
Abstract
Summary
This article reports a study that investigates the impact of a three-month online meditation programme for geriatric social workers in South Asian cities for mitigating stress, improving professional quality of life, and building work competencies.
Findings
Results indicated that the online meditation sessions were effective (Cohen’s d range = 2.21–4.17, p = . 001) in lowering perceived stress of geriatric social workers, mitigating burnout and vicarious traumatization and promoting higher levels of compassion satisfaction and geriatric social work competencies as compared to online music sessions. Meditation was more effective for women workers, Hindus and Buddhists, who undertook therapeutic interventions, and whose clientele were older adults with physical ailments, in home-care with cognitive impairments and hospice-living elderly. This was in comparison to men, Christian workers, whose work profile comprised resource mobilization and whose clientele were healthy community-dwelling older adults. Regular attendance of the online meditation sessions and self-practice were significant mediators of intervention impact.
Applications
The findings contribute to intervention research on mitigating stress at work and more specifically the stress of professional geriatric care-work. In addition to mitigating burnout and reducing emotional exhaustion, this person-directed online meditation programme also led to compassion satisfaction and bolstered competencies for geriatric practice.
Keywords
Geriatric social work professionals are increasing in demand owing to the growing older adult population worldwide. Within the interdisciplinary context of geriatric care, professional social workers undertake a combination of therapeutic interventions and support role, resource mobilization and implementation of policies and programmes (Lehning, Nicklett, Davitt, & Wiseman, 2017). Geriatric social work can be in community-based, home-based and hospice or hospital settings (Lafortune, Huson, Santi, & Stolee, 2015).
Stress among geriatric social work professionals is an occupational hazard owing to the nature of care-work, which includes dealing with physical illness, age-related cognitive decline and cognitive impairments and end-of-life care, and the accompanying emotional and physical investments and exhaustion (e.g. Dulon, Kromark, Skudlik, & Nienhaus, 2008). The psychosocial workload of professional geriatric care is thus high (e.g. Glaser, Lampert, & Weigl, 2008). Compassion fatigue, secondary traumatic stress or vicarious traumatization and burnout are thus common among geriatric care professionals (e.g. Kolthoff & Hickman, 2017). Geriatric care work stress also leads to low self-efficacy, sense of personal accomplishments and diminishing work competencies (e.g. Bria, Spânu, Băbana, & Dumitraşcu, 2014). This has implications for the professional quality of life, which for care workers generally involves compassion satisfaction (CS) and in stressful situations which faces the risk of burnout, depersonalization and vicarious traumatization (Ray, Wong, White, & Heaslip, 2013), thereby impacting work competencies (Jennings & Mitchell, 2017).
Geriatric social work-induced exhaustion and diminished vigour thus require recovery periods to offset future deleterious consequences for mental and physical health. It is therefore important to understand the factors that affect recovery (e.g. Bardach & Rowles, 2012). Interventions for eldercare workers include empowerment programmes to impact on work conditions and that primarily improved the quality of care (Petterson, Donnersvärd, Lagerström, & Toomingas, 2006), mindfulness, referring to paying attention to present experiences and respite experiences (Marzuq & Drach-Zahavy, 2012), relaxation exercises to manage compassion fatigue (Aycock & Boyle, 2009), and, guided imagery as a relaxation technique that relies on descriptive language to facilitate listener visualization of detailed, calming images, with the goal of achieving a relaxation response (Kiley et al., 2018). Music therapy or controlled listening to instrumental music is also often used as a relaxation technique (e.g. Hanna-Pladdy & MacKay, 2011). Specifically, Mackenzie, Poulin, and Seidman-Carlson’s(2006), randomized controlled trial have found the effectiveness of mindfulness-based stress reduction programmes in mitigating burnout among eldercare nursing staff and a significant impact on emotional exhaustion.
Meditation is the spiritual technique that involves centring, transcendence and mind–body balance and encompasses various forms such as mindfulness, compassion, transcendental and cyclic, among others (Goyal et al., 2014). The general focus of all forms is relaxation and centring, observing, describing, acting with awareness, non-judging, and non-reactivity of inner experience (Dekeyser, Raes, Leijssen, Leysen, & Dewulf, 2008). Systematic reviews (e.g. Fjorback, Arendt, Ornbøl, Fink, & Walach, 2011) and randomized trials have confirmed the beneficial effects of meditation in reducing stress (e.g. Khoury, Sharma, Rush, & Fournier, 2015; Rosenkranz et al., 2013).
Given the growing importance of geriatric social workers as a part of the interdisciplinary care team, and their vulnerability to stress, burnout and compassion fatigue, there is a need to investigate interventions that address those. There is some existing evidence on educational interventions and training needs of elder care staff which are work-directed (therapy and rehabilitation for clients), person-directed (client interventions and worker education/capacity building) and combined (both for the client and the worker; see Westermann, Kozak, Harling, & Nienhaus, 2014). Though mindfulness and meditation have been recommended for informal caregivers (e.g. Wennerberg, Lundgren, & Danielson, 2012) and chaplains or pastoral care professionals (e.g. Liefbroer & Berghuijs, 2019), apart from Mackenzie et al. (2006) study on mindfulness-based interventions, there is no research investigating the impact of meditation on geriatric social workers’ stress. To address this gap in evidence the present study investigates the impact of an online meditation programme on a cohort of South Asian geriatric social workers in mitigating their stress, improving professional quality of life and building work competencies, with online music sessions as the active control condition.
This is further in line with growing research on online or internet-based meditation programmes as found to be useful owing to their convenience, cost-effectiveness and low risk (Wahbeh & Oken, 2016). Spijkerman, Pots, and Bohlmeijer’s (2016) systematic review of 15 RCTs indicated that online mindfulness-based interventions had a significant impact on stress reduction and that was further moderated by the number of sessions.
