
Abstract
Summary
The Deprivation of Liberty Safeguards were introduced in England and Wales to protect the interests of people with learning disabilities, dementia and neurological conditions resident in hospitals and care homes. The Safeguards apply when residents lack capacity to make decisions about their care and treatment in circumstances that may amount to a deprivation of their liberty. Best Interests Assessors must establish whether a deprivation of liberty has occurred. However, there is no definition in statute; instead, the identification of factors which define a deprivation of liberty is evolving through case law. A factorial survey was used to identify the factors which influenced the professional judgements of 93 Best Interests Assessors (three-quarters social workers) who generated 798 responses to randomly generated vignettes.
Findings
Coercive staff behaviour was the strongest statistical predictor of a deprivation of liberty judgement, followed by the resident’s response. Other indicators of staff control, including the use of medication to reduce agitation, restriction of movement and family unhappiness with care were also significant. The resident’s condition, gender/age and the setting were not significant predictors. Best Interests Assessors were generally confident in their decision making; there were no differences in confidence associated with Best Interests Assessors’ professions.
Applications
Reviews of the operation of the Safeguards stress significant complexity in defining a deprivation of liberty. Nevertheless, this study suggests that the factors which Best Interests Assessors take into account are rooted in the fundamental principles of the Safeguards and an informed appreciation of case law. Best Interests Assessors and local authorities, in their role as supervisory bodies, must keep up to date with developments.
Introduction
Social workers and other professionals are sometimes faced with taking decisions and acting on behalf of people who lack the capacity to make decisions for themselves. These people are, by definition, among the most vulnerable to oppression in any society. In England and Wales, the Mental Capacity Act 2005 (MCA), implemented in 2007, was designed to protect such individuals and ensure that they are supported, as far as possible, to make decisions for themselves.
In some cases people who lack capacity to make decisions about their care may, in the opinion of professionals, need to be protected for their own safety and in their own best interests in a way which deprives them of their liberty. Before the implementation of the MCA, professionals in England and Wales, while being expected to act in the best interests of their clients, did not have to justify their decisions; the only way to challenge a decision was through judicial review. However, this situation was ruled unlawful by the European Court of Human Rights which examined the case of a man (HL) with a learning disability, diagnosed with autism, who had been admitted to hospital over professional concern about his agitated behaviour in day care. He was unable to communicate clearly and either consent to, or refuse admission; however, he made no attempt to leave and was treated as an informal patient. This decision was challenged by his carers and the Court decided his admission constituted a deprivation of liberty (DoL), not sanctioned by a proper legal procedure and which was therefore in breach of Article 5(1) of the European Convention of Human Rights. Further, because he had no means of applying quickly to a court to see whether his DoL was unlawful, it also breached Article 5(4).
In order to avoid further such breaches of Article 5 of the Convention, Parliament amended the MCA to allow the DoL in either a hospital or care home. (The MCA had previously only permitted the ‘restriction of’ liberty, not its deprivation.) The amendment introduced safeguards for people who lack capacity specifically to consent to care or treatment in cases where detention under the Mental Health Act 1983 (2007) was not appropriate. These safeguards are referred to as the Deprivation of Liberty Safeguards (DoLS); they were implemented in England and Wales in April 2009.
A Code of Practice was issued by the Ministry of Justice (2008). This explains that the DoLS apply to people: … who have a mental disorder and lack capacity to consent to the arrangements made for their care and treatment, but for whom receiving care and treatment in circumstances that amount to a deprivation of liberty may be necessary to protect them from harm and appears to be in their best interests. (MoJ, 2008, sec. 1.7)
The Code emphasises (sec. 1.13) that the decision to deprive someone of their liberty ‘ … should not be taken lightly’. In addition to it being in their best interests, it must be a ‘proportionate response to the likelihood and seriousness of harm’ and only if there was no ‘less restrictive’ alternative.
DoLs procedures
Under the DoLS, whenever a care home or hospital believes someone in their care is likely to be deprived of their liberty, they must apply, in England, to the local authority for an authorisation to detain them. (Until April 2013, Primary Care Trusts shared this responsibility.) In Wales, the equivalent ‘supervisory body’ is the local authority in the case of care homes and the local health board for a hospital, although in at least one area (Gwent) there is a joint DoLS team. The supervisory body is responsible for carrying out assessments to determine whether a DoL is occurring, and if so, whether it is in the individual’s best interests or whether care can be provided in a less restrictive manner, or if it would be more appropriate to use the Mental Health Act 1983 (2007). A total of six assessments must take place within 21 days for a ‘standard authorisation’ or seven days, with an additional seven days if needed in exceptional circumstances, for an ‘urgent authorisation’. If all the qualifying requirements are met, the supervisory body is required to give an authorisation. It also sets the time period and imposes conditions where appropriate. These procedures were set out in detail in a Code of Practice (Ministry of Justice, 2008).
