
Abstract
Background: The angiotensin-converting enzyme (ACE) gene insertion/deletion (I/D) polymorphism has been reported inconsistently as being associated with risk of pregnancy hypertensive disorders (PHDs). We examined these associations by performing a meta-analysis.
Methods: Two investigators independently consulted the Medline, Embase, CNKI, and Chinese Biomedicine databases. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated in fixed- and random-effects models when appropriate. Subgroup analyses were performed by ethnicity, types of PHD (gestational hypertension, pre-eclampsia and eclampsia), country and Hardy–Weinberg equilibrium (HWE) in controls.
Results: This meta-analysis included 30 case–control studies with 3523 cases and 4817 controls. Overall, we found that the DD variant of the ACE I/D polymorphism was associated with a significantly increased PHD risk. In the subgroup analysis by ethnicity, the results suggested that the DD genotype was significantly associated with risk of PHD development among Asians and Caucasians. Moreover, when stratifying by types of PHD, a significantly increased risk was observed for pre-eclampsia. Interestingly, when stratifying by country, a significantly elevated risk was found among ‘others’ countries (those that were not China or Korea). Limiting the analysis to the studies within HWE, the results were persistent and robust.
Conclusion: This meta-analysis suggests that the I/D polymorphism of ACE may be associated with PHD risk, especially among Asians and Caucasians.
Introduction
Hypertensive disorders in pregnancy significantly increase perinatal maternal and neonatal morbidity and mortality. Pregnancy hypertensive disorders (PHDs) – mainly including gestational hypertension (GH), pre-eclampsia and eclampsia – are the second most common cause of maternal death following postpartum haemorrhage in China.1,2 The incidence of PHDs in China is 9%, while incidence of GH, pre-eclampsia, and eclampsia is 5.4, 3.5, and 0.1%, respectively.1,2 As reported by Khan et al., 3 PHDs are among the top four causes of maternal mortality in developed and developing regions of the world. Two studies, performed by Clark et al. 4 and Berg et al., 5 reported that PHDs were the first and the third most common cause of maternal death among US populations. The best approach to reduce PHD-related complications is early identification of individuals who have higher risk. Despite extensive research in this field, the aetiology and pathogenesis of PHDs are still obscure. More and more studies have evidenced that PHDs are diseases with genetic susceptibility.6,7
The renin–angiotensin system (RAS) is pivotal in regulating blood pressure and uteroplacental blood flow. 8 Genes coding for components of the RAS are considered to be candidates that may affect the risk of GH and pre-eclampsia. 9 Angiotensin-converting enzyme (ACE) is an important circulating enzyme in the RAS, which catalyses the conversion of angiotensin I to angiotensin II and degrades bradykinin. A common insertion/deletion (I/D) polymorphism in intron 16 within the ACE gene was previously reported to be associated with different plasma ACE levels, and individuals carrying the D allele had higher ACE activities.10,11 The I/D polymorphism within the ACE gene has therefore been extensively studied in several cardiovascular adult diseases, such as coronary heart disease, stroke, and renal disease.12–15
Over the last two decades, a number of case–control studies have been conducted to investigate the association between the I/D polymorphism of ACE and PHD risk in humans. However, these studies reported conflicting results. In 2006, Serrano et al. 16 published findings from a meta-analysis (based on 2596 cases and 3828 controls from 22 studies) of the ACE I/D single-nucleotide polymorphism (SNP) and pre-eclampsia risk. They concluded that the observed small nominal increase in risk of pre-eclampsia associated with the ACE D-allele was due to small-study bias. On the contrary, Medica et al. 6 found a statistical significance between the ACE I/D polymorphism and pre-eclampsia risk when the polymorphism was considered under a recessive model (odds ratio [OR] = 1.51, 95% confidence interval [CI] = 1.17, 1.94). Both these meta-analyses were based on ACE I/D polymorphism and pre-eclampsia risk, and the sample size was small. In order to derive a more comprehensive estimation of the association between the ACE I/D polymorphism and risk of PHDs (including GH, pre-eclampsia and eclampsia), we conducted a meta-analysis to assess the association between the ACE I/D polymorphism and PHD susceptibility.
Materials and methods
Publication search
We consulted the PubMed, Embase, CNKI (China National Knowledge Infrastructure) and Chinese Biomedicine databases for all studies on the association between ACE polymorphisms and PHD risk (last search update 15 April 2011). The following key words were used: ‘pregnancy hypertensive disorders’ ‘pregnancy-induced hypertension’ or ‘gestational hypertension’ or ‘preeclampsia’ or ‘eclampsia’, ‘angiotensin-converting enzyme’ or ‘ACE’, and ‘polymorphism’ or ‘mutation’ or ‘variant’. The search was without restriction on language, conducted on human subjects. The reference lists of reviews and retrieved articles were hand-searched at the same time. If more than one article was published by the same author using the same case series, we selected the study where the most individuals were investigated.