Meditation impact however differs based on participant characteristics and engagement. Research indicates that women benefit more from meditation (Rojiani, Santoyo, Rahrig, Roth, & Britton, 2017) as it is aimed at decreasing the tendency to ruminate, which is the natural behavioural response of women to stressful life situations (Johnson & Whisman, 2013) as compared to men who tend to externalize and seek distractions. Though the evidence is inconclusive, some research indicates that education and class are significant moderators of meditation impact, with odds being in favour of advantaged cohorts (e.g. Sauer et al., 2013). However, studies have also suggested the positive impact of meditation techniques for vulnerable groups (e.g. Eva & Thayer, 2017). Meditation is also evidenced to benefit those who are culturally familiar with the technique and may need refinements for those who are not (e.g. Woods-Giscombé & Gaylord, 2014). Moreover, whereas standard duration of sessions is preferred for maximum benefit, there is also support for customized packages to meet the desired outcomes (e.g. Carmody & Baer, 2009). There is also no conclusive evidence on whether a low-dosage fairly long-term intervention would be more beneficial to the stress outcome or otherwise (e.g. Wolever et al., 2012). This is one aspect that needs to be investigated, which is done in the present study through a three-month programme. Further, participants’ attendance at sessions, prudent following of instructions intended by developers or adherence (e.g. Donkin et al., 2011) and self-practice or home practice, are crucial to determining impact (e.g. Parsons, Crane, Parsons, Fjorback, & Kuyken, 2017).
In the present three-month long study, intervention group geriatric social workers from four South Asian studies underwent the online meditation sessions and recommended self-practice. Outcomes on perceived stress, professional quality of life and geriatric social work competencies were compared pre- (T1) and post-test (T2) with a control group who underwent the online music sessions.
Based on the existing literature, the following hypotheses were developed: H1: Geriatric social workers who participated in the online meditation sessions would be more likely to report lower perceived stress, burnout, secondary traumatic stress and higher levels of compassion satisfaction and geriatric social work competencies at T2 as compared to those who participated in the online music sessions. H2: It is expected that the impact of the online meditation sessions would vary based on participants’ demographic and work-related characteristics (city, age, gender, religion, service duration, work profile, clientele) and intervention participation (online sessions attended, self-practice). H3: Online meditation sessions attended and self-practice will mediate the association between participants’ demographic and work-related characteristics and perceived stress, professional quality of life and geriatric social work competencies related outcomes.
Method
Intervention and control group characteristics
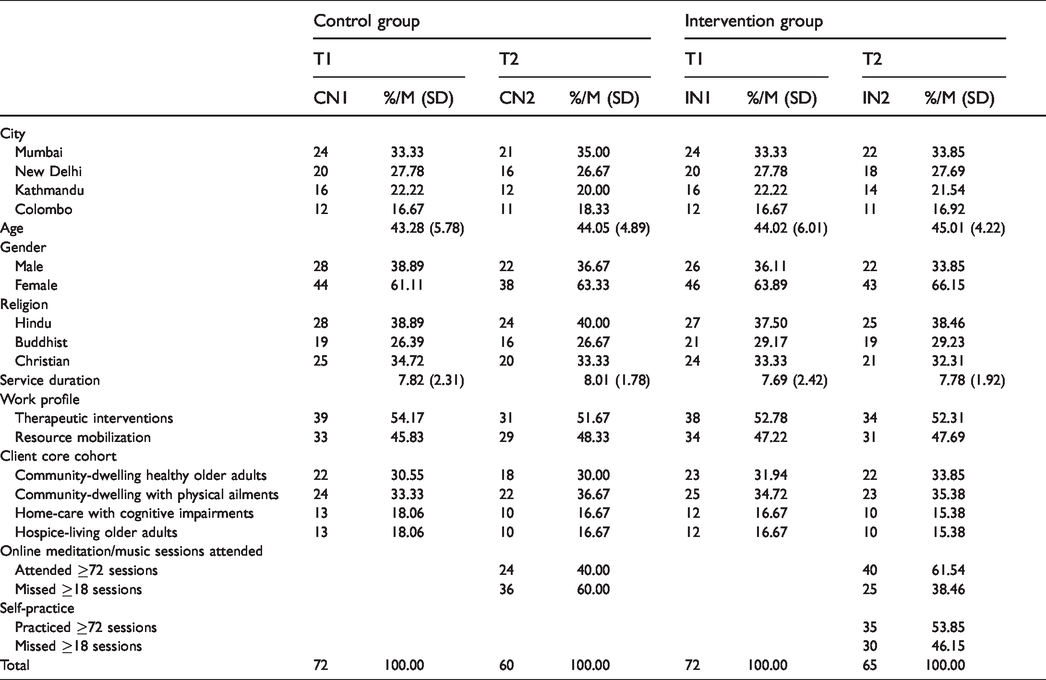
Table 1 depicts the intervention and control group characteristics at pre- (T1) and post-test (T2).
Introduction and control group characteristics.
Participant recruitment
For this study, geriatric social workers were recruited through networks of voluntary organizations and hospices working with older adults in Mumbai, New Delhi, Kathmandu, and Colombo. Flyers and e-news/announcements were made containing details of the online meditation and music programmes and the intended study. Through this process 168 social workers volunteered initially of whom 24 dropped out prior to the formal sign-up. At T1, 144 social workers were randomized into intervention and control groups using computer generated random numbers. Randomization process was masked from the potential participants. For this three-month study, the intervention group participated in the online meditation sessions and the control group participated in the online music sessions. Figure 1 depicts the flow of participants through each stage of the experiment.
