
Abstract
Summary
Mental Health and Psychosocial Support are integral components of the multisectoral programs addressing wartime sexual violence. In the Democratic Republic of Congo, an integrated framework known as the one-stop centre model was implemented at Panzi Hospital for delivering medical, legal, psychosocial, and socioeconomic support services for wartime sexual violence survivors. While recent developments broadly described this model with more focus on its medical pillar, there is limited knowledge on how its psychosocial support component can be harnessed in addressing wartime sexual violence. This article explored the roles and ethics of psychosocial support in integrated health services based on the research data from 11 in-depth interviews with the psychosocial support workers and desk reviews.
Findings
The findings of this study indicated that the roles and ethics of psychosocial workers in addressing wartime sexual violence are limited by the lack of adequately trained staff members, low professional status, and complex ethical challenges. In this case, psychosocial support draws more from virtue ethics and moral constructivism and less from professional utilitarianism and deontology. While both approaches are integral to providing support services, combining them is necessary for the complementarity and consistency of therapeutic processes. The study's findings also demonstrated the lack of professional social work and mental health interventions in the Congo and suggested coordinated actions engaging social work education, policy, and research developments.
Applications
We conclude that the roles and ethics of psychosocial support should be of serious concern to decision-makers, practitioners, and educators.
Keywords
Backgrounds
Sexual and gender-based violence is a global health issue of high significance. Although men and women may be equally affected by wartime sexual violence (Wirtz et al., 2014), women and children bear the biggest brunt of this phenomenon (Abrahams et al., 2014). Internationally, numerous resolutions of the United Nations Security Council recognised the disproportionate effects of conflict-related sexual violence on women and girls and urged member states to strengthen policies and health services that respond to the needs of the victims [See, for example, the resolutions 2,467 (in 2019), 2,106 (2013), 1,960 (2010), 1,888 (2009), 1,820 (2008), 1,325 (in 2000)]. These resolutions also called for monitoring, analysing, and reporting wartime sexual violence in gender-specific ways for all survivors (including boys and men) to access support services.
With the enactment of the sustainable development goals, there has been an additional momentum focusing on how health and human services may be improved to achieve the highest attainable health standards for all survivors of wartime sexual violence (see, for example, goal 3). Recent developments also highlighted the reciprocal effects and influences of biological, psychological, sociocultural, and macrosystemic factors on physical and mental health, as well as the need to support the implementation processes of biopsychosocial models of health care delivery in complex humanitarian settings (Babalola et al., 2017; Kanter, 1989; Lehman et al., 2017).
Conflict-affected settings are particularly challenging contexts where biopsychosocial models of health care are highly relevant, given the complexity of the physical and mental health conditions resulting from armed conflict, loss, and forced displacement. In line with sexual and gender-based violence, governmental and non-governmental agencies in humanitarian settings have developed integrated response programs referred to as “One-stop centre” models of care where medical, legal, social welfare and psychosocial supports are provided to survivors within the same support network, either under one roof (that is within the same health facility) or by different closely related partners (Mukwege & Berg, 2016; Mulambia et al., 2018). Although this is an appropriate model for delivering high-quality health services (Mulambia et al., 2018), little is known about the ethics and contribution of the psychosocial support workforces in this model. The lack of empirical knowledge on the roles and ethics of psychosocial support suggests that this component may be subject to significant limitations in the one-stop centre model of care implementation and in fostering the clients’ post-assault recovery.
In this article, we address the knowledge gap on the roles and ethics of psychosocial support in the integrated health services for wartime sexual violence survivors through the Panzi one-stop centre model of care. The article reports the data from in-depth interviews with 11 Psychosocial Assistants at Panzi Hospital and a desk review on Mental Health and Psychosocial Support in the Democratic Republic of Congo. The article argues that the roles and ethics of psychosocial support are underestimated and sometimes overlooked at the policy and agency levels. Psychosocial workers are also subject to low professional status and lack adequate guidelines and skills to intervene at their fullest potential.
Conflict-related sexual violence and the lack of mental health and psychosocial support infrastructures in the Congo
Recent developments on wartime sexual violence have moved from seeing this phenomenon as a natural product of conflict stemming from the suspension of societal norms during combat to seeing it as a war strategy, e.g., (Bosch, 2019; Nagel & Doctor, 2020). For instance, Bartels et al. (2010) argue that sexual violence in armed conflict is more an expression of power and domination than an instrument of sexual gratification. Baaz and Stern (2013) caution against the “desexualisation” of rape in armed conflicts as this phenomenon has complex root causes, including biological ones. Beyond these conflict-related motivations, wartime sexual violence is embedded in toxic masculinity that seeks to objectify the feminine gender (Alexandre & Moke Mutondo, 2021). Notably, the idea that rape against men, women and children may be used in armed conflict to punish and humiliate communities is grounded in its conceptualisation as a “weapon of war” (Mukwege & Nangini, 2009, Kasherwa and Twikirize, 2018b). Therefore, the view of wartime sexual violence as a weapon of war posits that combatants may perpetrate violence against women and girls based on group membership and gender identity (Park, 2017). In this case, sexual assault may be accompanied by other forms of gender-based violence explicitly targeting women and girls because of their perceived vulnerability, including massive killing, chopping-off private organs, torture, and abduction (Stark & Wessells, 2012).
Sexual and gender-based violence targeting women, children and men can also be motivated by the need to subjugate the perceived masculinity-related authority of adult men and elders to protect their families or communities. In this case, wartime sexual violence may occur as one of the myriad forms of sabotage and vandalism acts perpetrated by combatants, including torching houses, devastating crops, human abductions, vandalising stores and schools, or other public infrastructures. In addition to their gender and identity, women are targeted during conflicts owing to their procreative roles in sustaining lineages (Sharlach, 2000). Indeed, this reflects the genocidal dimension of the ongoing civil wars and armed conflicts in the African Great Lakes Region countries since the Rwandan genocide outbreak in 1994, which brought significant challenges to the peace and stability of the neighbouring Congo (Kasherwa, 2019).
