
Abstract
In this study, the anti-inflammatory and antioxidant known as lycopene was applied to rats with experimental diabetes with the aim of investigating the detection of diabetes-related complications, and to determine the possible role of lycopene in diabetes complications regarding the effects of ACE activity. In order to induce diabetes in rats in the diabetes (D) and diabetes+lycopene (DL) groups, rats were given 45 mg/kg single-dose streptozotocin (STZ) intraperitoneally (i.p.); lycopene (10 mg/kg/day dissolved in sunflower oil) was administered to the rats in the lycopene-only (L) and DL groups. Blood glucose levels and HbA1c% in diabetes+lycopene group and diabetes group increased (p <0.05) compared to control and only lycopene treated group. The highest level of ACE activity was observed in the (D) group (p < 0.05). Activity in the (L) group was also significantly greater than in the control group (p < 0.05). The (DL) group had lower (p < 0.05). ACE activity than the (D) group. Lycopene implementation was found to be effective in the inhibition of ACE activity, an important indicator of diabetes-related complications.
Introduction
Diabetes mellitus is a common illness with high morbidity and an early mortality rate, causing vascular, renal, retinal, or neuropathic disorders in the long term as well as acute metabolic complications.1,2 Much research shows that long-term hyperglycemia causes adverse changes in blood vessels.
Hyperglycemia, which occurs long before diagnosis, may cause organ damage. For this reason, early diagnosis is important, as is appropriate and effective treatment for patients with diabetes mellitus.1,3,4 Glycoprotein concentrations are very useful in the evaluation of glycemic control and long-term monitoring of blood glucose, and are widely used addition to blood glucose measurements. Among them, the most common is HbA1c (glycosylated hemoglobin).5,6
Angiotensin-converting enzyme (ACE) is a component of the renin–angiotensin system (RAS), and leads to the conversion of angiotensin-I to angiotensin-II in vascular tissues. Angiotensin-II is one of the most important vasoconstrictive substances and an effective dipeptide in pathological events, and is produced in pulmonary vascular endothelial cells and in the vessel wall structure.7-10
The RAS plays a role in the regulation of fluid and electrolyte balance, cardiovascular functions and the control of arterial pressure.8,11 ACE inhibition increases the success rate in the treatment of hypertension and congestive heart failure. 8 It has been reported that ACE plays a key role in the formation of atherosclerotic lesions. High levels of tissue or circulating ACE lead to atherosclerosis in the vascular wall. 9
The RAS is an important factor in the pathogenesis of diabetic nephropathy. It has been observed that renal damage in diabetic patients was stopped with the inhibition of RAS. The ACE gene leads to an increase in plasma ACE activity and increases the tendency to nephropathy. 12 Üstündağ et al. 13 found that ACE levels in individuals with diabetes were increased in serum, lung, liver and kidney, depending on the diabetic complications.
Increases in ACE levels in plasma are an important potential marker in many cardiovascular complications and diseases such as myocardial infarction, diabetic nephropathy, stroke and multiple sclerosis.14-17 Decreased levels of ACE are important in Alzheimer’s disease and lung and liver tumors.18,19 It was reported that serum ACE activity in diabetics with retinopathy was significantly increased compared with controls. It was considered that this situation significantly increases the activity of this enzyme in diabetic vascular damage. 20 As several studies of ACE inhibitors in patients with diabetes, nephropathy and cardiovascular events show reduced mortality, therapy with ACE inhibitors in hypertensive diabetic patients is recommended. 21
Lycopene, found naturally in fruits and vegetables, is a pigment which belongs to the carotene family (a carotenoid). Although found in many fruits and vegetables, lycopene is mostly found in tomatoes and tomato products.22,23 It demonstrates antioxidant activity due to its acyclic-shaped long-chain form, extremely hydrophobic nature and conjugated double bond. Lycopene’s antioxidant properties work by destroying oxygen radicals, as retinol, α-tocopherol and carotenoids do. 24
It has been observed that when patients with type 2 diabetes consume tomato juice, the malignant transformation of oxidized ‘bad’ cholesterol was significantly reduced, which was dependent on a significant increase in the level of plasma lycopene. Serum carotenoids (which also contain lycopene), are closely associated with type 2 diabetes, and decrease in a linear fashion as a result of deteriorating glucose metabolism and abnormalities of glucose tolerance. 25
Little is known about the relationship between carotenoids and diabetic complications. Lycopene can be effective on macrophages and foam cell formation and ox-LDL uptake, with an increase in natural immunity and the prevention, particularly long-term, of diabetic complications, namely cardiovascular diseases.26,27
The use of experimental animal models is widespread to understand the pathogenesis and prevention of various diseases, and to examine treatment possibilities. Experimental models of diabetes have an important role in the investigation of complications caused by diabetes and the determination of treatment approaches. This study aimed to investigate the possible role of lycopene in diabetic complications, and demonstrate the effects of lycopene, known for its anti-inflammatory and antioxidant protection, on ACE activity, in rats with experimental diabetes.
