
Abstract
Summary
Former inmates encounter a variety of challenges when returning to their community, including poor health status and limited access to healthcare services. This qualitative study examined how former male inmates with chronic conditions perceived, understood, managed, and coped with their illnesses.
Findings
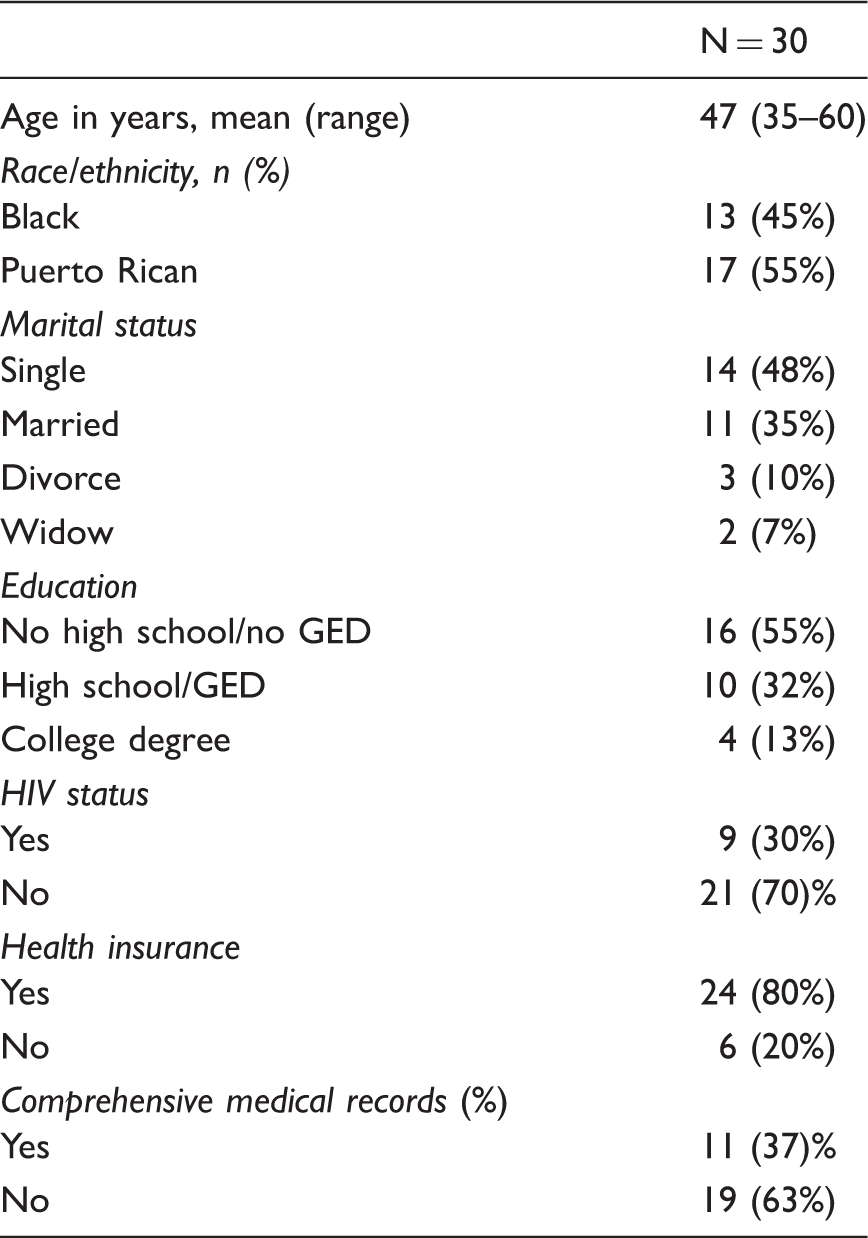
The participants were Black and Puerto Rican, with a mean age of 47 years, who were interviewed within three years of their release. Participants reported at least one chronic condition, with 21 HIV-negative men using chaos narratives to depict their approach to disease management. Nine HIV-positive men used quest narratives to present their illnesses and were immediately linked to supportive services, enabling them to overcome the barriers to community reintegration.
