
Abstract
Summary
In the past 20 years, research suggests that social workers and counselors are at risk of developing secondary traumatic stress from working with traumatized client populations. However, only a few studies have examined specific risk and protective factors that may buffer the social worker from developing secondary trauma symptoms. This article reports the results from a cross-sectional survey-based study of clinical social workers in which a predictive model of secondary traumatic stress was sought. In order to obtain an optimally predictive subset of variables from a larger set of candidate variables, this study employed a rigorous variable selection procedure using criteria-based methods for arriving at a final model predicting secondary trauma.
Findings
The results suggest that the ratings of the supervisory relationship, salary, caseload size, and personal anxiety may be salient factors that impact the development of secondary trauma among clinical social workers. Specifically, positive ratings of supervision and higher income level were found to predict a substantial decrease in the degree to which a social worker possessed secondary trauma symptoms.
Applications
Secondary trauma threatens clinician health, client quality of services, and contributes to increased financial burdens to nonprofit agencies due to burnout and employee turnover. At an organizational level, administrators and policymakers can address these problems by providing higher salaries, encouraging reasonable client caseloads, and ensuring that social workers have access to skilled clinical supervisors. At an individual level, personal self-care to reduce daily anxiety may be important to protect clinical social workers from developing secondary trauma symptoms.
Commonly thought of as a problem that occurs among soldiers who experience traumatic events during military combat, posttraumatic stress disorder (PTSD) is prevalent among many groups of adults and children, including those who live in poor communities with high levels of neighborhood violence and crime, those who have experienced interpersonal violence such as physical or sexual abuse, and those who experience trauma due to natural and man-made disasters (National Center for Post-Traumatic Stress Disorder, 2013). Moreover, in many circumstances trauma happens repeatedly over months or years, leaving a person to cope with such symptoms as extreme anxiety and panic, feeling unsafe during most times of the day and night, struggling with chronic insomnia, and repeatedly re-experiencing memories of the trauma (Dorahy et al., 2013; Quinn, 2008).
Many people who struggle with PTSD seek formal help from a trained mental health counselor, such as a clinical social worker. As a result, the counseling and social work professions have sought to develop effective psychotherapeutic treatments to help people experiencing symptoms of PTSD (Cusack et al., 2016). However, since the beginning of the 21st century accumulated research findings suggest that mental health professionals—clinical social workers in particular—may develop what has variously been called secondary trauma, vicarious trauma, or compassion fatigue as a result of working with and being exposed to traumatized client populations (Ludick & Figley, 2017). For example, social workers who provide trauma-based counseling have frequently reported experiencing PTSD-like symptoms, including (a) feeling emotionally numb, (b) reliving the trauma experiences of their clients, (c) developing panic-like symptoms when thinking about their clients outside of work, (d) having disturbing dreams about their clients’ trauma experiences, and (e) experiencing increased irritability and difficulty concentrating; all of which parallel PTSD symptoms (Bride, Robinson, Yegidis, & Figley, 2004; Ewer, Teesson, Sannibale, Roche, & Mills, 2015).
Referred to as secondary traumatic stress (STS) in the current article, this phenomenon has become a growing concern particularly in the social work field (Bride, Radey, & Figley, 2007; Gil & Weinberg, 2015; Kintzle, Yarvis, & Bride, 2013; McCann & Pearlman, 1990). As a result, many research studies have examined (a) STS prevalence rates, (b) individual risk factors such as clinician past-trauma history, as well as personal depression and anxiety related to STS, and (c) the influence of general workplace factors such as job satisfaction and social support upon STS (Bride, Jones, & Macmaster, 2007; Bride & Kintzle, 2011; Ewer et al., 2015; Pearlman & Mac Ian, 1995). However, only a handful of studies have investigated the predictive strength of specific risk and protective factors common to a clinician’s everyday experiences of helping others, including the supervisory relationship, the type of work (e.g. in a community setting and/or in the mental health field), client trauma type (e.g. developmental versus episodic) and caseload size (Slattery & Goodman, 2009; Williams, Helm, & Clemens, 2012).
A better understanding of the relationship between these latter factors and STS may further assist policymakers, administrators of mental health agencies, and other organizations toward developing best-practice guidelines with the goal of safeguarding counselors and social workers from developing secondary trauma (Dworkin, Sorell, & Allen, 2016; Ivicic & Motta, 2016; Kulkarni, Bell, Hartman, & Herman-Smith, 2013; Ludick & Figley, 2017; Slattery & Goodman, 2009). Therefore, the current study contributes to the literature by developing a predictive model that describes the impact of specific risk and protective factors upon STS symptoms among clinical social workers.
Literature review
Concerns regarding PTSD-like symptoms among helping professionals who treat traumatized client populations began to consistently appear in counseling and social work literature during the last decades of the 20th century. While these concerns can be traced back to at least the 1970s (Danieli, 1980; Haley, 1974), in the late 1980s and 1990s McCann and Pearlman (1990) developed one of the first operational definitions of STS symptoms in which they defined “vicarious trauma” as the change that occurs within a clinician as a result of empathic engagement with client trauma material (Pearlman & Mac Ian, 1995). McCann and Pearlman (1990) also argued that STS symptoms were distinct from the concept of burnout, in which a helping professional in reaction to job-related stress may feel emotionally exhausted, lack feelings of professional efficacy, and develop negative perceptions and feelings toward their clients (Daley, 1979; Schaufeli, Leiter, & Maslach, 2009). Whereas burnout is considered to occur in the course of experiencing general job stressors, STS and related concepts are considered to occur specifically as a result of exposure to traumatized clients (Salston & Figley, 2003).
Paralleling the work on vicarious trauma by McCann and colleagues described above, during the same time period Figley (1995) likewise contributed to this emerging literature base by linking a similar concept called “compassion fatigue” with his novel concept of “secondary traumatic stress disorder,” which he defined as extreme stress experienced as a result of helping or wishing to help a suffering or traumatized person (Figley, 1995, 2002). Building on Figley’s work, Bride, Robinson, Yegidis, and Figley (2004) developed an STS self-report scale to measure clinician-reported trauma symptoms, designed to approximately mirror the PTSD symptom clusters of the Diagnostic and Statistical Manual of Mental Disorders (DSM; American Psychiatric Association, 2000, 2013).
As a result of this early foundation-building research, subsequent studies have found that the prevalence of STS among helping professionals exposed to client trauma is approximately two to five times the 7% US prevalence rate of adults with PTSD, including 15% of social workers, 34% of child welfare workers, 39% of juvenile justice workers, 33% of military mental health providers, and 19% of substance abuse counselors (Bride, 2007; Bride, Hatcher, & Humble, 2009; Bride & Kintzle, 2011; Hatcher Smith, Bride, Oh, Moultrie King, & Franklin Catrett, 2011; Kintzle et al., 2013; National Center for Post-Traumatic Stress Disorder, 2013).
Furthermore, findings collected from the modest amount of research studies that have investigated potential risk and protective factors contributing to or reducing STS, suggest that past personal trauma history, anxiety and depression, and general workplace factors, such as job satisfaction, social support, and job turnover may be associated with secondary trauma among helping professionals (Bride & Kintzle, 2011; Bride et al., 2007, 2009; Devilly, Wright, & Varker, 2009; Dworkin et al., 2016; Ludick & Figley 2017; Slattery & Goodman, 2009; Williams et al., 2012). In particular, one study’s findings suggested that job satisfaction may mediate the relationship between STS and job turnover (Bride & Kintzle, 2011). In addition, a small number of studies have reported finding positive relationships between STS and workplace setting type, client trauma type, and caseload size, respectively (Devilly et al., 2009; Dworkin et al., 2016; Kulkarni et al., 2013).