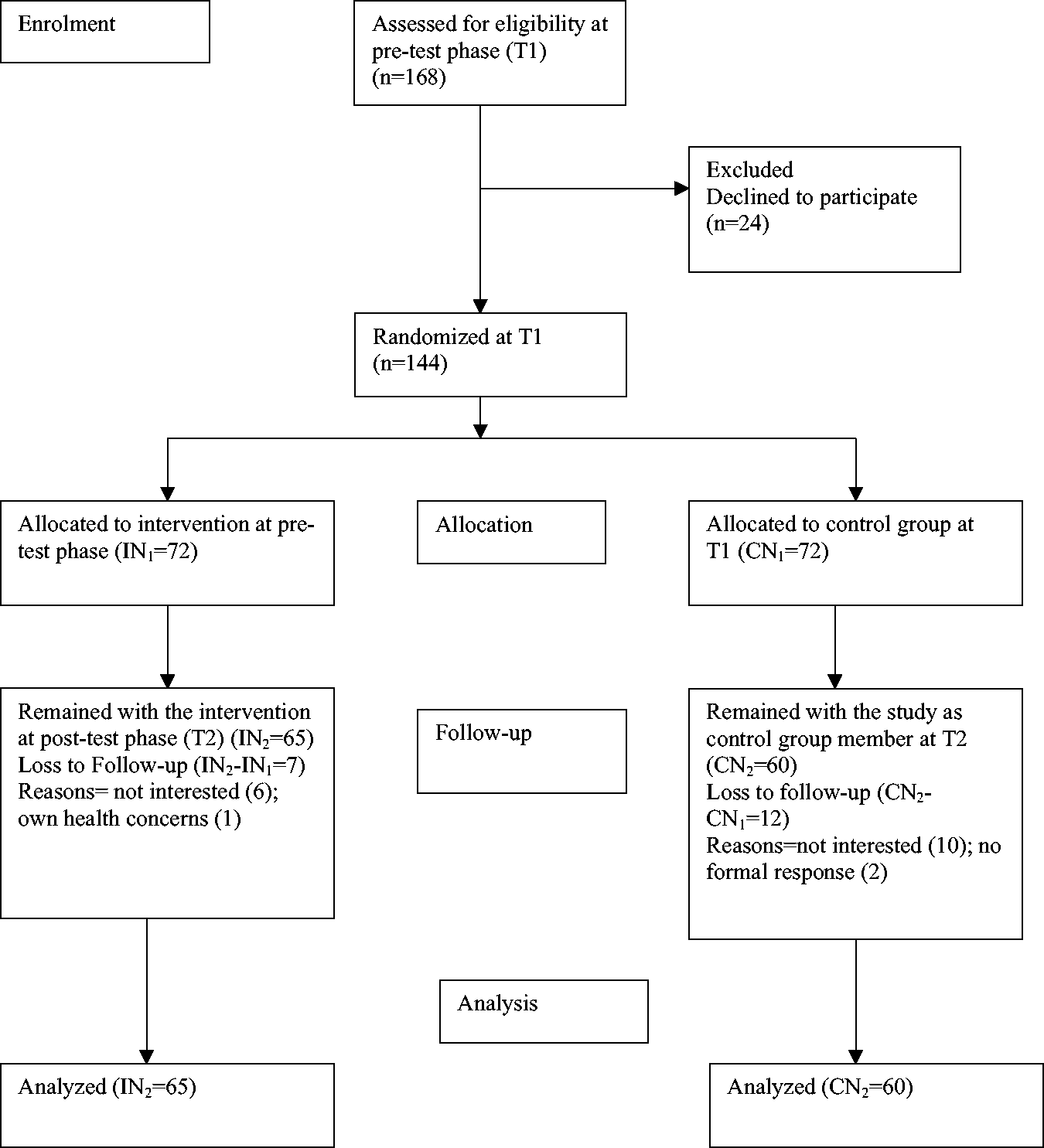
Flow of participants through each stage of the study.
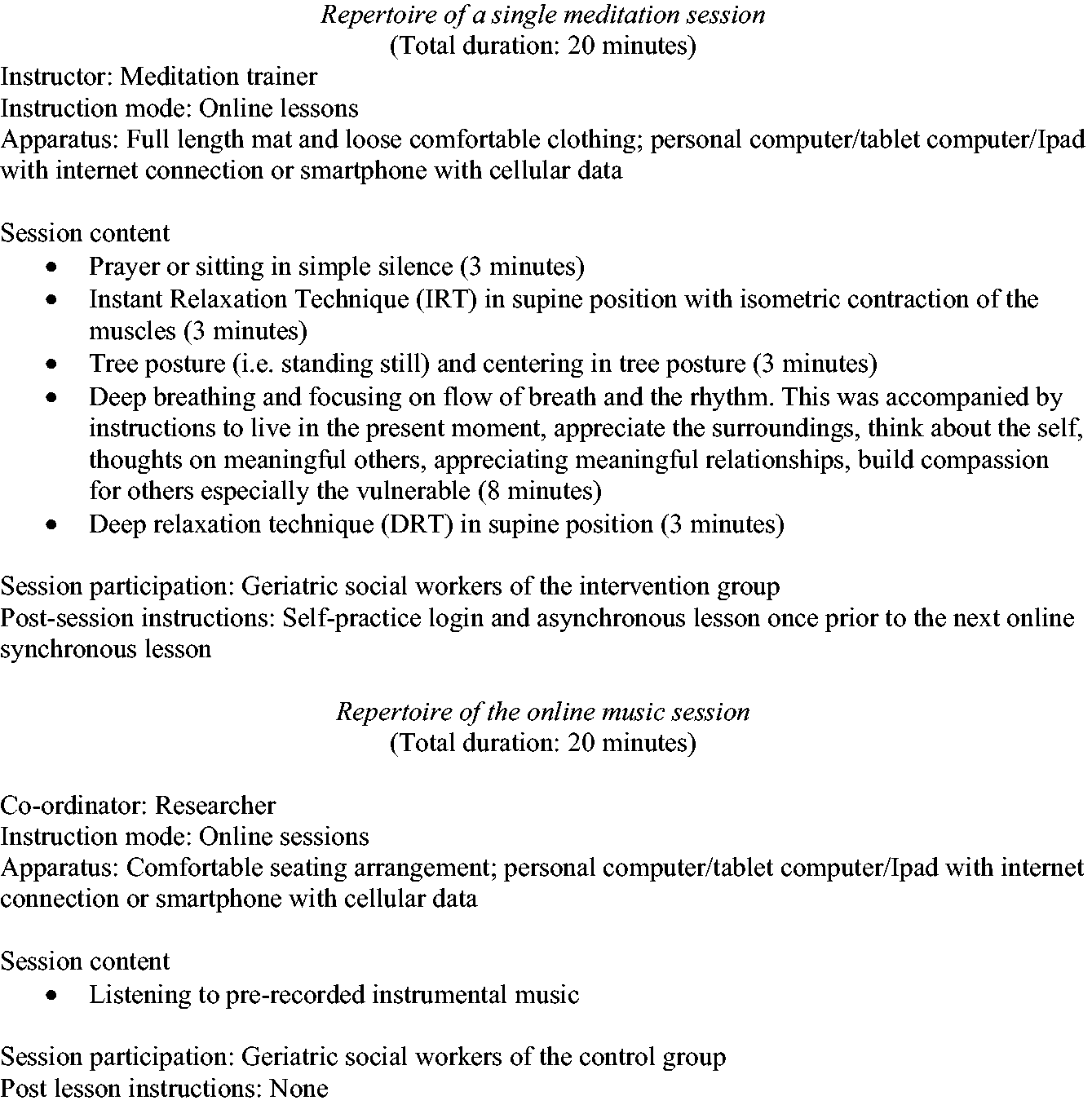
Repertoire of a single online meditation session and online music session.