Applications
Health interventions in the area of forensic social work ought to focus on conducting Medicaid outreach and enrollment efforts prior to correctional facility discharge.
Introduction
The United States criminal justice system is undergoing a demographic change in its inmate population, resulting in a rapid increase in the number of older individuals released from its prisons and jails (Aday, 2003; Lemieus, Dyeson, & Castiglione, 2002; Neeley, 1997; Williams, Goodwin, Baillargeon, Ahalt, & Walter, 2012). The term “older” has a different meaning in the criminal justice system than it does in general society. The National Institute of Corrections (NIC) defines older inmates as between the ages of 50 and 55 (Chiu, 2010), since those behind bars are thought to age 10 to 15 years more quickly than the typical individual (Duckett, Fox, Harsha, & Vish, 2010; Williams et al., 2010). This accelerated aging process has been attributed to the chronic and communicable diseases common among inmates, the majority of whom have engaged in high-risk behaviors and unhealthy lifestyles (Aday, 2003; Harrison & Beck, 2006). For instance, prison and jail inmates’ histories of substance use, particularly intravenous drug use, elevate their risk for contracting the hepatitis A virus—associated liver disease (Aday, 2003; Harrison & Beck, 2006). Older men in the criminal justice system are also disproportionately affected by viral infections such as hepatitis C (HCV) and human immunodeficiency virus (HIV). HIV prevalence among inmates is five times that of the general population (Okie, 2007). Older former inmates have higher rates of health problems compared to their younger counterparts, and many suffer from multiple chronic conditions (Loeb & Abudagga, 2006; Maruschak, 2004; National Commission on Correctional Health Care, 2002).
Along with high-risk behaviors, there are a number of other factors that contribute to the poor health status and inadequate health behaviors of the criminal justice population. These individuals often receive substandard medical care prior to, during, and after incarceration (Suhrcke, Rachel, Nugent, Struckler, & Rocco, 2006; Visher & Mallki-Kane, 2007). Once released to their communities, former inmates may have limited access to healthcare services and fail to continue treatments that were initiated during their incarceration (Golembeski & Fullilove, 2005). Many members of this population lack knowledge about applying for health insurance and seeking healthcare referrals, while some distrust and avoid healthcare providers altogether (Binswanger, Nowels, Corsi, Long, & Booth, 2011; Morrissey, Cuddeback, Cuellar, & Steadman, 2007). Multiple social and psychological problems, limited access to programs and entitlements, unemployment, and social stigma may play a role in hindering this population’s use of healthcare services (Binswanger et al., 2011; Golembeski & Fullilove, 2005; Morrissey et al., 2007; Petersilla, 2003; Visher & Mallki-Kane, 2007). Furthermore, former inmates often return to marginalized communities that create or exacerbate a host of concerns for these individuals (Adams, Nowels, Corsi, & Long, 2011; Binswanger et al., 2011; Olphen, Freudenberg, Fortin, & Galea, 2006; Freudenberg, Daniels, Crum, Perkins, & Richie, 2005).
The increase in individuals reintegrating into society after incarceration is creating a unique healthcare challenge for the nation. However, we know little about the health-related experiences of this population, especially among former inmates with chronic conditions. To address this information deficit, we designed this study, held in Bronx, New York, to examine the factors that impact the physical health of former inmates. Our study objectives were (1) to explore the health behaviors of recently released men and (2) to understand the barriers to community reintegration among former inmates with multiple chronic conditions using Frank’s (1995) typology of chaos or quest narratives.
Method
Study setting
Bronx, New York is one of the poorest counties in New York City; over half of its residents receive public assistance (New York City Department of Health, 2012). The Bronx’s 2012 violent crime index is among the highest in New York State (University of Wisconsin Population Health Institute, 2012), and the county has below average educational attainment and labor force participation, with an unemployment rate of 13.9% (New York State Department of Labor, 2012). The county suffers from a disproportionate incidence of multiple chronic health conditions (New York City Department of Health, 2012). Individuals returning from prisons and jails to the Bronx face numerous hurdles to successful reentry, including addiction, joblessness, unstable housing, and poor mental and physical health (Mellow et al., 2008).