Likewise, a few studies have investigated the relationship between the supervisory relationship and STS. The supervisory relationship is considered a necessary component of effective psychotherapy, both in enhancing supervisees’ feelings of efficacy and in contributing to positive client change (Watkins, 2017); and is also considered to be a potential protective factor from developing STS (Gil, 2015). Among studies investigating the supervisory relationship, a significant inverse relationship has been reported in which the supervisory working alliance reduced secondary trauma symptoms among counselors-in-training (Toren, 2008). Moreover, Slattery and Goodman (2009) found that the supervisory relationship reduced domestic violence advocates’ likelihood of developing trauma symptoms.
In general, however, the overall findings are equivocal. Some studies have reported no relationship between factors such as job satisfaction, caseload size, frequency of clinical supervision, the supervisory relationship, and STS (Devilly et al., 2009; Dworkin et al., 2016; Ivicic & Motta, 2016). For instance, Williams, Helm, and Clemens (2012) found no relationship between a measure of the supervisory working alliance and secondary trauma among a sample of mental health counselors; Wood (2011) also reported similar findings.
In summary, the research base examining the role of risk and protective factors in the development of STS among counselors and social workers is modest, and the results are mixed. Therefore, the current study seeks to develop a predictive model that will further clarify which risk and protective factors most impact STS symptoms among clinical social workers.
Purpose of the study
The purpose of this exploratory study is to better understand how clinical social workers’ personal and professional experiences impact the development of STS. Specifically, the goal of this study is to investigative the impact upon STS of risk and protective factors relevant to the experiences of social workers, such as the clinical supervisory relationship, work type, client trauma type, and caseload size, among others described below. In order to develop an accurate model that reliably predicts secondary trauma among clinical social workers, this study utilized a variable selection statistical method to obtain an optimal subset of explanatory variables among a larger candidate set.
In this way, a more complete picture of what particular factors influence the occurrence of STS can potentially be obtained, with an overarching intent to provide guidance for administrators and policymakers toward implementing best practices within mental health organizations in order to mitigate the incidence of STS among helping professionals.
Methods
Data was collected using a cross-sectional study design consisting of a state-wide, mail-based survey of randomly selected clinical social workers in the Southeast United States conducted in October 2013.
Participants
Human subjects
Approval from the university Institution Review Board was obtained prior to beginning the study. In order to achieve confidentiality, each respondent was assigned a number that provided a link to the respondent’s mailing address. When the data-collection time frame expired (i.e., approximately six weeks), the document containing the link between a respondent’s number and his or her identifying information was destroyed. In addition, informed consent was obtained by providing a cover sheet in the mailed survey packet with a description of the study, a consent script, and contact information regarding further questions.
Recruitment
As Figure 1 illustrates, the sample was selected from a larger sampling frame of social workers who had obtained their intermediate social work license (i.e., Licensed Master’s Social Work (LMSW)) during the previous four years. By law, the state in which this study was conducted requires that a clinical social worker possessing an LMSW receive a minimum of three years of clinical supervision training prior to becoming a Licensed Clinical Social Worker (LCSW). The LCSW is the highest clinically-based license that can be obtained in social work, and is required by many employers; therefore, clinical social workers are highly motivated to obtain their LCSW.
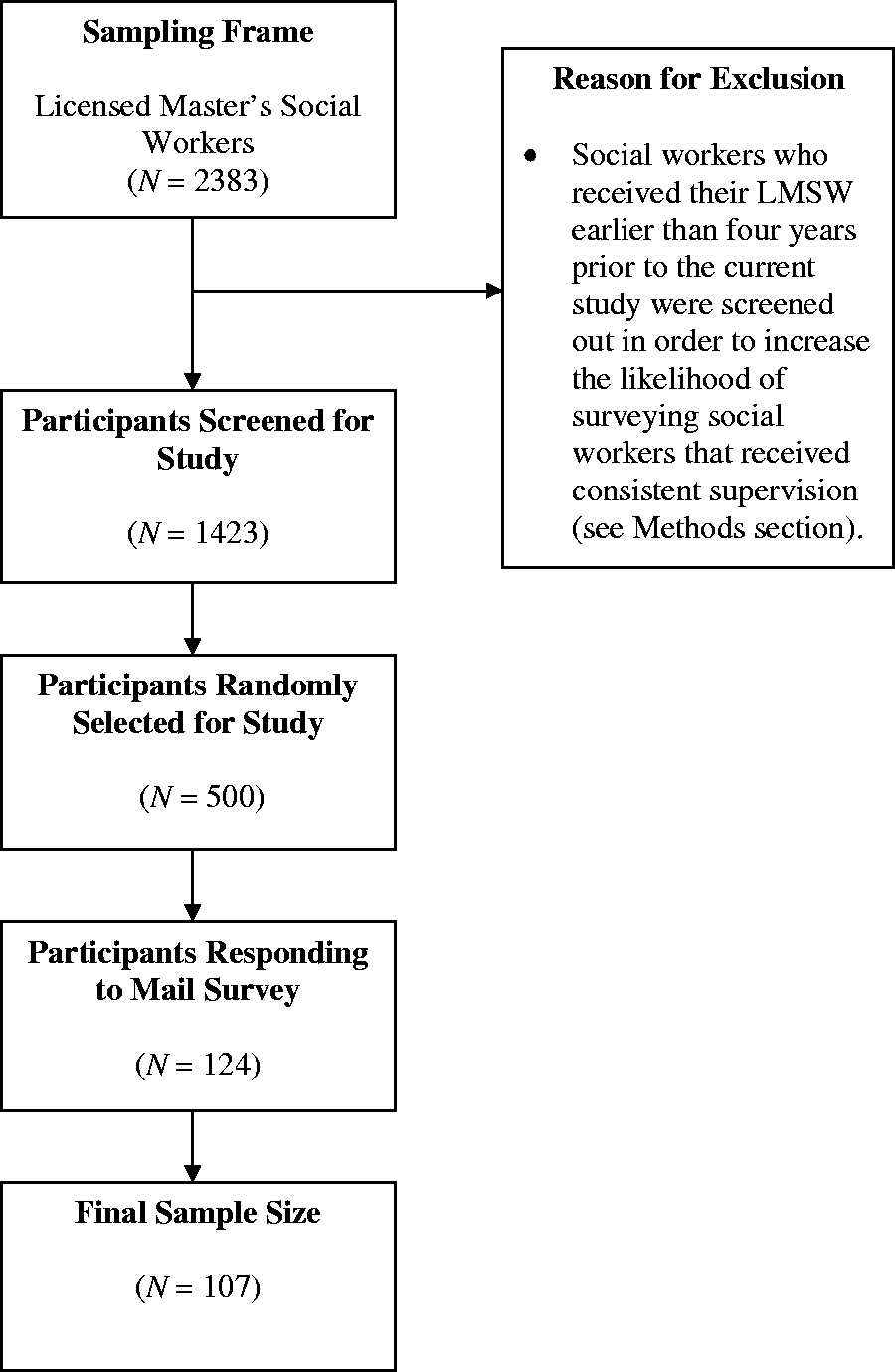
Participant selection flow diagram.