Measures
Data were collected at T1 and T2 via an online questionnaire comprising demographic details and work-related details (city, age, gender, religion, service duration, work profile, client core cohort). T2 attendance at online sessions and self-practice where applicable were recorded in the online system.
Three scales were used to assess the outcomes: Perceived Stress Scale (PSS), Professional Quality of Life-Version 5 (PrQOL-5) and Geriatric Social Work Competency Scale II with Lifelong Leadership Skills (GSWCS-II-LLS).
The PSS, originally developed by Cohen, Kamarck, and Mermelstein (1983) as a 14-item version, is a widely used measure to assess the perception of stressful experiences by asking the respondents to rate the frequency of his/her feelings and thoughts related to events and situations that occurred over the previous month (Cohen & Williamson, 1988). Seven negative items represent perceived helplessness and other seven positive items represent self-efficacy. Each item is rated on a five-point Likert-type scale (0 = never to 4 = very often). Total scores are calculated after reversing positive items’ score and then summing all scores. PSS-14 scores range from 0 to 56, with higher scores representing greater stress. The PSS has good psychometric properties including reliability, convergent validity, and cross-cultural application (e.g. Leung, Lam, & Chan, 2010). For the present study: Cronbach α = .88; item-scale intercorrelation = .88–.91.
The ProQOL, developed by Stamm (2010), consists of three subscales measuring facets of CS and compassion fatigue, targeted at individuals working in caring or helping professions. The three subscales are compassion satisfaction (CS), burnout (BO), and, secondary traumatic stress (STS). Compassion satisfaction is the pleasure derived from being able to do the helping/care work well. Burnout is the first element of compassion fatigue and is associated with feelings of hopelessness and difficulties in dealing with work. Secondary traumatic stress is the second component of compassion fatigue and is about work related, secondary traumatic stress, also called vicarious traumatization. Each subscale consists of 10 questions on work related experiences in the past 30-days, and scoring is done for the three subscales separately, initially on a five-point Likert-type rating ranging from 1 = never to 5 = very often. Five items on the burnout subscale are reverse scored. Raw scores for each of the subscales range from 10 to 50, which are then converted to t-scores having mean 50 and standard deviation 10, as per the manual (Stamm, 2010). The cut scores for the subscales are around 43 for the 25th percentile (indicating low scores) and 57 for the 75th percentile (indicating high scores). Higher t-scores on CS, BO and STS subscales indicate higher compassion satisfaction and fatigue, respectively. The PrQOL has good psychometric properties and wide cross-cultural application (e.g. Hegney, Rees, Eley, Osseiran-Moisson, & Francis, 2015). For the present study for PrQoL-CS subscale: Cronbach α = .88, item-subscale intercorrelation = .78–.84; PrQOL-BO subscale: Cronbach α = .76, item-subscale intercorrelation = .72–.84; PrQOL-STS subscale: Cronbach α = .82, item-subscale intercorrelation = .71–.87.
The GSWCS-II-LLS, developed by CSWE Gero-Ed Center (Council on Social Work Education, National Center for Gerontological Social Work Education, 2014), under the aegis of the Hartford Partnership Program in Aging Education (HPPAE), consists of 50 statements measuring five sets of competencies or skills considered important to social workers working on behalf of and with older adults, including: values, ethics, and theoretical perspectives; assessment; intervention; aging services, programmes and policies; and, leadership in the practice environment of aging. The first four sections are used for learners and the last one is added for practitioners and professionals. The GSW-II-LL utilizes a Likert-type response system, with each skill rated from 0 = not skilled at all, 1 = beginning skill, 2 = moderate skill, 3 = advanced skill, and 4 = expert skill. Total scores range from 0 to 200, with higher scores indicating better competencies. The GSWCS-II-LLS has acceptable psychometric properties including reliability, internal consistency and is increasingly being used in cross-cultural contexts (e.g. Daniel, Monteiro, Ferreira, & Galhardo, 2019). For the present study: Cronbach α = .88; item-scale intercorrelation = .79–.86.
Intervention details and procedure
The online meditation programme was developed by two meditation experts associated with transnational spiritual organizations and invited in their honorary capacities. The programme was planned in a 90-day synchronous format and the self-practice component was in an asynchronous form. In consultation with two software developers, graphic user interface software was used for the multimedia synchronous sessions, to be virtually attended. The synchronous delivery of the online sessions was by meditation experts. Logging in for self-practice at least 80% of the times (≥72 sessions) was considered regular and missing more than 20% of the login sessions (≥18 sessions) was considered occasional self-practice. The online music sessions were developed by two instrumental music experts based on Mumbai and Kathmandu, respectively. Figure 2 gives details of both the programmes. Treatment adherence was auto-recorded through the online logins. T1 data were collected at the commencement of the study and T2 three-months later.
Statistical method
T1 and T2 scores of the intervention and control groups on the outcomes were compared and effect sizes were measured using Cohen’s d statistics. Mixed design two-way ANOVA was used to identify significant Group × Time interactions and the main and interaction effects of significant predictors/independent variables on outcomes. Multivariate analyses were conducted on the change scores (pre- and post-test) and significant predictors of outcomes were further examined through Kruskal–Wallis non-parametric testing. Structural equation models using standardized coefficients and the maximum likelihood method were developed to investigate significant mediators of T2 outcomes.
Results
This intent-to-treat analyses present scores at baseline and T2 mean differences in outcomes and effect sizes. Group × Time effects, predictors of change scores, and mediators of T2 outcomes are presented.
