
Abstract
Within their Grand Challenges for Social Work (2025), the American Association for Social Work and Social Welfare (Sherraden et al., 2014) identifies the need to close the health gap as a priority for improving individual and family well-being. To make progress toward closing the health gap, social workers need research findings that facilitate a better understanding of access to reproductive healthcare and substance use treatment in the context of drug use in regions of the United States (US) where health disparities exist. This research would be useful to inform social work practice and policy intervention strategies in medically underserved communities.
One region of the US where there is a dire need to close the health gap is Appalachia. Appalachia is a historically health-underserved geographic region of the US spanning the Appalachian mountain chain from southern New York to northern Mississippi, which is home to nearly 27 million residents (Appalachian Regional Commission [ARC], 2023). Appalachian communities often encompass rural areas that experience substantial barriers to healthcare access and elevated rates of health disparities. Social workers serving these communities are often responsible for providing a broad range of services. Appalachian social work practice may require competency in a broad range of skills that must be applied regularly across dynamic practice settings to meet client needs in the context of a dearth of regional physicians and other health providers (ARC, 2021; Ely et al., 2012).
Research indicates that approximately 10% of pregnant women across the US reported illicit substance use in the last month; rates of prenatal substance use in Appalachia exceed national averages (Substance Abuse and Mental Health Services Administration, 2023; Umer et al., 2023). This elevated rate of prenatal substance use in the region is an area of concern for social workers. Appalachian social workers need research to inform their practice and intervention strategies, yet research on reproductive health access in the context of pregnancy and regional substance use is limited.
To add to the knowledge base in this area, we conducted a secondary analysis of data from a larger study on unmet reproductive health needs in the context of the opioid epidemic in the greater Appalachian region to examine associations between past-year illicit drug use and reproductive healthcare access and utilization among sexually active, reproductive-aged women in Appalachia.
Literature Review
Substance Use During Pregnancy In Appalachia
The health risks of perinatal substance use are well documented. Specific to Appalachia, findings from one study of 34,000 Appalachians who had given birth in the prior 2 years indicate that 12.4% of the sample reported illicit substance use while pregnant (Umer et al., 2023). The consequences of substance use during pregnancy may include increased maternal mortality, low birth weight, risk of child welfare involvement, developmental delays, a twofold increase in the risk of stillbirth, a 60% increase in the risk of preterm delivery (before 37 weeks), and up to a fourfold increased risk of sudden infant death syndrome (Baer et al., 2019; Chen et al., 2024; Driscoll & Ely, 2019; Hansen & Moloney, 2020; Hauck & Blackstone, 2022; National Institute on Drug Abuse, 2020; Weber et al., 2021). In 2021, drug overdose-related mortality rates among Appalachian adults ages 25–54 were 72% higher than rates in the rest of the US (ARC, 2023). As substance use during pregnancy increased nationally, the problem has been compounded by barriers that impede access to reproductive healthcare and substance use disorder (SUD) treatment programs in the Appalachian region (Morrone et al., 2021; Pollard et al., 2024; Wilson & Brown, 2024). Pregnant women who fear stigma and criminalization may not be inclined to seek drug treatment or reproductive healthcare when pregnant (Ostrach & Leiner, 2019; Stone, 2015).
Access to Healthcare in Appalachia
In the US, healthcare is not a right, it is a privilege offered to those who hold health insurance, which covers some, but usually not all, health expenses (Stepanikova & Oates, 2017). Many residents of Appalachia with SUDs are underinsured or have no health insurance, and they may face health access barriers, including poverty, problems with transportation, unemployment and lack of steady employment, housing insecurity, and problems meeting basic needs (National Opinion Research Center & East Tennessee State University, 2025; Pollard et al., 2024).
The Affordable Care Act (ACA), a federal health insurance marketplace program put in place in the US in 2014, was designed, in lieu of a universal healthcare system, to expand access to health insurance for families who do not receive employer-sponsored health insurance (as is typical in the US; French et al., 2016). The ACA makes it possible for states to expand the ability to enroll in Medicaid, the public health insurance program for poor families, by raising income limits so more working poor people qualify for the program (Gaffney & McCormick, 2017). The ACA also provides access to health insurance through an expanded marketplace. It provides subsidies for purchasing health insurance, and it allows families to continue coverage for adult children up to age 26, among other benefits (French et al., 2016). Some Appalachian states have used the ACA to expand access to Medicaid in their states, which improved health insurance coverage for those Appalachian residents (Kaiser Family Foundation [KFF], 2024). However, five Appalachian states (Alabama, Georgia, Mississippi, South Carolina, and Tennessee) have yet to expand Medicaid and have high rates of uninsurance, particularly in Appalachian counties (KFF, 2024), creating additional barriers to healthcare for residents of these states.