This particular sampling frame of social workers (i.e., those having obtained the mid-level LMSW license within 4 years prior to October 2013) was chosen in order to increase the likelihood that a sample of practicing social workers receiving ongoing weekly or biweekly supervision would be obtained. The rationale for this decision was based upon speaking with multiple licensed clinical social work supervisors. These supervisors agreed that once a clinical social worker has obtained his or her LCSW license the likelihood of continuing to receive frequent and ongoing clinical supervisor decreases (i.e., LCSW’s are no longer required by law to receive supervision, though ethical guidelines encourage life-long supervision for practicing social workers; and licensure renewal requires continuing education units (CEU) to be obtained, but not necessarily supervision).
Randomization
Due to documented low response rates for surveys focusing on this population, combined with cost restrictions, the initial mailing sample was chosen to be 500 participants. Previous STS studies that conducted mail-based surveys of helping professions (e.g. social workers, substance abuse counselors, and nurses) have reported response rates between 20% and 50%, though these response rates tend to cluster around 20% to 30% (Bride et al., 2009). Therefore, a mailing sample of 500 was expected to yield a minimum of 100 respondents and a maximum of 250 respondents, or a 20% to 50% response rate, respectively.
As Figure 1 indicates, 1,423 participants were screened for this study based upon the time frame in which they had initially obtained their LMSW certification. Subsequently, a simple random sample of 500 participants was obtained from this larger sampling frame. The response rate for this study was 24.8%, or 124 respondents. After removing unusable questionnaires, the overall sample size was reduced to 107, a final response rate of 21.4%. The 16 unusable questionnaires were removed due to over half the survey left blank or due to respondents returning a completely blank survey with a note explaining why. The reasons for not filling out the survey were generally due to time constraints. While low, the final response rate of 21.4% fell within the bounds of what is typical for this type of mail-based survey study that seeks information related to secondary trauma among helping professionals (Bride et al., 2009).
Procedures
Using survey design guidelines suggested by Dillman, Smyth, and Christian (2009), a survey packet was mailed to the sample of 500 clinical social workers with a requested completion date three weeks in the future. A week later, a respectful and appreciative letter was mailed to all who had not responded, reminding the participants of the completion date. Moreover, when the completion deadline arrived, a third reminder letter was mailed to all who had not responded, requesting completion of the packet at a date one week in the future. Finally, a thank you letter was sent to all respondents upon completion of the study.
Measures
The survey used in this study asked respondents to provide (a) demographic information (i.e., age, race/ethnicity, income, education), (b) information related to clinical experience, workload, work setting, type of work, extent and type of client trauma, and personal experience of anxiety and trauma, and (c) information related to clinical supervision, including supervisor gender, frequency of supervision, duration of current supervision, and satisfaction with supervision. In addition, the survey asked respondents to complete two multi-item instruments, the Secondary Traumatic Stress Scale (STSS; Bride et al., 2004) and the Supervisory Relationship Inventory (Schacht, Howe, & Berman, 1988), both of which were Likert scaled. The final variables for each of these constructs were generated by aggregating the 17-item and 40-item instruments, respectively.
Moreover, of the 34 variables measured in this study, 20 were continuous and 14 were categorical. Table 1 provides a list of the final set of candidate variables used in the current study after certain variables were removed due to being highly collinear; the final number of candidate variables in this study was 24, composed of 11 continuous and 13 categorical variables.
Initial set of candidate explanatory variables by category.
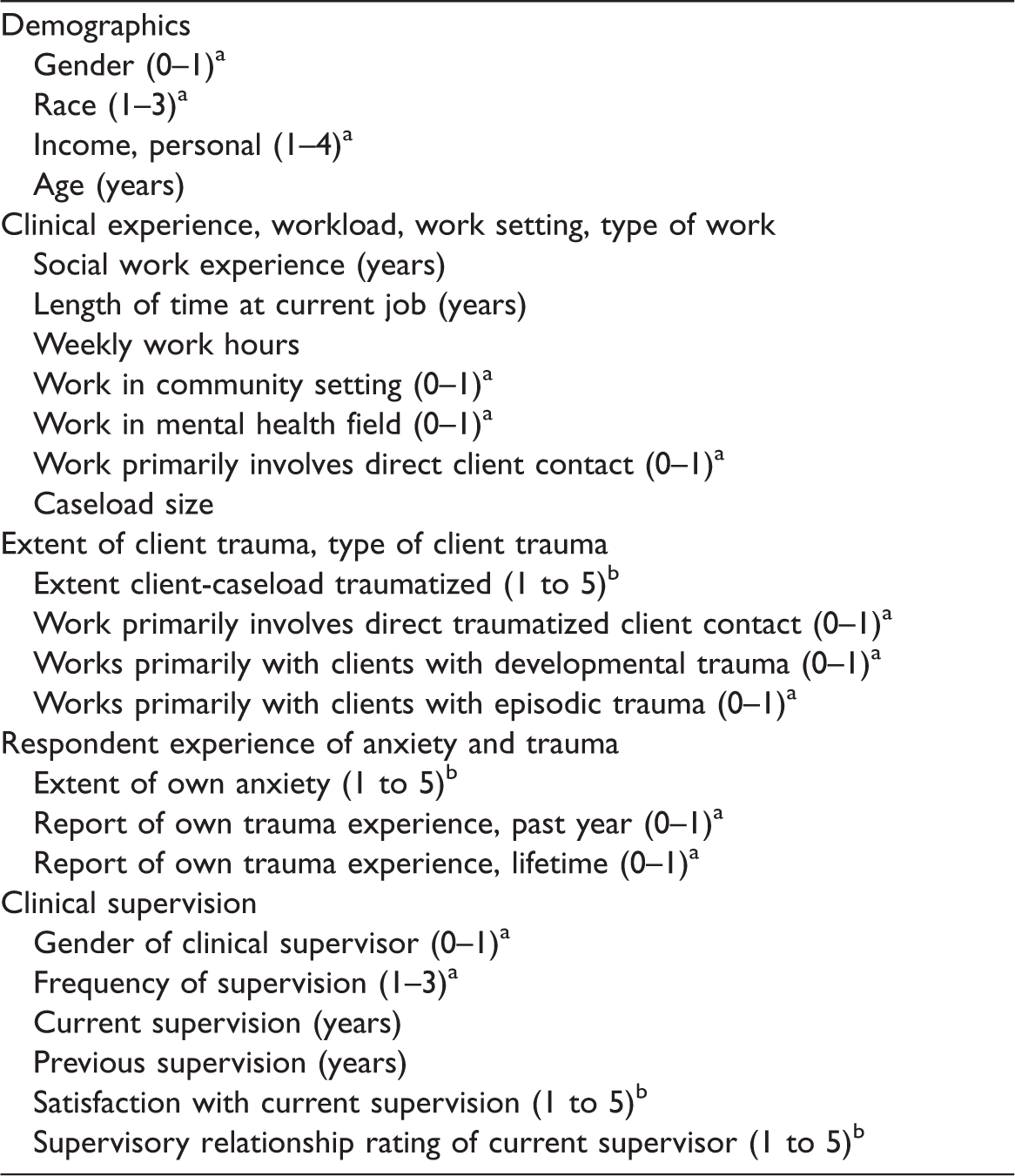
aIndicates categorical variable.
bIndicates Likert scale.