Study participants
Recruitment took place over a three-month period between March 2011 and May 2011. Using a venue-based sampling approach (Muhib, Lin, Stueve, Miller, & Ford, 2011), men were primarily recruited via fliers placed in the criminal court, parole, and probation offices, addiction treatment centers, and reentry agencies in Bronx, New York. Participants underwent an informed consent process and completed semi-structured interviews with a trained interviewer. Each interview was conducted in a private meeting space and was digitally recorded. We interviewed 30 racial and ethnic minority men released from state prison or a local jail. The eligibility criteria were (1) male; (2) ages 35–65 years old; (3) reside in the Bronx; (4) report prior criminal justice status within the past five years; (5) report no previous diagnosis of cancer or other chronic disease that requires intense or on-going care; (6) report substance abuse history; (7) provide informed consent; and (8) agree to the interview being audio-taped.
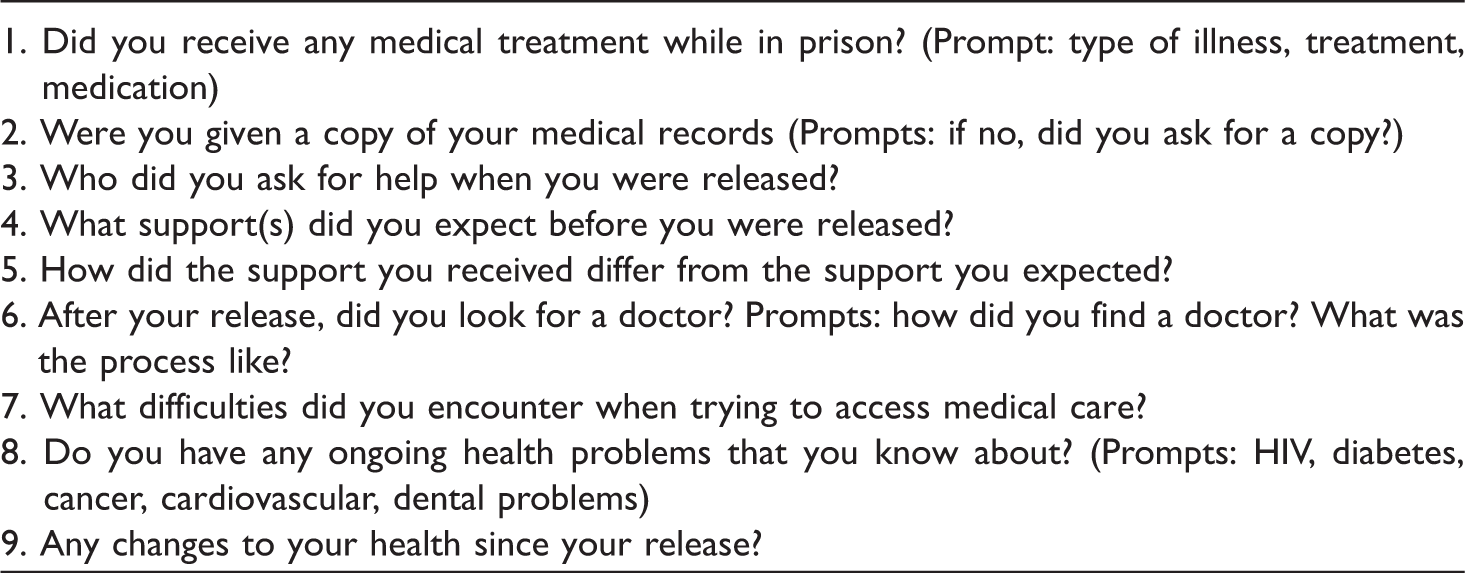
Examples of semi-structured interview questions.
Digital recordings were transcribed by a professional transcriptionist, uploaded in a secure drive, and entered into NVivo qualitative data analysis software (QSR, 2011). Study authors coded transcripts and met bi-weekly from August 2011 through January 2012 to deliberate upon coding differences and to develop the final codebook. This document included the code itself, a definition of the code, a quotation illustrating the code, and guidelines for its proper use (Coffey & Atkinson, 1996; Strauss & Corbin, 1990).