Materials and methods
Animals
For this study, 28 male Wistar-Albino male rats weighing 200–250 g were obtained from the Experimental Research Laboratory of Yuzuncu Yil University Medical School. Rats were accommodated in cages with permanent food and fresh water, 12 hours dark / light and temperature set to 22 ± 2°C during the 4-week trial. The experiments were conducted according to ethical guidelines and under the supervision of Yuzuncu Yil University Local Ethics Committee of Animal Experiments.
Preparation of the trial groups
To create the diabetes (D) and diabetes+lycopene (DL) groups, 45 mg/kg single-dose streptozotocin (STZ) (Sigma, USA) in pH 4.5 citrate buffer was administered by the intraperitoneal (i.p.) route.
Control group: selected randomly, rats were separated for the control group. A single dose of physiological serum was injected i.p.
Diabetes group (D): 45 mg/kg single-dose STZ was applied to seven rats; 72 h later the glucose levels in blood samples taken from the tail vein were determined by PlusMED Accuro brand glucometer equipment and through its strips. Those rats with blood glucose 270 mg/dl and above were regarded as diabetic, and were included in the study.
Diabetes+lycopene group (DL): STZ was administered to the group of seven rats i.p.; 72 h later, the glucose levels in blood samples taken from the tail vein were determined by PlusMED Accuro brand biosensors glucometer. Lycopene, dissolved in corn oil (Redivivo-10% FS (DSM Food Ingredients Ltd. Co.)) was applied orally to those rats with blood glucose levels of 270 mg/dl and above, at 10 mg/kg/day for 28 days.
Lycopene group (L): lycopene, dissolved in corn oil was applied orally 10 mg/kg/day for 28 days.
Sample collection
After the 4-week trial, blood samples were taken the from the animals, under ether anesthesia, from the left ventricle of their hearts, into tubes with anticoagulant and gel.
Glucose levels were determined in blood samples taken from the tail vein. Determination of the amount of HbA1c was performed in whole blood with a commercial kit (Roche Diagnostics GmbH, D-68298 Mannheim, Germany) and an autoanalyzer (HITACHI-911) on the same day. Measurement of ACE activity was performed by using a commercial kit (Colorimetric ACE Angiotensin-Converting Enzyme Assay-enzymatic Bühlman Laboratories AG).
The data from control and experimental groups were analyzed with a One Way Variance analysis and the Duncan test was applied for multiple comparisons. Differences were considered as significant when the p-value was less than 0.05.
Results
Blood glucose values were evaluated statistically (see Table 1). The highest blood glucose concentration was detected in the experimental diabetic group (D) (p < 0.05). Although blood glucose levels of the (D+L) group were high (p < 0.05) with respect to the control group and the (L) group, they were significantly lower (p < 0.05) than the (D) group. Blood glucose levels between control and (L) groups were not statistically significantly different.
The glucose and HbA1c levels and ACE activities of control, diabetes, diabetes+lycopene and lycopene groups
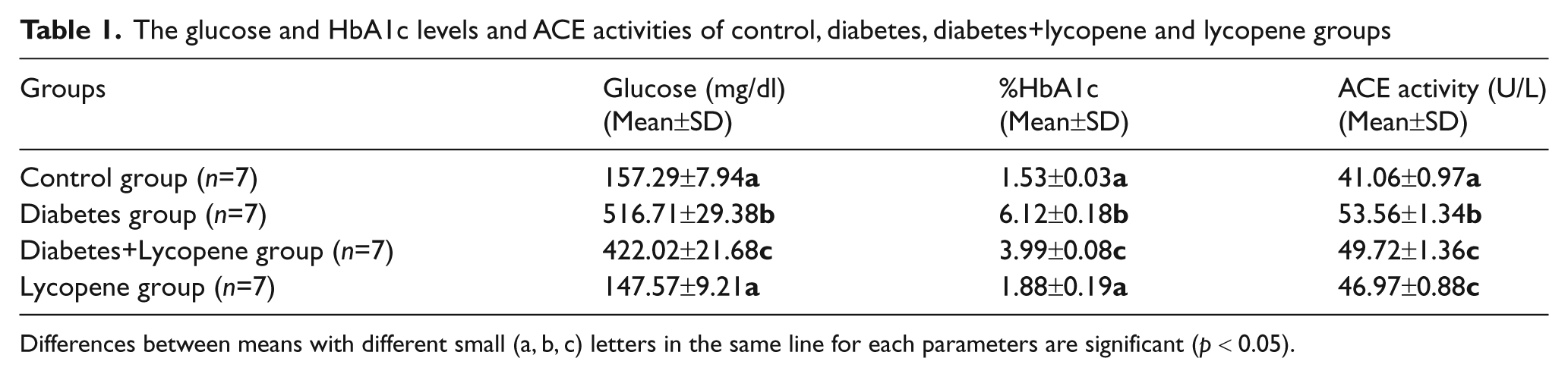
Differences between means with different small (a, b, c) letters in the same line for each parameters are significant (p < 0.05).