Likewise, in a comparative study of wartime sexual violence in Guatemala and Peru, Leiby (2009) indicates that sexual violence in both countries has been used to commit genocide and ethnic cleansing and weaken the opposition. In the eastern Congo, rape against men, women and children is reported to be an effective method to maintain control over mineral sites, as armed perpetrators expect that local populations will flee and leave the land open for economic exploitation (Banwell, 2014). Wartime sexual violence is more complex than how it is often portrayed in most humanitarian reports. Understanding this phenomenon in a unidirectional view of “a weapon of war” may overlook the underlying cultural, political, and socioeconomic factors. Importantly, like sexual violence in relatively peaceful settings, wartime sexual violence involves the “abuse of power” and may be “organised or planned” to serve militarist aims (Kasherwa & Twikirize, 2018a).
Conversely, some cases of wartime sexual violence may not target the victims based on their ethnic groups or ideological orientations. Some perpetrators perceive collectively raping the same victims as essential for creating strong bonds and reinforcing cohesion among militiamen (Bitenga Alexandre et al., 2021). Schneider et al. (2015) contend that some commanders deliberately provide incentives such as drugs, alcohol, and marijuana to their combatants to encourage them to perpetrate acts of violence, including sexual violence against civilians. This finding contrasts with Baaz and Stern (2008), who wrote against the weapon of war discourse. We argue that these different representations of sexual violence in the eastern Congo should be seen as complementary rather than contradictory, as each framing encompasses some uniqueness. For instance, research evidence reveals that while some commanders explicitly or implicitly encourage sexual violence in armed conflicts (Mukwege & Nangini, 2009; Schneider et al., 2015), motivations of sexual violence transcend strategic purposes and include myriad sociocultural, political, legal, and socioeconomic factors (Baaz & Stern, 2013). Hence, the focus on wartime sexual violence as a weapon of war may not account for the different ramifications of this phenomenon, such as gender inequality and the violence perpetrated by civilians. Some research studies indicated a continuum of rape committed by civilians and armed groups in the aftermaths of armed conflicts, e.g.: (Christian et al., 2011; Kasherwa & Twikirize, 2018a; Spangaro et al., 2013). The stress of armed conflict, loss, and forced displacement may also increase levels of intrafamilial violence, including domestic violence, intimate partner violence, child sexual abuse (CSA), physical or emotional abuse and neglect.
The various patterns and contexts of wartime sexual violence suggest different mental, emotional, and health complexities, highlighting the need for systematic support services for survivors and perpetrators. For instance, wartime rape may result in rape-induced pregnancy, children born from rape, obstetric fistulas, HIV/Aids transmission, and mental and developmental impairments, which may be experienced differently among survivors (Kasherwa & Twikirize, 2018a). While different humanitarian interventions are in place to provide emergency responses, most survivors of wartime sexual violence are experiencing lifelong health and mental outcomes that require more significant interventions.
However, Mental Health and Psychosocial Support infrastructures are underdeveloped in the Congo and subject to social stigma as people using these services may be labelled as becoming “mad” or “crazy.” Besides, Mental Health and Psychosocial Support services are not adequately funded and are often relegated by administrative authorities. The few support programmes of the humanitarian agencies are not accessible to the large populations experiencing mental problems, and most mental health conditions, such as depression, dissociation, and anxiety, are not often recognised as such because of low mental health literacy. Clinical practices primarily focus on the physical health outcomes of sexual violence in medical terms. There is limited focus on mental health and the social, cognitive, or emotional effects of assault experiences among survivors at policy and frontline agency levels.
Understanding the Panzi One-stop centre model of care
The Panzi One-stop centre model of care was developed at Panzi Referral Hospital and Panzi Foundation to address the complex needs of adult women survivors of sexual violence through a holistic (person-centred) care model. Panzi Hospital is located in Bukavu town in the eastern Congo and is internationally recognised as a Centre of excellence in providing holistic care to wartime sexual violence survivors. It was founded by Doctor Denis Mukwege (Nobel Peace Prize Laureate 2018) in 1999 in Bukavu and aimed to provide high-quality reproductive health care services to local populations. Cumulative reports of Panzi hospital indicate that they have treated 30,521 survivors of sexual violence from 1999 to 2020, 1.5% of whom are men and 28% are girls below 18 years. The Hospital has 245 beds and 120 staff members, of whom 60% are women, and 40% are men (Panzi Foundation, 2019). At the time of data collection for our research, only 18 staff members (all women) worked in the psychosocial support teams of Panzi Hospital and Panzi Foundation. Doctor Denis Mukwege created the Panzi Foundation in 2008 to complement the medical services they provided at the hospital. Through this foundation, they provide empowerment-driven programs like legal support, vocational training, and counselling services. Together, Panzi Hospital and Foundation work to achieve the primary goal of providing holistic or integrated support services to sexual and gender-based violence survivors.
Through this model, they provide a variety of free-of-charge services articulated in four significant pillars: medical, psychosocial, socio-economic, and legal pillars. In this sense, the model is an outstanding response to the detrimental effects of wartime sexual violence. The entry point for most survivors is the medical pillar, which revolves around psychosocial support, legal assistance, and socioeconomic assistance. However, before the clients are referred to a physician, they are received by psychosocial assistants who listen to them, identify their needs, and provide them with initial counselling services. The medical pillar addresses the physical consequences of sexual/physical violence, including sexually transmitted diseases, unwanted pregnancy, and physical injuries. The medical team is composed of physicians, nurses, and laboratory technicians. The model also involves the socioeconomic and legal pillars. The socioeconomic pillar provides a wide range of vocational training in income-generating activities for the socioeconomic reintegration of the clients in their communities. The legal pillar aims to support women in deciding whether to take legal action against their offenders. It involves listening to the client's stories (in Panzi's legal support clinics), raising their awareness of their human rights, and supporting the clients’ legal processes against the alleged perpetrators in the court.
