
Abstract
Summary
Cross-boundary children and their parents suffer from various stressors and mental health problems. This pilot study aimed to investigate whether an emotion regulation parallel intervention for children and parents enhanced resilience and mental health among both groups. A total of 38 pairs of cross-boundary children and parents participated in concurrent but separate intervention sessions. Three waves of tests (i.e. pre-, post-, and one-month follow-up tests) were conducted, using t-tests to evaluate the time effects during the intervention.
Findings
The children and parents reported significant improvements in positive affect, resilience, and family harmony, as well as a reduction in depressive symptoms following the emotion regulation intervention. For both children and parents, over half of the participants who were in the high-depression category have crossed the threshold, from high to low level of depression at post-test, and participants with higher depression levels generally benefited more from the intervention.
Applications
Future researchers seeking to implement demand-driven and practice-based interventions in community settings should consider contextual and cultural sensitivity, and involve community stakeholders (e.g. cross-boundary family members and social workers) in all aspects of the research process with a given community-based participatory research approach. Screening based on depression may maximize the benefits to the participants. The essential components, as well as the fidelity measures of the intervention, should be refined. Randomized controlled trials are advocated in future studies to test the efficacy and effectiveness of the intervention in different contexts (e.g. clinical and community populations).
Keywords
A large number of children travel between mainland China and Hong Kong every day to pursue education, who are known as cross-boundary children (P. W. K. Chan & Kabir, 2014). Shuttling between two cities and two cultures every day, cross-boundary children are exposed to multiple stressors, such as physical fatigue, language hassles, limited participation in after-school activities, and ambiguous and stigmatized citizenship status (A. K. W. Chan & Ngan, 2018; P. W. K. Chan & Kabir, 2014). These acculturation-related stressors can increase the children’s risk of suffering from poor mental health, such as depression and anxiety (Perreira et al., 2018; Schwartz et al., 2015). The parents of cross-boundary children also face various stressors, such as economic strain, uncertainties about the future, difficulties in reaching the schools, and unfamiliar with Hong Kong (A. K. W. Chan & Ngan, 2018; P. W. K. Chan & Kabir, 2014). These cumulative parenting-related stresses put parents at a high risk of mental health problems (Nomaguchi & Milkie, 2017).
The issue of cross-boundary children is not limited to the China–Hong Kong border (A. K. W. Chan & Ngan, 2018), but rather also exists in the Singapore–Malaysia border (Yuen & Cheung, 2014), the US–Mexico border (Orraca et al., 2017), countries in Europe (Central Statistics Office, 2016), and areas in Africa (Vlassenroot & Büscher, 2013). These cross-boundary children and their families can facilitate sociocultural exchanges and provide new blood to the destination regions and countries. However, no psychological intervention is available for cross-boundary children or their parents who struggle with the daily transitions in China–Hong Kong border. The needs of this marginal group have not been fully addressed in resilience enhancement programs, despite its large size.
Resilience is generally described as the positive adaptation to significant adversity (e.g. stress and trauma; Windle, 2011). Among individuals who engage in cross-cultural mobility, resilience is found to be negatively correlated with depression, anxiety, and stress (Brailovskaia et al., 2019), and positively associated with subjective happiness, life satisfaction, and mental well-being (Brailovskaia et al., 2019; Khawaja et al., 2017). A range of effective interventions has been applied to enhance resilience and mental health among various groups (Joyce et al., 2018; Zolkoski & Bullock, 2012). For example, a brief intervention enhanced resilience and adaptation of immigrants from mainland China to Hong Kong by promoting self-efficacy, positive thinking, altruism, and goal setting (Yu, Stewart, et al., 2014), which is of referential importance in developing cost-effective resilience interventions.
Development of the intervention
Intervention targets
Before the intervention, we conducted a preliminary needs assessment through semi-structured interviews with the parents of cross-boundary children and social workers serving cross-boundary families. The needs assessment revealed that family conflicts often occurred when the cross-boundary families faced stressful events. For example, language barriers led to lower academic performance in some cross-boundary children, while parents were unable to supervise children’s homework. Frustrated with their lack of emotion regulation strategies, the children and parents often vented their anger and anxiety on each other, which sometimes led to physical abuse. A participant talked about her experience—which is similar to other parents—in the needs assessment interview: My son doesn’t like me, because I often scold him. … When I notice that my son cannot focus on his homework, I want to beat him. I think I suffer from poor mental health. … In the mainland, kindergarten children usually learn to write in the simple Chinese, but people in Hong Kong use the traditional Chinese. I know how to read (the traditional Chinese), but I don’t know how to write. My son is stressed out. … I just want my son to finish his homework faster and be more concentrated, but I’m very impatient. (P2) I think emotional regulation (is important). As for the parents, I have noticed that disciplining a cross-boundary or new immigrant child may cause a lot of pressure and anger to parents, but they do not know how to manage (their emotions). In addition, their pressure has to do with differences in culture or values within the cross-boundary marriages and families. … The Cantonese courses and stress reduction interventions we conducted are very popular. … Emotional regulation is all good. For children, teaching them how to communicate and express emotions can also improve the parent-child relationship. (SW3)
Intervention features
Family system theory states that families function as systems of interdependent individuals in which each member can impact others (White & Klein, 2002). It has been found that children’s emotional problems are related to the stressful experiences and emotional symptoms of their parents (Banez & Compas, 1990; Ursache et al., 2017). Therefore, we involved both parents and children concurrently in the intervention in the hope of maximizing the intervention benefits. The parallel group model is widely advocated in family-based intervention, but its implementation has a certain degree of difficulty. A parallel group comprises two concurrent but separate intervention groups (e.g. a child group together with a parent group); participants from the two groups engage in similar activities in different rooms with corresponding goals and contents (K. L. Chan et al., 2002). Compared with an intervention for individuals alone, involving family members in a family-based intervention can lead to greater benefits (Dowell & Ogles, 2010). Separating parents from children could prevent children from their parents’ over-control (Xu et al., 2005) and let each group deal with their own problems (K. L. Chan et al., 2002). The parallel group model has been used to deal with different problems in parents and children (K. L. Chan et al., 2002; Valdez et al., 2013). For example, a parent–child parallel group helped to improve the psychological functioning of depressed mothers, the mothers’ caregivers, and children in Latino immigrant families (Valdez et al., 2013). Therefore, the parent–child parallel group is considered as an appropriate format for addressing the needs of cross-boundary families.