Perceived Stress, Professional Quality of Life and Geriatric Competencies Scores
Baseline controls and post-test mean differences
Table 2 indicates that the control and intervention group outcome measure scores were equal at baseline, with no significant difference at T2 (p = .30–.76; d = 0.05–0.17). There was no significant difference in the T2 outcome measure scores of the control group (p = .15–.56; d = 0.10–0.25). T2 PSS scores of the intervention group were lower than the control group (mean difference = −27.67, p = .001, d = 4.17) and their own T1 scores (mean difference= −25.24, p = .001, d = 3.87). T2 PrQOL-CS t-scores of the intervention group were higher than the control group (mean difference = 23, p = .001, d = 2.75) and their own T1 scores (mean difference = 23.5, p = .001, d = 2.74). T2 PrQOL-BO t-scores of the intervention group were lower than the control group (mean difference= −25.72, p = .001, d = 3.21) and their own T1 scores (mean difference= −22.53, p = .001, d = 2.80). T2 PrQOL-STS t-scores of the intervention group were lower than the control group (mean difference = −22.93, p = .001, d = 2.65) and their own T1 scores (mean difference = −19.49, p = .001, d = 2.21). T2 GSWCS-II-LLS scores of the intervention group were higher than the control group (mean difference = 49.63, p = .001, d = 2.71) and their own T1 scores (mean difference = 55.53, p = .001, d = 3.15).
Effect of intervention on control and intervention group outcomes.
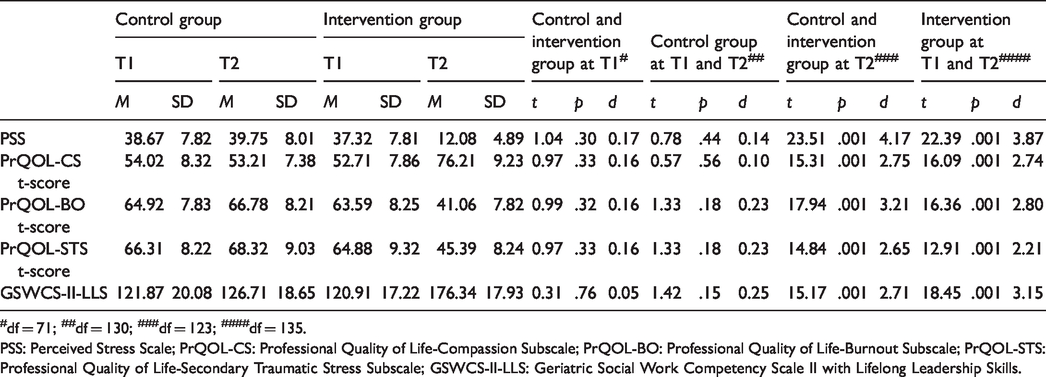
#df = 71; ##df = 130; ###df = 123; ####df = 135.
PSS: Perceived Stress Scale; PrQOL-CS: Professional Quality of Life-Compassion Subscale; PrQOL-BO: Professional Quality of Life-Burnout Subscale; PrQOL-STS: Professional Quality of Life-Secondary Traumatic Stress Subscale; GSWCS-II-LLS: Geriatric Social Work Competency Scale II with Lifelong Leadership Skills.
Interactions between different time points and different groups
Results of the mixed-design two-way ANOVA indicated that there were some significant interaction effects between time points and groups on outcome measures. There were no significant interaction effects between T1 scores of the control and intervention groups and between the T1 and T2 scores of the control group (all p ≥ .05, ηp2 ≤ .001). There were significant interaction effects between T2 PSS scores of the intervention and control group geriatric social workers, F (1, 123) = 38.62, p = .02, ηp2 = .49, and the T1 and T2 PSS scores of the intervention group, F (1, 135) = 39.44, p = .01, ηp2 = .63. There were significant interaction effects between T2 PrQOL-CS t-scores of the intervention and control group geriatric social workers, F (1, 123) = 42.36, p = .03, ηp2 = .48, and the T1 and T2 PrQOL-CS t-scores of the intervention group, F (1, 135) = 46.33, p = .01, ηp2 = .66. There were significant interaction effects between T2 PrQOL-BO t-scores of the intervention and control group geriatric social workers, F (1, 123) = 39.42, p = .02, ηp2 = .51, and the T1 and T2 PrQOL-BO t-scores of the intervention group, F (1, 135) = 51.22, p = .001, ηp2 = .75. There were significant interaction effects between T2 PrQOL-STS t-scores of the intervention and control group geriatric social workers, F (1, 123) = 46.72, p = .03, ηp2 = .56, and the T1 and T2 PrQOL-STS t-scores of the intervention group, F (1, 135) = 53.28, p = .01, ηp2 = .73. There were significant interaction effects between T2 GSWCS-II-LLS scores of the intervention and control group geriatric social workers, F (1, 123) = 62.48, p = .03, ηp2 = .59, and the T1 and T2 GSWCS-II-LLS scores of the intervention group, F (1, 135) = 60.92, p = .001, ηp2 = .78.
Simple main and interaction effects at different time points within each group
Analyses of variance indicated that at the pre- and post-test phases for the control group and at the pre-test phase for the intervention group, the main effects of gender were significant. Post hoc analyses using Tukey’s HSD indicated that within the control group at T1 and T2, perceived stress, burnout and secondary traumatic stress scores were lower and compassion satisfaction and geriatric social work competencies scores were higher for women workers as compared to men (p = .01, ηp2 = .72). This was also for the pre-test scores of the intervention group. All other main and interaction effects were insignificant (p ≥ .09, ηp2≤ .01).
Group differences post-test and main effects
At T2, when the intervention and control group had significant differences on all outcome measures, the main effects of gender continued to be significant. Additionally, the main effects of religion, work profile, client cohort, online meditation sessions attended, and self-practice were significant. Post hoc analyses using Tukey’s HSD indicated that T2 perceived stress, burnout, and secondary traumatic stress scores were lower and compassion satisfaction and geriatric social work competencies scores were higher for women, Hindus and Buddhists, whose work profile comprised therapeutic interventions, who worked with older adult clients with physical ailments, in home-care with cognitive impairments and hospice-living, and, who attended and self-practiced ≥72 online meditation sessions. This was in comparison to men, Christians, whose work profile comprised resource mobilization, who worked with healthy community-dwelling older adults, and, who missed ≥ 18 online meditation sessions as well as self-practice login sessions. All other main effects were insignificant.