Methodology
The research design was exploratory, descriptive, and cross-sectional (Mills & Birks, 2014). Its exploratory aspect addressed the research question based on the assumption that there is a great deal of uncertainty and limitations in the existing body of knowledge on the roles and ethics of psychosocial assistants in the one-stop centre model of care and clinical settings, more broadly, while the descriptive aspect aimed at an evidence-based analysis of the phenomenon being studied (Vaismoradi et al., 2013). The study was cross-sectional because the data were collected at only one point (Rindfleisch et al., 2008). The study employed a qualitative approach, including in-depth interviews with psychosocial support workers and a desk review of the literature on psychosocial support in the Democratic Republic of Congo. This method is appropriate when seeking an in-depth understanding of how participants construct meanings from their personal experiences in a specific context (Goodman, 2001; Riessman & Quinney, 2005) and is relevant when exploring a topic on which there is limited knowledge. The study population involved psychosocial assistants, also known as case managers, engaged in the Panzi one-stop centre model of care for wartime sexual violence survivors.
The sample size for this study was 11 participants interviewed at Panzi Referral Hospital in eastern Congo. All participants were women aged 30 to 64. For the desk review, three types of literature searches were conducted: the national policies on psychosocial support, key reports and working tools of the Panzi One-stop centre model and peer-reviewed publications on wartime sexual violence. Since all interview participants worked in the Panzi one-stop centre framework, the study adopted convenience sampling. Data was collected using an in-depth interview guide around a set of fluid questions directed to the psychosocial workers. Generally, respondents were asked about their profiles, roles, and functions, as well as the ethical challenges and experiences of providing support services to wartime sexual violence survivors. Interviews were held at Panzi Hospital in French and Swahili. Each interview took approximately 60 min to complete.
To provide an account of the validity and reliability, the study was based on data triangulation from the desk review and individual interviews (Blanche & Durrheim, 1999). Data collection and analysis were conducted concurrently. Thematic analysis was used to identify patterns in the interview records (Langdridge & Hagger-Johnson, 2009). Thematic Analysis offers an accessible and theoretically flexible analytical approach and a rich, detailed, yet complex account of the data (Nowell et al., 2017). It was employed to link the structure of the research question to the accessed data and to allow a detailed and nuanced interpretation of the data from the field (Braun & Clarke, 2006). We presented examples of quotes from research participants that accurately illustrated our arguments. These quotes reflected the salient themes we extracted from the data. No elements of participants’ identities, such as name or age, were mentioned. This helped to ensure that their identities were protected regarding their professional relationships with the agencies and client service relationships. All other ethical principles for studies involving human participants were adhered to. Participants provided informed verbal consent and entitlements such as confidentiality, voluntary participation, and the right to withdraw from the study at any time with no penalty. The combination of different data collection methods (interviews and desk reviews) yielded significant prospects for data triangulation and for key themes to be extracted from the data while answering the research questions. Overall, this research generated new insights using appropriate methodological approaches.
Findings
Roles of psychosocial assistants and interprofessional relationships in the Panzi model
Psychosocial Support is the most complex component of the Panzi one-stop centre model of care. It responds to survivors’ multiple social, emotional, and psychological needs. Indeed, wartime sexual violence survivors often face complex mental health conditions such as chronic anxiety, depression, dissociation, shame, guilt, self-blame, and social stigma. Thus, this pillar assumes that the recovery of survivors is a complex process that goes together with psychological and social healing (Panzi Foundation, 2019). This pillar thus encapsulates two subcomponents: psychological care, which includes psychotherapeutic techniques addressing severe trauma, and psychosocial support, which involves welcoming the clients, assessing their needs, providing initial counselling services, and explaining to them the confidentiality aspects of the treatment process. The Psychosocial assistants interviewed in this study reported that their roles encompass case management, information gathering and sharing with other services, helping the clients feel safe, building emotional resilience and trust, and gaining a sense of self-worth.
Likewise, the Panzi handbook of holistic care ascribes different roles to Psychosocial assistants: welcoming the client at the hospital, conducting the initial needs assessment, gathering the socio-demographic information, and making a holistic care plan with the client (Panzi Foundation, 2019). Participants in the interviews also mentioned that they often provide counselling services to survivors and their family members, such as husbands, parents, or children. They also played a vital role in the family and community reunification process and in organising the referrals of the clients to other services out of the hospital. Psychosocial assistants were also involved in health promotion activities (animation), conducting play therapy sessions, advocacy, court case follow-up, family therapy, and mediation.