Response variable
The response variable is the level of STS reported by the respondents on a 17-item instrument. The STSS (Bride et al., 2004) measures the frequency of intrusion, avoidance, and arousal symptoms associated with STS as a result of working with traumatized clients in the past week. To meet diagnostic criteria each item must be rated 3 or higher on a 5-point Likert scale ranging from never (1) to very often (5). A total STS score is found by aggregating the 17 items. The STSS was chosen over other scales due to its congruence with the diagnostic criteria of PTSD. Moreover, the STSS has demonstrated strong convergent, discriminant, and internal validity (Bride et al., 2004; Ting, Jacobson, Sanders, Bride, & Harrington, 2005). In addition, past studies have reported the Cronbach’s alpha coefficient of reliability in order to assess internal consistency of the STSS, α = .93 (Bride et al., 2004), α = .94 (Ting et al., 2005), α = .86 (Choi, 2011), and α = .95 (Kintzle et al., 2013). The Cronbach’s alpha for the STSS in this study was found to be comparable to past studies, α = .92.
Explanatory variables
Exposure to traumatized clients. A primary explanatory variable in this study is the level of client-trauma exposure experienced by respondents surveyed. According to Bride and colleagues (Bride, 2001; Bride et al., 2004; Ludick & Figley, 2017) client exposure is theorized to precede in time the occurrence of STS. Although this study is cross-sectional, assessing the relationship between exposure to client trauma and level of STS is important to the theoretical underpinnings of this study. Exposure to client trauma is operationalized by assessing the number of traumatized clients on a social worker’s caseload as well as the degree to which the respondent reports his or her caseload as being traumatized on a 5-point Likert scale ranging from never (1) to very often (5). In addition, a dichotomous variable was created from measures of weekly work hours with various types of clients, indicating whether a respondent’s clinical work was primarily with traumatized clients, based upon exposure to traumatized clients for 50% or more hours of a typical work week (i.e., a 50% cutoff was chosen after interviewing multiple clinical supervisors who stated that the current expectation in the mental health field is that a full-time clinician submits 20 to 25 hours of reimbursable clinical billing per week, or about 50% of an average work week is spent primarily seeing and thinking about clients).
The supervisory relationship. Another primary variable in this study is the quality of the supervisory relationship provided by the respondent’s supervisor, as rated by the respondent. A good supervisory relationship is hypothesized to be one that promotes a facilitative relationship for a supervisee, in which the supervisor consistently conveys a genuine attitude of acceptance, openness, and understanding to the supervisee (Nelson & Friedlander, 2001). This type of relationship is typically considered to positively facilitate a supervisee’s ability to perform his or her job well, feel efficacious as a counselor and, as a result, provide quality clinical services to his or her clients (Hill, 2007; Hill et al., 2016; Kadushin & Harkness, 2002; Rogers, 1957; Watkins, 2017). The measure of a supervisory relationship is operationalized as a mean score obtained from the 40-item Supervisory Relationship Inventory (Schacht et al., 1988). The Supervisory Relationship Inventory was chosen over other supervisory alliance/relationship instruments due to the strong theoretical link with the psychologist Carl Rogers’s proposed therapeutic conditions, and due to research which consistently suggests that facilitative qualities similar to Rogers’s therapeutic conditions are important to and common factors within clinical supervision (Nelson & Friedlander, 2001; Watkins, 2011, 2017). Moreover, previous research has reported that high and low supervisory relationship ratings using this instrument are strongly correlated with supervisees’ perceptions of therapists who respectively contribute most and least to their feelings of therapeutic effectiveness (Schacht, Howe, & Berman, 1989).
The Supervisory Relationship Inventory is composed of five subscales, measuring the relationship constructs of Empathy, Regard, Unconditionality, Congruence, and Willingness-to-be-Known. Conceptually, Empathy refers to the extent of one person’s immediate awareness of another person’s experience; Regard refers to affective aspects of an interpersonal relationship (e.g. liking versus disliking); Unconditionality refers to the variability of a person’s affective response to another; Congruence refers to the consistency of a person’s experience, as well as his or her overt communication with another; and Willingness-to-be-Known refers to the degree to which a person is willing to allow his or her experiences and perceptions to be known to another person, according to the other person’s desire for this. Four of the five subscales, save for Willingness-to-be-Known, are based on Rogers’s (1957) theorized therapist-provided facilitative conditions. Moreover, the Supervisory Relationship Inventory is a modified version of the widely used Relationship Inventory created by Barrett-Lennard (1962) to assess client-reported therapist effectiveness (Zuroff, Kelly, Leybman, Blatt, & Wampold, 2010). Each item of the Supervisory Relationship Inventory is rated on a 6-point Likert scale ranging from I strongly feel it is not true (1) to I strongly feel it is true (6), with some items of the scale requiring reverse-coding so that a 6 indicates “most facilitative” and a 1 indicates “least facilitative” across all items. The Supervisory Relationship Inventory has been found to possess strong convergent, discriminant, and internal validity (Schacht, 1986; Schacht et al., 1988, 1989). Cronbach’s alpha coefficient has been reported by past studies using this instrument, α = .95 (Dalton, 1983), α = .92 (Schacht et al., 1988), and α = .93 (Culbreth & Borders, 1999). The Cronbach’s alpha for the Supervisory Relationship Inventory in this study was found to be comparable to past studies, α = .96.
Additional explanatory variables. Additional variables included in the survey were chosen based upon past research as well as upon insight obtained by consulting with clinicians and clinical supervisors currently working in the field. The variables include the length of time at current job, work in a community setting, work in the mental health field, clinical work primarily involving direct client contact and primarily involving direct traumatized client contact, client caseloads with developmental trauma (i.e., childhood physical/sexual trauma), and client caseloads with episodic trauma (event-based trauma, such as an automobile accident, rape, or combat trauma). In addition, professional experience (number of years working in the social work profession), and respondent personal anxiety and trauma history were assessed. Additional supervision variables included the gender of the clinical supervisor, the frequency of supervision, length of time with current supervisor, extent of past supervision, and satisfaction with current supervision.
Demographic and control variables. Based on previous research (e.g. Bride & Kintzle, 2011; Schacht et al., 1989; Shah, Garland, & Katz, 2007), the following demographic/control variables were obtained in the survey: social worker age, gender, race/ethnicity, and personal income.
Missing data
Among the 107 respondents in the final dataset, the percent of missing data was extremely low both within the two psychometric instruments and in the dataset overall (i.e., less than 1%, respectively). Because percent of missing data was so low, and no discernible pattern in the missing data was found, item-mean substitution was performed, which replaces a missing cell with the mean value for the variable across all observations. This procedure is considered appropriate for dealing with missing data when the percent of missing data is very low and distributed randomly (Roth, Switzer, & Switzer, 1999).
Statistical methods
Data preparation was performed using SAS software, version 9.4 (SAS Institute, Cary NC). Multicollinearity diagnostics, summary statistics, multinomial confidence intervals, variable selection procedures, and model selection/diagnostics were obtained/performed using the statistical software R 3.2.3, which included the additional packages: “perturb,”, “cars”, “boot”, “leaps,” and “DescTools” (Canty & Ripley, 2014; Fox & Weisberg, 2011; Hendrickx, 2012; Lumley, 2009; Signorell, 2017).
Multicollinearity diagnostics
Prior to analysis, the data used in this study were assessed for problems of multicollinearity using methods for detecting and removing multicollinearity from data, outlined by Belsley, Kuh, and Welsch (2005) and Friendly and Kwan (2009).
