & Pilgrim, 2003; Tew, 2005). Also, it fits well with social work’s stated commitment to social justice, as it appears within the British Association for Social Workers (2002) Code of Ethics: a responsibility to address and counter the effects of structural discrimination and disadvantage on service users.
Reciprocity can also be seen as promoting the ‘recovery’ approach developed by mental service users to support each other (Wallcraft, 2005). It is a positive approach which sees mental well-being differently to the medical model. Well-being does not necessarily mean being symptom-free: each person will develop his or her own definition of what that means and how he or she might be assisted to achieve it. The principle of reciprocity therefore underlines the need to work with people to facilitate their recovery, through understanding their perspectives and the kind of approaches they find helpful. Whilst resources will always be finite, reciprocity speaks also of the values, perspectives and skills of workers in supporting a person’s recovery on a long-term basis.
However, to what extent is the principle enforceable? The fact that it is incorporated within the statute, rather than the Code of Practice, means that professionals and agencies can more clearly be held to account for their in/action and the services they may or may not provide. The Mental Health Tribunal in Scotland (MHTS), the legal decision-making forum for compulsory treatment orders (CTOs), can make the provision of a service a recorded matter: a requirement written into an order when it is granted (Scottish Executive, 2005). This could be a referral for a specialized type of counselling, provision of supported accommodation or facilitating contact with children or other family. Failure to meet a recorded matter can be grounds for requesting a MHTS review of the order. They are also subject to inquiry when the Mental Welfare Commission for Scotland, who have responsibility to monitor the care of all people defined as having a mental disorder, visit those subject to CTOs (Mental Welfare Commission, 2008).
The grounds for compulsory treatment
The MHA07 has two, and the MHSA03 three, tests to establish the grounds for compulsory treatment whether in hospital or in the community. Both require existence of a mental disorder and evidence that the person is placing themselves and or others at risk. The MHSA03’s extra test requires assessment of the person’s ability to make informed decisions: ‘that because of the mental disorder the patient’s ability to make decisions about the provision of such medical treatment is significantly impaired’ (Section (5) (d)). This provides an additional legal safeguard from the excessive paternalism that was apparent under the previous statute (Campbell & Heginbotham, 1991).
The Westminster government rejected a similar proposal because of its concern that there may be people whose decision-making was not impaired but who were none the less deemed dangerous. Their ‘agenda is to remove all obstacles, principled or not, to mental health detention of people with personality disorder where there is risk, so it is little surprise that the significantly impaired judgment test has been rejected’ (Fennell, 2007, p. 48). The principled obstacle, referred to by Fennell, is based on the growing acceptance that mental disorder of its own does not equate with irrationality (Bean, 2001; Campbell & Heginbotham, 1991; Szmukler & Appelbaum, 2001). It follows therefore that people defined as having a mental disorder should be free to make what other people may view as poor decisions, as well as preferred ones, unless their decision-making is significantly impaired.
Impaired decision-making is not the same as capacity to make decisions, and the latter is subject to different legislation in England and Wales (The Mental Capacity Act 2005) than in Scotland (The Adults with Incapacity (Scotland) Act 2000). Incapacity is deemed to be long-term and the result of cognitive impairment in the person. However, impaired decision-making takes account of wider factors such as how the person’s emotional state might influence judgments at that particular time (Patrick, 2006).
There are other aspects to the respective grounds of compulsion that support the argument that Scotland has much stricter criteria for imposing compulsory treatment. First, whilst both statutes have a clause regarding the necessity of compulsion for the health and safety of the person or others, the levels of risk and evidence are different. The MHSA03 requires the same level of risk for short-term orders as well as for long-term orders: the focus is on significant risk to the health, safety or welfare of the patient or to the safety of any other person. The MHA07 allows a short-term order in the interests of health or safety or with a view to the protection of others. Second, the MHA07 removed the exclusion of the sexual deviancy clause which means that sex offenders who have mental disorders, whether or not it is connected to their criminal activity, can now be held under mental health law (Fennell, 2007).