As to how these tasks align with the workers’ profiles and skills, a participant in the interviews reported: We are learning some of the skills while practising. Being from a nursing background, I already had some skills in case management. Today, I feel very confident working in this environment and helping many women recover from their experiences. (Participant 03)
The roles of psychosocial assistants in the one-stop centre model are immensely complex, raising several critical issues relating to their professional identities and inter-professional relationships. For instance, the psychosocial assistants working at Panzi hospital are subcategorised into those in charge of the follow-up of the client's progress throughout the healing process, those in charge of the clients’ reinsertion, reintegration processes and referrals to other providers and those who follow up the clients’ legal cases in the court. These categorisations indicate the interprofessional collaborations psychosocial assistants are expected to undertake with other legal, nursing, or medical professionals. While it was helpful for the different categories of psychosocial assistants to have adequate social work training and follow appropriate protocols in their practices, their professional identities and interprofessional relationships were often at odds with their complex missions. As stated earlier, we interviewed 11 psychosocial staff members (all women) directly involved in the Panzi Hospital's and/or Foundation's psychosocial support programmes. Most of these Psychosocial assistants (n = 6) were nurses by training with limited training in social work approaches to survivor-centred recovery. The five others, respectively, had a Bachelor of Arts degree in social work (n = 2), sociology (n = 1), and rural development (n = 2). The psychosocial assistants from nursing backgrounds had at least a 3-year university degree in nursing studies (n = 3). In contrast, the others were trained in nursing and midwifery at a technical high school level. These workers mentioned that they had received short professional training and local capacity-building workshops run by seniors from overseas countries in stress management, case management, and family mediation.
In terms of interprofessional collaborations, there was a blurred image of how psychosocial assistants can and do collaborate with other clinical practitioners. For example, in the one-stop centre, psychosocial assistants are supposed to work under the supervision of clinical psychologists. Together, they form what is referred to as psychosocial support workers. While this arrangement provided good professional outcomes in some cases, it was limited in other complex cases where the psychosocial assistants and the clinical psychologists lacked adequate social work skills.
Indeed, social work as a profession and field of practice is significantly under-recognised in the Congo. The few existing programs and developments are not substantially supported at institutional and policy levels. While we expected the few social work-trained workers who participated in this study to react differently to their roles compared to those from nursing and other backgrounds, their narratives were not too different. While the social work-trained psychosocial assistants had good theoretical understandings of some issues, they often needed more practical and experience-based illustrations of how these issues could be addressed. These social workers were recent graduates of the 5-year bachelor's degree program in social work that was launched at Université Evangélique en Afrique (UEA Bukavu) in 2013. In their training, these workers had completed their placement under the supervision of non-professional social workers, and most of their learning activities were facilitated by non-social workers. All these factors are the backdrops against which we contextualised their narratives.
Also associated with this is the low professional status of psychosocial assistants in the one-stop centre model. Unlike the other staff members, the roles of psychosocial assistants are sometimes overlooked. For instance, Mukwege and Berg (2016, p. 4) 1 state that “psychosocial care starts with meeting a psychologist to identify needs and plan for a specific treatment, which is carried out individually or in a group.” It remains unclear, from this perspective, what the roles of psychosocial assistants might be and how they could be distinguished from those of psychologists in the provision of integrated health care. Likewise, the Panzi Handbook of holistic care recognises case management as an integral component of the one-stop centre model. Still, it provides no standard profiles, academic backgrounds, or coordination arrangements for case management. Moreover, the handbook mainly refers to case managers as individuals who guide clients through the healing and recovery processes. Still, limited attention is paid to other duties such as family reunification, mediation, and community-based therapies, which may require specific social work and cultural competencies. Participants in the interviews reported that “there is no standardised protocol they follow in conducting a family mediation or reunification in the case of family violence or children born from rape” (Participant 04). Besides, it is unknown whether psychosocial support should be mandatory or optional for all potential clients in these medical settings. The programme also lacks a prevention component, and there is a limited understanding of the long-term physical and mental health outcomes of trauma on the survivors. Given the limited mental health literacy, there is a stigma of mental illness and other rape-induced conditions. But little is known about how psychosocial support workers can address this challenge at the community level.
Responding to the complex needs of sexual violence survivors
Working with wartime sexual violence survivors is always associated with multiple complexities. The complexities of this process in the Panzi one-stop centre model of care were exacerbated by the workers’ lack of adequate training and experience, coupled with the complex needs of most clients. From what we noted in our interviews, the work of psychosocial assistants often exceeded their roles and expectations prescribed in the Panzi handbook of holistic care. Besides, there was limited communication among key staff members in the different pillars of the One-stop centre model of care, which further complicated the tasks and schedules of psychosocial workers. For instance, one participant in this study reported: It happens that a client enters the program at Panzi while they have started receiving similar services from rural health clinics or other partners. In this case, there may be duplication and fragmentation of the interventions as it is tough to substantiate the kind of interventions they had received and, you know, … how this might be complementary to ours. (Participant 10)
Participants also mentioned the dilemma of balancing the requirement to respect cultural norms and the religious beliefs of the clients and to safeguard human rights while responding to the complex needs of their clients. Importantly, given the colliding effects of armed conflict, poverty, and limited health services infrastructures, psychosocial assistants often faced the tedious task of suggesting solutions that align with these multiple complexities. This was particularly challenging given the limited social work qualifications of the psychosocial assistants and the lack of other mental health programmes to which some clients could be referred for complex clinical interventions. For instance, a participant said: Some religious beliefs are at odds with the solutions we suggest to our client's problems. I remember working with a client who had conceived a child from rape and still who said she did not want to terminate that pregnancy, as deliberate abortion is considered to be against the will of God. (Participant 07)
It is worth mentioning that even when some survivors may choose to terminate a rape-induced pregnancy, they are often bound by existing anti-abortion legislation and religious or cultural norms. Another ethical challenge for Mental Health and Psychosocial Support programs in the one-stop centre, more generally, and the Panzi model, in particular, is how to develop interventions tailored to the specific situations of every client to align with the social work principle of individualisation. For instance, there is a need for specific interventions for men survivors of rape, survivors of sexual abuse, children born from rape, or survivors whose conditions may be compounded by physical impairments, social stigma, forced displacement and chronic poverty.
