
Abstract
Informed consent is critical in research with children. Although much has been written about the need to see consent as an ongoing process, less has considered how to do it in practice. This article reflects on the authors’ experiences of conducting a piece of research focusing on children’s experiences of safety from abuse within institutional contexts. It draws on feedback provided by participants and the guidance of three Children’s Reference Groups. The importance of presenting information in accessible and appropriate ways, of providing opportunities for participants to negotiate their participation and for in-the-moment challenges be dealt with collaboratively and reflexively are stressed. To illustrate our approach, we provide a number of consent tools and describe how they were utilised.
Introduction
Informed consent has been described as the ‘basis of morally valid decision-making’ (Mayne et al., 2016). Within the research domain, informed consent attempts to ensure participants are not subjected to coercion, deception or other forms of manipulation (Árnason et al., in Mayne et al., 2016). Children’s informed consent in participatory research has received significant attention from researchers emphasizing the importance of seeking children’s informed consent prior to their participation. Some have gone as far as to say that it ‘is the cornerstone of the research relationship’ (Graham et al., 2015: 338) as it demonstrates the researcher’s respect for the child’s dignity, their capacity and right to make decisions, their ability to understand, foresee and manage risks and benefits and to engage meaningfully in the research process.
Although processes to enable children to provide their informed consent prior to their participation in research are vital, children’s researchers have argued that consent needs to be seen as an ongoing process (Barker, and Weller, 2003) in which children’s participation is negotiated and renegotiated as in-the-moment ethical challenges emerge. Despite general agreement on the importance of this issue, Parsons et al. (2015) observed there is currently limited guidance, and even less specific examples, available to children’s researchers to inform the best ways to ensure informed consent from children.
This article addresses this gap, by outlining six elements we consider essential to the collection of informed consent within children’s research. We detail how each of these elements was managed within an Australian study on children’s perceptions and experiences of safety. The practical tools utilised are provided, along with our reflections and the advice and feedback provided by 3 children’s reference groups established to guide and inform the project. We do so because we agree that ‘it is not common for researchers to ask people what they think about research methods and even rarer for this to be reported in publications’ (Hill, 2006: 70) and without such description there remains little practical guidance on how to ensure quality in research conducted with children (Irwin and Johnson, 2005). Although new processes, including the use of digital technologies have been applied to improving the process of informed consent for young people (Hammond and Cooper, 2011), challenges remain to the development of other child-friendly ways to meet ethical requirements.
Background
For centuries children have been the focus of research, often without their knowledge or consent (Alderson, 2007). Prior to World War II, researchers accessed children to trial medical procedures and vaccines and explore the impacts of their exposure to things such as pain, distressing stimuli and emotional neglect (Burns, 2003). Such was the nature of childhood research that John Sants (1980: 21) wrote, ‘Many experimental child psychologists appear to have come close to child abuse in the interests of science’. At that time, researchers routinely made decisions based on what they believed were in the best interests of children (namely that children as a group would benefit from the outcomes of their studies). According to Prochner and Doyon (1997), researchers felt no need to consider the long-term impacts resulting from children’s involvement in research let alone whether children might consent.
After World War Two, the Nuremberg Code was enacted and the way that children were involved in research changed fundamentally. The Nuremberg Code required that research subjects had to freely give their consent, which required their comprehension of the risks and benefits of their participation and the capacity to withdraw their consent at any time (Farrell, 2005). The code is based on the presumption that when individuals are adequately informed of the nature, scope and potential harms of participating in a research project they are able to make an informed decision in their own best interests (Navratil, 2015).
This requirement led unintentionally to children being excluded as research participants because they were deemed to be unable to provide such consent (Grodin and Annas, cited in Burns, 2003). To remedy this situation, the Helsinki Declaration authorised parents (or other legally authorised representatives) to consent on the child’s behalf and required children, when they were legally competent to make decisions on their own behalf, to give their assent (Helseth and Slettebø, 2004).
These provisions have subsequently been codified in jurisdictions across the globe. In Australia, for example, the National Health and Medical Research Council (NHMRC) requires parental consent to a child’s participation but also urges researchers to ‘respect the developing capacity of children to be involved in decisions about participation in research’ and to seek their consent ‘whenever he or she has the capacity to make this decision’ (NHRMC, 2007). The NHMRC dictates that participation should be voluntary and ‘based on sufficient information and adequate understanding of both the proposed research and the implications of participation in it.’ This requires ‘an adequate understanding of the purpose, methods, demands, risks and potential benefits of the research.’ (NHMRC, 2007).
Within the research literature there is general agreement that to ensure that consent processes meet these requirements, informed consent should include (1) information presented to participants that is understandable and appropriate; (2) participant understanding of the information presented; and (3) the participant indicating formally that they understand they are consenting to participate (Cocks, 2006).
Although these requirements attempt to protect the child participant, there has been a growing view that consent processes increasingly aim to protect researchers and research institutions rather than participants themselves and that consent strategies have done little to progress ethical outcomes (Gallagher et al., 2010). Commentators (including, for example, Barker and Weller, 2003; Helseth and Slettebø, 2004; Renold et al., 2008; Rooney, 2015; Warin, 2011) have argued that for consent to be meaningful it needs to be considered as an ongoing process rather than a hurdle to be overcome prior to data collection. Meeting these requirements (i.e. procedural ethics) are important but consideration of, and response to, the in-the-moment ethical issues that emerge during ‘ethically important moments’ (Guillemin and Gillam, 2004) is also necessary (Holland et al., 2014). We argue that researchers can improve their research practice by negotiating and renegotiating consent with participants, including children before and during data collection.
