
Abstract
Summary
In light of Head Start’s recent move toward longer program implementations, the current study examined whether the duration of Head Start enrollment impacts outcomes for parents: parental involvement in school, perceived helpfulness of social support, and use of formal social services.
Findings
Linear mixed model analyses examined whether parental outcomes differed depending on the number of years enrolled in Head Start. Parents whose child enrolled more years in Head Start were more likely to participate in their children’s schools and received more helpful social support than those whose child enrolled in fewer years of Head Start. No difference was found for formal social service use depending on longer duration of Head Start enrollment. Minority status, household risk factors, and non-English speaking were negatively associated with parental outcomes.
Applications
Early intervention programs, such as Head Start, should recruit eligible low-income families earlier for longer participation on family-focused programs.
Keywords
Head Start began as an eight-week summer program in 1965, after Lyndon B. Johnson declared the War on Poverty. The purpose of the Head Start program is to support the cognitive, social, and emotional growth of young children in low-income families in order to promote school readiness. Recent studies suggested that Head Start’s impacts are more pronounced when children attended at an earlier age (Jenkins, Farkas, Duncan, Burchinal, & Vandell, 2016; Kline & Walters, 2016; Love et al., 2005; Mathematica Policy Research, Inc., 2011; Puma, Bell, Cook, & Heid, 2010; Raikes et al., 2006), for a longer hours and weeks per year (Loeb, Bridges, Bassoka, Fuller, & Rumberger, 2005), and for multiple years of enrollment duration (Wen, Leow, Hahs-Vaughn, Korfmacher, & Marcus, 2012). Due to the positive impact of variously defined Head Start dosage on children, after years of renovation and policy changes, Head Start is moving toward a full-day, full-year program serving approximately 1 million young children per year, totaling more than 30 million children since Head Start’s inception. Head Start emphasizes parental roles. Accordingly, the program includes the support, education, and resources for parents. Despite the general consensus about Head Start’s positive impact on children, the benefits of Head Start on parents are less known. In the context of Head Start’s recent initiatives emphasizing longer exposure for participants, the purpose of the current study is to examine whether longer years of Head Start experience (dosage defined by number of enrollment years) has a positive impact on parental outcomes.
Head Start’s emphasis on family components
Head Start was established based on ecological theory (Bronfenbrenner & Morris, 1998), which proposes that child development is influenced by complex systems that interact within the child’s environment, including proximal influences within the microsystem (e.g., family, school), the macrosystem (e.g., parent–school interactions), and the exosystem (e.g., social services). Head Start’s unique approach is to encourage active family participation. According to Head Start Program Performance and Standard, a program must address needs of families and integrate parent and family engagement strategies into all systems and program services to support family well-being, which in turn could promote children’s learning and development. Given the opportunities for and advantages of parental involvement in children’s development, the National Head Start Association (NHSA) has named parental roles as major components of Head Start’s mission.
Parental involvement
Head Start organizations strive to provide education and support to parents of preschoolers attending their programs to facilitate parent engagement in their children’s learning (Hindman, Miller, Froyen, & Skibbe, 2012; McWayne, Campos, & Owisianik, 2008). Head Start’s ecological model focuses on parental roles in children’s education. Accordingly, the Head Start Program Performance Standards (2016) mandate that Head Start should provide family-focused programs to enhance family engagement, promote parental activities, and build family partnership. The Head Start program holds regular parent–teacher conferences and calls for parental involvement by volunteering in school programs. Thus, Head Start parents can become involved in their children’s school through observing and volunteering in the child’s classroom, attending program or parent meetings, and attending classroom meetings (Castro, Bryant, Peisner-Feinberg, & Skinner, 2004; Hindman et al., 2012). Further, Head Start programs offer family workshops and education service by working together with parents. This is to ensure that they have the means to obtain health insurance, services for children with disabilities, adequate housing, job training, and adult education for parenting skills. During 2013–2014, Head Start had approximately 1,167,000 volunteers from families (800,000) and communities (367,000). Additionally, more than half of Head Start families (513,498 families) participated in parental education programs offered by Head Start. Among 259,000 Head Start program employees, parents of current or former Head Start children made up 23% of Head Start staff (US Department of Health and Human Services [DHHS], Office of Head Start, 2016).