Lack of access to health insurance in many Appalachian counties combines with other structural barriers like provider shortages and difficult travel across rural terrain to impede access to healthcare and SUD treatment in the region (ARC, 2024; Rural Health Information Hub, 2024). A recent review of barriers to utilizing SUD treatment in Appalachia found that stigma, limited resources (e.g., basic needs, childcare, transportation, lack of paid time off from work), and maladaptive social networks are prominent concerns that contribute to lack of healthcare utilization in the region (Wilson & Brown, 2024). Furthermore, SUD treatment providers are constrained by Medicaid rules that limit coverage of SUD treatment to 60 days postpartum (Meinhofer et al. 2020; Patrick et al. 2019; Ranji et al., 2021).
In addition to SUD treatment barriers, residents of Appalachia also face disparities in accessing family planning and reproductive healthcare services. Rates of unintended pregnancy in Appalachia are elevated, which studies have attributed to problems including high failure rates of user-dependent contraceptives, lack of contraceptive use, and difficulty with accessing contraceptive methods (Ely et al., 2020; O’Donnell et al., 2018). For example, study results indicate that Appalachian women often report not being able to use their preferred contraceptive method, and they report contraceptive coercion from partners and mistreatment from healthcare providers that was considered coercive and stigmatizing (Alspaugh et al., 2023; Huslage et al., 2022; Swan et al., 2023).
At the national level, Medicaid has established the Maternal and Infant Health Initiative to promote the use of effective contraceptive methods; yet refusals to fill contraceptive prescriptions have been documented in 26 states across the nation (Centers for Medicare & Medicaid Services, 2024; National Women's Law Center, 2024). Conflicts between federal and state mandates related to abortion and reproductive health also contribute to disparities in much of Appalachia (Serchen et al., 2023).
Pregnancy is typically a period of increased engagement with the healthcare system, which also represents a unique opportunity for engagement in health promotion, screening, and referral for SUD treatment (Turrentine et al., 2023). Women who use drugs may be more open to SUD treatment during pregnancy when health concerns may be prominent (Choi et al., 2022; Frazer et al., 2019). Conversely, research also suggests that pregnant women who use drugs may withhold substance use information, delay, or avoid seeking prenatal care due to fears of reprisal, stigmatization, and/or child welfare involvement (Ostrach & Leiner, 2019; Stone, 2015; Weber et al., 2021). Pregnant and parenting women who use drugs experience stigma from friends, family, and even practitioners themselves (Leiner et al., 2021; Nichols et al., 2021), which may further contribute to delayed healthcare seeking. These findings, taken together, suggest that more research in these areas is needed, and the implications of such research could be useful for improving social workers’ understanding of these problems and how to assist clients in this region.
Social Work in Appalachia
Social work practice in Appalachia is informed by community contexts, including a strong regional sense of place, a unique culture, and a strong regional identity (Denham, 2016; Weaver & Holtkamp, 2015). This unique context means that social workers in the region are serving populations whose needs may differ from similar populations in non-Appalachian areas of the US (Pope et al., 2014). As such, social workers in the Appalachian region often provide generalist social work services, like health education and advocacy, in the absence of an adequate number of regional physicians and other health providers (Ely et al., 2011). Research indicates that Appalachians report positive relationships with social workers in their communities, although there are not always enough social workers employed to fully serve clients in some settings (Ely et al., 2014).
The Present Study
The present study utilized secondary data from a larger study of unmet reproductive health needs in the Appalachian region to investigate differences in reproductive healthcare access and utilization between Appalachian women who report past-year illicit drug use and those who do not. We drew the data for the current study from an original, mixed-methods, anonymous, electronic study conducted in 2019 that utilized Facebook to recruit Appalachian women and pregnancy-capable people to complete a focus group-informed survey inquiring about the reproductive healthcare needs and barriers in their communities in the context of elevated rates of regional opioid use (see Alspaugh et al., 2023; Swan et al., 2023 for more detail). In this current study, we examined whether women who use drugs: (a) experience more barriers to accessing contraceptives, (b) are less likely to have a trusted healthcare provider, (c) are less likely to receive regular health checkups, and (d) are more likely to report unintended pregnancies.
Method
We conducted a secondary analysis of data collected in a broader survey of unmet family planning needs in the context of the Appalachian opioid crisis among reproductive-age women (18–49 years) living in the Appalachian region (N = 628; see Swan et al., 2021). The original study protocol was approved by the Institutional Review Board at the university where the study was conducted. Additional inclusion criteria were applied for the present study based on self-report items from the original survey. Those who reported sexual activity in the past year and engaging in sexual activity that can result in a pregnancy were included in this study. Participants who responded “I don’t know” or did not respond to a question probing past-year illicit substance use were excluded from the sample for this study. The analytic sample for the current study was n = 357.