In conclusion, the sum total of these changes may well be greater than the individual parts in creating a context, in England and Wales, of more limited citizenship for people defined as having a mental disorder. The Westminster government has created broader grounds for compulsory treatment, in line with its safety-first approach, and accorded fewer protective rights to those subject to it. The cumulative effect is that some previously acceptable risks may become seen as unacceptable; with people being hospitalized, or subject to community based treatment, more easily and more often than in Scotland. Yet there should not be complacency in Scotland: the number of new orders in Scotland has declined since the MHSA03 but the overall number of ongoing orders is slowly increasing and the reasons for this require investigation (Mental Welfare Commission, 2008). However, without the principle of reciprocity, social work has less of a mandate to provide wider services whether or not people are subject to compulsory intervention.
The social work role
The above section demonstrates that social work services, in England and Wales, when compared with those in Scotland, are being required to work within a narrower set of legal rights for those deemed to have a mental disorder, and may find their resources increasingly funnelled towards the policing aspect of mental health work (McLaughlin, 2008). Also changes to the ASW service may mean they will be less able than before to, first, guarantee independent decision-making (Fennell, 2007) and, second, provide accountability (Rapaport & Manthorpe, 2008). This may result in procedural rights, already more limited, being further eroded. The key differences are, first, that the MHSA03 continued to ring fence the role of mental health officer (MHO) for social workers only, whereas the MHA07 replaced the approved social worker with approved mental health professional (AMHP), who can be a nurse, psychologist, occupational therapist or social worker. Second, professionals do not have to be employed by the local authority in order to become an AMHP.
Both reviews considered whether the MHO/ASW role, of being a check and balance in compulsory intervention processes, should remain the preserve of social workers. Scotland’s decision was based on the view that social work was ‘currently the only profession to combine independence from health with training and experience of working within a statutory framework’ (Scottish Executive, 2001, p. 89). The Expert Committee for England and Wales was less equivocal about social workers’ unique knowledge and skills yet recommended that the role should probably remain with ASWs in the short term.
The argument about whether other allied mental health professionals could fulfil the role was not a new one and exemplified the professional rivalry that had existed for some time (Rogers & Pilgrim, 1996). One might argue that since the last review of mental health law in the 1980s mental health professionals, particularly community psychiatric nurses, undertake similar work (Wilson et al., 2009) so they also have the skills and knowledge to perform this statutory role. However, the Westminster government did not create the AMHP role to promote inter-professional equality. It has been argued that the real motivation was to get as many professionals as possible on board with the task of detaining those who were seen to pose a risk to society. This standpoint is supported by the parallel changes to the role of responsible medical officer, previously reserved for psychiatrists or doctors who have worked in the specialty for four years, to that of clinical supervisor who can be drawn from a wider range of mental health professionals. Pilgrim (2007, p. 86), referring to this latter change, argued the government imperative was ‘if medicine could not be trusted to embrace new expectations of devolved powers of social control, then other professions could be recruited, some of them maybe even willingly’.
Whilst there were difficulties recruiting enough ASWs in some parts of the country (Rapaport & Manthorpe, 2008) this could have been addressed by acknowledging and tackling the wider problems of staff vacancies and recruitment within social services. Such a decision is also indicative of the Westminster government’s managerialist agenda to prescribe the tasks its public servants undertake, to the detriment of professionals’ roles and expertise (Banks, 2004). However, these changes might also lead to a greater appreciation of the work of the different professions, each hopefully supporting the others to adopt best practice; challenging each others’ perceptions of mental disorder, risk and the merits of using the statute in any given situation.
At present most AMHPs are the old ASWs and we have yet to see how many other professionals volunteer for the new role. Questions remain about how professional training, experience and the location of employment will influence workers’ perspectives. For example, a nurse who has always worked on hospital wards may be less aware of community resources and of how risk may be managed without recourse to hospitalization. Also, how will staff be able to switch between their substantive role, where a psychiatrist is, relatively speaking, more powerful in the NHS hierarchy, to the AMHP role of independent decision-making (Fennell, 2007)? This is not to say that all ASWs/MHOs were good at making autonomous decisions and being prepared to take a stance against pressure being asserted by other workers (Pritchard, 2006). However, the degree of independence afforded by being a local authority employee was a buffer against such pressure, and will not be there for NHS staff who become AMHPs. With this in mind, the Codes of Practice, for England and for Wales, recommend that members of the same NHS team should only be involved together in considering the use of compulsory interventions under exceptional circumstances (Department of Health, 2008; Welsh Assembly, 2008a). They also state that there should be procedures to support those in the employ of the NHS who feel under pressure to comply with doctors.