As such, in this paper we argue, in addition to the accepted requirements outlined above, consent also requires (4) openings for choice and disagreement, (5) negotiation and renegotiation of the scope of children’s consent and (6) an agreement at the end of the research activity, that reaffirms children’s consent and negotiates any limits to sharing information that might have arisen.
The study
Before describing the approach taken to support children to engage in active and informed consent decision making a brief overview of the study is provided for context.
Context and aim of the study
In 2013, a Royal Commission was established in Australia to inquire into how institutions with a responsibility for children have managed and responded to allegations and instances of child sexual abuse. The Royal Commission will make recommendations on how to improve laws, policies and practices to prevent and better respond to child sexual abuse in institutions (Budiselik et al., 2014). To inform its findings, the Royal Commission contracted the authors to carry out a project that aimed to understand:
a) how children conceptualise and perceive safety;
b) children’s views on what gives rise to these perceptions;
c) children’s perceptions of safety within institutions;
d) what children consider is already being done to respond to safety issues and risks in institutions;
e) what children consider should be done to respond to safety issues in institutions (Moore et al., 2016).
Methodology
As noted, in designing the study we were conscious of our ethical responsibility to ensure that children were protected from harm. The study was reviewed by the Human Research Ethics Committee at the Australian Catholic University (review number 2014-57N).
To enable the study to be carried out in an ethical and appropriate way, time was spent considering the sensitivities related to researching an issue like safety from abuse and how best to develop a robust consent process. In partnership with the Royal Commission and an Adults’ Advisory Group, a methodology was developed that afforded participants a high degree of choice and control, physical and emotional safety, and checks to ensure they did not experience any distress through their participation (Moore et al., 2016). In addition to seeking adult’s perspectives on the nature of the study we established three children’s reference groups. These groups were made up of primary school children aged 9 to 11 years old, high school students aged 14 and 15 years old and a third with children aged 15 to 17 years old from a supported education program. These groups each met on three occasions and provided us with advice on the methodology and methods, and trialed a number of proposed tools.
Our methodology had a number of characteristics that are worth noting so as to place our observations about consent into context. These included that the study was:
1) Child-led: the methodology aimed to be driven by children’s conceptualisations of safety rather than relying on pre-determined assumptions about what safety concerns children hold and what issues would therefore be explored. Children decided not only what topics would be discussed but also how these issues might be explored.
2) Collaborative: although we were committed to being child-led we had also made commitments to fulfil the requirements of the funder. As such, we worked in collaboration with children: providing them information about what was required of us and negotiating, with children, how we would meet both their needs and wishes and those of the Royal Commission.
3) Scaffolded and iterative: each activity built on previous discussions. In early conversations, children decided what topics were most pertinent to them and then decided what they believed adults and institutions needed to understand and how they believed adults should respond. Participants also chose which of the research tools would be used to consider emerging issues and to answer our research questions.
Participants
A diverse group of participants from metropolitan and regional areas across Australia participated in a total of nine focus groups (N=121). Participants were recruited through organisations that reflected the institutions with which children interact: early learning centres; primary, secondary and boarding schools; disability support services; Aboriginal organisations; out-of-home care agencies; and camping and youth development programs. The ages of participants ranged from 4 to 17 years old.
Participants participated in two activity-based focus groups. Each focus group was facilitated by two researchers and went for 90 to 120 minutes. The focus groups were interactive and a variety of tools (games, discussion groups, individual and group-based activities) were used. The first focus group was concerned with building rapport and engagement with participants and primarily explored how children conceptualise and experience safety more generally (reported elsewhere). In the second session participants were encouraged to consider their experiences of safety within institutions and what constitutes a safe institution.
Why consent was particularly important in this study
A number of particular challenges or issues impacting on the study’s consent processes were identified prior to the study. These included: the sensitive nature of the topic under discussion; the exploratory and iterative nature of the project; and, the implications of using focus groups within institutional settings where children were already known to each other.
Our approach to consent was also developed within a study context which was highly scrutinised by a series of gatekeepers needing assurances that we were working ethically and appropriately. By developing and promoting our approach to consent to these gatekeepers we were able to demonstrate our appreciation of the risks that might emerge and propose strategies to deal with them if they arose. This assurance has been shown to be vital in research conducted on ‘sensitive topics’ (Heath et al., 2007).