The present study
This pilot study sought to develop a brief parallel group intervention to enhance the target group’s resilience and mental health. Both the cross-boundary children and their parents were expected to show benefits in post- and one-month follow-up tests, including higher levels of positive affect, personal resilience, mental health, and family harmony as well as lower levels of negative affect and depressive symptoms.
In addition to addressing the basic research question of “Does this intervention lead to improved health?”, we moved further to examine “For whom is this intervention effective?” (MacKinnon & Luecken, 2008, p. 1). As larger effect sizes have been observed in clinical than in nonclinical samples (Aldao et al., 2010), we also expected that cross-boundary children and parents who possessed higher levels of depressive symptoms at pretest would show greater benefits than those who possessed lower levels of depressive symptoms at pretest. This investigation aimed to identify the conditions under which planning and implementation intentions are most effective (Hagger et al., 2016).
Methods
Participants
Participants were recruited via an advert posted on the International Social Service Hong Kong Branch centers’ bulletin boards and website. The recruitment criteria were as follows: (a) children who were 7–12 years of age, lived in mainland China for more than six months, and commuted on a daily basis between mainland China and Hong Kong; (b) parents (father/mother) who provided care to at least one cross-boundary child and were participating in the group with their children at the same time; and (c) no history of severe psychotic symptoms in either children or parents, and no previous participation in a similar intervention program. A total of 38 pairs of cross-boundary children and parents were recruited.
Procedure
The International Social Service Hong Kong Branch provides help (e.g. bridging programs, parenting programs, community education) for cross-boundary families in Hong Kong and mainland China. Collaborating with the International Social Service Hong Kong Branch, we adopted a community-based participatory research approach in this study, which enabled researchers and community stakeholders to participate equally in all aspects of the research process (Bogart & Uyeda, 2009). We believed that the community-based participatory research approach would lead to a better intervention design by building partnerships and promoting knowledge-sharing with stakeholders. In addition, social workers, health psychologists, and agency administrators collaborated to design the intervention protocol.
This study used a parallel design whereby the children and parents were divided into two separate groups who participated in four weekly 2-hour sessions with corresponding themes. These four sessions covered the components of the awareness and knowledge of emotions (e.g. identification, functions and process of emotions; divided into two sessions for children), emotional regulation strategies (e.g. response modification, positive thinking, attention shift), resource building for positive emotions (e.g. seeking social support and engaging in joyful activities, specifically for parents), and emotion management to strengthen family relationships, respectively. These components were derived from the literature on emotion regulation models, effective strategies for emotion management, and existing emotional management programs (Fabrizio et al., 2015; Naragon-Gainey et al., 2017). After each session, there was homework for children and parents, respectively. Participants shared their homework before the commencement of each new session.
One month after the completion of the four sessions, there was a booster to combine children and parents. In addition to reviewing effective intervention strategies that benefited their emotion management, they also shared the problems and difficulties they experienced when they applied what they learned in the intervention to seeking support from social workers and peer participants. Table 1 shows session goals, essential content, and example activities of the four-session intervention and booster. The children and parents completed paper-and-pencil tests in separate rooms before (pretest, T1) and after the intervention sessions (post-test, T2), and a one-month follow-up test (T3).
In line with previous experiences (Lam et al., 2015), social workers pointed to the difficulty of recruiting a large number of community participants to conduct a multi-arm trial in social service settings, and noted that there are ethical considerations that prohibit them from withholding treatment from their service users. Thus, no control group was included in this pilot study.
Social workers with experience of serving cross-boundary families and conducting emotional management interventions were trained and certified to deliver the intervention. A fidelity checklist was developed for this study, to measure social workers’ adherence to the intervention protocol. The research team observed each session, ensuring that all intervention activities included in the intervention manual were carried out. The entire intervention program was closely supervised by the principal investigator and agency administrators.
Measures
Emotion regulation strategies were measured using a 10-item Emotional Management Strategy Questionnaire (Fabrizio et al., 2015). The children and parents were asked to rate how frequently they had used each strategy in the previous month on a 4-point Likert scale (1 = not at all to 4 = almost always) and a 6-point scale (1 = not at all to 6 = almost always), respectively. In all three test phases, Cronbach’s α was more than .88 and .89 for the children and parents, respectively.
Positive and negative affect were assessed with the 10-item Positive and Negative Affect Schedule (PANAS-10, Fabrizio et al., 2015; Watson et al., 1988). PANAS-10 had been validated in Hong Kong (positive affect subscale: Cronbach’s α > .89, negative affect subscale: Cronbach’s α > .87; Fabrizio et al., 2015). The participants responded to the PANAS-10 on a 5-point Likert scale (1 = not at all to 5 = almost always). The internal consistency of the positive affect subscale was good for both the children and the parents (children: Cronbach’s α > .70, parents: Cronbach’s α > .93) across all three time points, as was the negative affect subscale (children: Cronbach’s α > .70, parents: Cronbach’s α > .89).