Of particular interest to the profession of social work, and the concern of this article, is the opportunity provided by the DoLS and the MCA more generally, to promote the best interests of vulnerable service users with mental disorders (Rapaport, Manthorpe, & Stanley, 2009). The ‘best interests assessment’ is key to the operation of the DoLS. Specifically, this assessment must establish whether a DoL has occurred, or is going to occur. The assessor must consult the manager of the facility and examine any needs assessments and care plans. The assessor must then consider whether the DoL is in the person’s best interests, if it is necessary to prevent harm to the person and whether a DoL is proportionate (MoJ, 2008, sec. 4.58). This will involve seeking the views of the person themselves, family carers, others caring for the person and any personal representative. These views should be taken into account in determining an independent and objective opinion of whether there is justification for a DoL (MoJ, 2008, secs. 4.65–4.66). This opinion must be expressed in a report and conditions may be attached to any DoLS authorisation.
The Code of Practice specifies that the best interests assessment must be undertaken by an approved mental health professional (AMPH), social worker, nurse, occupational therapist or chartered psychologist with, in England, at least two years post-registration experience (sec. 4.60). This Best Interests Assessors (BIA) must also have received approved training and ‘ … have the skills necessary to obtain, evaluate and analyse complex evidence and differing views and to weigh them appropriately in decision making’ (sec. 4.60).
What is a DoL?
The then Labour government chose not to formulate a statutory definition of ‘deprivation of liberty’. The Code asserted that it is ‘ … ultimately a legal question, and only the courts can determine the law’ (introduction to Chapter 2). A list of factors relating to the identification of a DoL taken from case law followed, although the Code stressed that the list was not exclusive (Chapter 2, sec. 2.5). By implication, future legal cases could be expected to identify further factors. Factors identified included the use of restraint, including sedation, to admit a person to the facility; staff exercising complete control over the person’s care and movement, contacts and residence; the person losing autonomy because they are under continuous control; and the refusal of a request by carers for a person to be discharged to their care. However, the Code stressed that ‘There is unlikely to be any simple definition that can be applied in every case … ’ and that ‘no single factor’ was likely to determine whether the circumstances amounted to a DoL (Chapter 2, sec. 2.6).
Previous research
Around the time of the introduction of the DoLS, concern was expressed about the lack of a clear definition. For example, Boyle (2009) feared that this would lead in dementia services to a medical model perspective dominating; since a DoL referred essentially to the social conditions in a care home, the social model of disability should be used, she argued. In a subsequent article (Boyle, 2011), she noted that the number of DoLS applications in the first year of implementation had been much lower than expected by government and expressed concern that staff were insufficiently aware of the DoLS or applying them incorrectly. Phull (2011), a psychiatrist, noted that DoL remained undefined and open to ‘wide interpretation’.
Some of these concerns have been investigated empirically. Manthorpe, Samsi, and Charles (2011) reported an interview study of staff in five dementia care homes in England conducted in the year before the introduction of the DoLS. Managers’ understanding of the complexity of the issue was limited; the authors quoted one respondent baldly asserting, ‘Deprivation of liberty speaks for itself’ (p. 290).
Selmes, Roninson, Mills, Branton, and Barlow (2010) reviewed the circumstances of 55 informal mental health and learning disability patients in one health trust. Defining a DoL in terms of the presence of at least one significant safeguarding factor, 46 of these patients were being deprived of their liberty, mainly because the staff would prevent the person from taking their own discharge. However, adopting the more holistic approach advised by the Code, only six patients, all in old age psychiatry units, were identified with a DoL.