Firstly, as we were discussing a ‘sensitive’ topic we wanted to ensure children were aware that it was their decision to participate (rather than for example their parent’s decision) and empowered enough to make choices about whether and how they might participate, and to withdraw their consent at any time. Children in our reference group stressed this point:
I think because you’re talking about safety you need to give people lots of choices. They shouldn’t feel pressured into talking about things. They should definitely be given a chance to have a say but it has to be their choice. (Young Person, Reference Group)
Our experience (shared by others, including: Mishna et al., 2004) is that children often do not appreciate what is involved in research until they begin to experience it. We believed, then, that we needed to consider consent as an ongoing process and as one that is likely to take a prolonged period of time. We based our thinking on our observation that participants need to get a ‘feel’ for us as researchers and for what they are going to be asked to do before they can make informed decisions about their participation:
I think choice is important because most kids wouldn’t have done this stuff [participated in research] before so they won’t know what they’re saying yes to. (Child, Reference Group)
Our iterative approach encouraged participants to identify the safety concerns most relevant to them and which topics they would consider discussing. As a result, we needed to engage in ongoing negotiation and to ‘check in’ with participants to make sure that they understood the implications of choosing particular topics. For example, one group identified bullying, child abduction and adult’s playing favourites as three issues of concern. Participants were asked which of their ‘safety issues’ they would like to discuss and make recommendations about. As a group, participants decided to consider ‘bullying’: one participant proposed the topic, another asked others whether they agreed, and participants agreed either verbally or nodding.
It was good that we had choices – like it was up to us what we wanted to discuss. I mean you told us what the Royal Commission wanted us to talk about but then we got to decide which bits we’d talk about and what we wouldn’t. (Young person, Reference Group)
In choosing to use focus groups we were aware that there are a number of risks inherent, particularly when participants know each other and already have established power relationships (Gallagher, 2008). Hennessy and Heary (2005) note two further key ethical issues arise in focus groups due to (a) the fact that disclosures by participants are shared with all group members and not just the researcher; and (b) intense group discussion may give rise to stress or distress in individual participants. This reinforced the need for participants to understand what we were asking of them and the potential risks both in-the-moment but also after the focus group concluded. We also needed to be aware of the way that power played out: between us as adult researchers and the young participants and amongst each other (Gallagher, 2008).
Many focus groups were conducted in school settings. Previous studies have suggested that school participants find it difficult to slip out of their usual student role where they are required to do everything that adults (i.e. teachers) ask of them (David et al., 2001; Gallagher et al., 2010; Woodhead and Faulkner, 2000) and that students need to feel able to engage in a different type of relationship with the adult researcher: a relationship bounded by different expectations and responsibilities (Davies, 2008). Our reference group participants confirmed this view:
At school you’re not used to having choices. You pretty much do what’s expected of you, what teachers want. I mean you can go against them but if you do there’ll be consequences. (Young Person, Reference Group)
In an attempt to differentiate ourselves from school staff and the project from usual school activity, we often conducted groups in spaces not usually used for teaching. For example, at one school we used the school’s boardroom and explained the usual purpose of the room was for leaders to make important decisions about the school. In another school we used the After School Care room where children were used to less formal and more activity-based sessions. Children seemed to appreciate working in these spaces and school staff who could see the group’s interaction from outside the room reported they seemed more engaged than expected.
Elements of consent
As discussed above, we argue for an approach to informed consent which includes six key elements. This next section provides a rationale for each of these elements and a description on how we put them into practice.
Element 1: presenting information
To enable informed consent participants can expect to be provided with information that is accessible, appropriate and answers any questions that they might have (Tait et al., 2007). Previous studies on consent (mostly with adults), however, have generally shown participants often do not understand the purpose of research, the potential risks and harms of participating or their ability to withdraw (Nishimura et al., 2013). To address these concerns, researchers have been encouraged to develop information letters for participants that clearly articulate the nature and scope of the study and outline the ways they might be involved and the ethical responsibilities that researchers have to them.
In an attempt to provide thorough information, researchers have tended to write long and detailed letters which present complex concepts in often inaccessible ways (Ogloff and Otto, 1991; Spriggs, 2010a). Ironically, this has often led to children not understanding the nature of their involvement (Spriggs, 2010a). Our ethics committee and research partners (including the Royal Commission) allowed us to develop an information resource that was more accessible and ‘child-friendly’. This brochure, developed with children, aimed to introduce the researchers, and explain: the purpose of the study; how we would use the findings; how we would attempt confidentiality (and its limits and our limitations); and what ‘rights’ participants would have if they chose to participate.
We did not, as is usual research practice, include a list of topics that children might discuss during the focus groups or the discomfort that they might experience if they were to choose to talk about these issues. This was because the methodology was exploratory, grounded and iterative and, as noted above, the topics that were discussed in the focus groups were ones that participants identified themselves after being asked open questions such as ‘what are the things that are unsafe for children?’ and ‘what are the things that worry children?’. If we had listed potential topics in the brochure we may have influenced children’s answers. The impacts of talking about sensitive topics were then attended to and revisited as topics were highlighted by participants.
Our Ethics Committee accepted this rationale for omitting the topics and sensitivities but directed us to help children understand the implications of choosing particular topics, by asking things such as ‘what is it like for children when they come across a situation like this?’ and ‘what do children need when they are unsafe?’. We discuss this further below.
Element 2: understanding information
As some of the participants had completed their consent forms sometime before the group was held, we could not always be sure they had fully read and comprehended the information brochure and consent forms we had provided (Pedersen et al., 2011; Varnhagen et al., 2005). Alderson and Morrow (2005: 111) note,
Providing clear information which has an emphasis on children’s rights has been found to assist children and their parents to give informed and unpressured consent to participate in research.