Predictors of post-test change in outcome measure scores: Multivariate analyses
To investigate the T2 change in outcome measure scores of the intervention group, their pre- and post-test scores were further subjected to a MANOVA, with six variables: gender, religion, work profile, client cohort, online meditation sessions attended, and self-practice. These significant main effects were examined further through non-parametric testing (Kruskal–Wallis). The interactions between demographic and work-related predictors (gender, religion, work profile, client cohort) and intervention related predictors (online meditation sessions attended, self-practice) were significant (Roy’s largest root range = .07782712–.09734589, p = .01, ηp2 range = .58–.73). Using Bonferroni adjusted alpha levels of .0083 per test (.05/6), it was found that the independent and pairwise combinations of demographic, work-related, and intervention related predictors were significant. Further, the combined effects of significant predictors were also significant. T2 perceive stress, burnout, and secondary traumatization scores were lower and compassion satisfaction and geriatric social work competencies scores were higher for women geriatric social workers, Hindus, and Buddhists, whose work profile comprised therapeutic interventions, who worked with community-dwelling older adults with physical ailments, home-dwellers with cognitive impairments and hospice-living, who regularly attended the online meditation sessions and regularly self-practiced (≥72 sessions attended and logged in for self-practice). This was in comparison to men, Christians, whose work profile comprised resource mobilization, whose clientele were community-dwelling healthy older adults, and who were not regular in attending the online meditation sessions and practicing. All other main and interaction effects were insignificant.
Mediators of post-test outcomes
Tables 3 to 7 depict the structural equation models with standardized coefficients of the T2 perceived stress, compassion satisfaction, burnout, secondary traumatic stress, and geriatric social work competencies of participants with gender, religion, work profile, client cohort, online meditation sessions attended, and self-practice as independent variables. The maximum likelihood method was used with seven iterations. The tables indicated that all the aforesaid variables influenced the outcome measures. The goodness-of-fit measures were also significant indicating reliability of all models (PSS scores: Model 1: χ2(20) = −89.32, p ≤ .01; GFI = .95; NFI = .94; RMSEA = .05; Compassion Satisfaction subscale scores: Model 2: χ2(20) = 123.41, p ≤ .05; GFI = .95; NFI = .93; RMSEA = .05; Burnout subscale scores: Model 3: χ2(20) = −79.47, p ≤ .01; GFI = .95; NFI = .95; RMSEA = .04; Secondary Traumatic Stress subscale scores: Model 4: χ2(20) = −76.32, p ≤ .05; GFI = .95; NFI = .92; RMSEA = .05; Geriatric Social Work Competencies scale scores: Model 5: χ2(20) = 123.41, p ≤ .05; GFI = .96; NFI = .92; RMSEA = .05).
SEM of T2 PSS scores of participants (standardized coefficients).
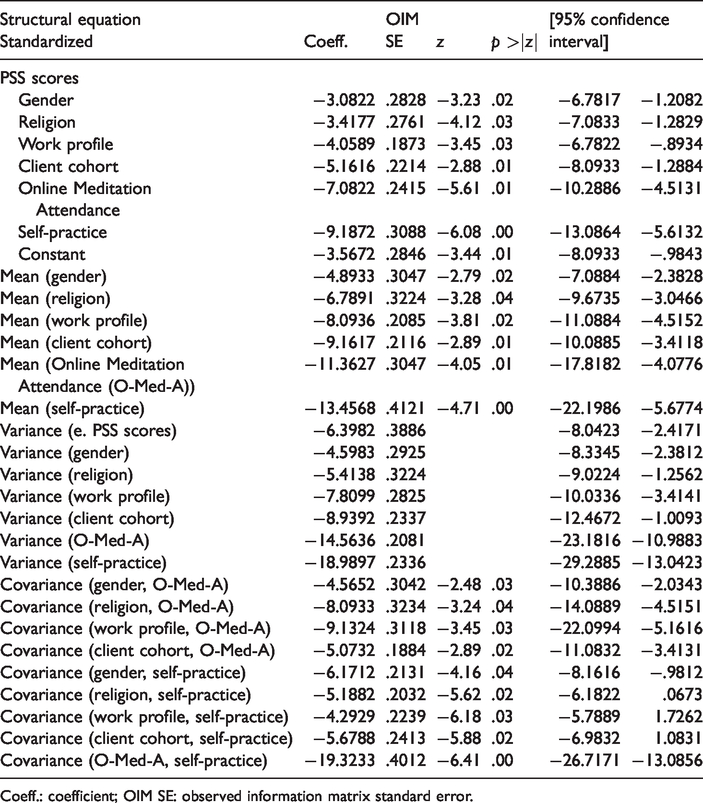
Coeff.: coefficient; OIM SE: observed information matrix standard error.
SEM of T2 PrQOL-CS t-scores of participants (standardized coefficients).
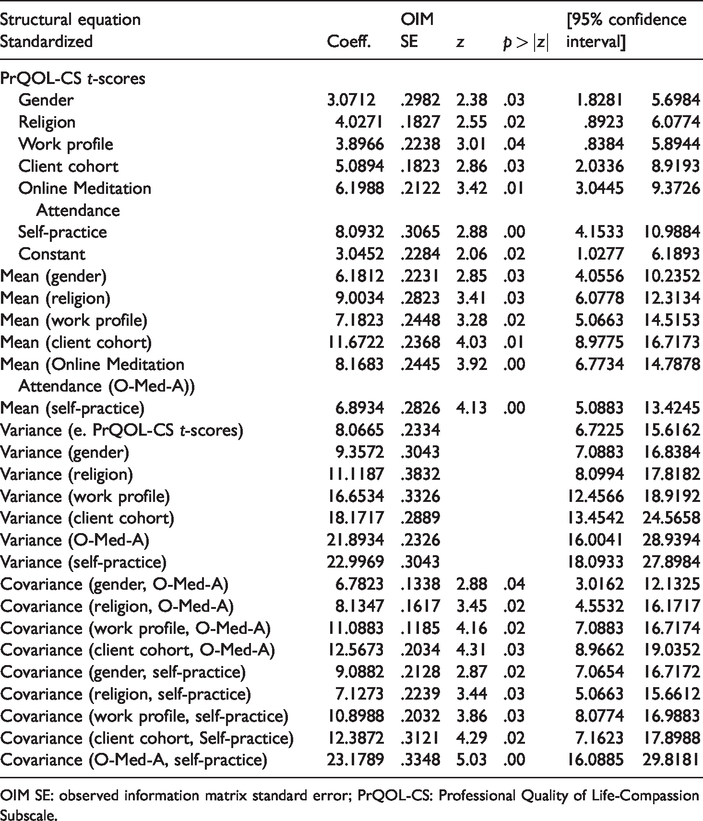
OIM SE: observed information matrix standard error; PrQOL-CS: Professional Quality of Life-Compassion Subscale.