Also in mental health services, Cairns et al. (2011a) developed a set of 28 anonymised vignettes from ‘real life’ cases. These were examined by a panel of six experienced lawyers who strived to reach a consensus about a possible DoL. With reference to the Code, case law and legal principles, they highlighted ‘freedom to leave’, the patient’s subjective experience and attitude to the DoL, and their circumstances before admission as key factors. In an associated study (Cairns et al., 2011b), they asked a panel of six lawyers, psychiatrists, independent mental capacity advocates and five BIAs, to consider 12 vignettes and indicate whether the circumstances amounted to a DoL. There was total agreement in only one case and statistically the levels of agreement were ‘slight’. The authors reported that lawyers were more likely to identify a DoL than BIAs or psychiatrists; however, the sample was very small for the analysis and not representative. Nevertheless, the authors believed that their study raised serious concerns about practical difficulties in making judgements about DoLs.
The number of DoLS applications in England has increased from 7157 in 2009–2010 to 11,393 in 2011–2012 (Care Quality Commission (CQC), 2013). The CQC noted considerable regional variation, with application rates per 100,000 population ranging from 17 in London to 51 in the East Midlands. The explanations for this variation are unclear, but may reflect differential awareness and understanding. In the last two years the proportion of DoLs applications which were subsequently authorised has settled at around 55% (CQC, 2013).
In conclusion, further systematic study about the factors which affect BIAs’ judgements of DoLS is warranted in the light of the development of case law and also the passage of time which have allowed knowledge and practice to become embedded.
Aims of the research
The aims of the study were to:
Identify the factors which influence the professional judgements of BIAs regarding whether an individual who lacks capacity has been deprived of their liberty. Assess the levels of confidence of BIAs in making such decisions. To explore the extent to which BIAs were making reference to case law in making their judgements.
This is one component of a study of the operation of DoLS in England some three years after its implementation. The other components involved discussions with DoLS managers, detailed multiple-respondent case studies and interviews with care home managers and BIAs.
Methodology
The present study employed a factorial survey of BIAs with randomly varied vignettes and open questions. The rationale for factorial surveys in social work research has recently been presented by Wallander (2012). They combine the benefits of both experimental and survey designs and have been used to investigate professional judgements in social and health care. For example, in a recent study quite similar to that presented here, Killick and Taylor (2012) reported a factorial survey of the factors which influence professional decision making in relation to identifying and reporting the abuse of older people. In these studies, respondents are presented with vignettes in which the characteristics of the person and the situation are simultaneously, randomly varied. Multivariate analysis of a large number of cases enables the identification of factors which predict the decision of interest and their relative importance.
The development of the factorial survey followed guidelines offered by Wallander (2012). Consideration of the Code of Practice and consultation with experts (three experienced BIAs) identified possible factors in making judgements. Methodology guidelines suggest a maximum of 10 factors (or independent variables) each with three or four levels. The following were agreed: gender, age of service user, condition, residence, behaviour, e.g. complaining, distress, staff behaviour, e.g. restraint, medication, staff supervision and interaction with staff.
The factorial survey was piloted in three local authorities in Wales in November 2011. Comments from respondents were reviewed and further discussion took place with experienced BIAs and their managers. The descriptions of the levels within factors were amended to increase sensitivity and clarity and factors with no predictive value were removed. Age and gender were combined into one demographic factor. Although ‘race’ is a plausible, probably unconscious, factor in decision making, it was not included because its presence in a vignette was considered too obvious and thus unlikely to be revealing.
Predictors of a deprivation of liberty decision (binary logistic regression, N = 798 vignettes).

Statistically significant p values shown in bold.
Vignette structure.
Respondents were asked for each vignette whether they considered it a DoL and then to indicate on a 1 to 10 scale how confident they were about their opinion (1 = very confident, 10 = not at all confident). They were asked whether there anything else they would want to know before making a judgement and, if so, to add a specific and brief comment. Finally, they were asked whether recent case law had affected their decision and, if so, in what way.
A random number generator selected 10 vignettes for each survey respondent. In other words, each potential respondent received a unique questionnaire with a randomised set of vignettes, with randomised factors in each.
The survey included a request for demographic information and details of professional experience and qualifications that might influence their decision making and their confidence. A copy of the survey is available on request from the corresponding author.
Sample of authorities
The sample was drawn from all nine regions in England as used by the NHS Health and Social Care Information Centre (IC) which receives quarterly data from the supervisory bodies. Two local authorities were recruited from each region; in London, three inner London boroughs and one outer London borough took part.
Procedure
BIA managers in each authority emailed an invitation to BIAs. If the BIA agreed, managers forwarded their email address to the researcher who sent a www link to the online survey. A reminder was sent after three weeks.