Inclusion and exclusion criteria
We reviewed abstracts of all citations and retrieved studies. The following criteria were used to include published studies: (i) case–control studies conducted to evaluate the association between ACE I/D polymorphism and PHD risk; (ii) sufficient genotype data were presented to calculate the ORs and 95% CIs; (iii) The paper should clearly describe PHD diagnoses and the sources of cases and controls. Major reasons for exclusion of studies were (i) no control; (ii) duplicate; (iii) insufficient data were reported.
Data extraction
Two investigators extracted information from all eligible publications independently according to the inclusion criteria listed above. Disagreements were resolved by discussion between the two investigators. The following characteristics were collected from each study: first author, year of publication, country/region of the first or corresponding author, ethnicity, number of cases and controls, genotyping methods, matching variables, minor allele frequency (MAF) in controls, and evidence of Hardy–Weinberg equilibrium (HWE). Different ethnicities were categorized as Asian, Caucasian, and others.
Statistical analysis
We first assessed HWE in the controls for each study using goodness-of-fit test (chi-square or Fisher’s exact test) and a p < 0.05 was considered as significant disequilibrium. The strength of the association between PHDs and the ACE I/D polymorphism was estimated using ORs, with the corresponding 95% CIs. The pooled ORs were performed for a co-dominant model (DD vs. II, ID vs. II), a dominant model (DD + ID vs. II), and a recessive model (DD vs. ID + II). We also carried out the stratified analyses by ethnicity, types of PHDs (GH, pre-eclampsia and eclampsia), country and HWE in controls.
Both the Cochran’s Q statistic 17 to test for heterogeneity and the I2 statistic to quantify the proportion of the total variation due to heterogeneity 18 were calculated. A p-value of more than the nominal level of 0.10 for the Q statistic indicated a lack of heterogeneity across studies, allowing for the use of a fixed-effects model (the Mantel–Haenszel method) 19 ; if the p-value in the Cochran’s Q statistic was less than 0.10, the random-effects model (the DerSimonian and Laird method) was used. 20 To explore sources of heterogeneity across studies, we did logistic meta-regression analyses. We examined the following study characteristics: ethnicity, country, types of PHD, HWE in controls (yes/no), genotyping methods and study sample size (≤ 200 and > 200 subjects). Sensitivity analysis was performed to assess the stability of results.
Several methods were used to assess the potential publication bias. Visual inspection of funnel plot asymmetry was conducted. The Begg’s rank correlation method 21 and the Egger’s weighted regression method 22 were used to statistically assess publication bias (p <0.05 was considered statistically significant). All analyses were done using STATA software, version 11.0 (STATA Corp., College Station, Texas, USA). All the p-values were two-sided.