To ensure and confirm children understood their rights within the research context, we utilised an activity used in previous studies. Double-sided cards were printed, with the research rights (such as ‘privacy’, ‘choice’, ‘respect’, ‘stop participating’) on one side and brief summaries of their meanings on the other. The cards were placed on a table with the rights facing up and children were asked to choose a card they thought they could explain to the group. One by one the rights were chosen and children invited to explain what the right might mean for the focus group and to give examples. After each right was explained, researchers provided additional information and checked in to make sure that all participants understood what the right meant in practice. Sometimes we gave the children a hypothetical like “so once you’ve agreed to participate you pretty much have to sit with us for three hours” and asked whether they agreed or not.
No, it means that you should be involved but you should be able to go if you don’t want to stay.
It said that you can choose what you do so I think that means you don’t have to be here all the time.
But it’s in class so maybe you do
Mine [my card] says it will be fun
So what would you be happy to agree to?
To be involved for as long as you want to
As long as it’s fun
So it has to be fun or you’ll leave?
No, but it shouldn’t be boring or we’ll want to go
We’ve got PE after lunch so make sure it’s funnier than that.
Make it interesting, something that kids want to do.
Well the situation is that how long you stay and whether you stay or go is entirely up to you. We’ll try to make it as interesting and fun for you as we can and we will give you lots of choices along the way so that you get to talk about things that YOU want to talk about. Really, although we’d love for you to stay, you don’t have to and you can leave at any time. We’re just delighted you’re giving us any time at all.
And we can keep the movie tickets?
Yep, they’re yours. Even if you decide to leave right now
Right, I’m leaving! [laughter] … Just kidding
A charter of rights.
In relation to the movie ticket mentioned in this last quote, we had decided that children should be given a small gift in recognition of their involvement in the study: for their knowledge and expertise. So that children did not feel obliged to participate once they were aware of, or received their movie ticket, we informed them that they could keep the voucher regardless of their participation.
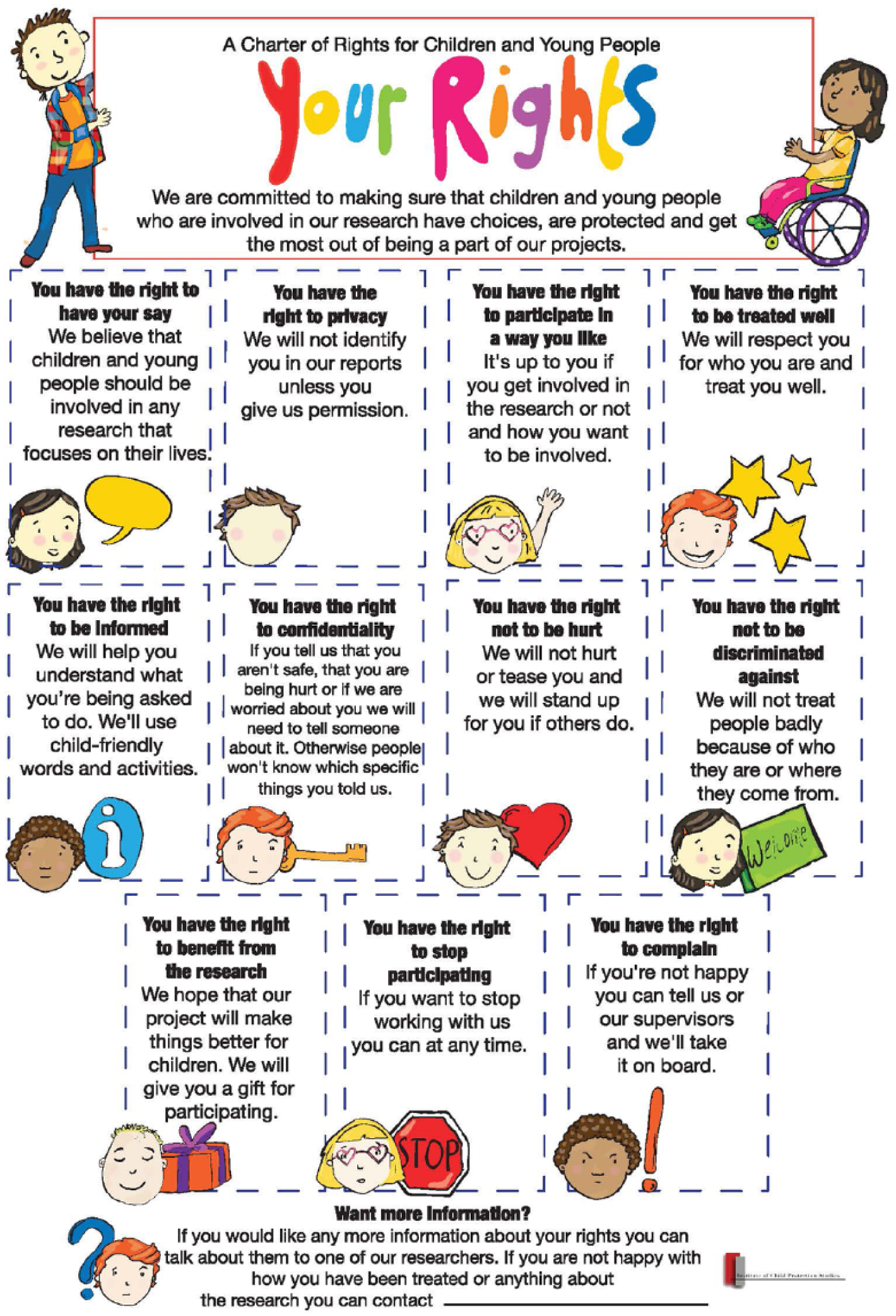
To reinforce this exercise, we provide participants with a copy of our ‘Charter of Rights for Children and Young People’ which we had developed in partnership with a Children’s Reference Group from a previous project (See Moore et al., 2008). The poster, illustrated by Fuzz Illustrations, articulates 11 rights related to children’s participation in research discussed in the preceding activity. It contains three components: a statement of the right, an explanation of it and a related image. Participants were asked retain the rights poster and refer to it throughout their involvement in the focus groups. We did this as we believe it is important to provide children with information in a variety of forms to ensure those with different needs are given multiple opportunities to explore and understand important concepts (in this case, their rights). Further discussion about the poster can be found elsewhere (Dockett et al., 2013; Moore et al., 2008).