Depressive symptoms were assessed using a Chinese version of the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001; Yu, Tam, et al., 2012). The participants were asked to describe the extent to which they had suffered from depressive symptoms in the previous month on a 4-point Likert scale (0 = not at all to 3 = nearly every day). The total score ranges from 0 to 27, and a cut-off point of 10 is recommended to identify major depressive disorder (Kroenke et al., 2001). In all three tests of the current study, Cronbach’s α was more than .80 and .87 for the children and parents, respectively.
Mental health was measured using the Mental Health Inventory (MHI-5; Berwick et al., 1991). The children and parents reported their emotional and psychological well-being in the previous month on a 4-point Likert scale (1 = all the time to 4 = none of the time) and a 6-point scale (1 = all the time to 6 = none of the time), respectively. The MHI-5 has been shown to have good internal consistency in Chinese studies (Cronbach’s α = .79; Mo & Mak, 2009). In all three waves, Cronbach’s α was greater than .73 and .85 for the children and parents, respectively.
Resilience was assessed using a short version of the Connor–Davidson Resilience Scale (Campbell-Sills & Stein, 2007). The participants responded to 10 items on a 5-point Likert scale (0 = not true at all to 4 = true nearly all of the time), which showed good reliability (Cronbach’s α = .91) and validity in a previous study of Chinese earthquake victims (Wang et al., 2010). In all three tests of the current study, Cronbach’s α was more than .91 and .89 for the children and parents, respectively.
Family harmony was measured using the Family Harmony Scale (Fabrizio et al., 2015) in accordance with Chinese culture. A 4-point Likert scale (1 = strongly disagree to 4 = strongly agree) and a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree) were adopted for the children and parents, respectively. This 8-item scale has been used in parental emotional management interventions in Hong Kong and showed good psychometric properties (Cronbach’s α = .94; Fabrizio et al., 2015). In all three tests of the current study, Cronbach’s α was more than .95 and .98 for the children and parents, respectively.
We selected measures that: (1) match the expected intervention outcomes; (2) have shown evidence of improvement in previous intervention studies (e.g. the Emotional Management Strategy Questionnaire, the Positive and Negative Affect Schedule, and Family Harmony Scale have demonstrated intervention benefits in a parental emotional management program in Hong Kong; Fabrizio et al., 2015); (3) have been culturally adapted or tailored to the Chinese population, with good psychometric properties (e.g. Patient Health Questionnaire, Yu, Tam, et al., 2012; and Mental Health Inventory, Mo & Mak, 2009 have been validated in various Chinese samples); and (4) have been widely used in previous studies (e.g. the Connor–Davidson Resilience Scale was the most commonly used measure for resilience; Goins et al., 2013; Windle et al., 2011; and widely quoted in resilience research; Kjellstrand & Harper, 2012; Yu, Lau, et al., 2011).
Statistical analysis
Baseline observation carried forward (BOCF) was adopted to handle participant dropout. Based on the assumption that participants might withdraw from the intervention because of a perceived lack of benefit, the BOCF approach uses baseline observation to replace the missing endpoint (Liu-Seifert et al., 2010). BOCF preserves all samples and, to some extent, can avoid the problem of biased parameters and estimates caused by list-wise deletion (Liu-Seifert et al., 2010).
A manipulation check was performed by comparing the frequency of use of emotion regulation strategies in pre-, post-, and follow-up tests using paired samples t-tests. Paired samples t-tests were performed on all outcome measures to determine whether significant improvements were observed among child and parent participants. To further analyze the changes of participants, the participants were divided into two groups according to the PHQ-9 cut-off score (i.e. lower depression group: PHQ-9 < 10 versus higher depression group: PHQ-9 ≥ 10). Changes of all variables were evaluated for each group across various time points through paired samples t-tests. The mean changes for each group in all variables in post- (T1 versus T2) and follow-up (T1 versus T3) tests were calculated, respectively. Next, independent samples t-tests were used to estimate the difference between the two groups at each time point. The significance level was set at p < .05. Cohen (1988) defined the effect size (d) as small (.20), medium (.50), and large (.80).
Results
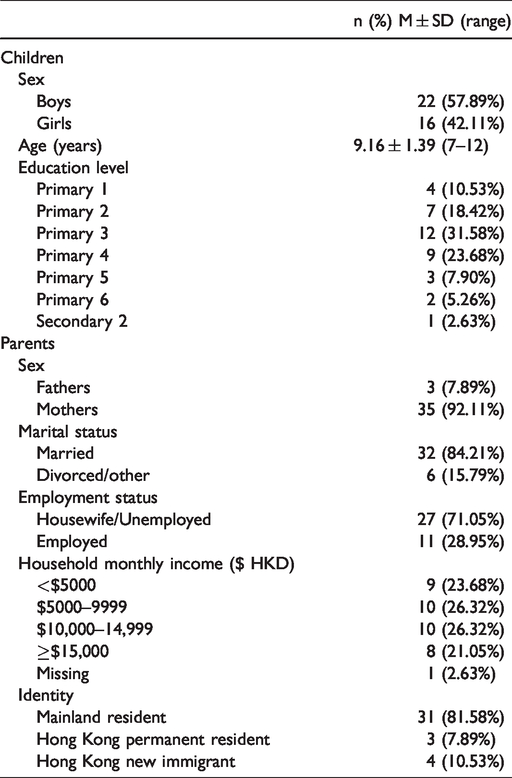
Table 2 shows that the child participants (Mage = 9.16, SD = 1.39) consisted of 22 boys (57.89%) and 16 girls (42.11%); over half of the child participants were pupils in years 3 and 4 of primary school. The parent participants were mainly housewives/unemployed with monthly household incomes of less than HK$15,000. All the children (N = 38) and parents (N = 38) completed the pretest; 4 children (10.5%) and 4 parents (10.5%) dropped out at post-test; and 17 children (44.7%) and 18 parents (47.4%) dropped out at the one-month follow-up test.
Summary of intervention manual contents.