Analyses
The primary question was whether there was a DoL (yes/no). Binary logistic regression analysis was used to identify the factors which statistically predicted this decision. This method calculates the likelihood or ‘odds’ of a vignette being judged as a DoL and used the 10 factors discussed above as the independent variables. The unit of analysis here is the vignette, not the respondents.
The statistical predictors of confidence in a given decision (measured on the 1 to 10 scale) were determined using linear regression. The unit of analysis here is the respondent. The predictor variables were, in addition to the vignette factors, the profession and number of years of experience of the respondent, the region in which they were employed and the number of BIAs they had undertaken.
Both binary logistic regression and linear regression analyses were calculated from the 25 non-redundant dummy variables using k–1 dummy variables for each of the 10 categorical independent variables.
Respondents
In total, 237 invitees for the 21 areas agreed in principle to take part in the online survey; however, the survey tool identified that 127 (54%) did not actually access it and 17 others, having read the introduction, did not proceed. Eventually, 93 responded, providing information on 798 vignettes. Almost three quarters (69, 74%) answered all 10 vignettes but 15 (16%) answered four or fewer.
Three quarters of the BIAs were women and eight out of 10 were 41 years of age or older. Nine out of 10 were white. Seventy (three quarters) were social workers; there were 16 nurses, six occupational therapists and no psychologists.
The respondents were generally experienced professionals: 82 (88%) had over six years’ professional experience – a third had 20 years or more. Two thirds had been in their present post for between six and 15 years. All respondents had been qualified as a BIA for at least two years; the average number of best interest assessments they had carried out in the previous six months was 12 (range 0–94); the most prolific assessors were independent practitioners and BIA coordinators. Three out of 10 were also approved professionals under the Mental Health Act (AMHPs). Eleven were independent BIAs and 13 were employed by health trusts, the remainder by local authorities.