Results
Characteristics of studies
A total of 248 papers were relevant to the search words. Through screening of the title and reading the abstract and the entire article, 30 eligible articles23–52 (26 in English23–48 and four in Chinese49–52) were selected for this meta-analysis, including 3523 PHD cases and 4817 controls. Study characteristics are summarized in Table 1. There were 15 studies analysing Asian patients, 12 studies analysing Caucasian patients, one study analysing African patients, one Mixed race and one Afro-Caribbean. Studies had been carried out in China, Korea, India, Japan, Turkey, USA, UK, Italy, Poland, Brazil, Finland, South Africa, Greece, Colombia, Canada and Russia. PHD types were distributed as follows: 21 studies were concerned with pre-eclampsia, two studies were separately concerned with pre-eclampsia and GH, two studies were separately concerned with GH, pre-eclampsia and eclampsia, and five studies were a mix of pre-eclampsia, GH and eclampsia. The DNA needed for genotyping had been extracted from peripheral blood in all studies and the genotyping methods used included the classic polymerase chain reaction – restriction fragment length polymorphism (PCR-RFLP) assay in 26 out of 30 studies, polymerase chain reaction with confronting two-pair primers (PCR-CTPP) in two studies, allele-specific oligonucleotide – polymerase chain reaction (ASO-PCR) in one study, and PCR in one study. Only 12 of 30 (40%) studies described the use of positive controls and a different genotyping assay to confirm the data. The genotype distributions among the controls of all studies were consistent with HWE except for three studies.44,46,52
Characteristics of studies included in the meta-analysis
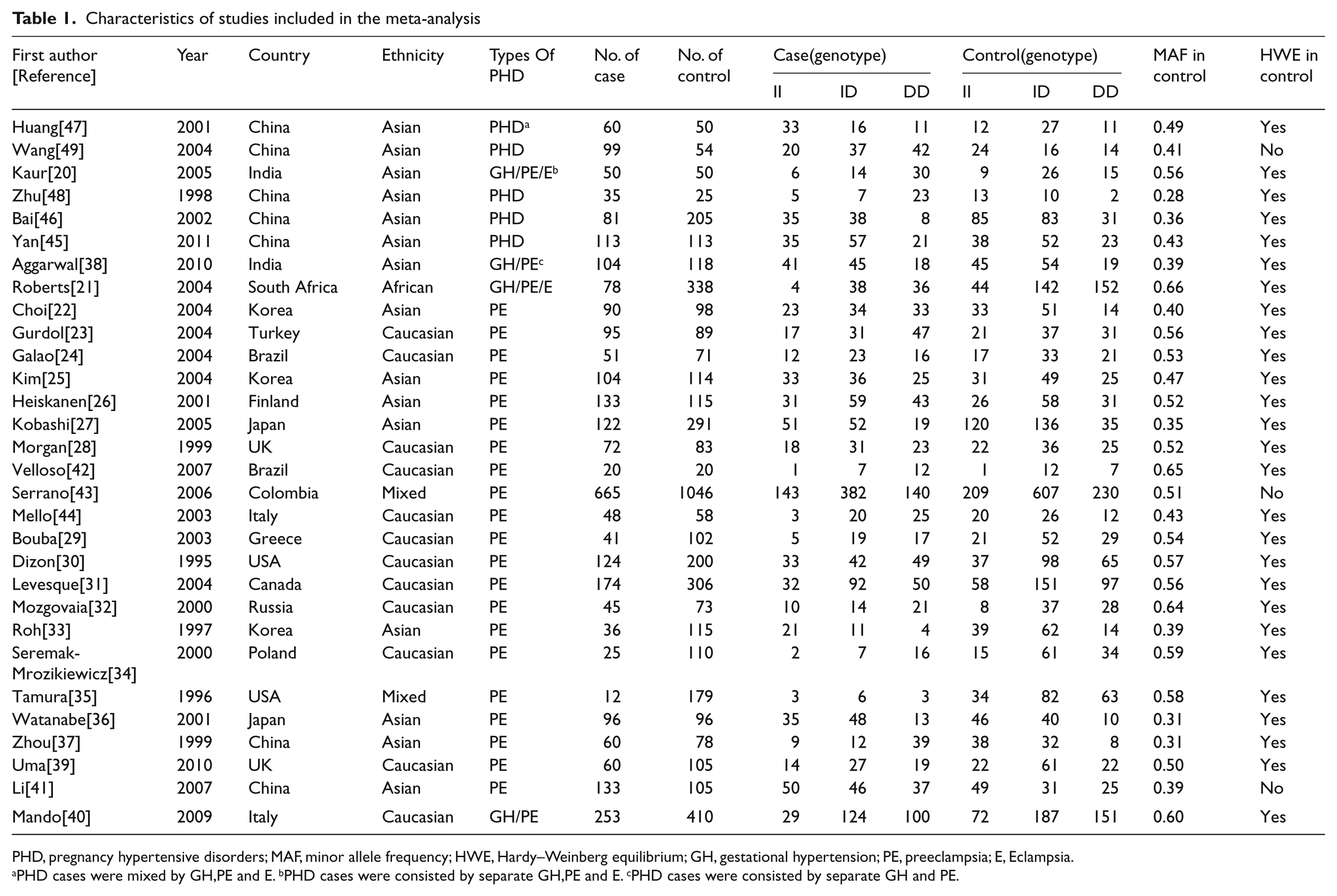
PHD, pregnancy hypertensive disorders; MAF, minor allele frequency; HWE, Hardy–Weinberg equilibrium; GH, gestational hypertension; PE, preeclampsia; E, Eclampsia.
PHD cases were mixed by GH,PE and E. bPHD cases were consisted by separate GH,PE and E. cPHD cases were consisted by separate GH and PE.
Quantitative synthesis
Table 2 lists the main results of this meta-analysis. Overall, we found that the variant DD genotype of the I/D polymorphism was associated with a significantly increased PHD risk (homozygote comparison: OR = 1.48, 95% CI = 1.14–1.92; recessive model comparison: OR = 1.51, 95% CI = 1.23–1.86) (Figure 1).
Stratified analyses of the angiotesin-converting enzyme gene polymorphism on risk of pregnancy hypertensive disorders (PHDs)

HWE, Hardy–Weinberg equilibrium; GH, gestational hypertension; PE, pre-eclampsia. For other abbreviations, see text.
Number of comparisons. bThe p-value of Q-test for heterogeneity test. Random-effects model was used when the p-value for heterogeneity test was < 0.1; otherwise, fixed-effects model was used.