Model selection procedures
The primary focus of this study was to obtain a best fitting model (i.e., a subset of variables) which predicts STS among clinical social workers who are likely to be receiving consistent supervision, as described earlier. The best subset selection procedure using the branch-and-bound algorithm was used to obtain subset model candidates. When the number of variables is not too large, the branch-and-bound algorithm provides an efficient means of performing an exhaustive search for minimum variance models across all possible (i.e., 2p−1) subsets of variables (Kutner, Nachtsheim, Neter, & Li, 2005).
Choosing best subsets. Best subsets of variables were found using the Akaike and Bayesian Information Criteria (i.e., AIC and BIC, respectively). The minimum of each criterion statistic is considered to be a best-model candidate. An F-test for model reduction (i.e., extra sums of squares F-test) was used to choose between the models with the smallest AIC versus smallest BIC statistics (Kutner et al., 2005).
“Always included” variables. Five variables, four categorical and one continuous, were chosen to be “always included” in all model subsets. These particular variables, gender, race/ethnicity, income, supervision frequency, and caseload trauma, were chosen due to theoretical considerations (Chatterjee & Hadi, 2006; Kutner et al., 2005). The first three variables, gender, race/ethnicity, and income, were chosen due to their demographic importance. Studies examining STS frequently fit regression models starting first with these demographic variables (e.g. Bride & Kintzle, 2011). Since this study examines the association between secondary trauma and the supervisory relationship, supervision frequency was chosen to be in all models in order to obtain subsets of variables most predictive of STS after controlling for frequency of supervision. Finally, the extent that respondents’ caseloads were reported to be traumatized (i.e., caseload trauma) was chosen to always be included due to the theoretical framework of secondary trauma. Secondary trauma is hypothesized to occur as a result of working with traumatized client populations (Ludick & Figley, 2017).
Results
Table 2 displays descriptive statistics for demographic and other key variables in the current study. In brief, nearly 92% of the respondents in the study were female with a mean age of approximately 36 years, M = 35.53, SD = 10.27; 69% were White and 24% were African American; the majority of respondents earned between $35,000 and $45,000 per year; the mean amount of social work experience reported was approximately seven years, M = 6.82, SD = 6.66; and the average number of hours respondents reported working per week was about 40 hours, M = 40.32, SD = 8.34. Approximately 77% of respondents reported receiving weekly or biweekly clinical supervision. The average respondent’s client caseload size was approximately 23 clients, M = 22.67, SD = 18.62, with the mean extent of caseload trauma falling between moderately and severely on a 5-point Likert scale, M = 3.31, SD = .96. In addition, the mean reported personal anxiety of respondents was mild to moderate, M = 2.69, SD = .98, while 71% of respondents reported one or more personal lifetime traumatic experience(s).
Descriptive statistics for demographic and other key variables.
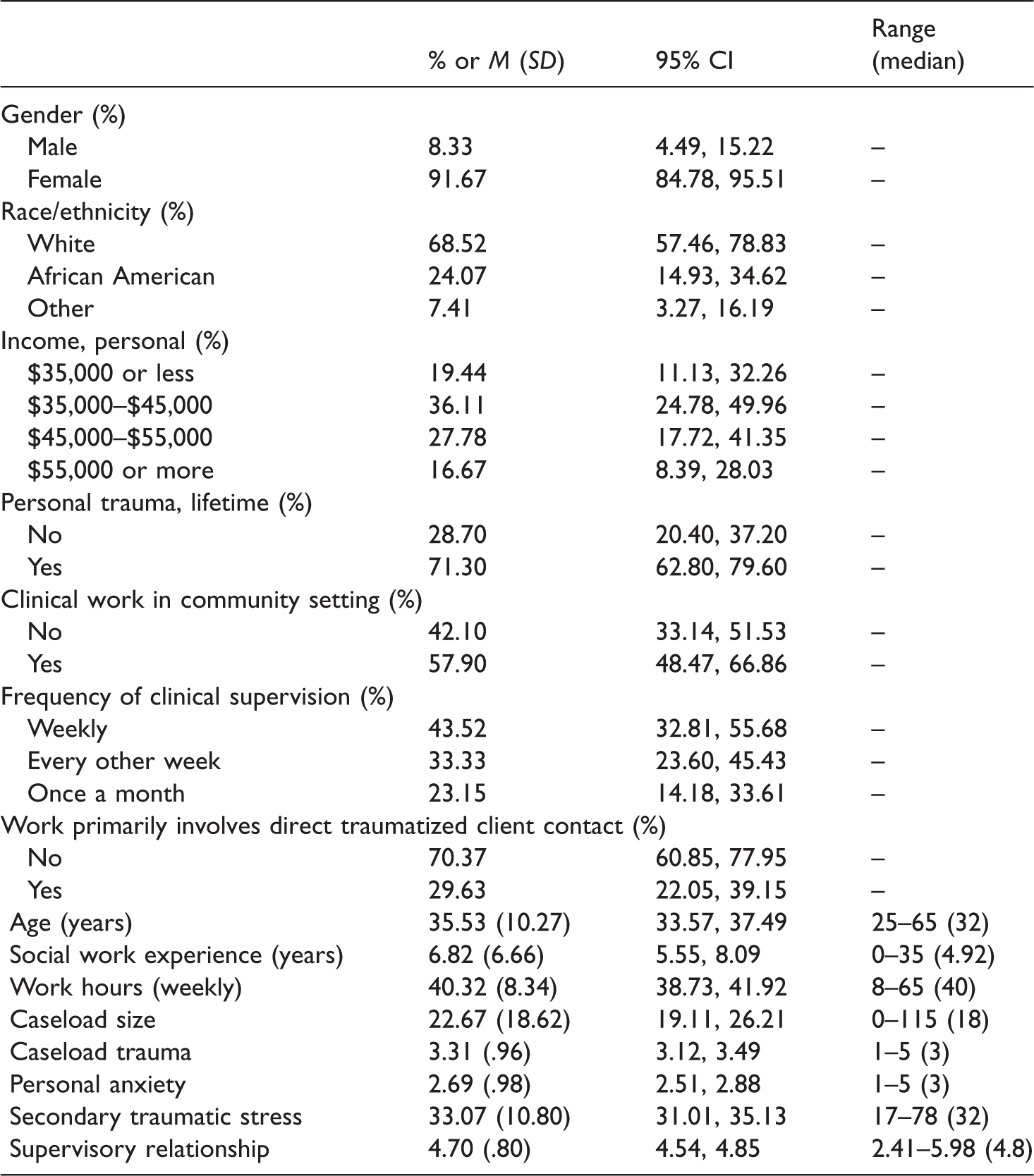
N = 107; 95% CI’s for categorical variables calculated using the Goodman method.
Overall, respondents endorsed modest levels of STS symptoms, M = 33.07, SD = 10.80, consistent with previous studies using the STSS scale (Bride, 2007; Kintzle et al., 2013). Based upon previous recommendations (Bride, 2007), the prevalence of diagnostic levels of STS in the current study can be assessed by using an algorithm in which an individual is considered to have a diagnostic level of STS if he or she endorses at least one item on the Intrusion subscale of the STSS, at least three items on the Avoidance subscale, and at least two items on the Arousal subscale. A symptom endorsement is considered a rating of three or more on an STSS item (Bride et al., 2009). Using this algorithm, 74% of respondents met diagnostic criteria on the Intrusion subscale, 32% on the Avoidance subscale, and 44% on the Arousal subscale. Moreover, 80% of respondents met diagnostic criteria on at least one of the three STS symptom clusters and 47% met criteria on at least two STS clusters. The overall prevalence of STS in the sample was found to be 22% of respondents; and among respondents who reported direct traumatized client contact being their primary work, the prevalence was 31%.