Measures
A subset of the items from the full survey was used for the present study. The following constructs were measured using self-report multiple-choice or multiple-selection items.
Demographic and Geographic Characteristics
Participants reported their age, race, ethnicity, and marital status, highest level of educational attainment, employment status, income, and whether they received state or federal social welfare benefits, such as disability payments. Participants reported their residential zip code, which was matched to 2013 Rural–Urban Continuum Codes 1 (Economic Research Service [ERS], 2024) and classified as metropolitan or nonmetropolitan.
Illicit Substance Use and Perinatal SUD Treatment
A series of survey items probed for illicit substance use and perinatal SUD treatment engagement. Participants reported illicit substance use by indicating whether they had used any of the following in the past year without a prescription: cannabis, cocaine, opioids, benzodiazepines, methamphetamines, heroin, crack, or other substance not listed. Participants answered whether they had ever used drugs while pregnant, and if so, whether they felt they had adequate support for making decisions about their pregnancy and whether they ever avoided going to the doctor for a pregnancy due to concerns about being judged about their drug use, fears of law enforcement, or concerns about child welfare involvement. Those who reported past-year illicit substance use were asked whether they had a plan for addiction treatment if they became pregnant. All participants were asked whether they were aware of medications to treat opioid addiction during pregnancy.
Reproductive History
Participants reported the total number of pregnancies and whether they were currently pregnant. Those who reported a history of pregnancy were asked whether any of the pregnancies were unintended.
Access to Healthcare and Contraceptives
Participants were asked whether they had health insurance and if it was public or private. Questions probed access to healthcare including: whether they had a regular primary healthcare provider, knowledge of where to get a physical exam, trust in healthcare providers, driving distance to primary care, driving distance to a women's health office, and whether they felt it was hard to get a healthcare appointment. Other questions probed access to contraceptives (referred to within the original survey using the term “birth control”), level of comfort calling to make an appointment for contraceptives, access to contraceptives in their area, affordability of contraceptives, worries about getting contraceptives, and difficulties obtaining contraceptives.
Utilization of Healthcare and Contraceptives
Participants were asked about their utilization of healthcare, including the date of their last health exam. Participants were also asked whether they had ever had a bad experience with a healthcare provider that made them not want to return, and if so, how they would characterize that experience. Several questions assessed participants’ contraceptive use and the types of contraceptives they used.
Analysis
Descriptive statistics were calculated for all measures, and bivariate tests were conducted comparing those who reported past-year illicit substance use and those who did not. Binary logistic regression models were conducted to examine which factors, including past-year illicit substance use, were most associated with several key indicators of perinatal healthcare access and utilization: trust in healthcare providers, difficulties obtaining contraceptives, engagement in primary or women's healthcare, and history of unintended pregnancies.
Results
Demographic Characteristics
See Table 1 for demographic characteristics of the full sample as well as for those who reported past-year illicit substance use (n = 97) and those who did not (n = 260). The average age of participants was 32.6 years old (SD = 5.9). Those who reported past-year drug use were 1.8 years younger on average, (t [346] = 2.55, p = .011, Cohen's d = 0.31). Most participants reported being partnered or married (88.5%) and White (90.2%). More than half reported having at least an associate's degree 2 (57.7%) and 2.8% reported having not graduated from high school or equivalent. Most participants reported full-time employment (57.1%). Most (52.7%) lived in counties classified as nonmetropolitan (ERS, 2024). Those who reported past-year drug use were more likely to receive public assistance (i.e., state or federal benefit programs, such as disability payments or food assistance; 20.6% vs. 11.9%; χ2 [1] = 4.36, p = .037).
Demographic Characteristics and Reproductive History.