Social support
Head Start programs promote family connections with peers and community to facilitate networks and group activities that support families’ strengths, interests, and needs. For example, Head Start includes parents as active participants in policy councils and other community opportunities to share skills, culture, and talents. Thus, Head Start supports families in identifying, developing, and utilizing informal and formal support networks (e.g., neighborhood groups, faith/spiritual communities, civic organizations). Parental social support and informal help seeking potentially benefits parents, and in turn, benefits their children. When mothers of preschool-age children received greater social support; at work, from neighbors, and through friends and families, they reported decreased depressive symptoms, and decreased work and family role strain (Goldberg, Breenberger, Hamill, & O’Neil, 1992). Social support has also been linked with a woman’s likelihood to seek outside help for distressing situations such as domestic violence (Leone, Johnson, & Cohan, 2007). Research examining the link between parental social support and child outcomes suggests that when a parent has greater social support, children show decreased internalizing and externalizing behaviors (de Leon Siantz & Smith, 1994; McConnell, Breitkrez, & Savage, 2012; Stacks & Goff, 2006; Taylor, Conger, Robins, & Widman, 2015) and academic outcomes (Cutrona, Cole, Colangelo, Assouline, & Russell, 1994; Hindman & Morrison, 2011; Melson, Ladd, & Hsu, 1993; Wang & Eccles, 2012).
Social services
Low-income families are also eligible to use formal social services due to their risk factors (e.g., financial uncertainty, lack of education, single parenthood, unemployed). However, low-income families may experience barriers to accessing formal social services due to lack of knowledge about available resources (Farmer et al., 2001), remote geographic and space conditions (Kissane, 2010), and other logistical difficulties (Lamb-Parker et al., 2001). One of Head Start’s family and community partnership components is to provide and refer available social services, facilitating access to community resources (e.g., health, mental health, nutrition, financial literacy, education, domestic violence, substance abuse treatment, child welfare services).
Head Start’s policy changes toward longer enrollment duration
In 2015, Head Start preschool services were provided mostly in center-based settings (96%) that vary in the number of days per week and hours per day. The center-based Head Start program consisted of various types of programs offering four or five days/week, with half-day or full-day options. Overall, Head Start has offered shorter duration than other center-based care programs subsidized by the Child Care Development Fund. In 2014, children three or four years old attended other center-based child care an average of 163 hours per month, approximately 2000 hours per year (US DHHS, Administration for Children and Families (ACF), Office of Child Care, 2015). Recently, Head Start has begun to offer longer duration of enrollment. New Head Start standards require that classes operate four or five days per week, with a minimum of 3.5 hours and maximum of 6 hours per day, with four hours being optimal: offering at least 1020 annual hours for preschoolers with a minimum of 32 weeks of scheduled days of class operations over an eight- or nine-month period.
Young children increasingly attend Head Start programs at an early age and enroll for a longer duration. According to the Annual Head Start’s Program Information Report (US DHHS, ACF, Office of Head Start, 2016), among all Head Start enrollees during 2014–2015 (941,418), 26.5% children enrolled in Head Start (including Early Head Start) for the second year and 5.2% children enrolled for the third year. Head Start enrollees are becoming younger. In 1980, 21% of children enrolled were five years of age and older, 55% of children were four years old, and 24% of children were three years old. Children under the age of 3 were not eligible. In 2014–2015, possibly as a result of Early Head Start, 17.5% of children enrolled were under three years of age, 36% were three years old, 44% were four years old, while only 1% were five and older.
The Head Start Impact Study (Puma et al., 2010) and the Head Start Family and Child Experience Survey (Mathematica Policy Research, Inc., 2011) found that Head Start’s impact on academic and health outcomes was more significant for children who entered at age 3 than at age 4. The National Early Head Start Research and Evaluation Study (Love et al., 2005) and other evaluation studies (Jenkins et al., 2016; Kline & Walters, 2016; Raikes et al., 2006) reported that earlier entry to Head Start had a positive impact on outcomes for children. Other studies suggest that children who attended more years of Head Start (Wen et al., 2012) or other enhanced preschool programs (Domitrovich et al., 2013; Magnuson, Ruhmb, & Waldfogel, 2007; Reynolds, 1995) had higher performance on academic outcomes than those who attended for one year. Longer durations of preschool attendance (Behrman, Cheng, & Todd, 2004) and extensive dosage intervention (Zhai et al., 2010) were positively associated with children’s outcomes. Loeb et al. (2005) also found that children who attended center-based care for an earlier age (ages 2–3), longer hours (15–30 hours/day), and longer months per year (nine months or more) had higher reading and math scores and fewer behavioral problems at kindergarten age.