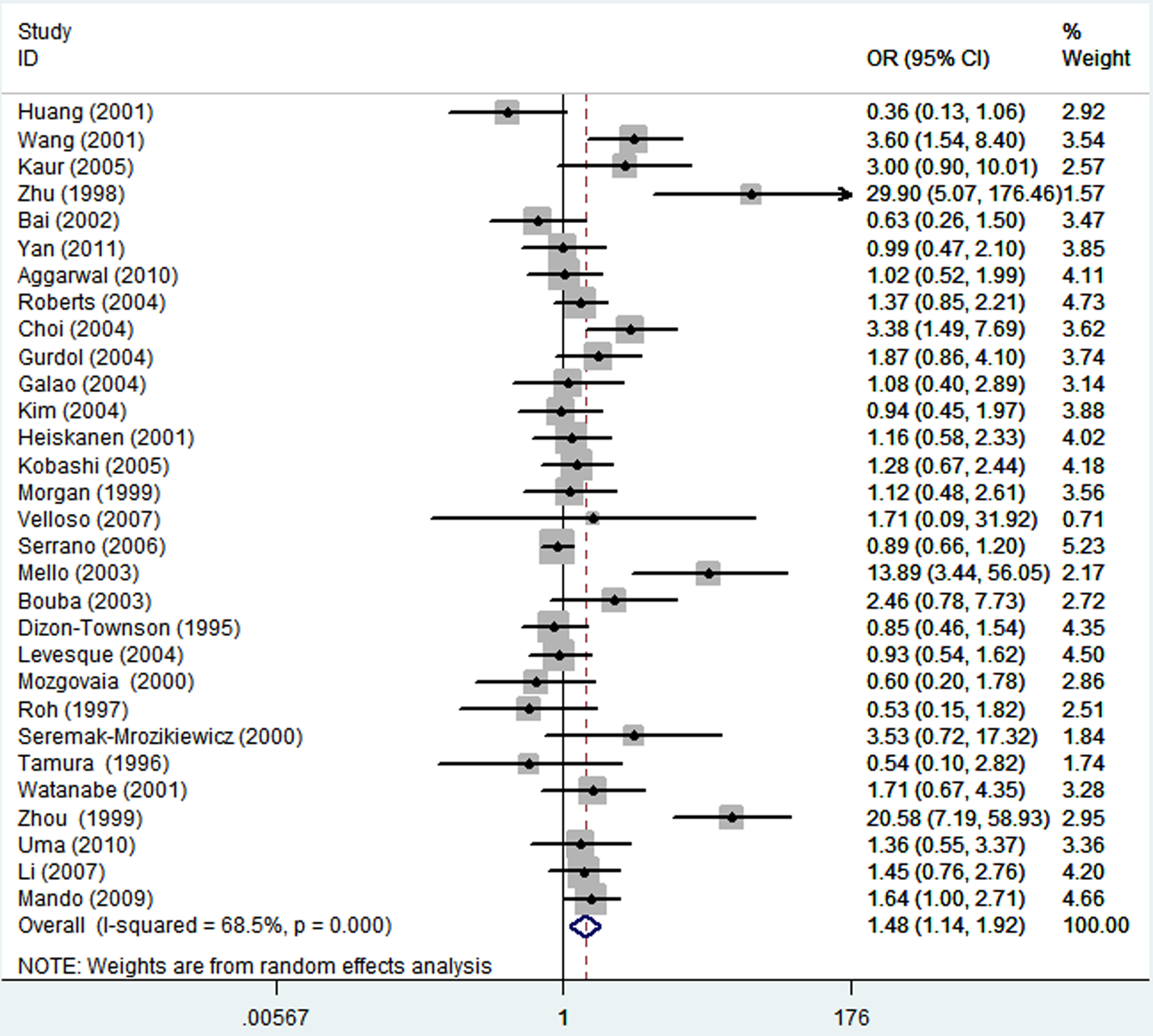
Forest plot of placental hypertensive disorder risk associated with the angiotensin- converting enzyme I/D polymorphism in overall analysis (DD vs. II).