After statistical evaluation of HbA1c% level, the highest (p < 0.05) level was observed in the (D) group. A significant increase in the levels of HbA1c% (p < 0.05) was determined in the (DL) group in respect to the control group and the (L) group. However, with regard to the (D) group, levels were significantly decreased (p < 0.05). There was no statistically significant change observed regarding HbA1c% in the control and (L) groups.
The highest level of ACE activity (p < 0.05) was observed in the (D) group. Activity in the (L) group was found to be significantly (p < 0.05) greater than in the control group. A significant decrease (p < 0.05) was observed in the (DL) group, in respect to the (D) group. The ACE activity of this group was significantly higher than in the control group (p < 0.05), but no statistical difference was observed with the (L) group.
Discussion and conclusion
Cardiovascular disease and peripheral vascular disease are important among the macrovascular complications that occur over time in diabetes mellitus. There is a close relationship between diabetes and arterial hypertension.28,29 The RAS is involved in blood pressure regulation and fluid electrolyte homeostasis, and plays an important role in the pathogenesis of hypertension by controlling water and salt homeostasis and vascular tone.29,30
The RAS plays a part in the pathogenesis of glomerular damage occurring in diabetes mellitus. Complications observed in diabetes mellitus are associated with the widespread vascular damage caused by changes of the RAS in the circulation. 30 Some organs (pancreas, fat, muscle and liver) are considered to have their own local RAS. 31 The existence of angiotensinogen, which is a RAS component, ACE and angiotensin type 2 and 1 receptors (AT1R and AT2R) in the pancreatic islets, makes this an important basis for verification of this hypothesis. 29
The RAS is an important factor in the pathogenesis of diabetic nephropathy. Inhibition of the RAS stops renal damage in diabetic patients. 12 The aspects of glucose metabolism which may have an activating effect on the RAS are not yet understood. A decrease in levels of RAS components, and secretion of insulin and an increase in cell apoptosis were found in pancreatic islet cells exposed to long-term incubation of glucose. 31
In the present study, by statistical evaluation of ACE activity, it was observed that the ACE activity was significantly increased (p < 0.05) in the experimental diabetic group when compared with the other groups. It was determined that these data are in agreement with other results in this area.
Contradictions were found regarding the research results on the activity of serum ACE in diabetic humans and rats. Varying information is available regarding ACE activity which could be normal, reduced or even higher in both humans and rats. 30
However, as shown in other studies as well as from the results obtained here, it was noted that ACE activity is usually increased. Several studies in patients with diabetes have found that levels of ACE were increased in 24–40% of patients. 28 It was reported that serum ACE activity in diabetic patients with retinopathy was significantly increased when compared with control subjects. It was considered that this situation led significantly to the increase in activity of this enzyme regarding diabetic vascular damage. 20 Üstündağ et al. 13 found that ACE levels were increased in individuals with diabetes as a result of complications in the serum, lung, liver and kidney.
Bor et al. 30 noted that serum ACE activity was increased in rats with experimental diabetes. They claimed that this could have been caused by damage in diffuse vessels, as a result of diabetes, which might have left ACE in the blood.
The determination of ACE activity, which is an important component of RAS, is particularly important in the diagnosis of cardiovascular and respiratory diseases. It was reported that high levels of activity of ACE in the tissues and circulatory system played a key role in vascular wall thickness and the formation of atherosclerotic lesions. Increased ACE levels in plasma have potential as an important marker in many cardiovascular complications and myocardial infarction, as well as in diabetic nephropathy.9,12,14-17
It has also been reported that ACE activity is increased in diabetes and in complications due to diabetes. Plasma ACE activity is associated with diabetic microvascular diseases such as microalbuminuria and diabetic retinopathy. 30 It was observed that plasma ACE activity in hypertensive diabetics was significantly higher than in diabetics. 28 Marre et al. 32 reported that ACE activity in patients with diabetic nephropathy and retinopathy was higher than in patients without retinopathy and nephropathy. Another study found that ACE levels in patients with diabetic retinopathy were higher than in diabetics without retinopathy. 33
ACE inhibition and angiotensin receptor blockade stand out in the literature as potential pharmaceutical treatments. Several studies have shown that not only was the incidence of diabetes reduced on treatment with ACE inhibition and angiotensin receptor blockade, but also that insulin sensitivity and glycemic control was improved. The use of these drugs provides significant blood pressure control for patients who have organ damage and hypertension, diabetes, chronic kidney disease, and for patients with heart failure.29,34
Watson et al. 35 suggested that the synthesis of ACE in diabetic subjects contributed to the acceleration of atherogenesis. In the light of this information, various studies have been performed to investigate new therapeutic options for the prevention of atherosclerosis in diabetes by blocking ACE-mediated pathways. 35 It has also been reported, in research for the prevention of retinopathy, that blockage of the RAS reduces the severity of retinopathy. 36
As a result of this study, it was observed that the ACE activity of the (L) group was significantly (p < 0.05) higher than the control group. The (DL) group showed an important reduction (p < 0.05) compared with the (D) group. ACE activity in this group was significantly higher (p < 0.05) than in the control group, but we found no statistical difference between this group and the (L) group.