Despite various dosage effects of Head Start on children’s outcomes, its impact on parental outcomes has received less attention. A previous study (Ritblatt, Brassert, Johnson, & Gomez, 2001) found that, independent of demographic differences, parents of children who attended Head Start for two years were more likely to read to their preschoolers than parents in families attending for one year. The Head Start Impact Study also found that mothers of Head Start children who enrolled at age 3 read more books to their children than those who enrolled at age 4 (Love et al., 2005). According to Head Start Impact Study final reports (Puma et al., 2010), Head Start impacts on other parenting outcomes were greater for parents whose children enrolled at age 3 than at age 4. Further, Head Start increased the likelihood that parents read to their children and engage in cultural enrichment activities by the end of the Head Start year. Thus, prolonged exposure to Head Start services may be associated with improved parenting skills.
Head Start emphasizes the importance of parental outcomes by promoting parental involvement, connecting family and community networks, and facilitating social service use. Parental outcomes have the potential to play a role in child outcomes. Low-income families face barriers to involvement in schools and experience difficulty establishing social networks and access to social services. Further, in Head Start’s recent initiatives to extend program hours (toward full-day full year) and strong emphasis on family and community engagement, it is important to consider parental factors when studying Head Start dosage. The current study intends to examine dosage effects on parental outcomes by considering the duration of enrollment in Head Start, including years enrolled in Early Head Start.
Methods
Target sample
In 2002, the Head Start Impact Study examined a nationally representative sample of 84 grantee/delegate agencies, including 4442 newly entering, eligible three- and four-year-old children (2449 and 1993), who were randomly assigned either to: (1) a Head Start group with access to Head Start program services (n = 2646) or (2) a control group that did not have access to Head Start but could enroll in other early childhood programs or non-Head Start services selected by their parents (n = 1796). Data collection began in fall 2002 and continued through 2006, following children from program application through the spring of their first grade year (US DHHS, ACF, Office of Planning, Research and Evaluation, 2010). Children who provided the primary focal care arrangements (n = 3785), Head Start (n = 2125), parental care (748), home based care (n = 270), and other center-based care (n = 637). Based on this, 2762 children were selected who enrolled in Head Start (n = 2125) and who enrolled other center-based care (n = 637). Children who were cared for by parents and home-based care were excluded from the current analyses due to lack of data on parental outcomes. This study was submitted for Institutional Review Board (IRB) review, following the guideline of the University Committee for Research involving Human Subjects. The IRB office determined this secondary data analysis study as nonhuman subject research since the data do not contain any identifiable personal information as defined by the DHHS [45.CFR.46.102(f)].
Measures
Years of Head Start enrollment (dosage of Head Start)
When children were five to six years old, data on previous experiences enrolling in Early Head Start were collected. Among 2125 Head Start children, 312 children enrolled in early Head Start for one year (11.2%), 784 children enrolled in early Head Start for two years (28.4%), and 1668 children did not enroll in early Head Start (60.4%). The final sample consists of four groups depending on enrollment duration of Head Start: never enrolled (0 year; n = 637), children who enrolled for two years (two years; n = 1031), children who enrolled for three years (three years; n = 310), and those who enrolled for four years (n = 784), with a total of 2762 children.
Parenting variables
Parental involvement
This measure is based on the parent interview where parents were asked how often they (1) volunteered or observed in the child’s classroom, (2) attended conferences, (3) attended parental meetings, (4) attended activities such as field trips, and (5) were involved in center planning groups. This question reflects the Head Start Program Performance Standard requirement that programs provide parents with opportunities to be involved in their child’s classroom and offer a variety of parenting education services. The current study used a computed score based on these five items. Parents answered either “Yes (coded = 1)” or “No (coded = 0)”. Then, a continuous variable was created (zero to five) to show how many of these activities the parent participated in (M = 2.4, standard deviation [SD] = 1.3, range = 0-5). The current study used this computed continuous variable. The reliability (Cronbach alpha) for the measure of parental involvement was <0.6 (Puma et al., 2010, chapter 7, p. 6).