Findings
In the collinearity check, there was a weak positive correlation between person’s behaviour and staff behaviour (rs = .232, p < .001) and between age/gender and condition (rs = .176, p < .001). These associations are not surprising, but insufficient to affect the regression analysis.
Deprivation of liberty
Overall, a DoL was identified in 457 (56%) of the vignettes. In general, respondents were quite confident in their decisions. Figure 1 presents boxplots of the confidence ratings for those vignettes judged as a DoL and not. Half the judgements were made with confidence ratings of between 1 and 3, indicating high confidence. The dark horizontal line represents the median. The box includes 50% of the ratings and the ‘whiskers’ encompass around 98% of all ratings. The circles represent outliers.
Boxplot of deprivation of liberty by confidence in opinion.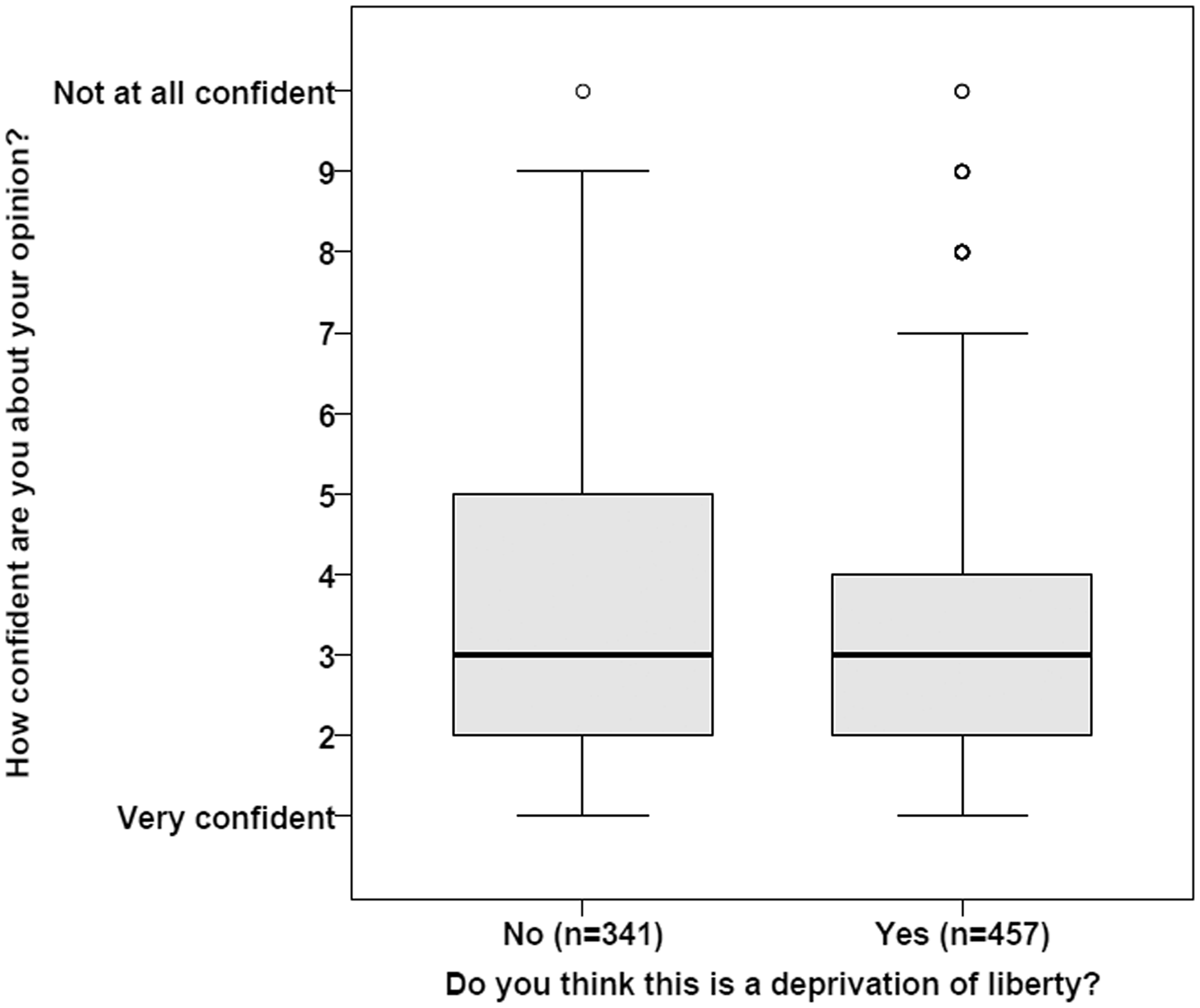
There was a statistically significant difference in the mean confidence ratings in vignettes where a DoL was identified compared to those where a DoL was not identified (M = 3.4, SE = .084 vs. M = 3.8, SE = .104; t(796) = 2.462, p < .05).
Judgement of DoL
All 798 vignettes responses were included in the binary logistic regression analysis (Table 1). The first variable in each category is the reference category; these are shown in each case. For example, a 70-year-old woman is the reference category for the combined age and gender factor.
The statistical model accounted for 30% of the variance. The statistical significance of each factor’s contribution to the model is shown together with the odds ratio (Exp(B)) and 95% confidence interval. In a large sample, the Wald statistic is a good indicator of the strength of the contribution (effect size) and these values are shown in Figure 2. In this model, seven of the 10 factors made a statistically significant contribution to the model and three did not.