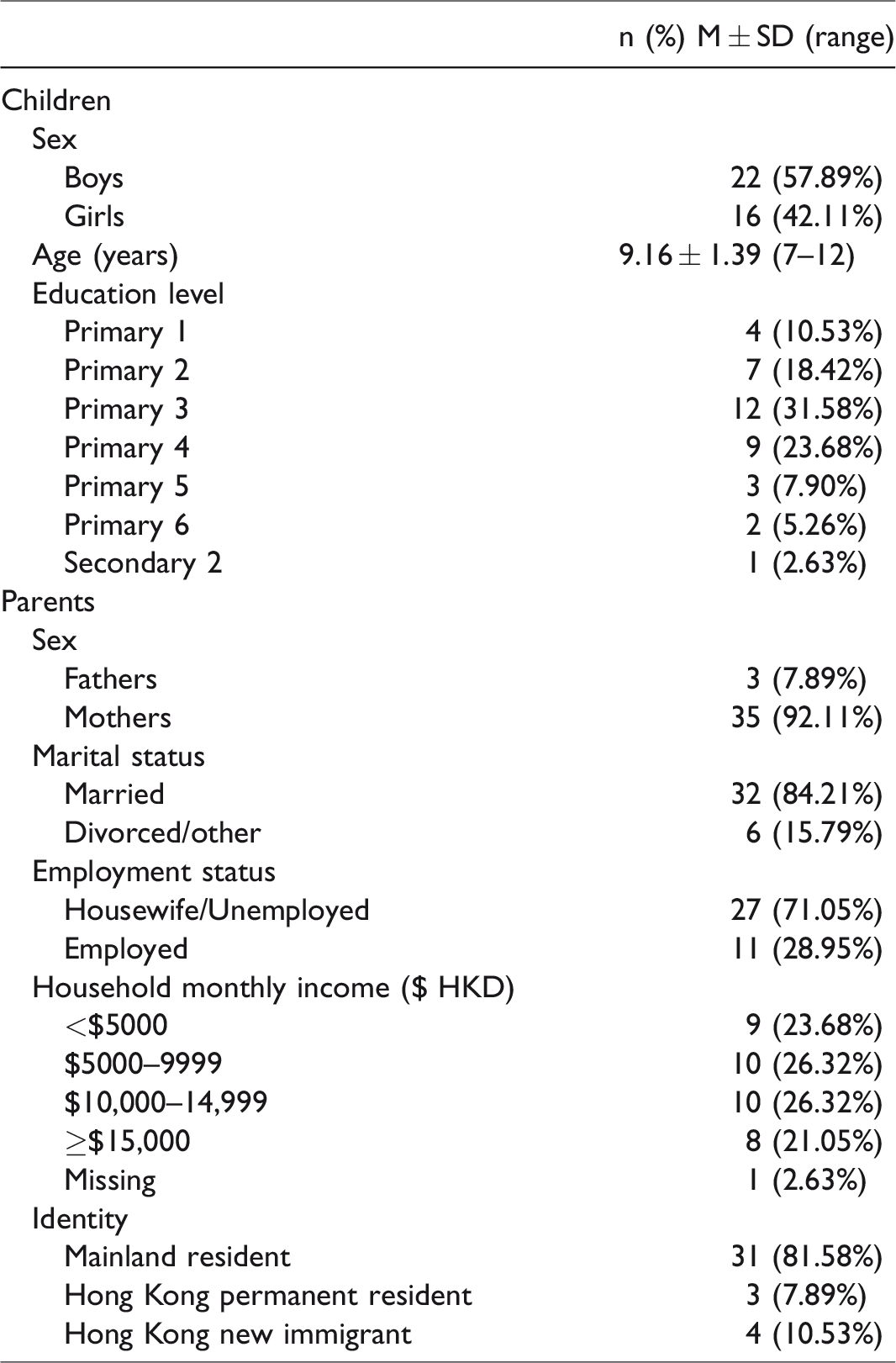
Demographic characteristics of participants (N = 38 pairs).
Manipulation check
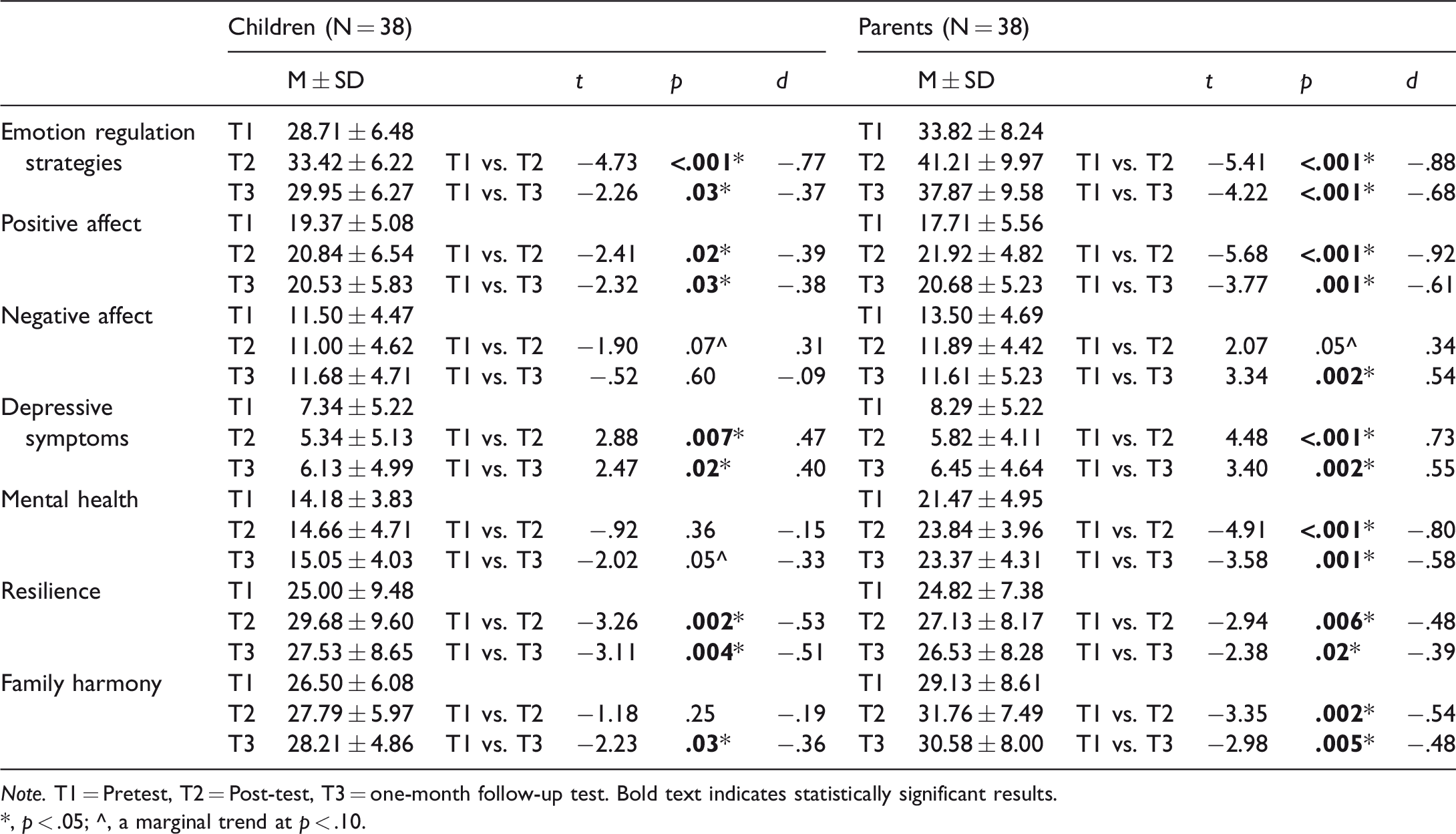
The frequency with which the participants used emotion regulation strategies significantly increased in the cross-boundary children (T2: t = −4.73, p < .001; T3: t = −2.26, p = .03) and parents (T2: t = −5.41, p < .001; t = −4.22, p < .001), indicating that the intervention had helped cross-boundary children and parents to use emotion regulation strategies more often in their daily lives.
General improvements of the participants
The results of the paired samples t-tests are listed in Table 3. Compared with T1, significant improvements in positive affect (T2: t = −2.41, p = .02; T3: t = −2.32, p = .03) and resilience (T2: t = −3.26, p = .002; T3: t = −3.11, p = .004) were observed in the children at T2 and T3, as well as a significant alleviation of depressive symptoms (T2: t = 2.88, p = .007; T3: t = 2.47, p = .02). Additionally, child-reported family harmony increased after the intervention, reaching statistical significance at T3 (t = −2.23, p = .03). The effect sizes were small to medium (Cohen’s d = 0.36 – 0.53). The parent participants reported significant improvements in positive affect (T2: t = −5.68, p < .001; T3: t = −3.77, p = .001), mental health (T2: t = −4.91, p < .001; T3: t = −3.58, p = .001), resilience (T2: t = −2.94, p = .006; T3: t = −2.38, p = .02), and family harmony (T2: t = −3.35, p = .002; T3: t = −2.98, p = .005) from T1 to T2 and T3, as well as a significant reduction in depressive symptoms (T2: t = 4.48, p < .001; T3: t = 3.40, p = .002). The effect sizes were mostly medium to large (Cohen’s d > 0.50).
Comparison of the study variables between pretest and post-test or one-month follow-up test for children and parents.
Note. T1 = Pretest, T2 = Post-test, T3 = one-month follow-up test. Bold text indicates statistically significant results.
*, p < .05; ^, a marginal trend at p < .10.
Changes among children with low and high levels of depressive symptoms
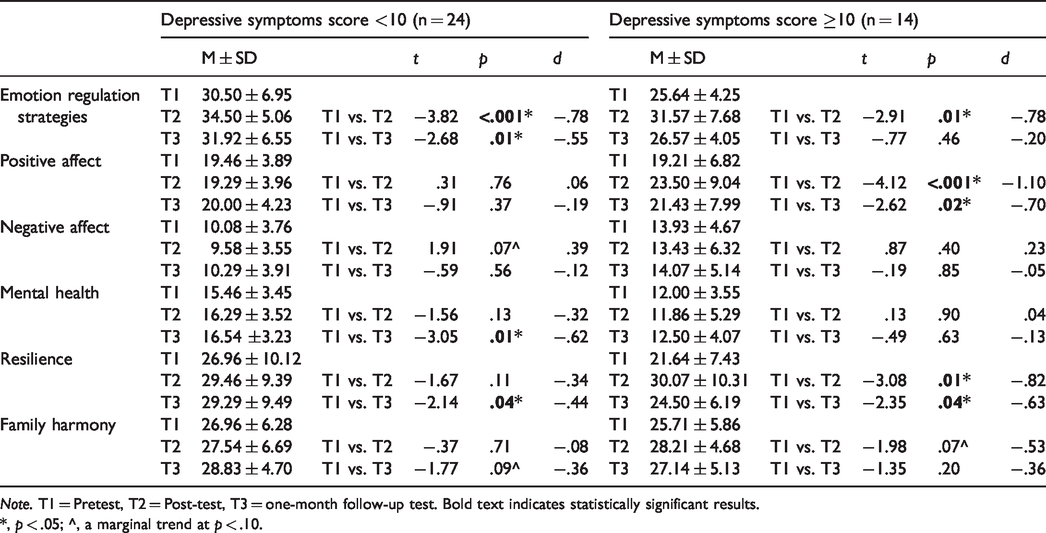
The child participants were divided into a lower depression group (low-children: n = 24, 63.16%; PHQ-9 < 10) and a higher depression group (high-children: n = 14, 36.84%; PHQ-9 ≥ 10) according to the PHQ-9 cut-off score. Compared to T1, 71.43 and 28.57% of child participants who were in the high-depression category crossed the threshold, from a high to a low level of depression at T2 and T3, respectively; further, 4.17% of child participants who were in the low-depression category crossed the threshold, moving to a high level of depression at both T2 and T3.