Furthermore, among all respondents the most frequently reported symptoms were (1) thinking about working with clients when not intending to, 60.53%, (2) being easily annoyed, 42.11%, (3) having trouble sleeping, 40.35%, (4) having trouble concentrating, 39.47%, (5) wanting to avoid working with some clients, 37.72%, and (6) feeling emotionally numb, 35.96%. The symptoms least reported were (1) disturbing dreams about work with clients, 14.91%, (2) reliving trauma(s) experienced by clients, 15.79%, and (3) noticing gaps in memory about client sessions, 16.67%. These figures are slightly higher than previously reported symptom frequencies (Kintzle et al., 2013).
In addition, the average supervisory relationship rating suggests a generally positive supervisory relationship as perceived by respondents, M = 4.70, SD = .80. This mean rating indicates that respondents tended to rate characteristics about the supervisory relationship as, “I feel it is probably true, more true than untrue.” Previous studies report similar mean ratings for the supervisory relationship (Culbreth & Borders, 1999; Schacht et al., 1989).
Model selection
Results from the best subsets model selection procedure are reported in Tables 3 and 4.
Best subsets selection final results showing model fit and selection criteria.
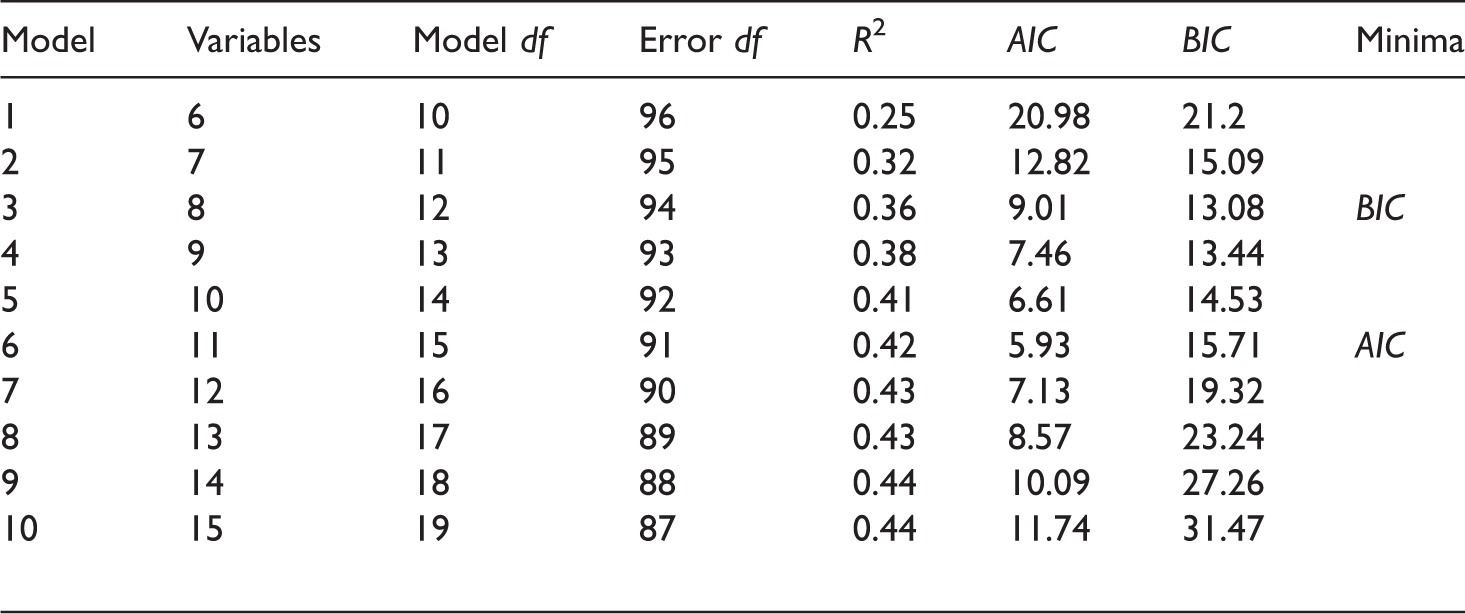
df: degrees of freedom; AIC: Akaike’s Information Criterion; BIC: Bayesian Information Criterion.
Shading indicates the final model selected after the F-test for reduction was performed comparing the minimum AIC model with the minimum BIC model; N = 107.
Final model predicting secondary traumatic stress displaying ordinary least squares estimates.
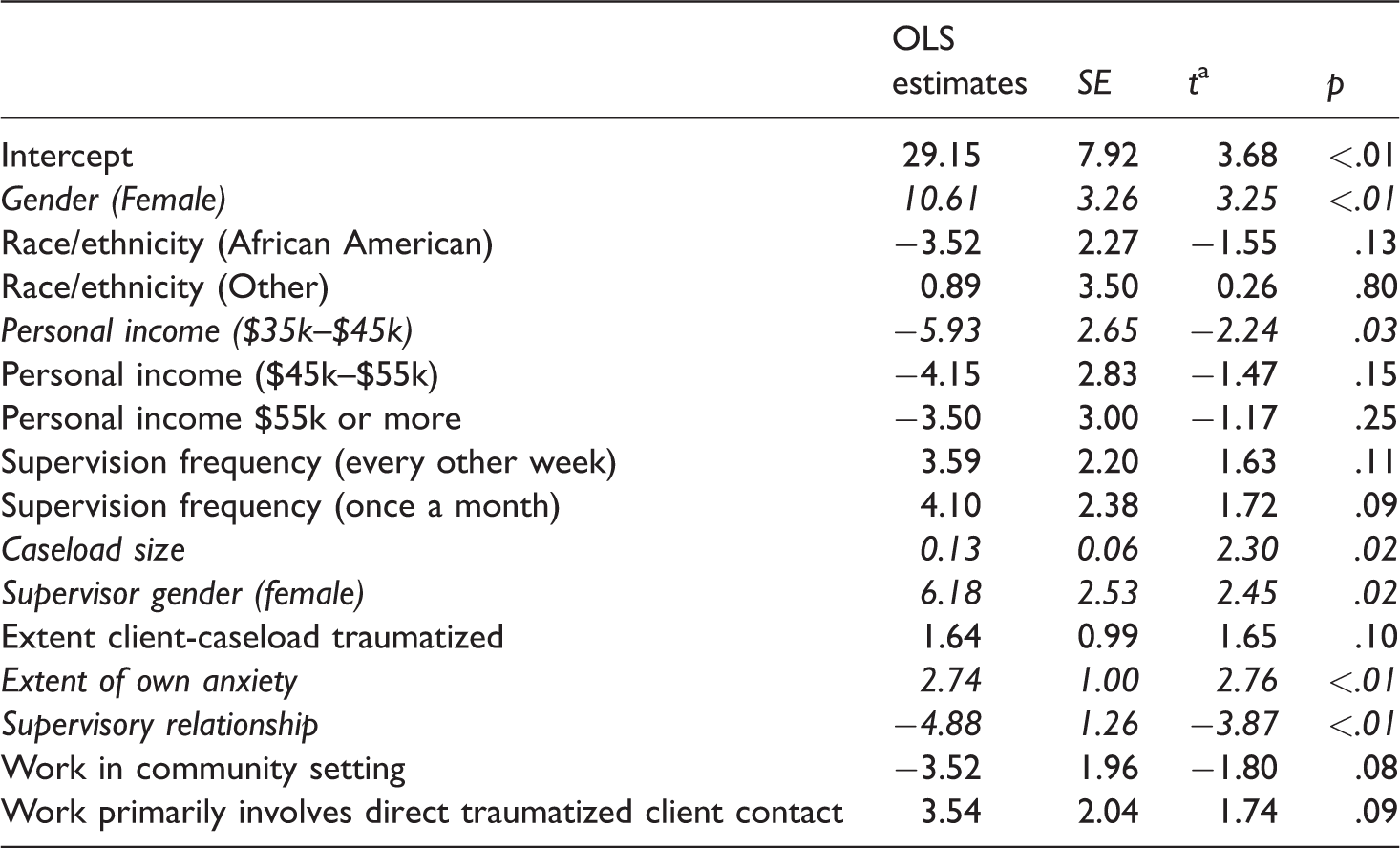
OLS: ordinary least squares.
