
Abstract
Background:
Endothelial progenitor cells (EPCs) are known to play a significant role in reendothelialization and vascular repair. Recently, a mineralocorticoid receptor was demonstrated to be expressed by EPCs. The study aimed to evaluate a potential influence of eplerenone treatment on the total number of EPCs in patients with chronic heart failure.
Methods:
Eighty-seven male patients with chronic heart failure were included (age: 23–83 years; body mass index 29.1 ± 5.1 kg/m2; New York Heart failure classification (NYHA) I: 29 patients, NYHA II: 32 patients, NYHA III: 26 patients). Numbers of circulating EPCs were quantified immediately using flow cytometry. Twenty-eight patients received therapy with eplerenone. Patients were further characterized by echocardiography, spirometry and laboratory markers.
Results:
Patients with ongoing eplerenone administration showed higher levels of circulating cells expressing CD34+ (p<0.05) and CD34+KDR+ (p<0.05) and CD34+CD133+KDR+ cells (p<0.05). The effects of eplerenone treatment could be shown to be independent of NYHA status, genesis of the underlying cardiovascular morbidity, left ventricular function and co-medication.
Conclusion:
Patients with chronic heart failure treated with eplerenone show higher numbers of EPCs. The clinical benefit for treatment with eplerenone has been demonstrated even for patients with mild heart failure and might be partially mediated by EPCs.
Introduction
Endothelial progenitor cells (EPCs) home to sites of ischaemia and vascular injury as a repair mechanism to damaged or impaired endothelium. They contribute to reendothelialization, neovascularization and normalization of endothelial function and restoration of blood flow at the site of vascular injury. 1 Furthermore, several studies have demonstrated that EPCs contribute to the improvement of myocardial neovascularization and function. 2 These processes are governed by a complex network of endogenous cytokines and are affected by exogenous agents such as medications. Not only an impaired function but also a reduced number of EPCs has been linked to endothelial dysfunction 3 as well as increased risk for atherosclerosis and cardiovascular morbidity and mortality. 4 Besides cytokines and medications EPCs are influenced by a number of factors: physical activity increases whereas cigarette smoking reduces the number and function of EPCs. There is for example an inverse relation between EPC number and the metabolic syndrome, 5 hypertension, 6 family history of coronary artery disease (CAD), 7 diabetes 8 and hypercholesterinaemia. 9
Recent findings from both experimental models and clinical studies indicated that the biology of EPCs is strongly related to the pathophysiology of heart failure (HF). Patients with HF irrespective of its aetiology have significantly reduced levels of circulating EPCs compared with healthy individuals. 10 Furthermore, the number of EPCs, as measured by the number of CD34+ mononuclear cells, was decreased in severe HF and increased in proportion to the amelioration of HF during hospitalization. 11 Nevertheless, other studies reported conflicting results regarding the levels of EPCs in patients with HF.12-14 This phenomenon can be partially explained by the lack of uniform criteria to precisely define the cellular characteristics of EPCs. However, pharmacological mobilization of EPCs and intracoronary infusion of circulating progenitor cells improved left ventricular remodelling and function in pilot studies on patients with post-infarction HF. 15
Different pharmacological and lifestyle interventions have been identified to increase number and function and decrease apoptosis of EPCs. 16 Experimental and clinical studies have revealed that the number of EPCs can be increased by substances such as hormones, statins, recombinant human erythropoietin, or drugs mediating angiotensin- converting enzyme (ACE) inhibition or angiotensin II receptor antagonism. 17 However, in patients with chronic heart failure only few substances have been investigated, although there is evidence that statins positively affect EPCs in patients with chronic HF. 18
Recently, Thum et al. demonstrated an expression of a mineralocorticoid receptor on EPCs. Treatment of human EPCs with aldosterone impaired function of EPCs, such as differentiation, migration and proliferation in vitro. 19 Impaired EPC function was rescued by pharmacological blockade or genetic ablation of the mineralocorticoid receptor (MR). In addition, EPCs from patients with primary hyperaldosteronism compared with controls of similar age displayed reduced migratory potential and endothelial dysfunction.
It is now well documented that the addition of the selective mineralocorticoid receptor antagonist eplerenone to standard evidence-based therapy reduces the risk of death and hospitalization in patients with different stages of HF. 20 Eplerenone mediates its effects by antagonizing the action of aldosterone at the MR. An elevated aldosterone level is documented in patients with HF, and conventional therapies, such as ACE inhibitors, angiotensin-receptor blockers and β-blockers, do not act on the MR. Since it has been documented that hyperaldosteronism is associated with a decrease in EPC numbers in rats 21 we hypothesized that eplerenone treatment is associated with increased EPC numbers in HF patients.