Element 3: formally indicating their consent
To formally indicate they understood and agreed to participate in the study, participants were given a consent form that reiterated the purpose of the research. Recognising that some children had not completed the form before coming to the focus group and as some found it difficult to read, we read the statements aloud and asked them to indicate that they understood what they were going to be asked to do and the nature of their rights within the research process. Rather than just providing one statement that included all these dimensions we listed each aspect of the study and their involvement within it separately – as captured in the figure below.
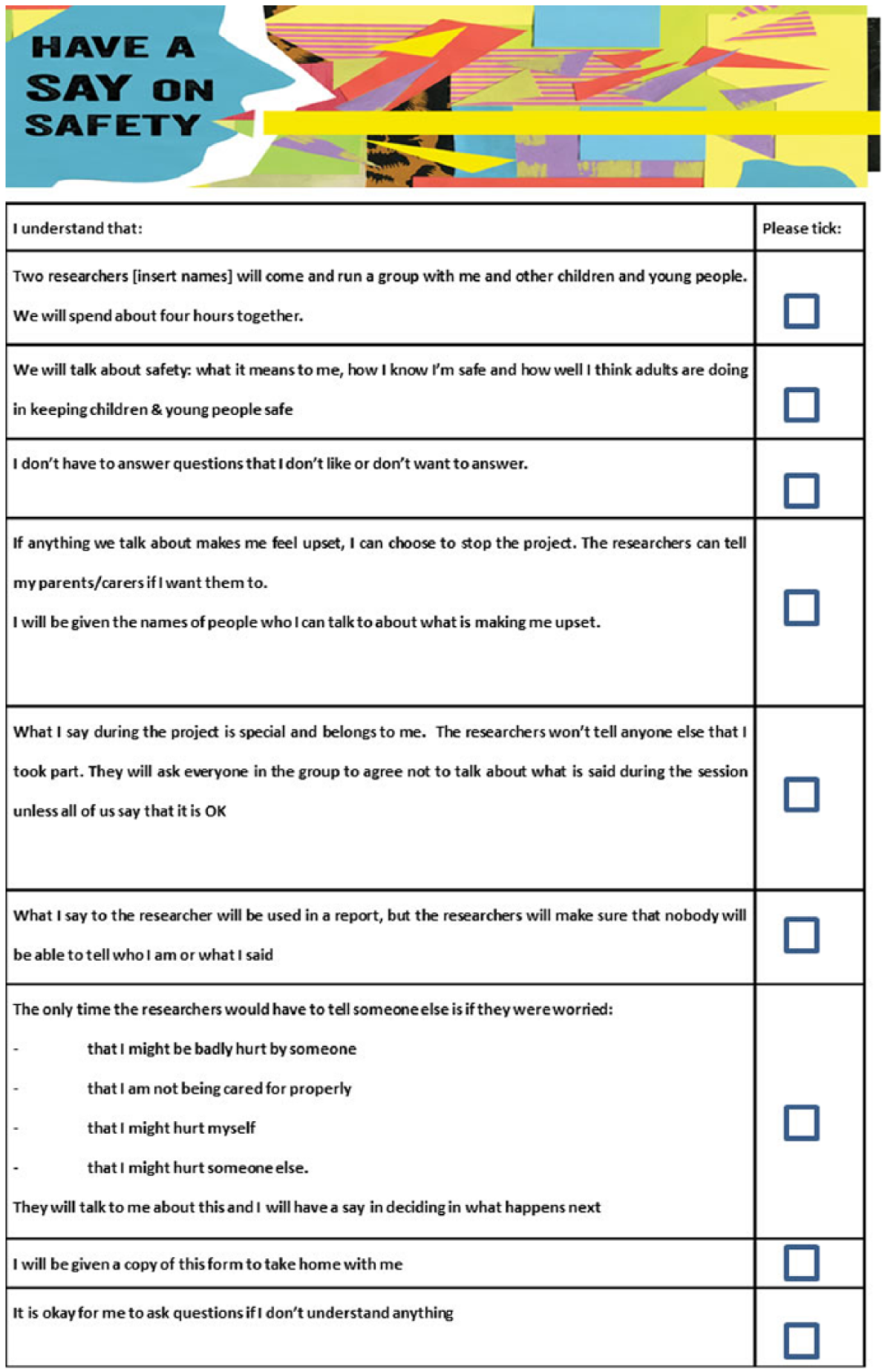
Consent form.