at test degrees of freedom = 91; N = 107; Variables found to be statistically significant displayed in italics.
Best subsets
Table 3 displays the results of the best subsets exhaustive search procedure. Model 6 with 11 variables and Model 3 with eight variables possessed the minimum criteria, AIC = 5.93, and BIC = 13.08, respectively. Model 3 is a subset of Model 6, and therefore can be tested for further reduction. An F-test for model reduction was performed, with a null hypothesis that the additional variables contained in Model 6 were equal to zero, and therefore Model 3 would be considered equivalent as well as more parsimonious. However, the F-test was significant, and therefore the larger AIC Model 6 was chosen, F(3, 91) = 3.66, p = .02. The 11 variables in the final model, R2 = 0.42, are displayed in Table 4 with their ordinary least squares (OLS) coefficient estimates, standard errors, Student t-values, and p-values. The final variables were: Gender, Race/ethnicity, Personal income, Supervision frequency, Caseload size, Supervisor gender, Extent client-caseload traumatized, Extent of own anxiety, Supervisory relationship, Work in community setting, Work primarily involves direct traumatized client contact.
Regression diagnostics. According to the guidelines provided by Chatterjee and Hadi (2006), the final model was assessed for normality and constant variance of the residuals, as well as for influential and leveraged observations. The final model in Table 4 was found to satisfy the above diagnostic criteria.
Regression coefficients
Table 4 provides OLS estimates which indicate both the directional relationship of each explanatory variable with the response variable, as well as the magnitude and statistical significance of each in predicting STS. Many of the variables in the final model appear to have significantly impacted the incidence of STS. Statistically significant OLS estimates will be reported using a significance cutoff of α = .05.
Female respondents and respondents possessing female supervisors both significantly predicted an increase in STS, b = 10.61, t(91) = 3.25, p < .01, and b = 6.18, t(91) = 2.45, p = .02, respectively (92% of respondents were female, and 84% of respondents reported having female supervisors). However, the over-representation of female respondents and female supervisors in this study makes the above results difficult to interpret. Moreover, compared to respondents reporting personal incomes of $35,000 or less—which was the reference-level category—respondents reporting incomes between $35,000 and $45,000 per year possessed significantly lower STS scores, b = −5.93, t(91) = −2.24, p = .03. The magnitude of the regression coefficient suggests that when all other variables are held constant, the STS level in respondents earning between $35,000 and $45,000 would be 5.93 units lower, as compared to respondents earning $35,000 or less. In addition, client caseload size was significant, b = 0.13, t(91) = 2.30, p = .02, indicating that when all other variables are held constant, a unit increase in caseload size (i.e., one client) increased STS by 0.13. While this effect seems small, if a clinician were to receive a 10-client or 20-client increase to his or her caseload, the results suggest that STS would increase by 1.3 and 2.6, respectively, which may be a substantial increase for a given clinician. In addition, the extent that a respondent experienced anxiety also significantly predicted an increase in STS, b = 2.74, t(91) = 2.76, p = <.01, indicating that a unit increase in anxiety level could result in a 2.74 increase in STS. Finally, the supervisory relationship was highly significant, b = −4.88, t(91) = −3.87, p < .01, indicating that a unit improvement in the quality of the relationship could lower STS by 4.88 units.
Taking the above results into perspective, STS was assessed using a 17-item instrument with each item rated on a Likert scale from 1 to 5. Therefore, a two-unit increase in STS suggests that a clinician could go from feeling that he or she never experienced a particular symptom to occasionally; or from rarely to often. Likewise, a five-unit decrease in STS, such as what was found for a one-unit increase in the level of the supervisory relationship, suggests that a clinician could go from very often experiencing a symptom to never, which is a substantial reduction in symptomatology.
Finally, the extent that respondent caseload was traumatized, b = 1.64, t(91) = 1.65, p = .10, working in a community setting, b = −3.52, t(91) = −1.80, p = .08, and work primarily involving direct client-trauma contact, b = 3.54, t(91) = 1.74, p = .09, were each found to be statistically nonsignificant, though the latter two coefficients were relatively large. Likewise, supervision frequency was not found to be significant, although compared to respondents who received weekly supervision, respondents receiving biweekly and once-a-month supervision possessed relatively large, positive coefficients predicting STS, b = 3.59, t(91) = 1.63, p = .11, and, b = 4.10, t(91) = 1.72, p = .09, respectively.
Discussion
As described earlier in this article, in light of the generally mixed findings reported by studies examining risk and protective factors thought to reduce the occurrence of STS among helping professionals, this study sought to develop a model that optimally predicts STS among masters-level clinical social workers. Using previous research, as well as clinical insight obtained from clinicians and supervisors in the field, this study was designed to obtain a large number of variables relevant to clinical social workers’ experiences practicing in the field. An exhaustive search regression analysis obtained a set of variables that possess a strong likelihood of best predicting STS among the larger candidate set of variables. After accounting for the effects of demographic/control variables, including gender, race/ethnicity, income, supervision frequency, and caseload trauma, a small set of factors were found to optimally predict STS, explaining 42% of STS among social workers. As displayed in Table 4, these factors included (a) supervisor gender, (b) the extent that a clinician’s caseload possessed trauma symptoms, (c) the level of the clinician’s personal anxiety, (d) the clinician’s rating of his or her supervisory relationship, (e) clinical work in a community setting, and (f) clinical work that primarily involves direct traumatized client contact. Furthermore, among the above variables, those that were found to be statistically significant were gender, personal income, caseload size, supervisor gender, personal anxiety, and the supervisory relationship. However, the results for gender and supervisor gender are difficult to interpret due to an extremely high frequency of female respondents and female supervisors found in this study.
The supervisory relationship
In the current study, the supervisory relationship was found to be a statistically significant inverse predictor of STS. Specifically, higher aggregated levels of supervisor empathy, unconditional positive regard, congruence, and willingness-to-be-known, as perceived by the supervisee, was found to significantly predict lower STS scores after accounting for the effects of the other factors in the regression model. This finding suggests that a clinical supervisor who can provide a genuine, open, understanding, and accepting environment for the supervisee, as operationalized earlier in this article, may contribute an important protective factor for reducing secondary trauma symptoms among clinical social workers. This finding supports previous research which found supervision to significantly reduce STS among clinical workers (Slattery & Goodman, 2009). In contrast, supervision frequency was not found in the current study to significantly predict STS, which is consistent with previous research (Dworkin et al., 2016; Ivicic & Motta, 2016). However, the trend suggests that less frequent supervision (e.g., biweekly and once-a-month) may be related to increased levels of STS.