From a gender perspective, existing responses to sexual violence in the Democratic Republic of Congo have mainly been developed to address sexual violence against adult women and need to be re-adapted to other categories like male survivors, children, and sexual minorities. Accordingly, the psychosocial assistants who participated in this study were all women. They reported how several male survivors often struggled to share their stories with them as female allied health professionals. There are also significant limitations regarding the gender dynamics and structural contexts in which wartime sexual violence occurs, including the lack of appropriate gender competencies and intersectional frameworks in the interventions and systemic barriers to gender equality in the country. Participants reported that Panzi Foundation and Hospital provided some training to their staff members and service users in gender roles and other aspects of gender-based violence. However, a more detailed understanding of gender construction and cultural norms about gender is needed to enable the workers and clients to design interventions well-informed by contemporary gender perspectives.
Indeed, participants in this study mentioned the need for further training in clinical social work ethics, gender, counselling, case management, and opportunities to exchange experiences with colleagues abroad. Capacity development in gender perspectives could help to address gender-specific issues arising in counselling practices with clients from different genders. Since the social work and mental health professions are underdeveloped in the Democratic Republic of Congo, many academic and professional collaborations can be pursued for co-engagement and sharing experiences with colleagues worldwide. Participants also mentioned organisational problems such as limited equipment and low professional status, which equally affected their positive contribution to the provision of support services. For instance, one participant in our interviews stated: One of the critical challenges is insufficient counselling rooms. There is no limitation on the number of clients we receive per day, as is the case for medical doctors (5–6 patients per day) and psychologists (4 patients per day). I wish we also had well-constructed counselling offices like those of medical doctors to be able to work in confidentiality. Sometimes, I am obliged to move to the shed building to receive my patients if the other colleagues still use the two counselling offices shared by 10 of us. (Participant 01)
This quote illustrates the negative impact of the low professional status of psychosocial assistants in the hierarchical health sector apparatus. This resonated with the experience of another psychosocial assistant who reported how the lack of adequate counselling rooms often breached confidentiality in the counselling interactions with her clients: We receive many patients in the counselling office, but we don’t have enough space. We have been sharing two small counselling offices with ten other colleagues, which often breaches privacy, as there is communication between the two offices. When I talk to the client in the office, people in the other office can hear everything. (Participant 02)
The low professional status and inadequate infrastructures limited the potential of the workers to maintain vital ethical principles such as privacy and confidentiality and exposed them to heightened risks of burnout and compassion fatigue. The words of participants 2 and 1 exemplify the trends of most participants in our interviews to discuss their challenges, status, and roles compared to those of other practitioners in the same agency, such as physicians, nurses, and clinical psychologists. These comparisons highlighted the frustrations that may exist in interprofessional collaborations and how these frustrations may lead to disproportionate effects of burnout and vicarious trauma among practitioners of a lower professional status.
At the policy level, the national protocol for Mental Health and Psychosocial Support in the context of sexual violence presents a hierarchical framework, which places psychosocial assistants at the second lowest level of the pyramid (see Figure 1). This also entailed lower salaries and contract-related issues among support workers. Most of the psychosocial assistants (n = 6) involved in the study had a permanent contract, while the others (n = 5) had a fixed-term contract of up to 12 months. Psychosocial assistants discussed their concerns about building productive helping relationships with their clients in the limited timeframes of these short-term contracts. Participants also reported that their salaries are estimated daily and include US Dollars 7 per day plus reimbursement of reasonable costs of transportation, housing, and family allocations that are calculated on a case-by-case basis. While these professional complexities demonstrated the different financial and budgeting challenges of clinical and human services, some practical measures, such as employing allied health professionals on long-term contracts, could help to improve the outcomes of their engagement with their clients and recognition in clinical settings.
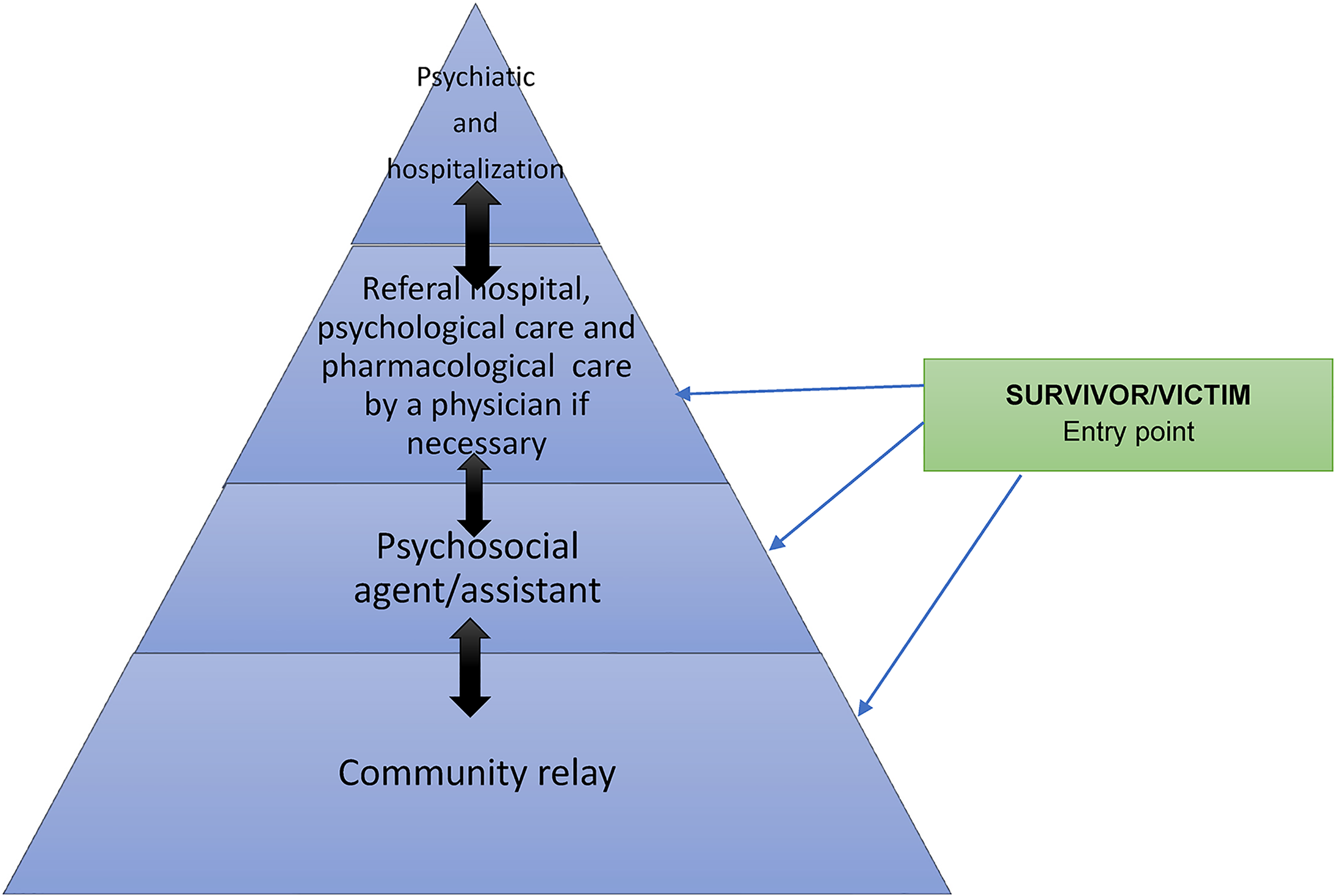
Pyramid of interventions in Mental Health and Psychosocial support of SGBV survivors. Adapted from National Protocol for MHPSS, (Min. Health & Min of Gender… DRC, 2012).