Completing this consent form provided a further opportunity for children to understand, ask questions, seek clarification and negotiate meanings prior to agreeing to commence involvement in the study. For example, we clarified that data would “be used in a report” from which we would develop journal articles, presentations to those working with children and conference papers. Although we did not go to the same extent that others have (see Mannay, 2014) we described the purpose and nature of these activities (to help a broader range of people know about the study and to influence practice) more fully.
A number of participants felt that this process was repetitive and were keen to begin, for others it became obvious that they needed more time to contemplate the rights before providing consent. This seemed to be particularly important for children who weren’t adequately briefed by their parents prior to arriving at the venue. These children reported they knew we were going to talk about safety, but did not fully appreciate what we would do with the information they provided.
This [focus group] was a lot different to what I expected. Like I read the letter and stuff but still didn’t know what I was saying yes to until it got going. (Young person, Focus Group)
Element 4: Providing openings for periodic disengagement or dissent
Previous studies have shown that children believe that adults can easily revoke their rights and often do so (Ruck et al., 1998). As such, we needed to demonstrate that we take children’s rights seriously and provide multiple openings for participants to affirm them. Participants were given a range of choices during the group interviews. We asked participants whether they would be happy for us to audiotape focus groups on a digital recorder. We explained that even if they said ‘yes’ we were happy for them to rescind their consent if they were unhappy with something they said or regretted saying something at a particular point. We also showed them how to stop and pause the audio recorder if they had any ‘off-the-record’ comments or questions they would like to ask. This practice is in line with other researchers who argue the consent process should not only inform participants about the use of the recordings but also include choices about what is recorded (Renold et al., 2008).
We also provided participants with ‘Stop’ and ‘Go’ cards and asked them to indicate, during each discussion, whether they were happy to talk about the topic being considered. In the groups with younger children we occasionally asked participants to use the cards to indicate whether they agreed with a view or idea that had been raised in the group – to confirm themes but also to remind them that they had cards and that they had meaning. Across the nine focus groups, only three children chose to use a ‘Stop’ card. When children pointed to the card or otherwise indicated that they were choosing to disengage from a particular conversation, the researchers quietly reminded the child that they could either stay seated with the group or have some ‘time out’. Although only a few participants utilised the ‘Stop’ cards, they stated they appreciated having the cards and would have used them if they needed to:
We didn’t need to use them but it was good to know that we could. It let us know that you were serious. (Focus Group, Young People)
Allowing periodic disengagement or dissent
In addition to enabling children to provide consent (outlined above) some argue that researchers must also enable children to actively and passively dissent (Dockett et al., 2012). Dockett et al (2012) describe dissent as: “children’s disinclination to participate, expressed verbally and/or non-verbally”. In this study, individual children in two of the groups decided to move away from the group and sit by themselves and play with some of the art materials or games that we had brought with us for focus group activities. In one circumstance, this was at the suggestion of the researcher who noticed that a boy seemed distracted and disengaged from the group. We believed that it was important to acknowledge the child’s disengagement and remind participants that they could choose whether they continued to participate or not. We, like others (including Gallagher, 2008; Mishna et al., 2004; Parsons et al., 2015; Warin, 2011), did so as we believe that it is important to be aware of, and responsive to, the more subtle signs or techniques children may use to resist power differentials or to indicate they may no longer wish to participate or discuss a particular issue.
Initially we thought that these children had totally disengaged from the research; deciding to remove themselves entirely. However, in both situations, the children returned to the group when discussing issues or completing activities of interest to them by either calling out or physically returning to the group and leaving again after making their point.
In addition, one young woman decided, during a break, that she did not want to continue participating. She stated that she had had a recent experience where she felt unsafe and that the discussion made her feel uncomfortable. She also remarked that the focus group was different to what she had expected and she appreciated that she did not feel pressured to stay. She took her movie voucher and called a parent to pick her up.
Supporting participants to voice different views, even when there was pressure for them to conform
Most of the groups that we formed for the research included clusters of children who already knew each other and had pre-existing power relationships. Although we did not attempt to neutralise these relationships, realising that this was often impossible and not particularly helpful (Gallagher, 2008), we did spend time encouraging participants to be “frank and fearless” in their participation. At the beginning of focus groups, we informed participants that we anticipated individuals to have different views and argued that one of the premises of the study was that adults and children often had different views about things like safety and that we were keen to explore these differences. We argued that, for the purposes of this study, we wanted to create a space in which children’s views were privileged (over adults’) and reinforced this in the way that we responded to children’s input: ‘I’d never thought about it that way’, ‘that does seem different to what adults have said – that’s important’.
Participants were also given opportunities to choose alternate ways of providing input (or ‘data’) – by writing things down or having side-conversations with the researchers when other participants were busy completing a task individually. As such, we gave participants permission to engage in ways that may have lessened or neutralised the power relations inherent within focus group settings.