Materials and methods
Study subjects
The study was approved by the local ethical committee. Eighty-seven patients were enrolled into the study after giving their written informed consent. The study complies with the Declaration of Helsinki. All patients were recruited consecutively in our university referral outpatient clinics for patients with chronic HF. Patients were included irrespectively of their HF genesis. Medical history including cardiovascular risk factors, previous and present cardiovascular events, current drug treatment and vital signs was obtained from a personal interview. Patients with acute coronary syndromes within the last three months were excluded from the study. Furthermore, only patients with stable conditions were included in the study. This was defined by no history of decompensated HF within the last three months and no change of more than one New York Heart failure classification (NYHA) class in clinical presentation. In addition, no patients in NYHA class IV were included. Further exclusion criteria were clinical or biochemical evidence for the presence of a systemic inflammatory disease, terminal renal insufficiency (serum creatinine >250mmol/L), malignant diseases, thrombocytopenia (<100,000/μl) or anaemia (haemoglobin <10.0 g/dl). Diabetes was assessed determination of fasting blood glucose (>6.0 mmol/L) and/or by personal medical history and an elevation of HbA1c above 5.3%. Patients with spironolactone were excluded from this study. Only male patients were included in order to avoid sexual differences in mineralocorticoid metabolism.
Echocardiography
The echocardiograms (Philipps iE33, Philipps, Germany) were performed by cardiologists not related to this study and unaware of the blood testing results. Left ventricular ejection fraction (LV EF%) was derived using Simpson’s modified biplane method; left ventricular end-diastolic diameter (LVEDD) was measured in parasternal long axis.
Electrocardiogram and laboratory investigations
The recording of the electrocardiogram and the determination of blood lipids, creatinine and red blood cell count, as well as brain natriuretic peptide (BNP), were done according to internal and international standards.
Circulating EPC number
A venous blood sample (10ml) was obtained in EDTA tubes for enumeration of EPCs. Different subpopulations were identified by using the haematopoietic progenitor cell marker CD34, the immature haematopoietic progenitor cell marker CD133 and the endothelial cell receptor VEGFR2 (vascular endothelial growth factor receptor-2, also known as kinase domain receptor, KDR), as described previously.22,23 Briefly, peripheral blood mononuclear cells (PBMCs) were incubated with allophycocyanin (APC)-conjugated anti-human CD34 monoclonal antibody (mAb) (BD Biosciences), phycoerythrin (PE)-conjugated anti-human CD133 mAb (Milteny Biotec) and fluoresceinisothiocyanate-conjugated monoclonal anti-VEGFR2 (R&D Systems) for 60 min at +4°C. Control isotype immunoglobulin antibodies were obtained from Becton Dickinson. The cytometer (FACScalibur, BD Biosciences, Franklin Lakes, NJ, USA) acquired at least 5 × 106 events. The frequency of peripheral blood cells positive for these reagents was determined by a two-dimensional side-scatter fluorescence dot-plot analysis of the samples, after appropriate gating. Data were processed using the Summit software program (BD CellQuest Pro, Version 5.2.1).
Statistical analyses
All data are expressed as mean ± standard deviation (SD). Continuous variables were tested for normal distribution with the Kolmogorov–Smirnov test. Non-normally distributed continuous variables groups were compared by the Mann–Whitney U test, while others were analysed by t test (two-sided, including Levene’s test for equality of variances). Bivariate correlation (Spearman’s rank correlation coefficient) was used to correlate circulating EPC counts with risk factors or drug treatment. Statistical significance was assumed if a null hypothesis could be rejected at p≤0.05. All statistical analyses were performed with IBM SPSS statistics, version 19.0 (IBM Inc.).
Results
The baseline characteristics of the 87 subjects are summarized in Table 1. Patients were divided into two groups according to their current eplerenone treatment status. The two groups were well matched for age, anthropometric indices, comorbidities and co-medication. Furthermore, there was no significant difference in the genesis of HF and in echocardiographic and laboratory findings (Table 2). Furthermore, there was no significant difference in exercise capacity as measured in the maximally achieved power stage (124 ± 46 Watt versus 125 ± 55 Watt, p=0.94), nor in maximum oxygen uptake (19.3 ± 5.0 ml/kg per min versus 21.4 ± 6.1 ml/kg per min, p=0.36).
Baseline characteristics of the study population. Patients were grouped according to their ongoing therapy with eplerenone.

BMI: body mass index; ACE: angiotensin-converting enzyme; n.s.: not significant
Characteristics of the study population regarding their heart failure, echocardiographic results, exercise capacity and laboratory values.