This leads to wider questions of accountability at agency level to ensure systems and individual practice support a person’s legal and procedural rights. In Scotland the local authority retains responsibility for training, appointing and overseeing MHOs. English and Welsh local authorities only appoint an AMHP and this has led Rapaport and Manthorpe (2008) to ask how local authorities can be fully accountable for the AMHP service. It is unclear how local authorities will address those aspects of providing a statutory service that usually need a degree of employer influence, for example, ensuring compliance with the above guidance and staffing rotas to ensure AMHP coverage of an area. As a result the local authorities, in England and Wales, are in a weaker position when trying to ensure that the AMHP supports rather than constrains procedural rights. It may quantitatively meet its quota of AMHPs but it will have less influence over the quality of the service as a whole.
Concluding comments
It was always envisioned that Scotland, England, Northern Ireland and Wales might diverge further in terms of law and policy after devolution in the late 1990s. However, the bulk of social work literature still tends to present the UK, to the wider world, as more or less uniform and this position is no longer tenable. In mental health social work, there are significant variances in both the context and the role of social work services and individual social workers. The differences are best summed up as Scotland taking a rights-based, compared to England’s safety-first, approach; not only in the statutes themselves but in the role they see for social workers. The creation of the AMHP signifies a more residual role for social work services as a whole in England and Wales. Whilst they have been given continued responsibility for the AMHP service, they may have less influence in overseeing it and upon individual practice. Alongside this Scotland has also advanced social rights due to its principle of reciprocity. It gives continued credence to the traditional role of social work in supporting the welfare of people defined as having a mental disorder.
Further variances will occur within mental health law and social work in the UK. Wales is seeking more devolved statutory powers in relation to mental health (Welsh Assembly, 2008b). It is proposing a duty to assess and consider the provision of care, similar to the reciprocity principle, and to make advocacy a universal service rather than conditional upon the person being subject to compulsory intervention.
Northern Ireland is benefiting from being last to modernize their mental health law. It has consulted on the recommendations of the Bamford Review of Mental Health and Learning Disability (Northern Ireland Executive, 2008), and it is looking more to the rights-based approach of Scotland (Northern Ireland Assembly, 2008). As a result social workers and social work services in England may find themselves with a legal framework that is least supportive of citizenship rights for people defined as having a mental disorder. However, it remains to be seen whether it will, also, dilute the wider contribution of social work to mental health services. It is also possible that these legislative changes may galvanize social workers and other mental health professionals to support citizenship rights as fully as possible to counter the safety-first approach that underpins the statute.
The current UK situation presents opportunities as well as concerns. It can potentially become a hub of research and debate around citizenship rights, for people defined as having a mental disorder, within social work and across different professions. The most important question of all is whether people subject to compulsion under the different mental health statutes have qualitatively different experiences. If so are the variables the law itself, professional practice or wider factors such, as personal circumstances and the availability of support services? How are MHO/AMHPs making decisions under the new statutes? How are they supporting people to express their views? How are MHO/AMHPs being informed and supported about best practice? How are local authorities addressing their accountability for an AMHP service? Social work on its own, and in partnership with other professions and service user groups, should start to answer these questions now. It should not wait to respond defensively the next time there are calls for changes within mental health law and services.
Statutes
Mental Health Act 1959
Mental Health (Scotland) Act 1960
Mental Health Act 1983
Mental Health (Scotland) Act 1984
NHS and Community Care Act 1990
Human Rights Act 1998
Adults with Incapacity (Scotland) Act 2000
Mental Health (Care and Treatment) (Scotland) Act 2003
Mental Capacity Act 2005
Mental Health Act 2007