Personal income
In addition, personal income was found to significantly predict STS, suggesting that social workers whose salaries fell in the range of $35,000 to $45,000 experienced a 5-point reduction in their STS scores compared to their counterparts earning less than $35,000. Surprisingly, a review of the literature suggests that the relationship between social worker income level and STS is rarely studied; though income, or socioeconomic status, is considered to be an important factor that predicts STS (Lerias & Byrne, 2003; Sabin-Farrell & Turpin, 2003; Shah et al., 2007).
Caseload size
Moreover, an increase in caseload size was found to significantly increase STS (the average caseload was 23 clients). Previous research reporting the relationship between caseload and STS have been mixed, with some reporting a significant positive relationship with STS, and others nonsignificant (Bride & Kintzle, 2011; Dworkin et al., 2016; Kulkarni et al., 2013). In particular, Bride and Kintzle’s (2011) nonsignificant results could have been due to outliers in the data that may have influenced the regression model fit (e.g., the authors reported an average caseload size of 34.58 with a standard deviation of 47.05, and a maximum caseload of 400 clients reported; Kutner et al., 2005).
Personal anxiety and past trauma history
Personal anxiety was also found to significantly increase STS in the current study, with an average level of social worker anxiety falling between mild and moderate. This finding also supports previous research suggesting that a clinician’s own experience of anxiety may contribute to the development of STS (Ewer et al., 2015). Notably, past lifetime trauma history, endorsed by 71% of social workers in this study, did not remain in the optimal regression model, suggesting that trauma history did not account for occurrence of STS among respondents in the sample (in particular, the mean STS score for social workers with a past trauma history was equivalent to those without a history). This latter finding is surprising given that a number of studies on secondary trauma among counselors have found a significant relationship between past trauma history and STS (Dworkin et al., 2016; Nelson-Gardell & Harris, 2003; Pearlman & Mac Ian, 1995). A possible explanation may be that when a number of potential factors for predicting STS are analyzed, the effects of certain related factors may dilute the impact of past trauma on STS.
Secondary trauma symptom severity
Similar to the prevalence rate from previous studies (Bride, 2007; Bride & Kintzle, 2011; Ivicic & Motta, 2016), the current study found that nearly 80% of social workers reported mild STS symptom severity, 47% reported moderate STS severity, and 22% reported full STS severity. However, in contrast with the commonly held theoretical framework which hypothesizes that STS is expected to occur as a direct result of exposure to traumatized-client work, in the current study this hypothesis was not supported. Although the measure of respondent-reported traumatized-client caseloads was positively associated with STS, it failed to reach statistical significance at or below a 5% probability level. In addition, a second variable that indicated whether or not the respondents worked primarily in direct contact with traumatized clients was also positively associated with STS, but failed to be statistically significant as well (among the sample of clinical social workers surveyed in this study, approximately 30% indicated that their work primarily involved direct contact with traumatized clients). This finding supports previous research suggesting that other factors may also account for STS symptoms among clinicians (Devilly et al., 2009).
Work setting and client trauma type
Finally, variables measuring clinical social work in a community setting versus a non-community setting, as well as type of client trauma (i.e., developmental versus episodic) were found to be nonsignificant in the regression model. However the fact that these variables as well as the client trauma exposure variables remained in the optimal model found to predict STS suggests that these variables may be important in future research and in understanding STS among social workers in this study (Kutner et al., 2005).
Overall, this study’s findings suggest that in addition to exposure to traumatized clients, other factors may contribute to the incidence of STS among clinical social workers. The results from this study suggest that positive ratings of clinical supervision, higher income levels, smaller client caseloads, and a reduction of personal anxiety may decrease secondary trauma symptoms among clinical social workers. Furthermore, these findings may have substantial implications for practice and future research.
Practice recommendations, future research, and limitations
Practice recommendations
The findings reported in this study suggest a number of recommendations for social work practice. At an administrative/policy level, the results suggest that providing clinical social workers poor-quality clinical supervision, providing low salaries, and assigning them large client caseloads may increase the risk of social workers developing secondary trauma symptoms. Given the high costs of providing health insurance to employees, as well as increased employee turnover and lost productivity due to STS and subsequent burnout, administrators may be able to reduce financial losses in the long run by providing skilled clinical supervision to clinical social workers, awarding larger salaries, and encouraging reasonable client caseloads, particularly to those social workers that primarily work with traumatized clients. At an individual level, the results suggest that social workers experiencing anxiety may possess an increased vulnerability to developing STS. Personal self-care to reduce daily anxiety levels may be important to protect clinical social workers from developing STS symptoms. Likewise, administrators can also play a role by providing free or reduced-cost stress-relief activities for their employees, including an Employee Assistance Program (EAP).
Future research
This study is one of few that examine, in particular, the impact of the supervisory relationship as a predictor of secondary trauma among clinical social workers. Further investigation of how the supervisory relationship, as well as other aspects of social workers’ work experiences, impact STS are needed in order to build an evidence base with the potential to affect positive change in the workplace as well as at the policy level. Future research should address the extent that the supervisory relationship mediates and moderates the hypothesized causal pathway between exposure to client trauma and the occurrence of STS. In addition, research should examine the positive benefits of providing workplace anxiety-reduction programs (e.g., yoga and other forms of stress-reduction activities provided in the workplace, or at reduced cost outside the workplace, may be a productive starting point for this type of research).
Limitations
This study possessed a number of limitations. First, the survey response rate was relatively low—though comparable to similar studies examining STS. Social workers who did not respond to the survey may possess qualitatively different characteristics compared to the respondents. For example, social workers with higher levels of STS may have been more likely to respond because the survey possessed personal meaning to them. In contrast, avoidance of trauma-related stimuli is a cornerstone of typical trauma symptoms and, therefore, social workers with higher levels of trauma may have been more likely not to respond. In addition, the sample of social workers in this study was selected based on increasing the chances of obtaining respondents who were currently receiving clinical supervision. As a result, the sample may not be representative of the population of social workers who experience secondary trauma. Another limitation was that the data was cross-sectional in nature and therefore limits the ability to draw inferences regarding causal pathways between exposure and trauma, as well as between the supervisory relationship and other variables, and STS. Finally, this study attempted to obtain a best subset of predictor variables from a relatively limited number of candidate variables. Other factors which are important to understanding STS may have been overlooked in the current survey.
Conclusion
This study sought to develop a predictive model of STS by examining a large number of potential candidate explanatory variables suggested for consideration by past research as well as by clinical insight obtained from current clinicians and supervisors in the field. A best predictive subset of variables was obtained by performing a rigorous variable-selection statistical procedure. The findings suggest that the supervisory relationship, salary, caseload size, and personal anxiety may be salient factors that impact the extent to which clinical social workers develop secondary trauma symptoms. In particular, positive ratings of supervision and higher income level were found to predict a substantial decrease in the degree to which a social worker possessed secondary trauma symptoms. The quality of the supervisory relationship, as well as salary, may be an important aspect in protecting social workers from developing STS.
Footnotes
Ethics
Ethical approval for this project was given by the University of Georgia Institutional Review Board [ref number 2013109290].
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.