Predictors of BIAs’ judgments of a deprivation of liberty: strength of variable category (Wald statistic, binary logistic regression), N = 798.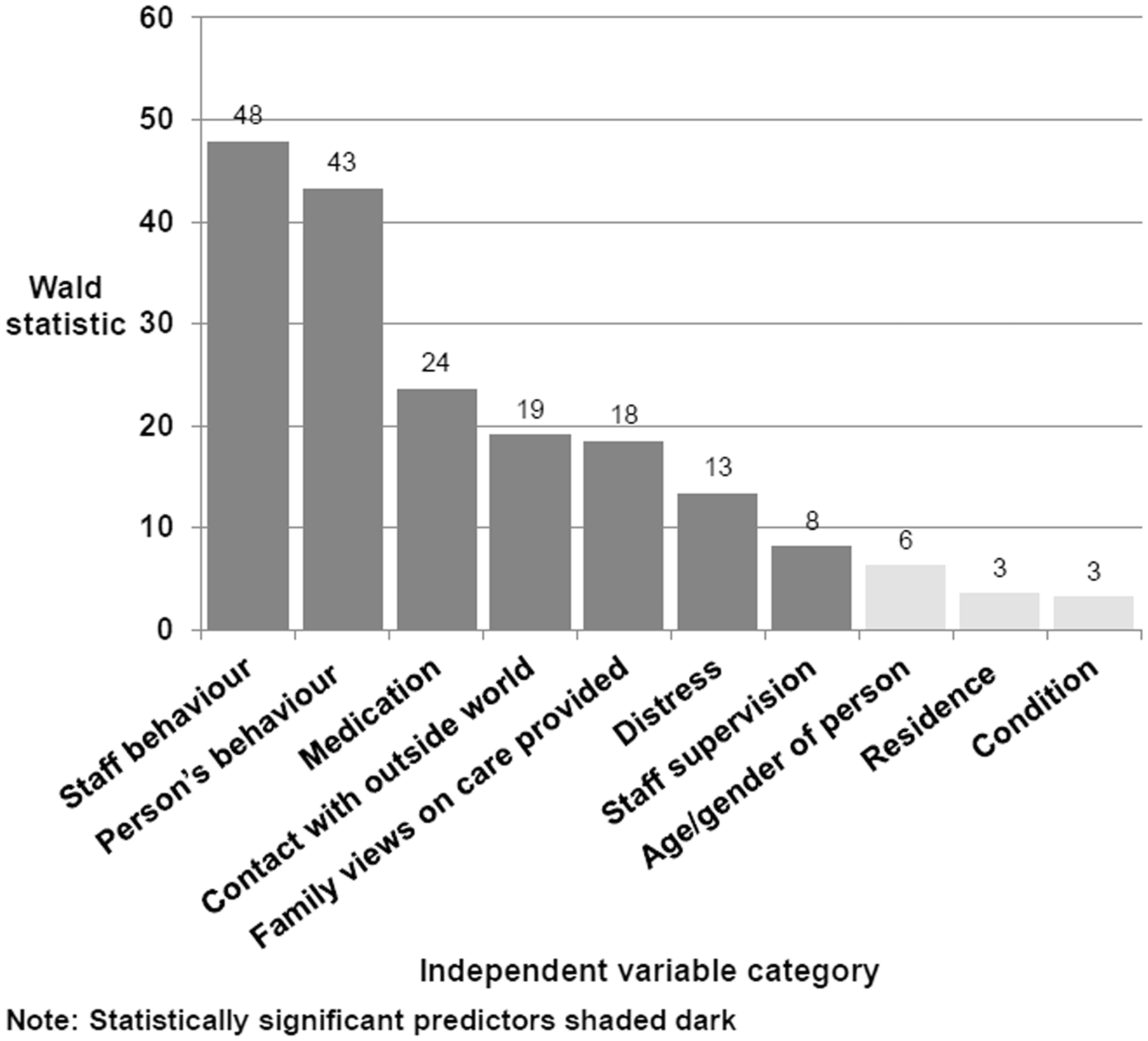
Staff behaviour was the strongest statistical predictor of a judgement of a DoL, especially if they were using coercive strategies to restrain the person from leaving the setting, but also if they were attempting to distract or verbally dissuade the person from leaving. Respondents are almost six times as likely to state that staff using coercive strategies was a DoL, compared to not taking any coercive action.
The service user’s (resident or patient) behaviour was almost as strong an influence as staff behaviour. Thus, if the user frequently makes purposeful attempts to walk out, saying ‘I want to leave’, respondents were five times as likely to consider this evidence of a DoL, compared to giving no such indication. If the user stated ‘I feel like a prisoner here’, but had made no serious attempt to leave, a DoL judgement was twice a likely.
The ward’s or care home’s use of medication also strongly influenced a DoL judgement. Respondents were nearly three times as likely to identify a DoL if the user was on regular and high level doses of medication, including use of PRN, to reduce agitation and anxiety, and nearly three times as likely if they were just on a PRN dose for the same reason.
The service user’s lack of contact with the outside world was also quite a strong predictor: compared to service users who went out frequently, those who went out infrequently or rarely were over twice as likely to be judged as experiencing a DoL.
The family’s views of the care and treatment their relative was receiving in the setting were influential in the BIA’s decision. If the family was unhappy with all aspects of the care, a DoL judgement was two and a half times as likely relative to cases where the family was satisfied; where the family was unhappy with some aspects of care, a DoL judgement was 1.7 times more likely.
The service user’s level of distress was considered an indicator: relative to users showing no sign of distress, respondents were over twice as likely to identify a DoL when a user was distressed and agitated on a regular basis.