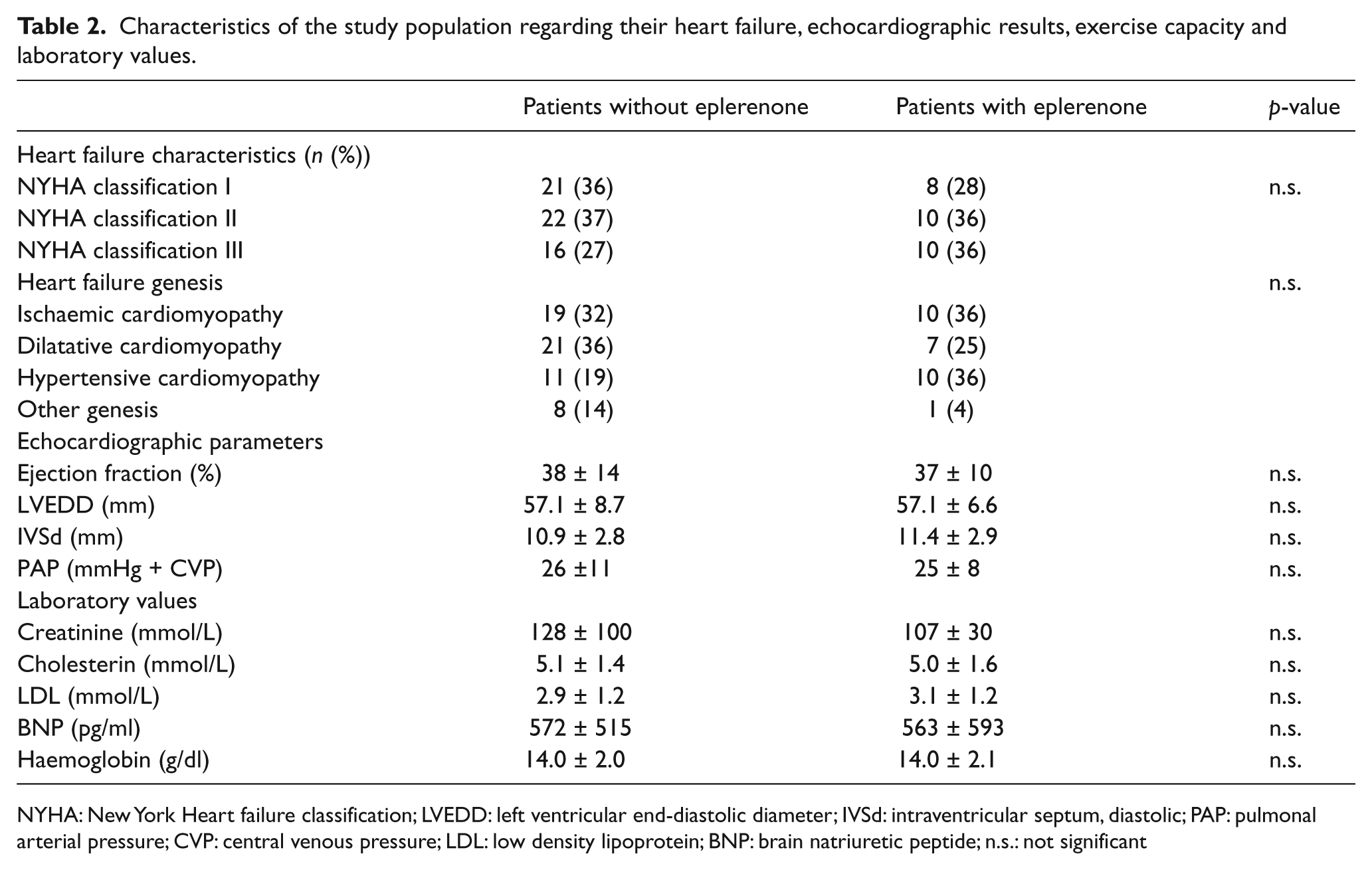
NYHA: New York Heart failure classification; LVEDD: left ventricular end-diastolic diameter; IVSd: intraventricular septum, diastolic; PAP: pulmonal arterial pressure; CVP: central venous pressure; LDL: low density lipoprotein; BNP: brain natriuretic peptide; n.s.: not significant
Comparing the different EPC subpopulations there were significant differences between patients treated with eplerenone for CD34+ (p=0.013, Figure 1), CD34+CD133+ (p=0.045), as well as CD34+CD133+KDR+ (p=0.019).

Endothelial progenitor cell subpopulations detected in patients with chronic heart failure divided according to their current eplerenone treatment status. Shown are CD34+ (upper left), CD34+CD133+ (upper right), CD34+KDR+ (lower left) and CD34+CD133+KDR+ (lower right) subpopulations.
If the cohort was split according to the NYHA classification and the comparisons made regarding eplerenone treatment, significant differences could be observed in the NYHA I group for CD34+ (p=0.027), CD34+CD133+ (p=0.030), CD34 +KDR+ (p=0.011) cells. There were no significant differences in the NYHA II group. In addition, CD34+CD133+KDR+ differed in the NYHA III group (p=0.026). However, there was no difference regarding the different EPC subpopulations if the patients were grouped for their HF aetiology.