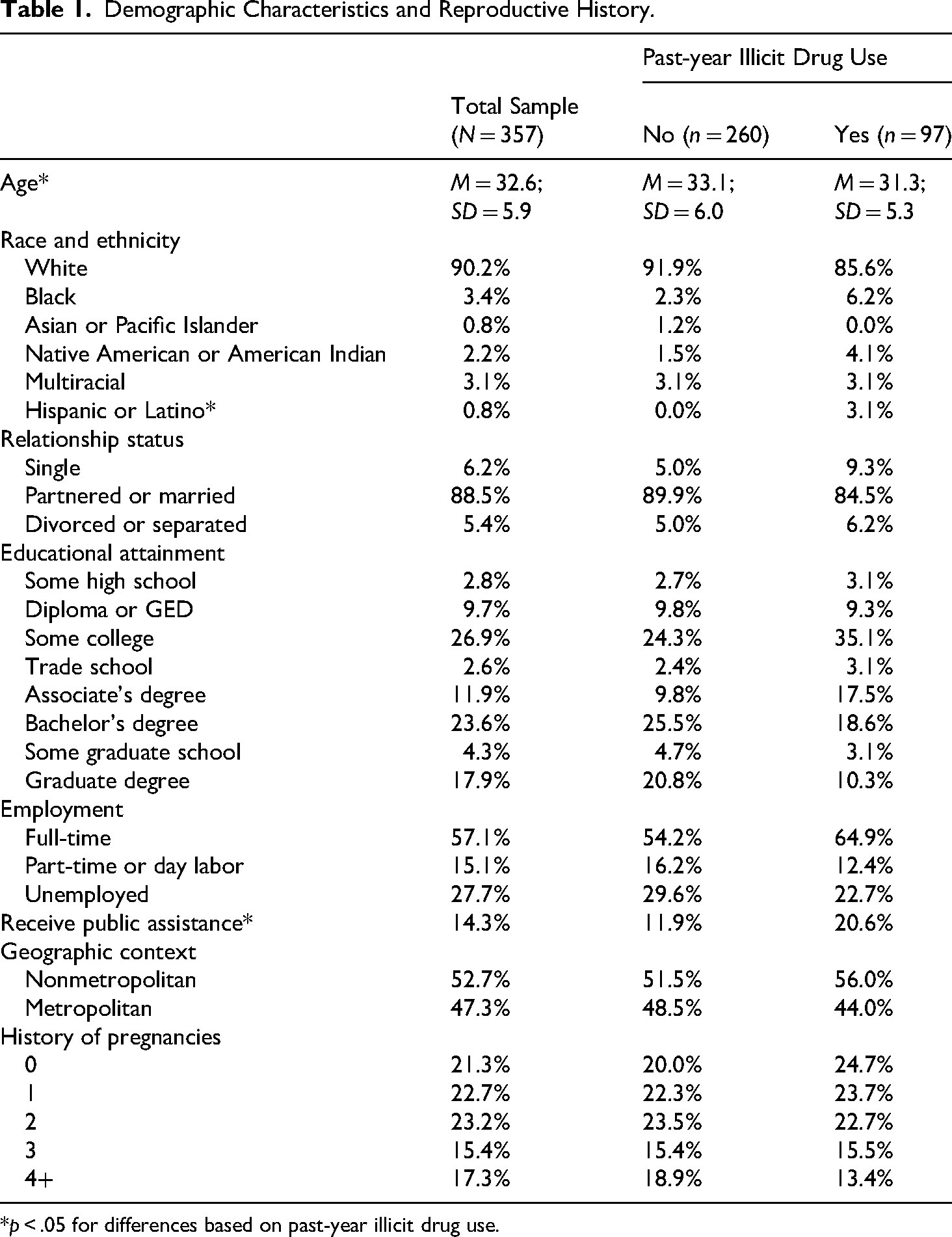
*p < .05 for differences based on past-year illicit drug use.
Illicit Substance Use
Just over a quarter of participants (27.2%) reported past-year use of at least one illicit substance. Cannabis was the most used illicit substance (20.2%) followed by cocaine (3.6%), benzodiazepines (2.5%), opioids (2.2%), and methamphetamines (1.1%). Among those who reported past-year illicit substance use, 13.5% reported ceasing use of contraceptives in the past year because of their drug use. About a quarter of those with past-year illicit substance use reported they had avoided going to the doctor for pregnancy care or contraceptives because they were worried about being judged for their drug use (26.0%), because of fears of legal issues related to drug use (24.0%), or because of fears of having children taken away due to drug use (28.1%). Among those who reported past-year illicit substance use, 14.6% reported a pregnancy that occurred while using drugs. Among those who reported drug use during pregnancy, more than a third (35.7%) reported not having adequate support for making decisions about their pregnancy that occurred while using drugs and 61.7% did not have a plan for addiction treatment if they became pregnant now. Among the total sample, 42.8% were not aware that there are medications available to treat opioid addiction during pregnancy.
Reproductive History
Most participants reported a history of pregnancy (78.7%) with an average of 2.1 (SD = 1.9) prior pregnancies. Some of the participants reported being currently pregnant (9.0%), including 12.7% of those who reported past-year drug use. Past-year drug use was not associated with current pregnancy (p = .176) or history of pregnancy overall (p = .330). However, those who reported past-year drug use were more likely to report a history of unintended pregnancy (68.6% vs. 50.7%; χ2 [1] = 6.70, p = .010).