In the subgroup analysis by ethnicity, the results suggested that the DD genotype was significantly associated with risk of PHD development among Asians (homozygote comparison: OR = 1.68, 95% CI = 1.05–2.68; recessive model comparison: OR = 1.71, 95% CI =1.14–2.57) and Caucasians (recessive model comparison: OR = 1.51, 95% CI = 1.17–1.95) (Figure 2). Moreover, when stratifying by types of PHD, a significantly increased risk was observed for pre-eclampsia homozygote comparison: OR = 1.44, 95% CI = 1.11–1.88; recessive model comparison: OR = 1.51, 95% CI = 1.22–1.87) (Figure 3). Since a large part of the analysed studies investigated Chinese and Korean populations, we also performed a stratified analysis by country, dividing the groups into China, Korea and others. Interestingly, when stratifying by country, a significantly elevated risk was found among ‘others’ countries (homozygote comparison: OR = 1.28, 95% CI = 1.03–1.59; recessive model comparison: OR = 1.34, 95% CI = 1.12–1.60), but not among China or Korea (Figure 4). Limiting the analysis to the studies within HWE, the results were persistent and robust (homozygote comparison: OR = 1.48, 95% CI = 1.10–1.99; recessive model comparison: OR = 1.56, 95% CI = 1.23–1.97).
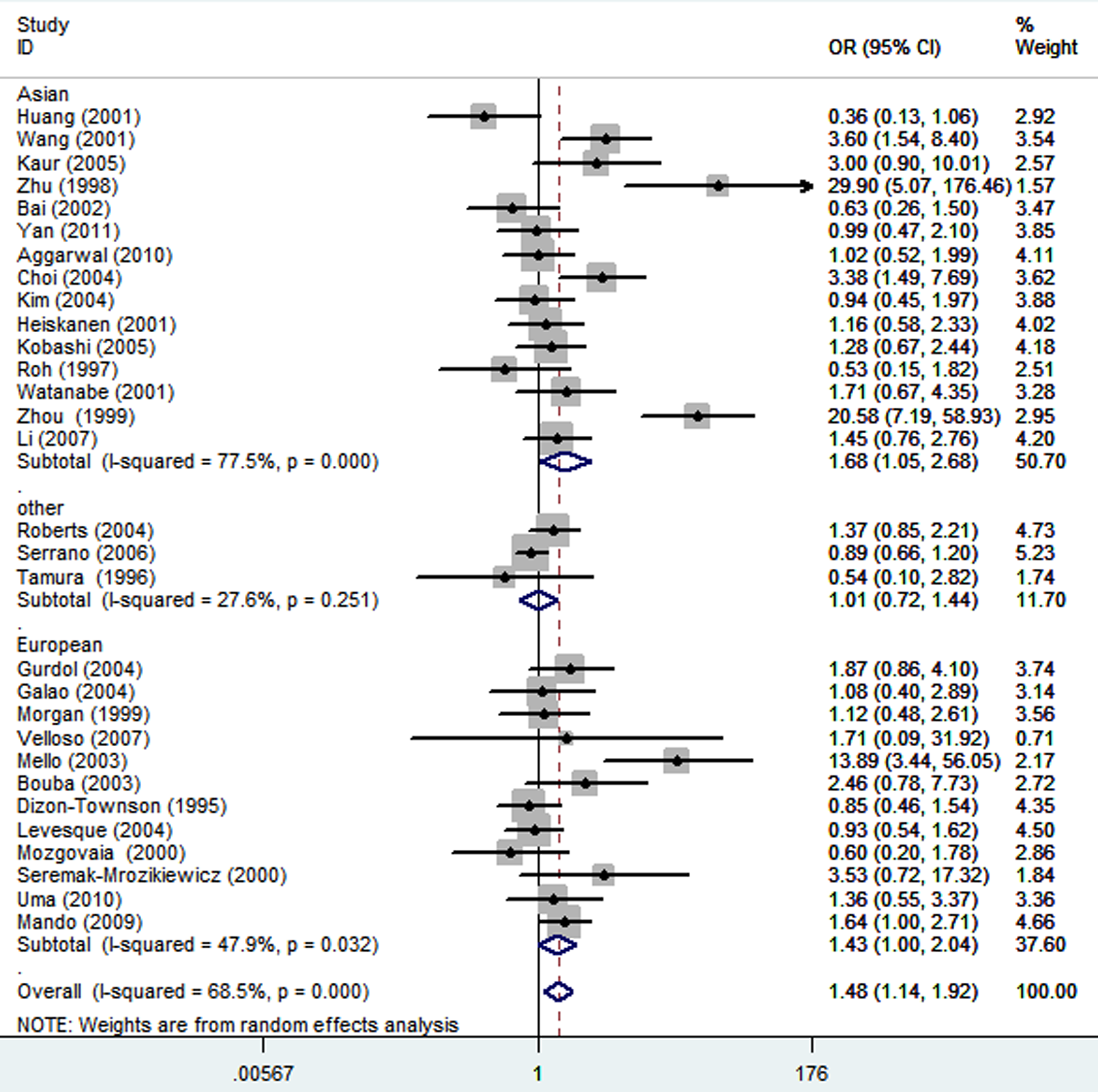
Forest plot of placental hypertensive disorder risk associated with the angiotensin- converting enzyme I/D polymorphism in different ethnicities (DD vs. II).