Finally, the level of special staff supervision was a weak predictor of a DoL judgement. Compared to cases where no such supervision was in place, respondents were 85% more likely to report a DoL for persons accompanied by staff when they are out of the care home or ward, and 69% more likely to report a DoL for users supervised one-to-one.
The other three factors did not predict a DoL judgement: the service user’s condition, whether dementia, learning difficulties, anxiety and delusional beliefs, and brain damage or brain injury: place of residence, whether care home, hospital ward or mental health unit; and overall, the combined age and gender factor.
Confidence about judgement of DoL
Over half the judgements were made with a high level of confidence. An exploratory series of analyses of variance (ANOVAs) was run prior to the linear regression analysis. This tested the differences in mean confidence ratings according to the demographic variables (gender, age, ethnicity and profession) and professional experience included in the survey. There were no statistically significant differences associated with any of these variables, with the exception of ‘number of years in post’ (F(4,87) = 4.13, p = .004). This effect was attributable to lower mean confidence ratings made by respondents (n = 8) who had been in their current post for less than one year, compared to ratings made by more experienced BIAs. Not surprisingly in this context, the linear regression analysis failed to produce a statistically significant model. The conclusion is that BIA’s confidence cannot be reliably predicted by any of the demographic and experience variables in this survey.
The influence of case law
In over a third of vignettes (37%), respondents stated that case law had affected their decision making about a DoL. It was used in 45% of vignettes where a DoL was identified, compared to 25% where a DoL was not identified. This difference was statistically significant (χ2 (1, 798) = 35.99, p < .0001). Sixty BIAs (65%) referred to case law in at least one vignette: in 55% of vignettes where a DoL was identified, compared to 33% where not (χ2 (1, 93) = 3.96, p = .046).
The case law most commonly cited was Hillingdon v. Neary (2011) which concerned the local authority’s failure to be clear about the capacity in which it was making decisions; and Cheshire and Cheshire West v. P & M (2011) and P & Q v. Surrey (2011) which indicated that a possible DoL be considered in the context of what was ‘normal’ for a person’s situation; Storck v. Germany (2005) defining a possible DoL in a mental health unit; DE & JE v. Surrey (2006) in which the council (not the care home) effectively prevented the person from leaving; and GJ v. The Foundation Trust (2009) which held that a person could not be detained under the DoLS authorisation for the treatment of his mental disorder, but could be for a physical disorder; and C v. Blackburn and Darwen Borough Council (2011) where the person was found not to be deprived of his liberty even though he had kicked down a door trying to leave his care home.
Discussion
The aims of the study were to identify the factors which influence the professional judgements of BIAs regarding a possible DoL and to assess their confidence in making such decisions.
DoLS judgements in the context of case law
In the survey, a DoL was most likely to be identified when staff were preventing someone who evidently wanted to leave from doing so; these factors are the core of defining a DoL. Patients’ freedom to leave was similarly highlighted by the lawyers in a previous study (Cairns et al., 2011a).
The other factors shown to influence the identification of a DoL were apparently considered as indicators of staff control over the person. Thus, the use of medication to reduce agitation and anxiety could have a restraining function; it is mentioned in the Code of Practice in the context of admission to the facility, but appears here to be interpreted as including restraint once admitted. The presence of regular distress and agitation was in itself a strong predictor of a DoL, presumably being interpreted as an indicator of a user’s negative response to their situation. The patient’s response was also considered important by the lawyers in Cairns et al.’s (2011a) study.
The Code of Practice refers to staff exercising complete control over the person’s movement and contacts. In line with recent case law C v. Blackburn and Darwen Borough Council (2011), survey respondents considered that lack of contact with outside world in itself was a significant factor.
The information that a user’s family was unhappy with the care and treatment provided was significantly associated with a DoL judgement. The Code mentions as a key factor what might well be the next step in these circumstances, the refusal of a request by the family for a person to be discharged to their care (DE & JE v. Surrey, 2006; Hillingdon v. Neary, 2011).
It is interesting to note that close supervision was only a marginally significant factor in predicting a DoL judgement. This is likely to reflect a view that such supervision is appropriate in some cases in order to protect the service user from harm, a point suggested in the P & Q v. Surrey and Cheshire West cases. Nevertheless, the finding that the person’s condition and their age and gender were not significant predictors indicated that the BIAs were, quite correctly, making their judgements about a DoL on the basis of the actions and behaviour of staff and user alone. Similarly, where this took place, whether care home or hospital, was not relevant.