Element 5: renegotiating consent at pivotal moments
As noted above, consent has been constructed as both the initial formal step when children are asked to agree to participate in research and also the ongoing opportunities for children to opt in and out of research along the way (Cater and Øverlien, 2014; Dockett and Perry, 2011; Morris et al., 2012; Spriggs, 2010b). It also incorporates processes that enable participants to make decisions about how they participate in the research itself (Moore et al., 2011). This is particularly necessary in qualitative research where methods are semi-structured, iterative and dialogical:
The reflexive nature of qualitative research, its use of unexpected ideas that arise through data collection and its focus upon respondents’ meanings and interpretations renders the commitment to informing respondents of the exact path of the research unrealistic. (Parry and Mauthner, 2004: 146).
Like Renold et al., (2008), we believed that it was important to check-in, at each stage of the process and to view consent as being ‘in process’ and ‘unfinished’ (Bahn and Weatherill, 2012). As explained below, this was particularly critical when concluding discussions and beginning new conversations and when discussing things that may cause discomfort.
When concluding discussions and beginning new conversations
After the end of an activity, after a break or when we sensed there was some discomfort (or boredom) amongst the group we would ‘check in’ with participants. To do this we used ‘kimochi’ dolls: small felt toys that have an emotion (such as happy, sad, hopeful) printed on one side and a face depicting that emotion on another (Townsend, 2012). We placed the kimochi dolls on the floor and asked children to choose a doll that reflected how they were feeling.

Kimochi dolls.
After ‘checking in’ we asked all children (particularly those whose kimochis suggested that they were unhappy, bored or displeased) if they wanted to continue and asked the whole group if there were things that they would like us to do differently. We also ‘checked in’ to see whether they felt enough opportunities had been afforded to them to make decisions throughout the focus group and asked for advice on how we might better respond to their needs:
Right this minute I’m feeling … happy but … yesterday I felt left out and sad but now I feel happy.
I’m sorry to hear that. When kids feel ‘left out’ what should we do? How can we get them more involved? Make them feel better?
You made sure that everyone got to say something and made us feel like what we said was good. You should do that and make sure that people don’t feel left out. [Other children offered suggestions]
Yeah good one. Thanks for your ideas. We’ll definitely do those things. We might check back in later to make sure that no one is feeling left out. Is that OK?
Yep.
Although we would hope that we were already mindful of children who ‘felt left out’, researchers made a concerted effort to watch the group and to utilise the strategies identified by participants when children seemed isolated from the group. At the suggestion of children, for example, one of the researchers approached a quiet child during one of the breaks and ‘checked in’ to see if there was anything they would like to add to what had been discussed. The child reported that they were OK and had nothing to add.
When discussing things that may cause discomfort
As noted above, we were aware that participants may raise sensitive topics when asked to identify their safety concerns. We recorded all topics raised together and, in summarising them back to participants we noted that some might be topics that some people may find difficult to discuss. Before further exploring them, we reminded participants that we needed to balance our interest in discussing topics that ‘mattered most’ to children and our need to make sure that everyone felt comfortable. We then reminded them of our agreements: to only discuss topics in a way that kept people emotionally safe (by not asking people for their personal experience but instead talking about issues generally), for people’s stories to remain confidential unless we worried about their safety; and for focusing our discussions on the relevant questions: in this case, ‘what children consider is already being done and should be done to respond to safety issues and risks in institutions?’ We then asked them to indicate that they understood what was being asked of them, any risks that might be foreseen and to re-affirm their consent to participate. We also reminded them that they did not need to answer any questions or do anything that might make them feel uncomfortable.
Element 6: an agreement at the end of the research activity
It has been our experience (and of others, for example: Richards et al., 2015) that after research is conducted with children, adults who have a relationship with the child will ask the researcher or participants what was discussed during the session. In previous studies, these adults (namely parents, teachers, principals and social workers) have been taken aback when we have given them vague responses like ‘they gave us some great ideas’ or ‘the group went really well but unfortunately I can’t say more’. We have noted that children, too, can sometimes be confused about confidentiality limits and what they are able to share with others.
To resolve these issues and reaffirm our commitment to viewing data as being owned by participants, each focus group ended with a confidentiality agreement activity. Researchers reminded participants (including any adults sitting in) that we had agreed not to share anything outside the group without their expressed permission.
We then informed participants about our previous experiences and asked them what they thought we should say if a parent, teacher or adult might ask about the focus group discussions. Like others, children often demonstrated a keen interest in discussing how their voices and views would be shared within and outside the research process (Pinter and Zandian, 2015). We asked them whether there were things that they would be happy for us to share and whether there were things that no member of the group (researchers, observing adults and children) should share. We noted these topics on the ‘Sharing Our Story’ form below and asked participants to indicate their agreement (using the Stop/Go signs or signatures).
Examples of ‘what we don’t want them to know’ were things that they thought might cause embarrassment (like ‘my teddy makes me feel safe’) or things that might cause repercussions (like ‘names of teachers who have favourites’). Among a substantial list of things under ‘what it is OK to tell them’ and ‘what are the things we want them to know’, participants included things like wanting adults to know that they were mostly doing a good job, to give children more options to have their say, and to work with them to come up with better responses to their safety concerns. At the end of the discussion, the group was asked to indicate that they were all happy with what had been recorded.