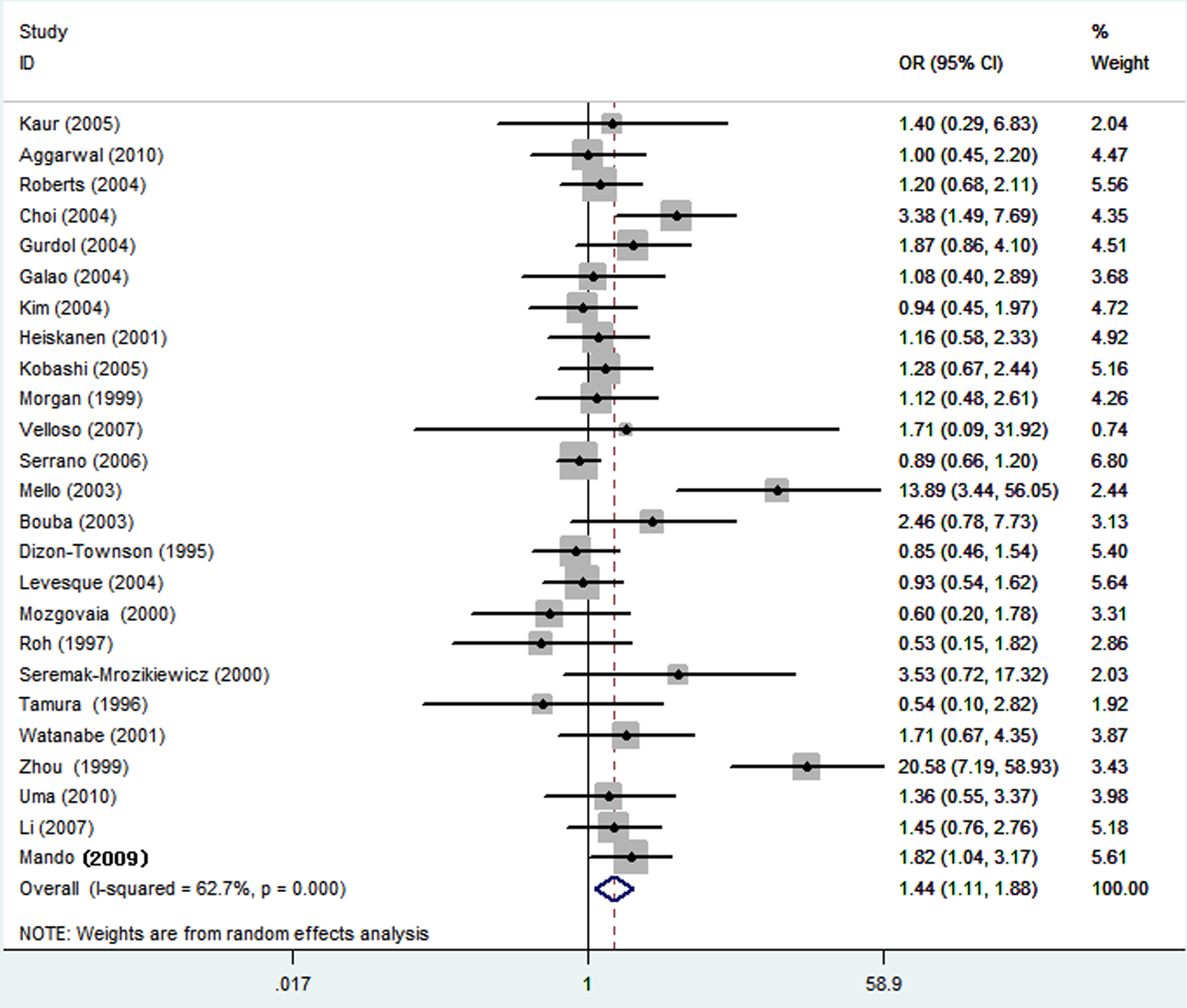
Forest plot of placental hypertensive disorder risk associated with the angiotensin- converting enzyme I/D polymorphism in pre-eclampsia (DD vs. II).

Forest plot of placental hypertensive disorder risk associated with the angiotensin- converting enzyme I/D polymorphism in different countries (DD vs. II).
Heterogeneity analysis
There was heterogeneity among studies in overall comparisons and also subgroup analyses. To explore sources of heterogeneity across studies, we assessed all comparison models by ethnicity, country, HWE in controls, genotyping methods and study sample size. As a result, sample size (DD vs. II: p = 0.04; recessive model: p = 0.002), but not the ethnicity, country, and HWE in controls or genotyping methods, was found to contribute to substantial heterogeneity (Table 3). Moreover, meta-regression analyses indicated that sample size could explain 27.90% (DD vs. II), and 66.31% (recessive model) of the τ2.