The BIAs were generally confident about their judgements; perhaps surprisingly, social workers, AMHPs and independent practitioners (who were generally the most experienced) were no more or less confident than other BIAs. The finding that profession and demographic factors did not affect confidence would be encouraging, if judgements were consistent. Coincidentally, the proportion of positive DoL judgements made in the factorial survey mirrored the proportion of authorisations in national statistics (CQC, 2013).
It is also encouraging to see that the majority of respondents were explicitly using case law to make their judgements and that they referred to relevant cases. This finding is in contrast to Braye, Preston-Shoot, and Wigley (2013) who found in a small vignette study (n = 6) that adult social care practitioners’ narratives were ‘strikingly’ free of legal references. The difference may reflect the provision of appropriate CPD opportunities for BIAs and support from local coordinators. Anecdotal evidence suggests that BIAs’ reports are increasingly likely to reference case law explicitly (Braye et al., 2013). Case law was being used to determine both what is, and what it is not a DoL. For example, P & Q v. Surrey (where the judge decided there was no DoL) seems to have been used conversely. In that case, the fact that there was ‘no objection’, ‘no close supervision’, and that the users were ‘going out’, apparently suggested that if there if the reverse were true, a DoL might be present.
Limitations
The obvious methodological limitation of this study was that the judgements were made from short constructed vignettes rather than real life investigations. According to the Code of Practice, BIAs are expected to consult widely and to examine assessments and care plans as described above. Understandably, respondents sometimes indicated that they would want further information and it is also possible that respondents misinterpreted the information presented. Conversely, the strengths of the factorial survey were that the vignettes included a larger number of factors than a conventional vignette study. Also, their systematic (random) variation and multivariate analysis can reveal and quantify the influence of factors, which the respondents themselves may not realise.
It was noted above that the proportion of vignettes that had to be removed because of implausible combinations of factors (one third) was much higher than usual (Taylor & Zeller, 2007). This was partly a consequence of the wide range of service user groups (‘conditions’) represented in this study, in comparison to studies which just focused, for example, on older people (e.g. Killick & Taylor, 2012). The other reason was because of the particular significance in this example of the interaction between person and staff behaviour: for example, staff would not use strategies to restrain the person from leaving the setting if s/he were not making an attempt to leave. The collinearity checks showed that the strategic removal of implausible combinations was almost entirely successful.
The response rate to the survey was less than expected. It could not be attributed to the nature of the task because half the respondents who had previously agreed to participate did not open the survey. It is possible that access to the Survey Monkey™ software was blocked by some agencies’ firewalls. We are not able to say whether the respondents were representative of BIAs nationally; however, the sample of vignette responses achieved was more than required by the prior statistical power calculation.
Conclusion
The reliance on developments in case law to guide the operation of the DoLS makes this a difficult area for specialist practice. The CQC (2012), while welcoming recent judgements, observed that there remained ‘significant complexity’ in defining what constitutes a DoL and when the Safeguards should be applied. In a recent case, the judge in A Local Authority v. PB & P (2011) warned that there will always be ‘borderline’ cases and advised applying the Safeguards to ensure the person’s rights are protected, and that providers and supervisory bodies are better protected against findings of an unlawful DoL. It therefore behoves individual BIAs and local authorities in their role as supervisory bodies, as well as care homes and hospitals to keep up to date with case law on the meaning of DoL. For example, at the time of writing, the Supreme Court Registry had confirmed (March 2013) that the controversial decision in the Cheshire West and Cheshire Council v. P & M (2011) case will be heard from 22 October 2013 to 24 October 13. This case and P & Q v. Surrey County Council had been given permission to appeal.
The need to protect the rights of service users who lack capacity to take their own decisions about their care and treatment and to promote their best interests should be at the heart of social work practice. The DoLS were generally welcomed by social workers and other professions, albeit with concerns about the clarity of making judgements. This study suggests that the factors which BIAs are taking into account are rooted in the fundamentals of the Safeguards and an appreciation of case law.
Footnotes
Ethics
The study was approved by the South West 5 NHS Research Ethics Committee.
Funding
This article presents independent research commissioned/funded by the NIHR School for Social Care Research. The views expressed in this publication are those of the authors and not necessarily those of the NIHR School for Social Care Research or the Department of Health, NIHR or NHS.
Acknowledgements
We would like to thank the Mental Health Research Network (West Hub) for invaluable support in recruiting participants to this study.