Perceived helpfulness of social support
Parents were asked to rate how helpful the following individuals were: spouse, mother, father, grandparents, other relatives, friends, social workers, religious group, and others. For example, mothers were asked to rate from 1 (not very helpful) to 3 (very helpful) on questions such as “How helpful is your spouse/partner?” “How helpful has your mother been?” “How helpful are social workers?” “How helpful are religious/social group members?” Total scores were calculated by adding the perceived helpfulness rating for all resources (M = 9.2, SD = 4.5, range 0–24).
Formal social service use
Parents were asked whether they received any of the following services over the past year (1 = yes, 0 = no): income assistance, nutrition assistance, housing assistance, utilities, job training, alcohol/drug abuse, mental health services, family violence, and foster care payment. Total social service use scores were computed by adding all individual items (M = 0.50, SD = .87, range 0–7).
Baseline variables
Race for the primary caregiver (White, Black, Hispanic), bilingual speaking at home (English vs. non-English), and household risk index were included in the study. Household risk index was determined by the number of the following characteristics reported in the baseline parent interview: (1) receipt of Temporary Assistance for the Needy Families (TANF) or Food Stamps, (2) neither parent in household has high school diploma or a general education diploma (GED), (3) neither parent in household is employed or in school, (4) the child’s biological mother/caregiver is a single parent, and (5) the child’s biological mother was age 19 or younger when child was born. A total household risk index score could range from 0 to 5 points. Three categories were created: low/no risk (0–2 risk factors), moderate risk (3 risk factors), and high risk (4–5 risk factors). All baseline variables were measured when they were three to four years old.
Data analyses