Ethics of psychosocial services for sexual and gender-based violence survivors
The study's findings suggest that the ethics of psychosocial support draws from virtue ethics and moral constructivism and less from professional utilitarianism and deontology. McBeath and Webb (2002) define virtue ethics as a reaction to the predominance of Kantian, utilitarian and meta-ethical theories which concern either giving ethical directives to specific moral problems or explaining the meaning of the predicate “good.” In social work and other professional practices such as medicine, virtue ethics mainly involves good practices resulting from habit, self-reflection, and morality (Adams, 2009; Pullen-Sansfacon, 2010). Hugman et al. (2021) argue that the application of virtue ethics in the social work profession draws from other disciplines such as business, health and education and involves common-sense related values such as courage, compassion, care, hope, perseverance, justice, humility, practical wisdom, and integrity. An integral aspect of virtue ethics is that professional actions are based on routine/experience and moral character and less on rational choices or utilitarianism. As for deontology, Reiman (2009) argued that this is an ethical theory that distinguishes optimal and non-optimal professional practices according to a clear set of rules. In social work, these processes protect autonomy, believing that autonomy enables a person to follow a universally accepted moral code. This also suggests a consequentialist perspective to social work practice through which people make choices that result in best practices.
In the Democratic Republic of Congo, the two significant legislations on psychosocial support (namely, the ministerial decree on social assistance 2 and the national protocol for Mental Health and Psychosocial Support 3 of 2012) do not provide any firm guidelines for psychosocial support services. For example, the ministerial decree on social assistance briefly states that social assistants should have “good conduct and good behaviours” (Art 7). Likewise, the national protocol for Mental Health and Psychosocial Support suggests that workforces should have good moral character and be able to apply principles of confidentiality, empathy, non-judgement, active listening, and self-reflection. However, there is no standardised code of conduct for allied health workforces in the existing interventions addressing the violence against women and children in the Congo.
Participants discussed their ethics in relation to moral values such as having a “good heart”, “courage”, and “perseverance”. They never linked the ethics of working with sexual violence survivors to rational choice models or evidence-based practices (EBP). For example, one psychosocial assistant reported: All of us are working with great determination and collaboration. Everyone shows excellent momentum to ensure that the patient is given excellent services. Therefore, part of our job involves welcoming the patients, listening to their problems attentively and referring them to the necessary services within the hospital. The work, therefore, requires that all of us have a good heart and perseverance, given the complexity of the cases we receive. (Participant 04)
Virtue ethics was also reflected in the account of another participant who said: Being a psychosocial assistant means having a big heart and great empathy. We aim to cultivate strong bonds with the women [survivors] while welcoming them to the Hospital. You know, this really makes them feel valued and empowered. (Participant 8)
While some participants were well-informed of these ethical principles, they needed standardised ethical guidelines, which made their practices ambiguous or inconsistent in different cases. Given the diversity of their academic backgrounds, there needed to be an evidence-based model to inform the knowledge-based practice systematically. The ethics of psychosocial support workers also overlaps the features of moral constructivism in that participants in this study described their actions and roles as the result of practical reasoning and less a result of rational choices based on pre-established norms and principles. This aspect was reflected in the narrative of (participant 05) which holds: I provide good services to women suffering from complex trauma due to sexual violence. …. Uhm, well, … this is not because I learned this at school but because of self-reflection, common sense, and knowledge of cultural values. Some of the training we also received from colleagues from Belgium have been helpful. (Participant 05)
While virtue ethics and moral constructivism are critical and might ensure individualised interventions, they may not always be adequate to achieve the duties and responsibilities of responding to the complexities of sexual assault through justified ethical standards. Given that morality is often shaped and assessed based on dominant discourses in public, it is more likely that decision-making using virtue ethics and moral constructivism becomes subject to the significant bias of the workers. Besides, given the complexity and sensitive nature of wartime sexual violence, virtue ethics must be combined with standardised utilitarian approaches and deontological practices. Hence, having a standardised code of conduct and protocol may help to address some of these issues.