Heterogeneity analysis in this meta-analysis

HWE, Hardy–Weinberg equilibrium; for other abbreviations, see text. aCochran’s Q statistic test, p <0.1 was considered as significant heterogeneity. bMeta-regression analysis coefficients, p <0.05 was considered as significant factor that contributed to heterogeneity.
Sensitivity analysis
In the sensitivity analysis, the influence of each study on the pooled OR was examined by repeating the meta-analysis while omitting each study, one at a time. This procedure confirmed the stability of our overall results. In addition, when excluding the studies that were not in HWE, the results were persistent and robust (Table 2).
Publication bias
Funnel plot, Begg’s and Egger’s tests were performed to evaluate publication bias of the literature on PHDs. Figure 5 displayed a funnel plot that examined the ACE I/D polymorphism and overall PHD risk included in the meta-analysis in the homozygote comparison. The shape of the funnel plot did not reveal any evidence of funnel plot asymmetry. The statistical results still did not show publication bias except in the recessive model (DD vs. II: Begg’s test p = 0.13, Egger’s test p = 0.26; ID vs. II: Begg’s test p = 0.54, Egger’s test p = 0.87; dominant model: Begg’s test p = 0.64, Egger’s test p = 0.21; recessive model: Begg’s test p = 0.03, Egger’s test p = 0.003).

Begg’s funnel plot for publication bias test (DD vs II). Each point represents a separate study for the indicated association. LogOR, natural logarithm of OR; s.e., standard error; horizontal line, mean effect size.
Discussion
The angiotensin-converting enzyme (ACE), a peptidyl carboxypeptidase, is an important member of the RAS family that regulates blood pressure by catalysing the conversion of angiotensin I into the potent vasoconstrictor angiotensin II. 53 Its action causes vasoconstriction, and elevated ACE activity leads to hypertension.54,55 The ACE polymorphism is due to the insertion or deletion of an Alu 289 base pair (bp) sequence located at intron 16. A deletion polymorphism (D allele) has been reported to be associated with increased ACE activity. 11 Some investigators have previously reported an association between the D allele of ACE and an increased risk of pre-eclampsia or GH.23,26,37,47 Moreover, a previous study 56 suggested that the DD genotype of the ACE insertion/deletion (I/D) polymorphism and those of either endothelial constitutive nitric oxide synthase (NOS) 4b/a (aa) or angiotensin-II receptor 1 (AT1R) 1166A>C (CC) may pose a genetic risk factor for pre-eclampsia. Given the different ACE activities for the two polymorphic protein variants of the ACE gene, it is biologically plausible that the ACE I/D polymorphism could be associated with an increased PHD risk.
The present meta-analysis, including 3523 cases and 4817 controls from 30 case–control studies, explored the association between the I/D polymorphism of the ACE gene and PHD risk. To the best of our knowledge, this is the first meta-analysis of the comprehensive assessment for the relationship between ACE I/D polymorphism and the risk of PHDs (although previous meta-analyses assessed the association between ACE I/D polymorphism and pre-eclampsia risk). We found that individuals with the variant DD genotype were significantly associated with an increased PHD risk. In the subgroup analysis by ethnicity, an increased PHD risk was found among both Asians and Caucasians. Moreover, when stratifying by types of PHD, a significantly increased risk was observed for pre-eclampsia. Limiting the analysis to the studies within HWE, the results were persistent and robust. Although some potential biases could not be eliminated, these findings indicated that the ACE I/D polymorphism might play a role, although modest, in PHD development, and particularly in pre-eclampsia.
When further stratifying by country, a significantly elevated risk was found among ‘others’ countries (including India, Japan, Turkey, USA, UK, Italy, Poland, Brazil, Finland, South Africa, Greece, Colombia, Canada and Russia), but not among China or Korea. Although the reason for these discrepancies is not well known, some possibilities should be considered. On the one hand, it may be due to the differences in the underlying genetic backgrounds and/or environmental and social factors in different populations studied; on the other hand, other factors such as selection bias, significant heterogeneity due to the sample size and different matching criteria may also play a role – for example, cases and controls were matched by age, race, etc. in some studies, but not matched in other studies; even in studies with cases and controls matched, the matching criteria were not the same in different studies.