Access to Healthcare and Contraceptives
Most participants (89.6%) reported having health insurance of some kind. Among those with insurance, the most common sources of coverage were employer-provided plans (35.6%), from their partner's job (21.9%), Medicaid (19.7%), and Medicare 3 (11.3%). While past-year drug use was not associated with having health insurance overall, those who reported past-year drug use were more likely to have Medicaid (30.1% vs. 16.0%) or Medicare (21.7% vs. 7.6%) and less likely to have insurance provided by their employer (33.7% vs. 36.3%) or their partner's employer (4.8% vs. 27.8%; χ2 [7] = 33.55, p < .001).
Most participants (73.0%) reported having a regular healthcare provider and knew where to go to get a general physical exam (84.6%). Time spent traveling to primary care averaged 27.0 min (SD = 25.1). Some (20.5%) felt it was hard to get an appointment with a healthcare provider; however most had a trusted healthcare provider in their community (78.0%), trusted that the healthcare services they received were confidential (75.0%), and thought their healthcare provider valued their thoughts and decisions (71.8%). Those who reported past-year drug use were more likely to indicate that it was hard to get an appointment (55.7% vs. 34.1%; χ2 [2] = 13.68, p = .001) and less likely to perceive that their healthcare provider valued their thoughts and decisions (64.6% vs. 74.4%; χ2 [2] = 10.72, p = .005).
Most reported that they could get contraceptives near where they live (84.6%) and would feel comfortable calling to get an appointment to do so (81.4%). The average travel time required to visit a gynecologist was 33.4 min (SD = 28.0) and 27.5 min (SD = 21.2) to visit a healthcare office to obtain contraceptives. Most participants (78.1%) either agreed or strongly agreed that they could afford contraceptives. However, 15.1% agreed or strongly agreed that they worried about where to get contraceptives and slightly more (18.6%) reported ever having difficulty getting contraceptives. Those who reported past-year drug use were less likely to report access to contraceptives in their area (78.1% vs. 86.9%; χ2 [2] = 6.23, p = .044) and less likely to report being comfortable calling to get an appointment for contraceptives (69.8% vs. 85.7%; χ2 [2] = 12.89, p = .002). Those who reported past-year drug use were less likely to agree that they could afford to get contraceptives (z = –2.51, p = .012), more likely to agree that they feel worried about where to get contraceptives (z = –4.39, p < .001), and more likely to report having had a hard time getting contraceptives (31.5% vs. 14.4%; χ2 [1] = 12.96, p < .001).
Utilization of Healthcare and Contraceptives
Nearly all participants reported their most recent general health exam was either in the past year (66.4%) or the past 5 years (21.5%). Similarly, 62.6% reported having had their most recent women's health exam in the past year and 27.2% reported it was in the past 5 years. Most (81.5%) reported either attending a general health or women's health checkup in the past year. Those who reported past-year drug use were less likely to report having had either a general health or women's health exam recently (z = –3.23, p = .001), with 71.1% reporting past-year checkups of some kind compared to 85.3% among those who did not report past-year drug use. Nearly two-thirds (64.3%) reported having had at least one bad experience with a healthcare provider that made them not want to go back. The most reported characterization was “the provider was rude/condescending to me” (75.1%) followed by “I did not feel listened to” (62.0%) and “I was not comfortable with the provider” (43.7%).
More than half of participants (55.6%) reported current use of contraceptives or engaging in behaviors intended for pregnancy prevention, including condoms (35.0%), withdrawal (25.2%), oral contraceptive medication (19.3%), abstinence (13.7%), intrauterine device (11.2%), and partner's vasectomy (5.6%). Past-year drug use was not significantly associated with current use of contraceptives (p = .054).
Logistic Regressions
A binary logistic regression model examined which factors were most associated with participants reporting whether they have healthcare providers in their communities that they can trust or not (χ2 [11] = 35.18, p < .001). Past-year drug use was not associated with having a trusted healthcare provider in the model (p = .125). However, compared to White participants, those who identified as Black (OR = 0.24, 95% CI [0.06, 0.92], p = .038) or Native American (OR = 0.18, 95% CI [0.04, 0.83], p = .028) had lower odds of reporting a trusted healthcare provider in their communities. Those living in metropolitan areas had lower odds of reporting a trusted healthcare provider in their community than those living in nonmetropolitan areas (OR = 0.50, 95% CI [0.26, 0.96], p = .037). Those with an associate's degree or higher were 2.26 times more likely to have a trusted healthcare provider compared to those with less education (OR = 2.26, 95% CI [1.18, 4.32], p = .014). Having health insurance increased likelihood of having a trusted healthcare provider (OR = 3.83, 95% CI [1.60, 9.17], p = .003) (Table 2).