Table 4 shows the results of paired samples t-tests for each group at various times. In the low-children, compared with T1, mental health (t = −3.05, p = .01, Cohen’s d = 0.62) and resilience (t = −2.14, p = .04, Cohen’s d = 0.44) improved, reaching statistical significance at T3. The high-children reported significant improvements for positive affect (T2: t = −4.12, p < .001, Cohen’s d = 1.10; T3: t = −2.62, p = .02, Cohen’s d = 0.70) and resilience (T2: t = −3.08, p = .01, Cohen’s d = 0.82; T3: t = −2.35, p = .04, Cohen’s d = 0.63) from T1 to T2 and T3. Significantly greater changes in positive affect (Δ positive affect; T2: t (36) = 4.23, p < .001, Cohen’s d = 1.42) and resilience (Δ resilience; T2: t (36) = 2.08, p = .04, Cohen’s d = 0.70) were observed from T1 to T2 in the high-children than in the low-children (see Table 6).
Comparison of the study variables between pretest and post-test or one-month follow-up test based on severity of depressive symptoms of children.
Note. T1 = Pretest, T2 = Post-test, T3 = one-month follow-up test. Bold text indicates statistically significant results.
*, p < .05; ^, a marginal trend at p < .10.
Changes among parents with low and high levels of depressive symptoms
The parent participants were divided into a lower depression group (low-parent; n = 23, 60.53%; PHQ-9 < 10) and a higher depression group (high-parent, n = 15; 39.47%; PHQ-9 ≥ 10) according to the PHQ-9 cut-off score. Compared to T1, 53.33 and 46.67% of parent participants, who were in the high-depression category, crossed the threshold, from a high to a low level of depression at T2 and T3, respectively; further, none of the parent participants who were in the low-depression category crossed the threshold from a low to a high level of depression at T2, and 4.35% of them shifted from a low to a high level of depression at T3.
Table 5 shows the results of paired samples t-tests for each group at different time points. The low-parent group reported significantly higher scores for positive affect (T2: t = −3.53, p = . 002, Cohen’s d = 0.74; T3: t = −2.70, p = .01, Cohen’s d = 0.56), mental health (T2: t = −3.06, p = . 01, Cohen’s d = 0.64; T3: t = −2.52, p = .02, Cohen’s d = 0.52), and family harmony (T2: t = −2.22, p = . 04, Cohen’s d = 0.46; T3: t = −2.25, p = .04, Cohen’s d = 0.47) from T1 to T2 and T3. The high-parent group indicated significant improvements in positive affect (T2: t = −6.00, p < .001, Cohen’s d = 1.55; T3: t = −2.73, p = .02, Cohen’s d = 0.70) and mental health (T2: t = −4.24, p = .001, Cohen’s d = 1.09; T3: t = −2.85, p = .01, Cohen’s d = 0.74) from T1 to T2 and T3. Resilience (t = −2.55, p = .02, Cohen’s d = 0.66) and family harmony (t = −3.30, p = .01, Cohen’s d = 0.85) also increased after the intervention, reaching statistical significance at T2, but decreased in the following month. Negative affect (t = 2.92, p = .01, Cohen’s d = 0.75) decreased, reaching statistical significance at T3. Significantly greater changes in mental health (Δ mental health) were observed from T1 to T2 and in the high-parent group (T2: t (36) = 2.43, p = .02, Cohen’s d = 0.82; T3: t (36) = 2.08, p = .04, Cohen’s d = 0.70; see Table 6) compared with the low-parent group. Additionally, changes in negative affect (Δ negative affect) from T1 to T3 were significantly greater in the high-parent than in the low-parent group (t (36) = −2.38, p = .02, Cohen’s d = 0.80; see Table 6).
Comparison of the study variables between pretest and post-test or one-month follow-up test based on severity of depressive symptoms of parents.
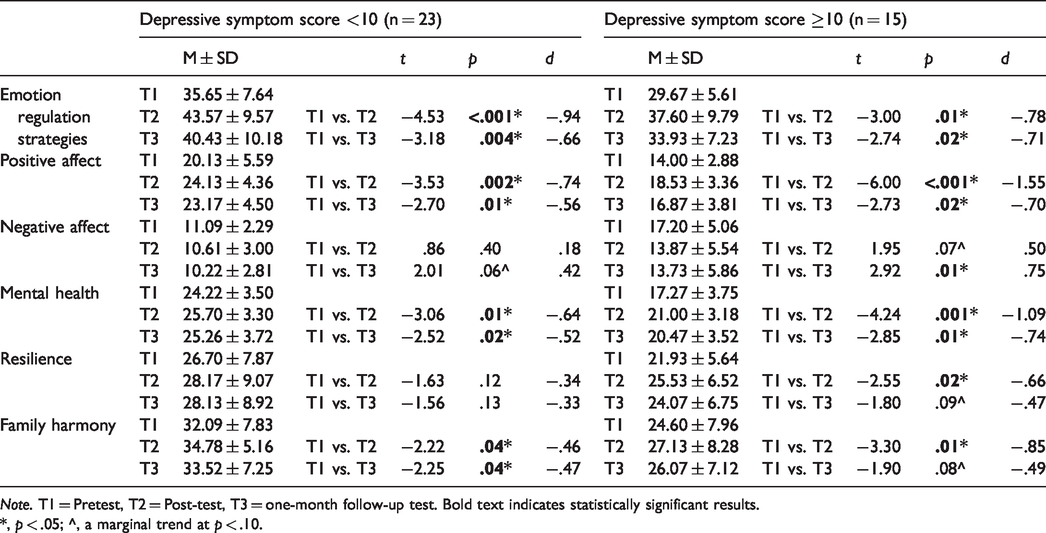
Note. T1 = Pretest, T2 = Post-test, T3 = one-month follow-up test. Bold text indicates statistically significant results.