Linear mixed model analyses were used to examine whether parental outcomes differ depending on the number of years enrolled in Head Start. After controlling for all baseline variables such as maternal race (reference group = Hispanic mothers), language speaking at home, and household risk (reference group = four to five risk factors), years of Head Start enrollment (reference group = enrolled for four years in Head Start) was entered into the model.
Results
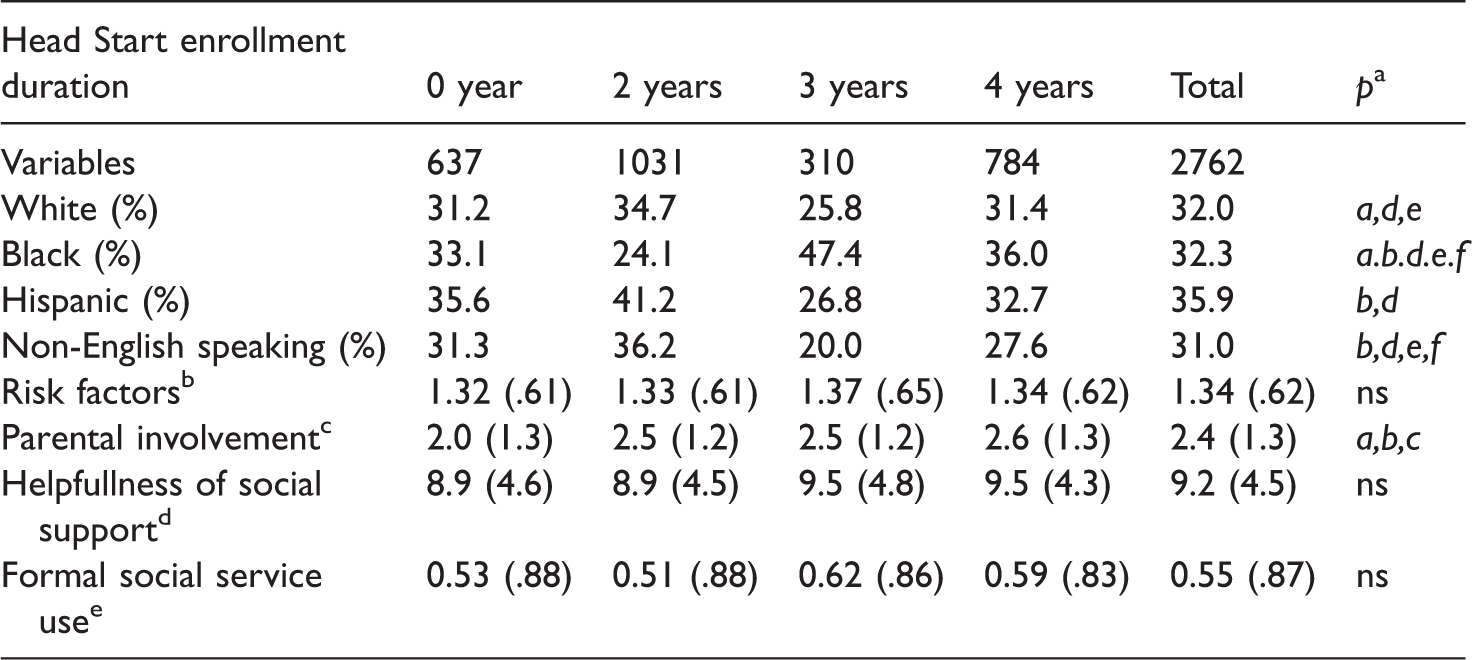
Table 1 shows the descriptive statistics for the variables used in the study. Black families tend to attend more years of Head Start and Hispanic families less years of Head Start. Families non-English speaking at home attended fewer years of Head Start than families speaking English at home. Parental who enrolled in more years of Head Start were more involved in their children’s schooling.
Descriptive statistics for variables included in the study.
a
bDetermined by (1) public assistance, (2) education, (3) employment, (4) single mother, and (5) teen mother. 1 = low/no risk (0–2 risk factors), 2 = moderate risk (3 risk factors), and 3= high risk (4–5 risk factors).
cNumber of parent participation in setting activities (range = 0–5).
dParents were asked how helpful for the following persons: spouse, mother, father, grandparents, other relatives, friends, social workers, religious group by rating from 1 (not very helpful) to 3 (very helpful) (range = 0–24).
eWhether parents received the following services (1 = yes, 0 = no), income assistance, nutrition assistance, housing assistance, utilities, job training, alcohol/drug abuse, mental health services, family violence, and foster care payment (range = 0–7).
Findings for dosage effects of Head Start on parental outcomes
As shown in Table 2, regression results indicate that compared to parents whose children enrolled in Head Start for four years, parents who had never attended Head Start participated significantly less in school activities (β = −.65, p < .001) and perceived less helpfulness of social support (β = −.58, p < .05). Parents of children who enrolled in Head Start for two years also participated less in school activities (β = −.23, p < .05) and perceived less helpfulness of social support (β = −.54, p < .10) than those who enrolled in Head Start for four years.