Logistic Regression Results.
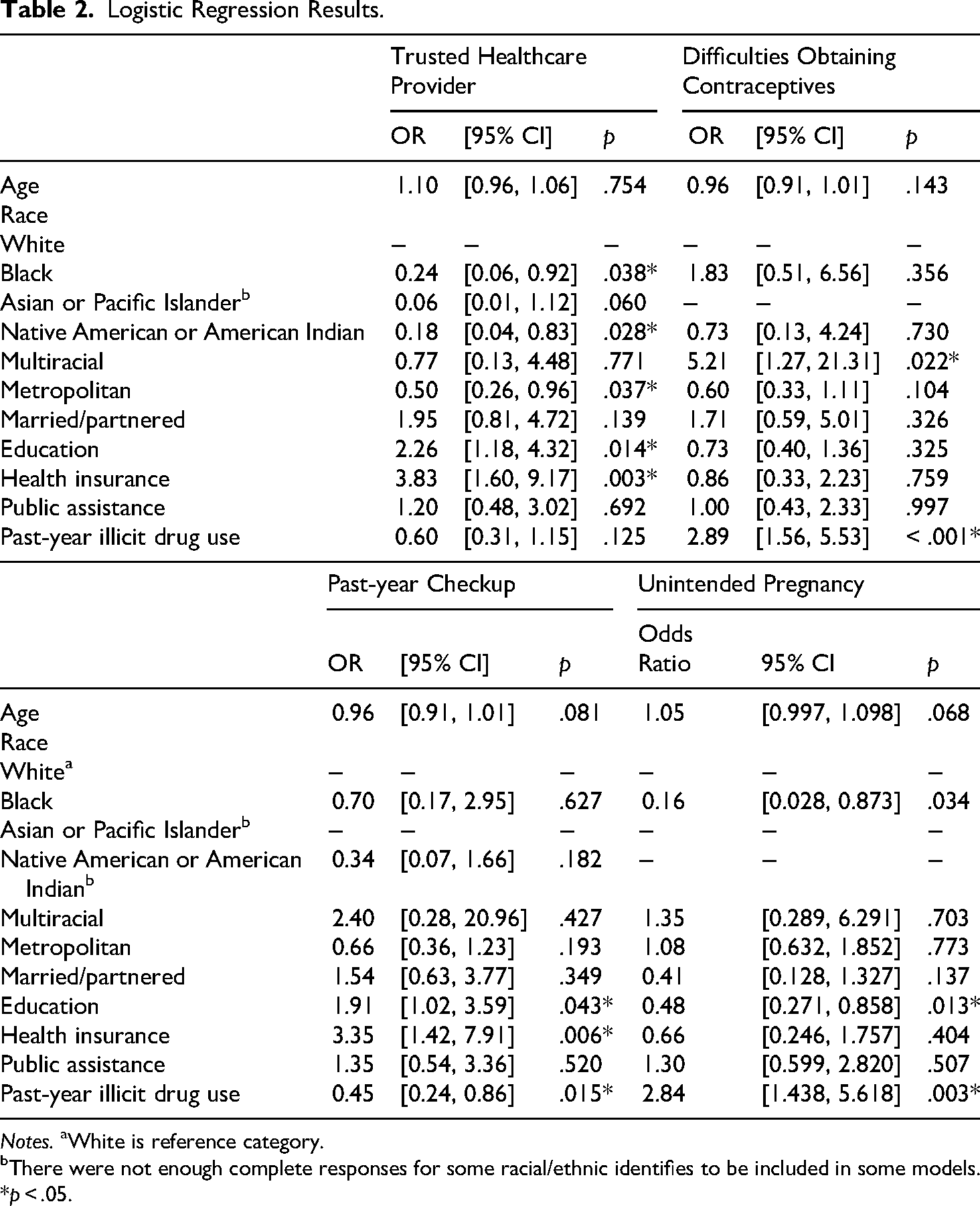
Notes. aWhite is reference category.
There were not enough complete responses for some racial/ethnic identifies to be included in some models.
*p < .05.
A binary logistic regression model examined which factors were most associated with having a hard time obtaining contraceptives (χ2 [11] = 28.69, p = .003). Those who reported past-year drug use were 2.89 times more likely to report having had a hard time obtaining contraceptives (95% CI [1.45, 5.35], p < .001). Compared to White respondents, multiracial respondents (i.e., more than one race) were more likely to report problems obtaining contraceptives (OR = 5.21, 95% CI [1.27, 21.31], p = .022).