Data analysis
We used a narrative method approach to investigate the data, examining how former male inmates with chronic illnesses perceived, understood, managed, and coped with their physical symptoms (Hall, 2011; Kleinman, 1988). Each narrative was analyzed individually and classified into Frank’s (1995) typology: chaos or quest. According to Frank (1995), chaos narratives reveal vulnerability because the individual is often overwhelmed by his or her chronic illness or disability and may find it difficult to speak about the illness in a coherent fashion. Events are told as he experiences them, often disjointed, and temporal without closure. On the other hand, individuals providing quest narratives have learned to accept their illnesses or disabilities and often suggest that there is something to be gained from the experience. Quest narratives are about healing, searching for alternative ways of coping with the illness, and finding a sense of purpose (Frank, 1995).
Results
Participant characteristics.
Using a narrative analysis framework, we examined how former male inmates with multiple chronic conditions experienced community reentry in Bronx County. Over the course of their interviews, nine of the participants—all of whom were HIV-positive—shifted to quest narratives when describing their current circumstances. These men appeared to accept their chronic condition and sought to employ the knowledge gained from challenging experiences to help others. In contrast, 21 participants—all of whom were HIV-negative—continued to speak about living in chaos, describing perpetual states of vulnerability and distress.
Chaotic narratives of HIV negative participants
The 21 men who described their lives with chaos narratives were overwhelmed by their health conditions and the competing demands they faced post-release. Most of them returned to chaotic neighborhoods where they were surrounded by drug use, violence, and poverty. Sixteen had difficulty resuming family ties, and others pointed to housing instability as causing their relapse into substance use. These participants depicted their illness symptoms as intolerable and distressing and described desperate coping behaviors. For instance, a 46-year-old Puerto Rican male with substance abuse addiction and HCV released for three years noted: I got on suboxone, because I was doing percocets and vicodins. And buying them in the streets; it wasn’t even prescribed. And I got hooked on them. I really got hooked on them. When you’re hooked on those percocets and vicodins, you can’t function right, once you get addicted to them. (ID: 17) I been dipping and dabbing, not letting the program know. I was more or less like getting urine from other people so they wouldn’t know ‘because they were taking my urine, every week. (ID: 11) I’m diabetic, so I had to make sure that I stayed on top of my blood sugar, and my medications … as long as I take it in the time, timely fashion, it’s usually pretty good. I can tell my blood sugar is acting up because I’ll start urinating frequently, the only problem is, where I’m located. And, everything that you eat and you have to cook is in the microwave. (ID: 26) I suffer from a mental illness. I see a psychiatrist and a therapist now. I take seroquel, wellbutrin, and some other medication, for that part, chronic depression and suicidal intentions, plus I have arthritis, I have glaucoma. I am supposed to get 2 knee replacements, because my knees are no good. It’s like I’m falling apart. Teeth are falling out. Everything is falling apart now. (ID: 27) My other 3 children, I watched ‘em grow up. And the last 2, I’ve been away more than I’ve been in their life. And I don’t see my daughter as much as I should. She’s in foster care. I lost my son through adoption. She got molested by some boys. And, I don’t even know what happened with the kids. I don’t know if they went to jail or not. I wish I was there so I could a helped her, what kills me is my daughter was waiting for me and I never made it there. (ID: 27) I came home to a sick mother that was in the hospital. She was in intensive care, so, the first couple a months, I was, trying to help nurse her back to health. (ID: 30) Interviewer: Have you had your blood pressure checked? Interviewee: I haven’t had my blood pressure checked in a long time. But, I know it’s high because I get migraines … My health is not important to me. I live day by day. So I don’t really think about the medical part of it. I really don’t think about seeing a medical doctor. (ID: 05)