Towards Ethical psychosocial support services for wartime sexual violence survivors
This study analysed the roles and ethics of psychosocial support workers in the integrated health services for sexual and gender-based violence survivors. It adds to the existing body of knowledge that highlights the lack of consensus (both in policies and developments) on what is and should be the roles, scopes, and ethics of Mental Health and Psychosocial Support in complex humanitarian settings (Andersen et al., 2020; Loughry et al., 2003; Nie & Olson, 2017; Torre, 2019). Results from our inquiry suggest that although the social work profession is still under-recognized in the Congo, clinical social workers can play an instrumental role in delivering ethical psychosocial services to wartime sexual violence survivors. Findings from this study aligned with the evidence from other conflict-affected settings such as Syria, South-Sudan, Maynard, Ecuador, and Columbia, where Mental Health and Psychosocial Support interventions are extremely limited despite the high prevalence of mental health issues resulting from armed conflicts (Kamali et al., 2020; Lee et al., 2018; Loughry et al., 2003).
Our findings also indicated that the roles of psychosocial support workers often exceeded case management or psychosocial assistance and required more vital skills, theoretical underpinning, and reflexivity from both the workers and the agencies. However, the lack of social work-trained allied health professionals in the Congo meant that the workers always performed tasks exceeding their roles and experiences. Their roles remained prescriptive and were limited by the lack of qualified allied health professionals in many parts of the country. Given the lack of qualified social workers, employing nurses and other non-social workers was also acceptable. However, this approach may not always be adequate when providing Mental Health and Psychosocial Support services to people experiencing complex trauma. Evidence from previous studies revealed that therapeutic Mental Health and Psychosocial Support interventions could cause significant harm to the clients and breach fundamental ethical standards when provided by unqualified practitioners (Carll, 2008; Jo de Berry, 2004; Raslan et al., 2021).
Since armed conflicts are commonly associated with complicated mental health and psychosocial problems (Purgato et al., 2018; Tol et al., 2020), it is more critical for countries emerging from armed conflicts to enact more robust policies and to have adequately trained Mental Health and Psychosocial Support workforces to address these complexities effectively. In line with this, policies and interventions in some humanitarian settings have moved from mere psychosocial support to armed conflict survivors to include Mental Health and Psychosocial Support in health systems (Andersen et al., 2020; Kamali et al., 2020; Tol et al., 2020). However, there is a limited understanding of the roles and ethics of psychosocial workers in the country. For instance, Osako (2007) used the words social activism or social interventionism, and social assistance to describe the roles of psychosocial workforces in different practice areas, such as human services, social education, sociocultural animation, counselling, family therapy, readaptation, and networking. Osako also argued that the roles of these social workforces in the Congo often exceeded institutional arrangements and included both informal communitarian performances and professional approaches, as well as public and private agencies.
Thus, decision-makers may often adopt a more systematic approach of including Mental Health and Psychosocial Support as an integral component of health care, with comprehensible referrals and outreach frameworks (Carll, 2008; WHO, 2012). As demonstrated in this study, policies and programs in the Congo are highly prescriptive and may also significantly impact the helping processes and support responses. Essentially, some guidelines suggested that these allied health professionals should only have a secondary school diploma or equivalent to a degree in social sciences (see the national protocol on Mental Health and Psychosocial Support). As we tried to check the curriculum of the social sciences fields provided at the secondary school level in the Congo, it is not designed to equip the learners with the necessary skills for providing psychosocial support to survivors of sexual violence. Likewise, the Université Evangélique en Afrique (UEA), which offers a social work degree, needs significant help regarding curriculum review, adequately trained social work educators, and teaching resources to enhance the quality of social work education. UEA is one of the rare Universities offering a comprehensible generalist Bachelor of Social Work (BSW) program in the Congo. There is a need to support the implementation of more BSW and Master of Social Work (MSW) programs in the country.
Policies and practices of Mental Health and Psychosocial Support in the Democratic Republic of Congo are also at odds with the guidelines of key international agencies such as the World Health Organization (WHO), Centre for Disease Control and Prevention (CDC) and Inter-agency Standing Committee (IASC), which suggest rich content of Mental Health and Psychosocial Support protocols; adequately trained practitioners and ethical standard of such interventions in humanitarian settings (Carll, 2008; Kamali et al., 2020; Ventevogel, 2018; WHO, 2012). In addition to the ethical challenges discussed in this article, organisational issues related to the supervision, referral, response, and prevention of sexual violence were not consistently explicated in policies and individual interviews with the practitioners. Notably, participants in the discussions reported that there is no other referral protocol for complex mental health conditions outside of the One-stop centre model. They often referred such cases to experienced medical doctors, only one of whom recently completed a Master of Arts degree in psychiatry abroad.
Due to the lack of qualified professional social workers and other allied health professionals in the country, the content and ethics of Mental Health and Psychosocial Support may be prescribed by non-qualified decision-makers. Practitioners providing Mental Health and Psychosocial Support Services in clinical settings are, therefore, subject to low professional status, as exhibited in the data from the study. Recent studies conducted with similar health practitioners, such as midwives and nurses, revealed that low professional status and low level of autonomy could significantly impact the quality of care, lack of recognition in the medical hierarchy, and low level of autonomy for workers to provide services on their fullest potential and confidence (Bogren et al., 2020, 2018). Accordingly, the efforts of Panzi hospital to include mental health and psychosocial support in the integrated health care for wartime sexual violence survivors may not be effectively harnessed due to similar reasons as those reported by previous researchers.