SEM of T2 PrQOL-BO t-scores of participants (standardized coefficients).
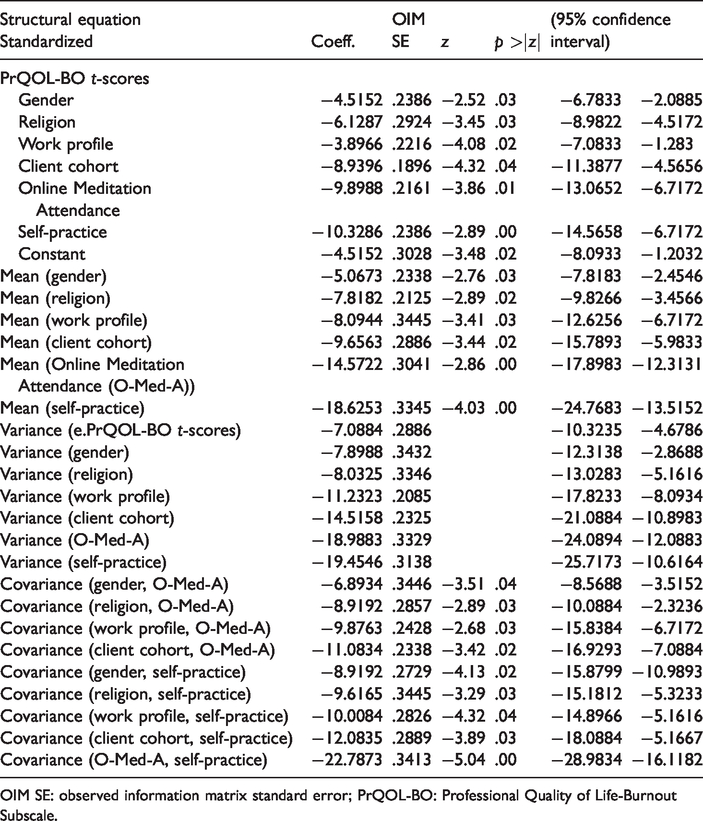
OIM SE: observed information matrix standard error; PrQOL-BO: Professional Quality of Life-Burnout Subscale.
SEM of T2 PrQOL-STS t-scores of participants (standardized coefficients).
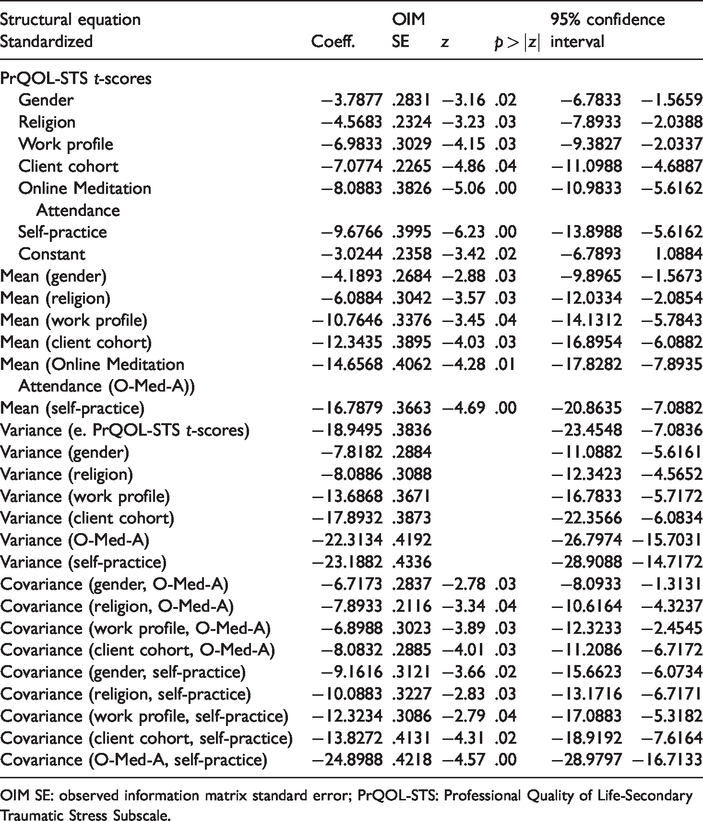
OIM SE: observed information matrix standard error; PrQOL-STS: Professional Quality of Life-Secondary Traumatic Stress Subscale.
SEM of T2 GSWCS-II-LLS scores of participants (standardized coefficients).
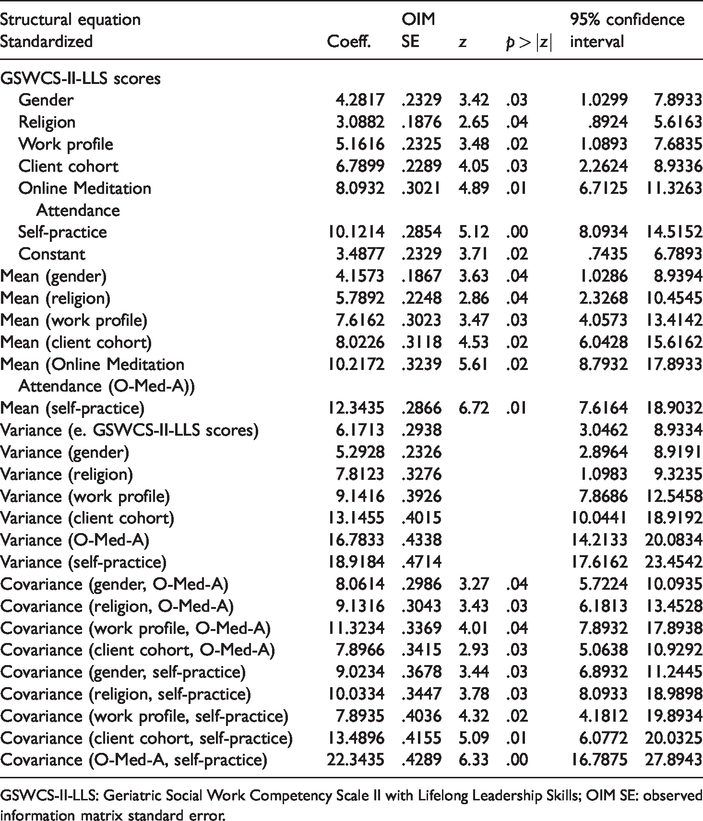
GSWCS-II-LLS: Geriatric Social Work Competency Scale II with Lifelong Leadership Skills; OIM SE: observed information matrix standard error.