A binary logistic regression model examined which factors were most associated with having had a general health or women's health checkup in the past year (χ2 [11] = 25.22, p = .008). Those who reported past-year drug use had lower odds of having had a checkup in the past year (OR = 0.45, 95% CI [0.24, 0.89], p = .015). Those with a college degree were more likely to have had a checkup (OR = 1.91, 95% CI [1.02, 3.59], p = .043) as were those with health insurance (OR = 3.35, 95% CI [1.42, 7.91], p = .006).
Among those with a history of pregnancy, a binary logistic regression examined which factors were associated with a history of unintended pregnancy (χ2 [11] = 39.11, p < .001). Those who reported past-year drug use were 2.84 times more likely to have had an unintended pregnancy (95% CI [1.44, 5.62], p = .003). Compared to White respondents, those who identified as Black were less likely to have had an unintended pregnancy (OR = 0.16, 95% CI [0.03, 0.87], p = .034) as were those with a college degree (OR = 0.48, 95% CI [0.27, 0.86], p = .013).
Discussion
Results indicate Appalachian women in this sample who use drugs reported barriers to accessing reproductive healthcare, which represent a source of concern to social workers seeking to improve health equity in this medically underserved geographic region of the US. Participants who reported past-year drug use experienced more difficulties obtaining contraceptives, perceived contraceptives as less accessible, were more likely to have a history of unintended pregnancies, were more likely to feel uncomfortable getting an appointment for contraceptive care, were more likely to report affordability concerns, and more likely to report general worries about obtaining contraceptives.
Implications for Social Work Practice and Policy
These findings suggest the existence of a health gap in Appalachia that needs attention from social workers if we are to advance toward closing that gap in this region, as is called for in the Grand Challenges for Social Work (Sherraden et al., 2014). Some of the participants who reported drug use also reported stopping contraceptives because of their drug use. Those who reported past-year drug use were also more likely to report a history of unintended pregnancies, even after controlling for other factors. A quarter of participants who reported past-year drug use avoided going to a doctor for pregnancy or contraceptive care because of concerns about stigma or being judged, concerns about legal consequences of their drug use, and/or fears of having children taken away. These findings highlight areas in which social workers may play a supportive role through resource navigation, referrals, education, and advocacy. At the same time, because social workers may be associated with child welfare, such efforts should be approached carefully and grounded in trust, transparency, and nonpunitive support. Responding effectively to these concerns requires generalist skillsets that social workers in the region should be trained in and familiar with (Ely et al., 2012).
However, these findings should not be interpreted to suggest that social workers can or should compensate for broader deficits in healthcare infrastructure. The challenges described in this study are also shaped by policy and structural conditions, including provider shortages, transportation barriers in rural communities, uneven Medicaid expansion across Appalachian states, postpartum Medicaid coverage limitations, and reduced family planning infrastructure. Social work intervention is therefore best understood as one component of a broader response that must also include healthcare system investment and policy reform.
Our findings also revealed that nearly two-thirds of respondents reported at least one prior negative interaction with a healthcare provider that made them not want to return. This should be considered alongside the finding that many participants reported having a regular or trusted provider, suggesting that women may have confidence in at least one provider while also carrying the effects of prior stigmatizing or discouraging healthcare experiences. Research suggests that when women feel their voices are not valued, they may delay or avoid essential care (Falk et al., 2023; Morrone et al., 2021). Together, these findings underscore the need to strengthen trust between healthcare systems and the communities they serve in Appalachia. This is an area in which macro-level social work intervention may be especially valuable.
These results highlight the opportunity for social workers to intervene to improve resource links between patients, SUD treatment, and contraceptive care in the region, which would potentially enhance reproductive well-being and reduce drug-exposed births in Appalachian communities (Axelson et al., 2022). Because social workers in the Appalachian region are often trained to connect clients to resources and engage in education and advocacy (Ely et al., 2011), they are positioned to educate patients in general health settings about the health and SUD resources available in the region, connect patients to reproductive health and SUD treatment, and advocate for the improvement of regional treatment services that are pregnancy-friendly, child-friendly, and promote self-determination in a manner aligned with the NASW code of ethics.
Social workers must also advocate for improved health policy, while recognizing that policy reform and healthcare system expansion, rather than social work labor alone, are necessary to address these gaps in care. One example is expanding Medicaid in states that did not adopt Medicaid expansion under the ACA (ARC, 2021), which would enhance opportunities for lower-income Appalachian families to access public health insurance. This is especially important in light of our current findings indicating that participants with a history of drug use were more likely to be on public insurance programs. Social workers can also advocate for restoration and expansion of the Title X program (the federal program that provides funding for low-cost and free family planning services), which has historically been one of the most successful public health programs in U.S. history (Marcella, 2022). Improvements in the Title X program, 4 which has been dismantled by the current federal administration (National Family Planning & Reproductive Health Association, 2025), would improve contraceptive care in regions like Appalachia where health disparities are notable and full access to contraceptive care is critical for addressing opioid exposure during pregnancy and other concerns reported in our current study.