In recent years, intensive experimental and epidemiological studies have strengthened the hypothesis that regular consumption of fruits and vegetables rich in carotenoids has an important role in protection against colon, stomach and prostate cancers, widely seen in humans. Oxidative stress plays an important role in the pathogenesis of type 2 diabetes and its complications. Due to its potential role in the prevention of chronic diseases caused by oxidative stress, lycopene, which belongs to a group with very powerful antioxidant carotenoids, has received considerable interest in recent years.22,23,37
Li et al. 37 reported that lycopene levels in a diabetic group were lower than in the control group, and a negative correlation between the levels of HbA1c and serum lycopene was found in the correlation analysis in a study of serum lycopene levels in diabetic patients. In diabetic patients, especially those with advanced diabetic retinopathy, serum lycopene levels were found to be significantly lower.
It was observed that consumption of tomato juice in patients with type 2 diabetes resulted in a significant increase in plasma lycopene levels, and the transformation of oxidized ‘bad’ cholesterol to products hazardous to blood vessels could be reduced significantly.
It has been reported that glucose metabolism and serum carotenoid levels showed a linear decrease, linked to glucose tolerance abnormalities. 25
Ali and Agha 38 reported the effects of the application of different doses of lycopene on hypoglycemic, hypolipidemic and antioxidant activity in a study carried out among rats with STZ-induced experimental diabetes. In this study it was found that glucose levels decreased in a dose-dependent trend with gradual implementation of lycopene corresponding to the dose of exogenous glucose in hyperglycemic rats, causing an increase in total antioxidant capacity.
Kuhad and Chopra 39 established the importance of antioxidants, such as lycopene, as adjuvant therapy in the treatment of diabetic neuropathy, as a result of application of lycopene to rats with STZ-induced experimental diabetes.
In addition, in our laboratory, we performed a project examining the effects of lycopene on pro-oxidant/total antioxidant status and vitamin levels in experimental diabetic rats, using the experimental method of Yüztaş. 40 Yüztaş 40 reported that in the diabetic group there were decreased TAS (total antioxidant status), retinol and α-tocopherol levels which were significantly different compared with the control and lycopene groups (p < 0.001). When compared with the diabetic group, in the lycopene+diabetic group an increase in TAS and α-tocopherol levels was observed, and these changes were not sufficient to constitute statistical significance in the lycopene+diabetic and control groups, which were similar in retinol levels.
In this study, it was observed that in the (D) group with the highest (p < 0.05) blood glucose concentration there was a significant decrease (p < 0.05) when compared with the (DL) group, as observed in the statistical evaluation of blood glucose values. However, blood glucose concentration in the control and (L) groups was still determined to be higher (p < 0.05). Blood glucose levels between the control and (L) groups were not statistically significantly different. Likewise, in this study, the statistical results obtained for HbA1c% levels were consistent with the results determined for the blood glucose levels.
The highest levels were found in the diabetic group (p < 0.05). Although the HbA1c% level decreased significantly (p < 0.05) in the group with lycopene+diabetes, it was still higher (p < 0.05) than in the control and lycopene groups.
It is possible to conclude, by looking at the blood glucose and %HbA1c levels, that the implementation of lycopene to rats with experimental diabetes may have beneficial effects on impaired glucose metabolism. As a result, lycopene implementation, which showed the highest antioxidant activity during lipid peroxidation and proved to be anti-inflammatory, provides a decrease in blood glucose and HbA1c levels, although being high in (D) group compared with the control group, and was found to be effective on the activity of ACE. In this study we concluded that the implementation of lycopene may be essential to prevent ACE activity, which is implicated in the pathogenesis of the complications of diabetes, in the diabetic group. This research is considered to be important to determine the effects of lycopene implementation for a current issue such as diabetes, especially for the treatment of the disease and the regulation of prognosis.
Footnotes
Funding
This work was supported by Yuzuncu Yıl University Scientific Research Projects Fund (grant number 2010-SBE-068).
Conflict of interest
The authors declare that they have no conflict of interest.