Further, in all the models, significant covariance was observed between significant demographic and work-related predictors (gender, religion, work profile, client cohort) and intervention related variables (online meditation sessions attended, self-practice). Perceived stress scores were likely to decrease by −19.71% (±6.82%) with increase in online meditation sessions attendance and regular self-practice. Compassion satisfaction subscale scores were likely to increase by 23.03% (±6.87%) with increase in online meditation sessions attendance and regular self-practice. Burnout subscale scores were likely to decrease by −22.63% (±6.43%) with increase in online meditation sessions attendance and regular self-practice. Secondary traumatic stress subscale scores were likely to decrease by −22.53% (±6.25%) with increase in online meditation sessions attendance and regular self-practice. Geriatric social work competencies scale scores were likely to increase by 22.34% (±5.55%) with increase in online meditation sessions attendance and regular self-practice. All the models also established that online meditation sessions attended and self-practice mediated the relationship between demographic and work-related predictors and outcomes.
Discussion and conclusion
Results support the initial hypotheses. Geriatric social workers who participated in the online meditation sessions reported lower perceived stress, burnout, secondary traumatic stress, and higher levels of compassion satisfaction and geriatric social work competencies at T2 as compared to those who participated in the online music sessions. The difference in T2 scores of the intervention group was statistically significant and the effect sizes were moderately high (Cohen’s d range = 2.21–4.17, p = . 001). At the point of no intervention, women in both the cohorts exhibited lower stress, greater compassion satisfaction, lower burnout symptoms and vicarious traumatization and better work competencies compared to men. This was also for post-test scores of the geriatric social workers who participated in the music sessions. This is contrary to evidence on gender difference in professional care-work coping and resilience, which says that women report greater distress (see Fredman, Cauley, Hochberg, Ensrud, & Doros, 2010; Pinquart & Sorensen, 2006). One possible explanation for this could be that within social work as a profession, women social workers are more tuned into the work-profile compared to men (see Ferguson & Schriver, 2012), though more investigation is needed.
Results of this study indicated that at T2, meditation was more effective than music for the intended outcomes, women geriatric social workers within the online meditation cohort reported lesser stress, better professional quality of life and competencies as compared to men. This falls in line with meditation research, which indicates that women gain more from meditation as compared to men (Rojiani et al., 2017). This also possibly indicates that work stress, burnout, and secondary stress mitigation interventions for men specifically into care-work professions need to address their natural behavioural response of externalization. Further, Hindu and Buddhist geriatric social workers, whose work profile comprised therapeutic interventions, and whose clientele were older adults with physical ailments, in home-care with cognitive impairments and hospice-living, reported greater effectiveness of the online meditation programme. This was in comparison to Christian workers, whose work profile comprised resource mobilization and whose clientele were healthy community-dwelling older adults. Religion as a significant moderator in meditation intervention response is in line with the work of Woods-Giscombé and Gaylord (2014), which highlights that participants who find a greater cultural familiarity with the technique respond better and hence refinements are needed for those who do not.
Two other predictors were significant in determining the impact of meditation: participants’ work profile and clientele characteristics. Geriatric social workers engaged in therapeutic interventions responded better to meditation with reportedly significant improvements in stress reduction, professional quality of life and competencies as compared to those engaged in resource mobilization. One explanation could be that since therapeutic interventions are more emotionally demanding for the worker and older clientele requiring those be a greater challenge (e.g. Dulon et al., 2008; Kolthoff & Hickman, 2017), those geriatric workers would be more inclined to actively seek interventions that mitigate emerging stress and burnout. Geriatric social workers primarily engaged in resource mobilization and with healthy community-dwelling older clients, may be more interested in seeking technical inputs and practical suggestions/tips to prevent stress emerging therefrom rather than introspective and centring focused interventions.
Regular attendance of the online meditation sessions and self-practice were important mediators of intervention impact, which corroborates existing evidence (Carmody & Baer, 2009; Parsons et al., 2017). Additionally, findings support this fairly long duration online daily dosage type intervention (e.g. Wolever et al., 2012)., which can be recommended for geriatric social workers, with prudent adherence as a prerequisite (e.g. Donkin et al., 2011).
The findings contribute to intervention research on mitigating stress at work and more specifically the stress of professional geriatric care-work. In addition to the results of Mackenzie et al.’s (2006) study, where mindfulness programme mitigated burnout and reduced emotional exhaustion, findings of this person-directed online intervention study propose that practicing meditation also leads to compassion satisfaction and builds competencies of geriatric social workers.
Limitations of the study
The study has some of the following limitations. Data were collected at two specific time points in this fairly long dosage experiment, and interim changes or unexpected stressors in active work life were not controlled or accounted for. The measures were self-report, and even though randomization was masked, there is an inherent bias, which needs to be addressed in future investigations. The control condition was less robust than the experimental condition and did not have a self-practice component, which was the most significant mediator determining treatment effect. Though it is possible to conclude that meditation is effective (compared to music) in mitigating geriatric social workers’ stress, a more balanced control is needed in further research. Several other client-centred intervening variables such as intensity/severity of impairment, stage of ailment, and availability or otherwise of social/kin support, that may also effect worker stress and interfere in intervention participation, need attention in further research. Finally, differing durations of meditation intervention need to be compared to investigate relative effects.
Concluding remarks
With adequate emphasis on regular attendance and self-practice, the online meditation programme is effective for geriatric social workers to mitigate stress, improve professional quality of life and competencies. Some refinements would be needed for male geriatric social workers, Christians, primarily working on resource mobilization and with community-dwelling healthy older adults. These could include externalization activities, including more universal and broad-based tenets, and addressing stress arising from non-therapeutic social work interventions.
Footnotes
Ethics
Informed written consent was obtained from all the study participants. No risks resulting from taking part in the study were identified. The study complies with the independent ethics committee of the University of Mumbai, India and conforms to the norms prescribed by the Declaration of Helsinki, 1975 as amended in 2000, and comparable ethical standards. There are no conflicts of interest to report for this submission.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
Acknowledgements are due to the meditation experts and all the study participants.