Quest narratives of HIV positive participants
Nine men living with HIV described their lives using quest narratives, despite the numerous challenges they faced, including the detrimental effects of their physical symptoms. These individuals even appreciated what the disease had brought to their lives and were hopeful about their future. One 49-year-old Puerto Rican male living with HIV and HCV, released for less than two years, put it this way: I got Hep C, I got neuropathy. I got erratic heart rate. I’m on all kind a drugs, but in general, I think I’m pretty healthy. I mean I can’t walk up a hill too quick, but I think I’m pretty healthy. As long as I do not exert myself. My health is very important. I got 9 grandchildren. And, I wanna be around, at least until they get to high school or, you know college if possible. I wanna be around long enough so I can be with them. (ID: 19) I’m running out of regimens, that there’s not too many pills left that I can take so that’s what’s eating me up, now that I wanna be clean. I’ve been using for over 25 years. And, everything good is happening to me again. I got my ex-girlfriend from 20 years ago back in my life, and she knows I’m positive. She’s negative. I wanna live, and I know I don’t have too much time left. No one is guaranteed tomorrow, but when you live with that fact that this is what’s gonna take you out. (ID: 13) I received very good medical treatment. ‘Cause not only am I HIV positive, but I’m co-infected with HIV and HCV. I’ve had several biopsies. I thank God I have no cirrhosis of the liver. My health is excellent. My T cells are about 800 and my viral low is undetected. I eat right, sleep right, exercise. I try to always keep a positive attitude. It’s very important in my recovery, as a drug addict, former drug addict, and goin’ in and out of prison system, HIV/AIDS and HCV. around me. (ID: 07) When I was being released they brought me down to [Facility A] with 38 days left to my release date. And the first day I got out they gave me my keys to my room in a private house, which I live downstairs now a rental apartment. I don’t have that thought of going back into the streets, or doing anything like that. If I can help somebody out, I say well here’s $20. (ID: 04) I started to do this program and so far it’s been like I found a place to live, which they helped me with. Actually I got a pretty good apartment. It’s like a studio. I had already known that HASA would provide a certain amount a cash flow, they would pay for a room and apartment and things like that, so I didn’t really need to go back to that house, which was a good thing. (ID: 02)
Discussion
From an illness narrative perspective, the interviews clearly revealed a sharp divide between HIV-positive and HIV-negative study participants. Nine men living with HIV presented their illnesses using quest narratives, whereas those without HIV resorted to chaos narratives. Each participant encountered significant barriers post-release, including illness symptoms, housing instability, family responsibilities, and a lack of social support. However, only those participants living with HIV were able to overcome these challenges. They emphasized that their diagnosis had provided them with access to healthcare, social services, supportive housing programs, and financial assistance. Furthermore, they perceived HIV as a terminal illness, which helped them focus on making things right with their families and communities.
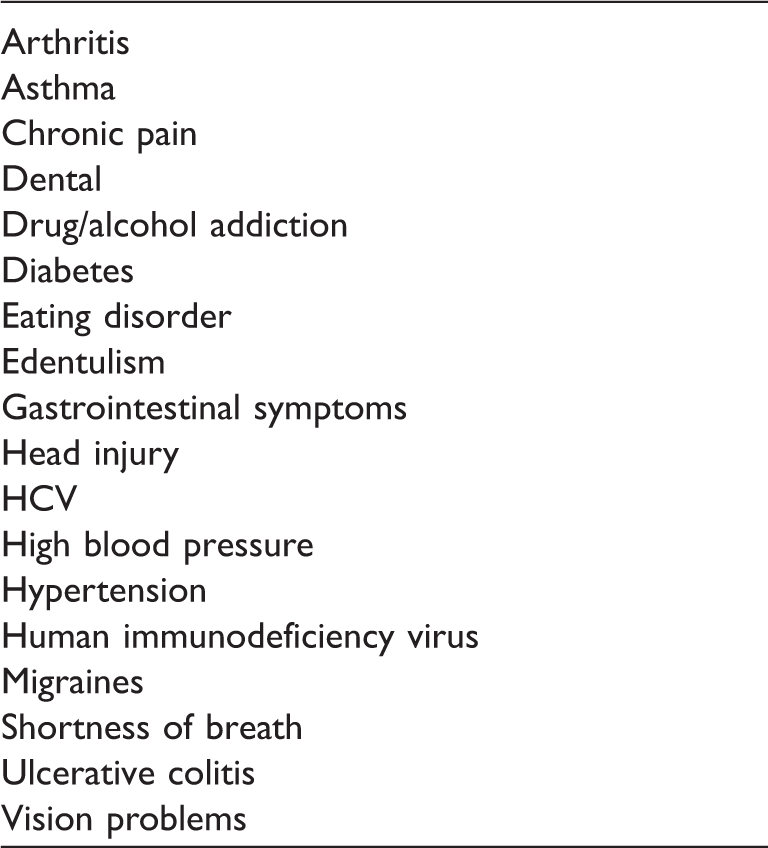
Medical health problems of older former inmates (N = 30).