As for ethics, our research findings demonstrated that there is no standardised code of conduct for Psychosocial support workers in the Sexual and Gender-based violence field in the country. Practitioners implicitly draw from virtue ethics and moral constructivism, whereby they apply moral principles in the profession based on intuitive common sense and cultural values and not on theoretically justified ethics. Indeed, moral character is recognised as an essential element of social work ethics that helps to model ways of life and counselling over morally problematic situations (Clark, 2006). However, this approach is inexhaustive for addressing the complex trauma of wartime rape. Scholars suggested that social workers in complex settings adopt a pluralistic ethical approach to what is good and right and seek to find a way to balance moral ideas and scientifically justified evidence (Hugman et al., 2021).
Scholars also suggested that Mental Health and Psychosocial Support workforces in complex humanitarian settings adopt a principle-based approach (Adams, 2009; Hugman et al., 2021). Given the complexity of wartime rape, professionals working with survivors must align with current social work debates on trauma-informed practices, cultural safety, co-regulation, and self-regulation in addition to social work principles of confidentiality, do no harm, consent, gender, and diversity issues. Regarding the personal identity of the practitioners, the efforts of employing women psychosocial assistants, as Panzi Hospital does, is a good practice example. There is a plethora of research highlighting the need for counselling clients to be consulted by people of the same gender as themselves, especially in the case of sensitive issues such as sexual and gender-based violence (e.g., Landes et al., 2013; Mathews et al., 2013). However, this should be cautioned since there are also boys and men survivors who would hardly disclose their experiences to female case managers, as exhibited in our participants’ narratives. It is essential to clarify the supervision framework and scope of psychosocial support and how this delineates the roles of clinical psychologists and other support workers like nurses and physicians in the different pillars of the One-stop centre model.
As critical reflections for Mental Health and Psychosocial Support in the integrated services for sexual violence victims, we suggested to policymakers, practitioners, educators, and the other stakeholders coordinated actions encompassing:
Increased resources and efforts for appropriate education of clinical social workers, case managers and other Mental Health and Psychosocial Support workforces in the Congo. These efforts should focus on training qualified social workers (at BSW and MSW levels) and offering different options of qualifying programs to practitioners from other backgrounds (e.g., nursing, sociology, or psychology) who wish to get social work professional accreditations. This process also supports a drive towards Evidence-Based Practices (EBP) – with an emphasis on the “social” or psychosocial dimensions of service delivery, Adopting a tailored intervention strategy that effectively integrates individual/therapeutic and environmental dimensions in the provision of Mental Health and Psychosocial Support services through coordinated packages, Ensuring that psychosocial workforces are equipped with adequate professional protocols, scopes, and safe working environments, Involving psychosocial workforces in the decision-making processes for the fight against wartime sexual violence and decisions about human resources for health, Incorporating the aspects of clinical social work ethics and case management in the curriculum for the training of social workers in the Congo, Elaborating and implementing a comprehensible code of conduct for allied health services in Mental Health and Psychosocial Support services provisions.
Study limitations
This study has some limitations, including its cross-sectional design and the lack of interviews with service recipients and decision-makers. Indeed, the study did not aim to generalise findings to broader populations. Instead, the focus was on the experiences of providing psychosocial support in the framework of integrated health services for wartime sexual violence survivors. Hence, engaging a small number of participants was deemed appropriate. However, collaborating with larger groups of practitioners, including physicians, clinical managers, and service users, could yield additional perspectives. Furthermore, the study's cross-sectional design and the sensitive nature of the discussions meant that we could only interview participants who had worked in the hospital for an extended period exceeding six months.
Conclusions
The findings of this study suggest that the roles, contents, and ethics of psychosocial support in complex humanitarian settings should be of serious concern to decision-makers, practitioners, and educators. Our findings also indicated that despite the ethical complexities of their work environment, social work-trained psychosocial workers could certainly contribute to a more effective One-stop centre model of care for wartime sexual violence survivors. As demonstrated in the study, psychosocial assistants in the Congo are driven by virtue ethics and moral constructivism. Their role in the integrated frameworks of health service delivery is limited by inadequate training, low professional status, and complex ethical challenges. Hence, although the social work profession is still under-recognized in the country, social work-trained workers can play a significant role in developing psychosocial interventions for wartime sexual violence survivors. Our findings also demonstrated that despite the growing interest and literature on Mental Health and Psychosocial Support in complex humanitarian settings, more efforts and research evidence are needed to inform policy, practice and multisectoral collaborations in the sexual violence field. However, our findings should be taken with caution as they clearly may not reflect the reality of psychosocial services outside the Panzi one-stop centre model of care. Future developments may also consider case-control studies involving participants from other non-governmental and governmental structures employing psychosocial assistants in different sectors like child protection, social development, or civil society-based agencies.
Footnotes
Research ethics
The Université Evangélique en Afrique and the International Centre for Advanced Research and Training (ICART) provided institutional approvals for this project. No further Ethical clearance was required because we did not intend to conduct interviews with survivors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Acknowledgements
The authors acknowledge the invaluable contribution of the 11 psychosocial assistants who consented to participate in the study. The authors also acknowledge the insightful feedback of the three anonymous reviewers.
Authors’ contributions
All authors contributed to developing and testing the interview instrument. ACK and MGM conducted the interviews and the desk search of the literature. ACK and ACF coded the interview transcripts and generated the initial themes from the data. BJB supervised the data collection and analysis process. All authors reviewed the coded transcripts. ACK conducted the in-depth analysis of coded materials and wrote the manuscript with inputs from AAB and BJB. All authors attended a meeting to reflect on the anonymous reviewers’ feedback. ACK led the overall study, finalised the manuscript review, and responded to the editors’ and reviewers’ comments.