*, p < .05; ^, a marginal trend at p < .10.
Comparison of improvements in the study variables between pretest and post-test or one-month follow-up test based on the severity of depressive symptoms of children and parents.
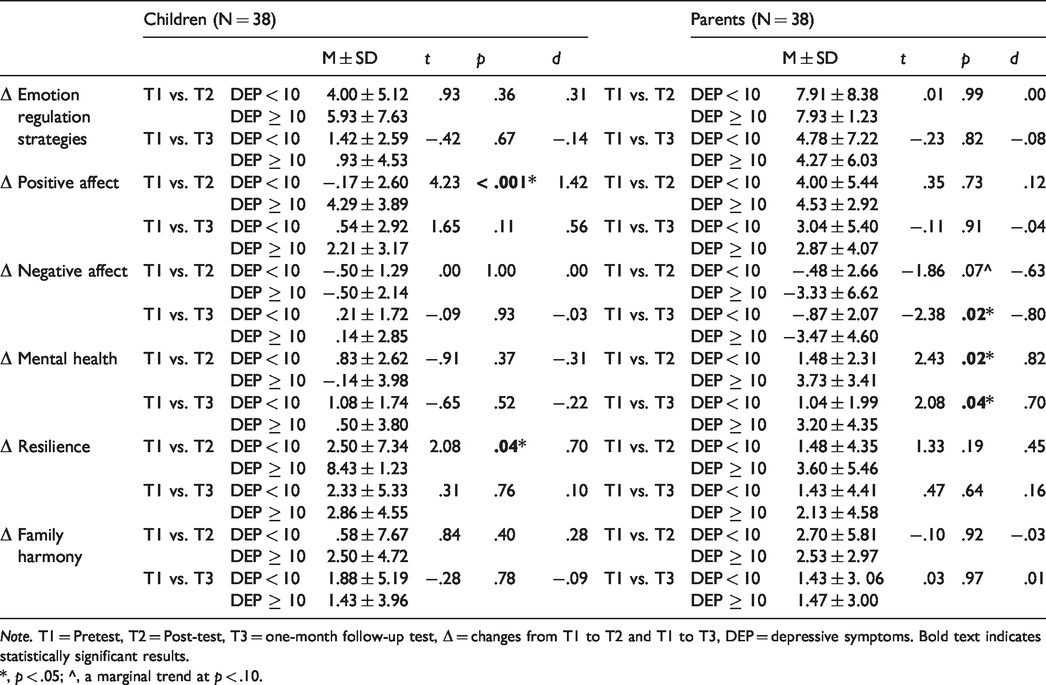
Note. T1 = Pretest, T2 = Post-test, T3 = one-month follow-up test, Δ = changes from T1 to T2 and T1 to T3, DEP = depressive symptoms. Bold text indicates statistically significant results.
*, p < .05; ^, a marginal trend at p < .10.
Discussion
An initial evaluation of this pilot study revealed that the parent–child parallel group model targeting cross-boundary children and parents can enhance positive affect, resilience, and family harmony, and reduced depressive symptoms. Both the children and the parents with higher levels of depressive symptoms generally showed greater improvement. All the positive results indicated that the theory-based psychological intervention helped to meet the needs of the cross-boundary children and parents.
In general, larger effect sizes were observed in the parents than in the children. In addition to positive affect, resilience, depressive symptoms, and family harmony, significant improvements in mental health and negative affect were present in the parents, which did not reach statistical significance in the children. The capability for emotion regulation develops throughout childhood and adolescence, so the relationships between emotion regulation and outcome variables are not as strong in children as in adults (Aldao et al., 2010). In addition, as Tan (2009) claimed, children are more inclined to control their positive emotions. It is worth noting that negative affect in the cross-boundary children at post-test decreased, reaching marginal significance (t = −1.90, p = .07), but rebounded at T3. This surge in negative affect may have been due to the stress of an upcoming school exam at the time of the follow-up test, as reported by some children in the booster session.
Our findings on discrepant benefits among participants in different levels of depression highlight the necessity of conducting screening before enrolling participants, as depressed participants benefited more from the intervention. Such screening would identify participants who are in urgent need of receiving intervention and may thereby maximize the intervention benefits (Goodman et al., 2003; Siu & US Preventive Services Task Force, 2016). For example, some of the cross-boundary children reported a happy schooling experience, and parents were not troubled (A. K. W. Chan & Ngan, 2018), which implied that they had no strong motivation to participate in an additional intervention.
It is noticeable that less than 5% of child and parent participants showed side effects of moving from a low to high level of depression. This finding highlights the risk of individuals, although a small number of participants, who suffered rather than benefited from the intervention program (Barlow, 2010; Cuijpers et al., 2006). Future studies may use classification methods and analyses, such as recursive partitioning and latent class analysis to detect these participants and examine their specific features (Beck et al., 2010; Lanza & Rhoades, 2013). Identifying these individuals—and the characteristics that distinguish them—will enable the development of tailor-made intervention components to address their needs (Beck et al., 2010; Lanza & Rhoades, 2013). To highlight side effects and improve the precision of interventions, researchers may consider using systems approaches to model a feedback loop, such that interventionists and researchers can have a broader understanding of the improved outcomes and possible side effects of a new intervention (Elias & Cavana, 2000; Midgley, 2006).