Limitations
Our findings from this study have several limitations. First, the sample size is too small to detect differences between racial and ethnic groups, with respect to certain demographic variables (e.g. education status, health insurance, and marital status) and their co-morbid chronic conditions, risky behaviors, and competing needs. Second, our interviews were limited to men returning to New York City; therefore, our findings may not be generalizable to all former inmates. The research described here should be replicated with other study populations by increasing the sample size, examining inmates returning to different areas of US, and including women, as female former inmates may experience unique access to and use of healthcare services.
Community reintegration for former inmates is not only a public health and social work problem in US; it is also an international issue. Our results indicate that former inmates may have poor health status and could face major challenges as they reintegrate into society and that those linked to stable support services are much better positioned in terms of successful reentry and maintaining a sense of general well-being. The dire need for such supportive care is highlighted in this study by the contrast between the post-release experiences of participants with or without HIV.
Implications for forensic social work
Forensic social work is a specialization in the field of social work, which focuses on issues related to law and the criminal justice system. Forensic social workers work directly with the court system, legal system, and individuals involved with the justice system (Maschi & Killian, 2011). Given the application of this field, a practitioner trained in this area offers an opportunity to address the community reintegration needs of former inmates. Prior to discharge, forensic social work staff should begin exploring individuals’ illness narratives. At the time of release, these narratives could be used to develop coordinated and comprehensive discharge plans. Further research is necessary to determine how best to improve the resources available to former inmates without HIV but with other debilitating chronic conditions. In addition, health interventions in the field of forensic social work could focus on conducting Medicaid health insurance outreach and enrollment efforts prior to correctional facility discharge.
Implications for public policy
Our findings have larger public policy implications regarding how we understand the nature of aging among criminal justice populations. While NIC defines older inmates as persons between the ages of 50 and 55, the men in the present study do not fit this category of older inmates (Chiu, 2010). In this study, the participants’ average age was 47. It also appears from the findings that participants living with HIV had more services available to them compared to those without HIV. Bug chasing—the practice of intentionally having unprotected sex—has been examined in the men who have sex with men literature (Grov & Parsons, 2006), but very little is known whether this could be a particular problem for newly released inmates. Further studies could examine newly released inmates and their exposure to HIV. The challenge to community reintegration is unique to older male inmates without HIV, and, therefore, additional resources, such as aftercare programs, are necessary to improve this population’s health status (Fazel & Bailargeon, 2011; Health Resources and Services Administration HIV/AIDS Bureau, 2012). The US Supreme Court decision to uphold the Affordable Care Act allows many more members of the criminal justice population to enroll in Medicaid and Medicare health insurance and enables them access to substance use treatment services, medical homes, and other patient-centered programs; this could dramatically improve the health status of former inmates in US (Cuellar & Cheema, 2012).
Footnotes
Ethics
The IRB #2010-448, entitled “Health-seeking behaviors among men with criminal justice and substance abuse histories” was approved by Albert Einstein College of Medicine of Yeshiva University’s Institutional Review Board.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgement
This research was supported by a NIH/NCI grant awarded to Dr. Valera (NCI Grant# K01CA154861). The authors thank the following people for their contributions for providing technical assistance and helpful comments: Janine Burgess, Dr. Rachelle Darout, Christopher McLaughlin, and Mario Rodriguez.