Result of estimate of fixed effects (standard error) predicting parental outcomes.
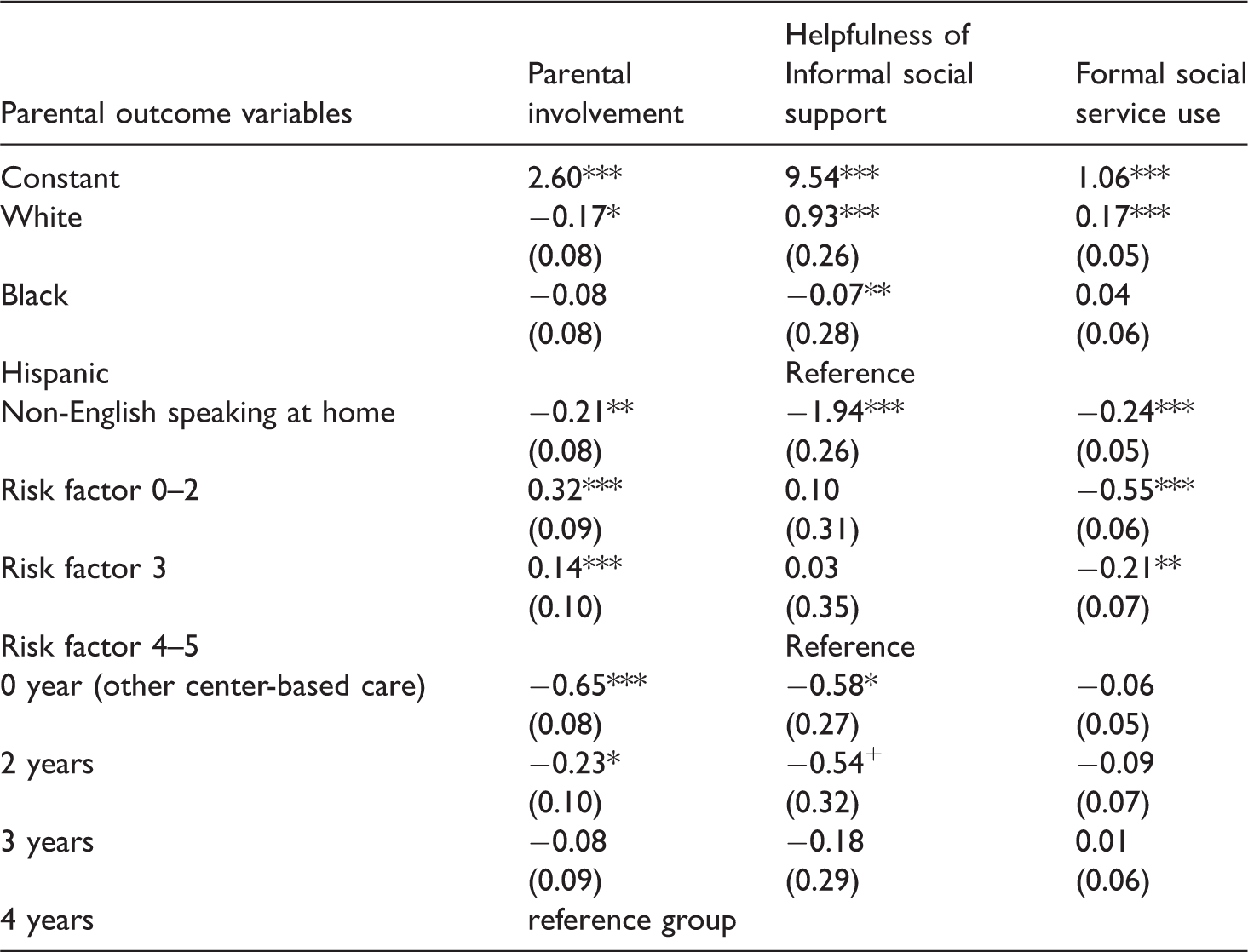
+p < .10. *p < .05. **p < .01. ***p < .001.
Compared to Hispanic parents, White parents participate less in school activities (β = −.17, p < .05), perceived more helpfulness of social support (β = .93, p < .001) and used more formal social services (β = .17, p < .001). Black parents perceived less helpfulness of social support (β = −.07, p < .001) than Hispanic parents. Compared to parents who speak English at home, non-English-speaking parents participated less in school activities (β = −.21, p < .01), perceived less helpfulness of social support (β = −1.94, p < .001), and used less formal social services (β = −.24, p < .001). Compared to parents who had four to five risk factors, parents with fewer household risk factors participated more in school activities (β = .32, p < .001; β = .14, p < .001) and used less formal social services (β = −.55, p < .001; β = −.21, p < .01).
Discussion
The current study found that more years of Head Start exposure show more positive parental outcomes. Compared to parents who enrolled their children in Head Start for four years, parents who did not participate in Head Start or those who participated just for two years were less likely to be involved in their children’s schooling (attending teacher conferences, volunteering in school activities, etc.). As shown in dosage effects of Head Start enrollment on children’s outcomes (Love et al., 2005; Mathematica Policy Research, Inc., 2011; 2010; Raikes et al., 2006; Wen et al., 2012; Zhai et al., 2010), parents enrolled more years in Head Start obtained positive outcomes. Head Start’s mission is to educate parents as teachers, so parents can fill a teacher’s role after exiting the program. Active parental involvement is associated with children’s academic and social–emotional outcomes (Hindman et al., 2012; Love et al., 2005). Parent involvement in children’s schooling reduced the negative effects of risk factors often experienced by Head Start families, such as single-parent status and limited neighborhood resources (Kingston, Huang, Calzada, Dawson-McClure, & Brotman, 2013).