Our results showed that the DD genotype may increase risk of pre-eclampsia, which is consistent with a previous meta-analysis based on pre-eclampsia. 6 This is probably because most of the pre-eclampsia studies included in the present paper had already been used in the former meta-analysis. However, the ACE I/D polymorphism seems not to increase the risk of GH or eclampsia. One possible factor that would contribute to the discrepancy between different studies which include different types of PHD is that the polymorphism might play a different role in them. GH is defined as a systolic blood pressure of at least 140 mmHg and/or a diastolic blood pressure of at least 90 mmHg measured on at least two occasions at least 6 hours apart after the 20th week of gestation in women known to be normotensive before pregnancy and before 20 weeks’ gestation. Pre-eclampsia is primarily defined as GH plus proteinuria (300 mg or more per 24-hour period). The definition of eclampsia is secure in the presence of generalized edema, hypertension, proteinuria, and convulsions. All of them are characterized by maternal hypertension, but they have different, well-defined characteristics. The simultaneous presence of more than one risk factor could be necessary for leading to the pathology. Thus, the I/D polymorphism and PHD risk may be more relevant in pre-eclampsia patients because the I/D polymorphism needs to act together with further characteristics that cannot be present in other PHD types. A recent study performed by Amaral et al. 57 suggesting that inducible nitric oxide synthase genetic variants may affect the susceptibility to pre-eclampsia, but not to GH, supports our hypothesis. Also, even for the same types of PHD, considering the possible small effect size of the genetic polymorphism to disease and the relatively small sample size in some studies, the discrepancy will become apparent since some of these studies may have been underpowered to detect a small but real association. For GH and eclampsia, there are only four and two studies, respectively, included in the analysis with limited sample sizes; therefore, the results should be interpreted with caution.
It seemed that selection bias could have played a role, because the genotype distribution among control subjects disobeyed the law of HWE in three studies.44,46,52 It is widely believed that deviation from HWE may be due to genetic reasons including non-random mating, or the alleles reflect recent mutations that have not reached equilibrium, as well as methodological reasons including biased selection of subjects from the population or genotyping errors.58,59 Despite the reasons for disequilibrium, the results of genetic association studies might be spurious if the distribution of genotypes in the control groups were not in HWE.60,61
When stratifying for HWE in controls, a significantly increased risk of PHD was found among those studies with controls in HWE, suggesting that this factor probably had little effect on the overall estimates.
Obvious heterogeneity between studies was observed in overall comparisons and also some subgroup analyses, and then meta-regression analysis was used to explore sources of heterogeneity. We found that the study sample size contributed to potential heterogeneity in this meta-analysis. Moreover, the types of PHD could also be a potential factor contributing to between-study heterogeneity. Different types of PHD are pooled together in this meta-analysis, which is a potential source of large heterogeneity, even though the use of meta-regression analysis did not show it. Another important issue for any meta-analysis is publication bias due to selective publication of reports. In the current study, Begg’s funnel plot and Egger’s test were performed to evaluate this problem. Both the shape of funnel plots and statistical results did not show publication bias except for in the recessive model. It is worthy of mention that the results held when the sensitivity analysis was performed, which implied that the results were reliable.
Some limitations of this meta-analysis should be addressed. First, the total number of cases and controls seemed perfectly; however, the subjects for GH and eclampsia were too small to detect the potentially existence of a small genetic effect. Therefore, more studies with a larger sample size and providing more detail information are needed. Second, a significant publication bias was observed in the recessive model. It is possible that some unpublished studies, which more often provide evidence of negative or null effects, were not included in this analysis. This is because of studies with negative or null results would have been harder to publish than studies with positive results. Third, there was significant between-study heterogeneity in the sample numbers from studies of the ACE I/D polymorphism, and the genotype distribution also showed deviation from HWE in some studies.
In spite of these limitations, our meta-analysis also had advantages. First, a comprehensive searching strategy based on computer-assisted and manual searching allowed the eligible studies to be included as far as possible. Second, the quality of case–control studies included in the current meta-analysis was satisfactory and met our inclusion criterion. In addition, the method of this meta-analysis was well designed before initiation, by using explicit methods for study selection, data extraction, and data analysis.
Conclusions
In conclusion, this meta-analysis suggests that the ACE I/D polymorphism may contribute to genetic susceptibility for pre-eclampsia. Since limited studies were from Africans, African-Americans and Americans, it is critical that larger and well-designed multicentric studies based on Africans, Africans-Americans and Americans should be performed to re-evaluate the association. Moreover, further studies estimating the effect of gene–gene and gene–environment interactions may eventually provide a better, comprehensive understanding of the association between the ACE I/D polymorphism and PHD risk.
Footnotes
Acknowledgements
We would like to thank the anonymous reviewer and the editor for their constructive comments on revising this manuscript.
This work was supported by grants from the National Natural Science Foundation of China (No. 30901720) and PhD Programs Foundation of Ministry of Education of China (No 20090181120111).
We declare that there is no conflict of interest.