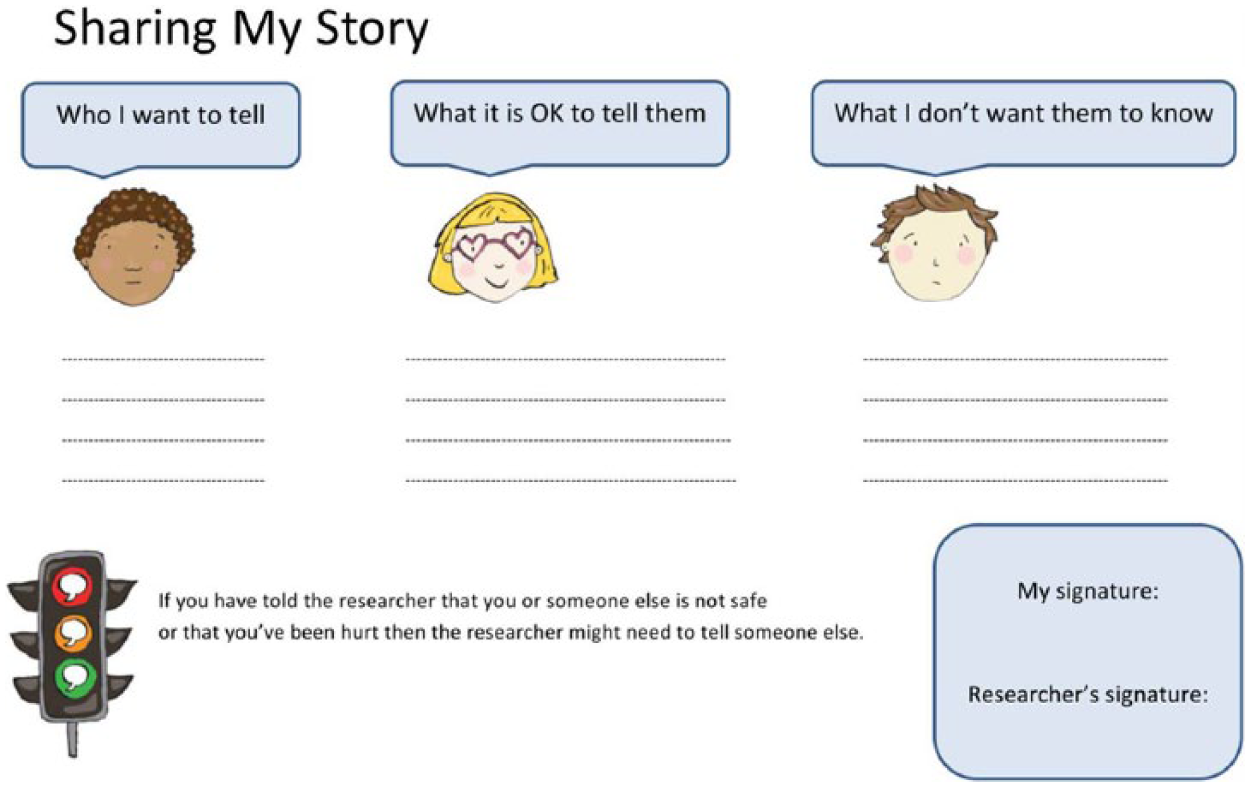
Sharing My Story.
Conclusions
Children’s informed consent in participatory research is as an essential component to ethical research practice. Although there has been significant attention from researchers about the importance of seeking children’s informed consent prior to their participation in data collection, this paper supports the view that it is critical to see consent as an ongoing process rather than a hurdle to be overcome prior to data collection.
Drawing on our experience within a highly scrutinized study that aimed to explore children’s experience and conceptualization of safety from sexual abuse (among other safety concerns), we provide observations about the tools we used and the rationale for their inclusion. This includes the need to ensure children understand what is expected of them in the research process and the need to renegotiate consent at different points throughout the interaction (particularly when participants have choice about topics being discussed and when other in-the-moment ethical concerns emerge such as discomfort). We have also argued for the need to develop an agreed position on what can be shared with others outside the focus group.
Finally, we have offered examples of some of the strategies and tools we used to support the consent processes which we hope will be of assistance to other researchers. Along with our reflections on how particular tools can be utilised to support consent, of particular significance is the feedback offered by children in our reference groups and focus groups. Their feedback provides some confidence that tools such as these can support participants to engage in the consent process to ensure quality in research conducted with children.
Footnotes
Acknowledgements
The methodology presented was strengthened as a result of the active participation of three Children’s Reference Groups and the insights of the 121 children who engaged in focus groups. We would like to close by thanking them for their advice and guidance and their willingness to engage in a collaborative effort. We would also like to acknowledge the Royal Commission into Institutional Responses to Child Sexual Abuse, our University’s Human Research Ethics Committee and to the schools and youth organisations who enabled us to explore these issues comprehensively. We hope that our observations prove helpful for those embarking on the children’s research journey.
Funding
This project was only possible as a result of the funding and ongoing support and commitment of the Royal Commission into Institutional Responses to Child Sexual Abuse.