Parents who did not participate in Head Start perceived social support as less helpful than those who participated for multiple years. Family and community engagement is Head Start’s unique strategy. Parents of children who enrolled in Head Start for multiple years tended to have more opportunities to connect to social networks. As Head Start connects families and communities through parental education, Head Start parents learn to find quality social networks. Parents who enrolled their children in Head Start for only two years perceived less helpful social support than those who participated for more years. It takes time to connect quality social networks among low-income parents. Head Start offers intervention for parents (parent education and workshops) on a monthly basis. Policy councils or parent committees meet less frequently. Only half of Head Start parents participate in parental education programs (US DHHS, ACF, 2016). Opportunities to serve on councils/committees are limited. Head Start’s dosage for parents is significantly less than the dosage for children. Further, Head Start-eligible low-income families experience more difficulty establishing advantageous social networks (Browne-Yung, Ziersch, & Baum, 2013; Zambrana & Zoppi, 2009). Studies indicate that higher parental social support is associated with lower levels of parental stress, effective parenting skills (McConnell, Breitkreuz, & Savage, 2011). Head Start should provide more parental programs so that parents can have more opportunities to acquire stable quality social networks.
Longer exposure to Head Start does not impact parental social service use. Social service use measured in the current study was mostly related to household risk factors such as income assistance, nutrition assistance, housing assistance, utilities, job training, alcohol/drug abuse support, mental health services, family violence support, and foster care payment. According to the Head Start Program Information Report during 2014–2015, fewer than 10% of Head Start families used social services, whereas half of the families participated in parent education or health education, preventive services offered by Head Start. Most formal social services included in the current study are post-curative services rather than preventative services tied to psychological stigma (Goodban, 1985). Further, among low-income families, receiving income assistance (TANF) has been adversely associated with outcomes for children and parents (Smith, Brooks-Gunn, Klebanov, Smith, & Lee, 2000). Formal social services are likely to be used as a last resort. Low-income parents experience more barriers to establishing beneficial social networks (Browne-Yung et al., 2013) and are more apprehensive about using social services (Goodban, 1985). Given higher demand for social services among impoverished parents, Head Start’s ongoing partnership with family and community resources should be continuously strengthened.
Family characteristics were associated with different parental outcomes. Compared to Hispanic mothers, White mothers were less likely to be involved in children’s schooling and more likely to use formal social services. White mothers also perceived more helpfulness from their social support than Black and Hispanic mothers. Black and Hispanic low-income parents engaged in their children’s schooling more than White parents (Bradley, Corwyn, McAdoo, & García Coll, 2001). Several studies documented ethnic minority groups’ barriers to social support and social services (Almeida, Subramanian, Kawachi, & Molnar, 2011; Radey, 2015). Though Hispanic mothers were more involved in their children’s school, they perceived less helpful social support than White mothers. This disparity might be due to the risk factors associated with Hispanic ethnicities, who are likely to speak Spanish and to have recent immigrant status (Zambrana & Zoppi, 2009). Language and cultural misunderstandings (Earner, 2007) have been found to be a barrier to access social services. Head Start should provide culturally and linguistically appropriate social support and services for diverse participants.
Regardless of duration of enrollment in Head Start, parents who have more household risk factors were less involved in schools and used more formal social services. Numerous studies indicated adverse effects of these risk factors on parental involvement (Bradley et al., 2001; Brooks-Gunn, Klebanov, Smith, Duncan, & Lee, 2003; Fendrich, Warner, & Weissman, 1990). Household risk factors used in the current study were low income (receiving welfare), fewer years of parental education, unemployment, single parent, and teenage mothers. The current study includes social services such as income (TANF), nutrition (Supplemental Nutritional Assistance Program), and housing assistance, utilities, job training, alcohol/drug abuse, mental health services, family violence, and foster care payment. Most of these social services are means-tested aid programs that provide benefits only to low-income persons and those with other risk factors. Thus, among Head Start-eligible low-income families, those who had more cumulative household risk factors might be able to receive various social services than those who had fewer risk factors. Studies have indicated that impacts of Head Start were different depending on family risk factors (Lee & O’laoire, 2013; Miller, Farkas, Vandell, & Duncan, 2014). A follow-up study can examine whether dosage effects (longer duration of enrollment in Head Start) can enhance positive parental outcomes for children with cumulative risk factors.