Our findings also showed relatively low awareness of addiction treatment options during pregnancy among participants who use drugs, representing another concern and area of potential intervention for regional social workers. Social workers are well trained to design and implement novel treatment programs, which could include designing and operating SUD treatment programs that incorporate trauma-informed care techniques and are accessible to women and parenting people, and which integrate reproductive health services with drug treatment and other mental health supports. This type of social work-led, integrated program design could help mitigate the risk of unintended pregnancies and increase utilization of SUD treatment during the perinatal period. Social workers can also advocate for policy change to eliminate the rule that Medicaid will not cover healthcare past 60-days postpartum. The elimination of this rule would open up care options for Appalachians with substance use histories. Social workers, who are already trained to implement evidence-based, trauma-informed care (Mersky et al., 2019) can collaborate with health professionals to improve trust between the medical community and Appalachian residents, thereby helping to reduce the stigma that may undergird the lack of health engagement represented in our study findings.
Research suggests that stigma may be a driver of health inequity in the Appalachian region (Alspaugh et al., 2023). Taken together, our findings on the reported lack of engagement in necessary health behaviors suggest that stigma surrounding both drug treatment and reproductive healthcare are likely influencing health behaviors in these communities. These findings align with previous studies suggesting that stigma damages relationships with health providers in the Appalachian region, which potentially perpetuates the opioid epidemic (Skaggs et al., 2023), and results in a lack of healthcare seeking in Appalachians who experience problems like homelessness (Powney et al., 2025). Because social workers can be trained in both health advocacy and mental healthcare, they are uniquely positioned to decrease stigma around substance use and pregnancy, and improve the relationships between health providers and their patients.
Directions for Future Research
Recommendations for future research include conducting a study that maps SUD treatment and contraceptive care in Appalachian counties to create a comprehensive resource list. Results from such a study would be useful to social workers and agencies that connect clients to comprehensive SUD treatment and reproductive healthcare. Other recommendations include research that assesses and compares reproductive health and SUD treatment needs between Appalachian and non-Appalachian counties, and between counties in states where Medicaid has and has not been expanded. This would provide social workers with more information to tailor interventions as we advocate for Medicaid expansion to come to all Appalachian states. Future research should include testing community-informed educational interventions to determine what best serves Appalachian communities. Research on the best ways to integrate SUD treatment and reproductive healthcare in a manner that is culturally sensitive and responsive to regional stigma is also suggested.
Limitations
This is a cross-sectional study, which has noted advantages, including being simple to administer, cost-effective, and having a low burden on participants (Taris et al., 2021). However, the limitations are also well known and include the inability to separate out cause from effect, and sampling bias (Taris et al., 2021; Wang & Cheng, 2020). The results of this study are exploratory and not generalizable outside the study population.
Conclusions
Appalachia is an expansive, often rural, culturally unique geographic area of the US with many strengths and notable health challenges. It has been characterized as a region where “place matters” in relation to health (Behringer & Friedell, 2006). It is also a region where many communities do not have adequate access to physicians and other health professionals. In this context, social workers may step in to fill gaps in care by connecting clients to resources and providing health education and other interventions. As such, social workers employed in this region need a breadth of skills that allow them to navigate micro- to macro-level regional concerns (Ely et al., 2011), so they can intervene and advocate for changes intended to improve health in Appalachian communities (Pope et al., 2014) in relation to improving reproductive healthcare and use of SUD treatment programs in the context of regional drug use. If the social work profession is going to achieve its goal of closing the health gap (Sherraden et al., 2014), more needs to be done in remote geographic areas like Appalachia to address the reproductive health concerns and SUD treatment needs that are highlighted in the results of this study.
Footnotes
Ethics
Ethical approval for the study was given by the University at Buffalo Institutional Review Board.
Consent to participate
Participants were anonymous and gave consent to participate by reading a consent document and clicking to proceed at the beginning of the study survey.
Author contributions
Aaron Brown developed the research questions and analytic methods, conducted the analyses, wrote the results, and collaborated on the literature review and discussion. Zak Amen drafted literature review and collaborated on the data analysis and discussion. Gretchen Ely designed the original study, collected original study data, and assisted with drafting all parts of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the original project was provided through a Society of Family Planning Innovations Research Grant (Grant No. SFPRF12-II2).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.