In the present study, both cross-boundary children and parents indicated benefits after the intervention, including higher levels of resilience and mental health, which partially confirmed our hypothesis. The parent–child parallel group approach demonstrated positive time effects for cross-boundary families. In the context of family, the parent–child parallel group method involved parents and children in the intervention. Interaction between parents and children may help to enhance the mental health of cross-boundary children and parents. The parent–child parallel group model also took into account the cultural characteristics of Chinese parents, who are prone to “govern” their children (Xu et al., 2005, p. 525), by separating the parents and children in different rooms for the intervention sessions. Social work practitioners, health psychologists, and educators who develop resilience enhancement interventions in multicultural context for cross-boundary families in other countries or other types of cross-boundary families (e.g. cross-boundary commuters work in one country while children live in another country, both parents and children commute cross boundaries) should take into account the cultural and contextual sensitivity of these families’ situations (Masten, 2014). For example, the culturally sensitive component of a Family Group Conference may be integrated into resilience enhancement intervention programs to serve the black and minority ethnic families (Barn & Das, 2015).
Our parent–child parallel group model was a community-based-participatory-research-approach-driven intervention. The community-based participatory research approach provided academic partners with practical insights (e.g. the needs of participants, the setting of control groups, and the choice of intervention strategies) and facilitated participant recruitment, data collection, intervention implementation, and the dissemination of the results (Bogart & Uyeda, 2009; Lam et al., 2015). Community partners found a platform upon which to become acquainted with evidence-based knowledge and scientific endeavors (Bogart & Uyeda, 2009; Lam et al., 2015). Therefore, the parent–child parallel group method with emotion regulation as the core strategy in this study was a demand-driven and practice-based intervention. Future researchers who seek to implement intervention in community settings may take the community-based participatory research approach into consideration.
Referring to the five-step model of designing and developing social programs (Fraser & Galinsky, 2010), our study mainly focused on the first three steps (i.e. Develop problem and program theories, Specify program structures and processes, and Refine and confirm in efficacy tests). Before conducting further studies, researchers and other stakeholders should review and revise the intervention protocol, and develop fidelity measures related to the essential components as next steps in the development of an evidence-based emotion regulation parallel intervention for children and parents (Fraser & Galinsky, 2010). For example, future interventions should reinforce strategies to address the negative affect and improve the capability for effortful control of cross-boundary children (i.e. the ability to shift attention and concentrate as needed, including shifting attention from negative to positive thoughts; Eisenberg et al., 2010). It is also necessary to develop specific interventions for children in response to significant stressful events (e.g. exams). Pursuant to the recommendation of Fraser and Galinsky (2010), we will continue to test the efficacy and effectiveness of the intervention in different contexts (e.g. clinical and community populations), through maintaining high control, examining intervention components, and modifying the intervention, based on our preliminary moderation results, as specified in Step 3. Fidelity criteria and measures will be developed and revised in accordance with the essential components of the intervention. Recently we have been expanding the intervention to neighboring cities and conducting the intervention among community participants who are not from cross-boundary families. There are promising results regarding improvements in positive affect, mental health, and family harmony. If possible, we would like to further extend this intervention to the clinical context and investigate the intervention effects. The clinician must be trained and certified by our intervention team.
Limitations
This study’s major limitation was the lack of a control group, which made it impossible to clearly attribute the participants’ positive changes to the intervention effects. We believe that this intervention exerted positive time effects because the intervention strategies adopted in this study have a robust empirical foundation and have been used in previous randomized controlled trials (Fabrizio et al., 2015). Our preliminary findings underscored the importance of evidence-based practice in the field of social services (Lam et al., 2015). Therefore, the next step of our study is to incorporate a control group (e.g. provision of social services related to adjustment) and conduct a randomized controlled trial to test the effectiveness of this emotion regulation intervention. Another limitation of this study was the small sample size, as the results may thus have been affected by outliers and low statistical power. For example, to obtain significant results for the children’s negative affect from pre- to post-test, according to the effect size calculated in the current study (Cohen’s d = 0.15), the total sample should have consisted of at least 351 participants (α = 0.05, power = 0.8). Larger samples and multiple assessment methods would be conducive to a more comprehensive evaluation of the interventions. Moreover, researchers could assess changes in other family members who did not participate in the intervention to test improvements in family members.
In sum, this pilot study targeted cross-boundary children and parents with the purpose of enhancing their resilience and mental health and ultimately helping them to better adapt to the cross-boundary life. Despite some limitations, this study contributed empirical evidence to the literature of cross-boundary families and demonstrated a feasible, theory-based, and cost-effective model of social services.
Footnotes
Acknowledgements
Ethics
Ethical approval was obtained from the Research Committee of City University of Hong Kong (Reference No. 3-2-201901_01).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shenzhen Philosophy and Social Sciences Fund in the 13th Five-year Plan, China (Project No. SZ2018B020), Strategic Research Grant of City University of Hong Kong (Project No. 7005158 and 7005349), and contract research project of the International Social Service Hong Kong Branch (Project No. 9231298). The implementation of this study was substantially supported by the Shenzhen Research Institute, City University of Hong Kong.
Acknowledgements
The authors thank the study participants. We also appreciate social workers of the International Social Service Hong Kong Branch, including Ms Jolian Pui Ling Chui, Ms Sheryln Chia, Mr Ming Yip Ming Chiu, Mr Torres Chi Hung Lee, Mr Alex Lap Shan Lui, Ms Florence Yim Ping Wong, Ms Cherry Mei Ling Zhong, Ms Grace Xiao Jing Xie, and Ms Joanne Ai Qiong Zhong, for their generous contributions to this study.