Limitations of the study
One of the major limitations was that the design of this study was not a true experiment testing dosage effects, which limits the degree to which causal inferences can be made. Among non-Head Start children, information on whether they had ever enrolled in Head Start was not available. Some non-Head Start children might have attended Early Head Start. The current study used children who have attended Head Start for four years as a reference group to extract the dosage effects of Head Start enrollment. Due to this reason, the findings should be interpreted cautiously, not as a causal inference of dosage effects. All parental outcomes were measured by parental self-reports and were conducted with non-standardized measures that did not have official validity and reliability. In Head Start Impact Study data, various data collection instruments were used to assess children’s outcomes by reporting reliabilities as shown in Exhibits 3.11–3.15 (US DHHS, ACF, Office of Planning and Evaluation, 2010). However, no specific information was provided for the parental outcome variables The only information reported was that the reliability of the parental involvement was less than 0.6 (Puma et al., 2010, chapter 7, p. 6). Since the reliability of the scale should be generally greater than 0.7, this also should be considered in the interpretation.
Parental involvement was measured by counting the frequency that parents participated in school activities, but reasons for parental involvement were not considered. Some might be over/undercounted. Some parents might need to be involved (e.g., attend teacher conferences) due to their children’s negative outcomes such as low scores or similar problems. Social support was measured by the perceptions of the social support parents actually received. This measure did not consider whether parents had access to available social networks such as parents, spouse, friends, neighbors, etc. Social service use was measured by how many services parents used. The current study did not consider quality of programs or what kind of formal social services are actually available at and near Head Start school sites. Rather, the variables were based on maternal conceptual satisfaction about social supports and whether various kinds of public assistance and social services were used. A future study needs to examine the “social support” and “social service use” variables that measure both accessibility and actual use status.
Implications for social work practice and policy
Longer exposure to Head Start programs positively affected parental outcomes. Parents who enrolled in Head Start for multiple years were more involved with their children’s school and received more helpful social support. The longer dosage of Head Start did not affect parental use of formal social services. Generally, it is more challenging to change parental outcomes than child outcomes. This is perhaps due to the fact that parents might receive a less intense dosage of intervention specifically targeted for parents. Compared to Head Start children who attend formal daily schooling with enriched curriculum, Head Start parents receive limited interventions that are offered monthly at most, such as participating in parental workshop, health education, policy councils, and volunteering in schools. Head Start was established based on an ecological systems theory (Bronfenbrenner & Morris, 1998). From the perspective of social work practice, this requires an approach that facilitates family engagement in the program. According to new Head Start program performance standards, (1) Head Start is trying to offer longer service duration (minimum 1020 hours toward full-day, full year programs) and (2) Head Start will solidify the critical role of parents in the program through better family partnership services.
Although the longer hours of Head Start programs can benefit children’s outcomes, the benefits parents could obtain are not as much as children receive. Further parental program components should be enhanced both qualitatively and quantitatively. Compared to children, what Head Start implements for parents is limited. Although the new Head Start program performance standards emphasize the parental role to enhance children’s outcomes, there are no specific required hours of service for parents and no program components targeted for parents. Despite the importance of evidence-based policy, evaluations for parental outcomes have not conducted as rigorously as those for children’s outcomes. One of Head Start’s ultimate goals is to make parents as like teachers through Head Start program so that parents can play teachers’ role when children leave Head Start. In order to do this, social workers in Head Start programs play important roles to recruit parents with young children earlier and to have parents actively participate in intervention programs Head Start is offering. Despite the fact that Head Start was created as a program of community action to break the vicious cycle of poverty, Head Start evaluation has not been extensively conducted in the context of social work perspectives. Head Start should be evaluated from social work approach that proposes a change toward positive outcomes through intervention. Further, social workers should participate in Head Start evaluations as researchers to find out what works for parents and to advocate in the policy making process. Child development is the interaction between child and environments that requires family, school, and community. Parents, teachers, social workers, policy makers, and other community members can work together to raise a whole child.
Footnotes
Ethics
This study was submitted for Institutional Review Board (IRB) review, following the guideline of the University Committee for Research involving Human Subjects. The IRB office determined this secondary data analysis study as nonhuman subject research since the data do not contain any identifiable personal information as defined by the Department of Health and Human Services [45.CFR.46.102(f)].
Funding
The author received no financial support for the research, authorship, and/or publication of this article.