There was no further influence on EPCs if coronary artery disease was present. Furthermore, there was no difference between patients with and without diabetes. In addition no association to the smoking status and the use of other medications, including statins and ACE-inhibitors, could be detected. However, patients overweight as defined by a body mass index (BMI) >30kg/m2 had higher CD34+ (p=0.044) and higher CD34+CD133+ cell counts (p=0.002).
There were no significant correlations between laboratory findings and exercise capacity in the whole cohort. However, analysing the cohort separated according to HF aetiology, there is in patients with ischaemic cardiomyopathy a strong association between CD34+ cells and exercise capacity (p=0.039, R2: 0.576) and a negative correlation to BNP values (p=0.033, R2: −0.435). Such associations could not be detected in the other aetiology cohorts.
Discussion
The main finding of the present observational study is a positive effect of eplerenone treatment on the number of EPCs in patients with congestive heart failure (CHF). The benefit of eplerenone treatment on hard clinical endpoints has been extensively demonstrated. The protective mechanisms are poorly understood, but it has been hypothesized that an activation of the MR by both aldosterone and cortisol plays an important role in the pathophysiology of HF and MRs are overexpressed in the failing heart. 24 Activation of the MR has been shown to promote cardiac fibrosis in experimental models, and in patients with HF, as well as in patients after myocardial infarction, the use of MR antagonists decreases extracellular-matrix turnover, as assessed by measuring serum levels of collagen biomarkers. 25 Thus, a so-called reverse tissue remodelling with a resulting improvement of cardiac function might be initiated.
Experimental and clinical studies suggest that MR antagonists favourably affect several other important mechanisms known to have a role in the progression of HF. 20
However, no human study has investigated the effects on EPCs, a cell population that has been associated with endothelial regeneration and improved cardiovascular outcome. In vitro studies revealed an expression of a MR on EPCs and impaired EPC function following aldosterone treatment. In addition, impaired EPC function could be restored by pharmacological blockade or genetic ablation of the MR. Kobayashi et al. found a positive effect of eplerenone treatment on EPC in an animal model of hindlimb ischaemia. 26 Therefore, the current study adds to the body of knowledge that this effect has clinical relevance and that an increased number of EPCs might functionally contribute to the positive effect of eplerenone treatment in patients with CHF. The prognostic impact of EPC levels has been confirmed in a large study in patients with CHF, in which they were demonstrated to be the most important determinant of prognosis with advanced age and diabetes mellitus at a Cox proportional regression analysis. 27 However, the relation between HF and EPC levels is complex and the existing data are conflicting. It has been demonstrated that functional NYHA class is related to different levels of CD34+ cells. 12 Indeed, compared with healthy control subjects, patients in the lower functional classes (NYHA I and II) had higher levels of CD34+ cells, which, in contrast, were significantly lower in NYHA III and IV patients. These lower levels of EPCs were interpreted to be related to the higher serum levels of tumour necrosis factor alpha (TNFa), a known myelosuppressive cytokine. In contrast, in a large study in patients with ischaemic or non-ischaemic HF, Michowitz et al. found a mild direct correlation between number of e-CFUs and NYHA class. 27 Recently, novel evidence has been provided in patients with post-ischaemic HF indicating a selective functional exhaustion of the EPCs. Interestingly, bone marrow niches as well as the colony-forming capacity seemed to be reduced, whereas bone marrow haematopoietic progenitor cell number was preserved. 10 One possible explanation could be the relation between a reduction in the bio-availability of nitric oxide (NO) in the bone marrow niches since NO has a pivotal role in modulating the activity of MMP-9 that is required for the mobilization of EPCs but also for the transfer of endothelial cells to a proliferative niche. Another explanation for conflicting results is the lack of a uniform EPC definition in different studies in the literature.
Several positive observations regarding a pharmaceutical modification of EPCs have been made. Especially, statins have been extensively tested and randomized trials exist confirming a positive effect in number and function in these cells among different patient populations, including patients with HF. 28 Furthermore, ACE inhibitors and angiotensin II receptor blockers and oestrogen are understood to positively influence EPCs. Tousoulis et al. recently tested rosuvastatin and allopurinol treatment in patients with CHF and demonstrated a positive effect of rosuvastatin treatment, indicating that the treatment effect is independent of changes in inflammatory and oxidative status. 29 In the current study no associations were detected to co-medications although different treatment regimes and dosages were used. Of interest is the positive association between EPCs and overweight, which has been described in adults without HF already. 30 However, treatment effects on EPCs are thought to modulate the recruitment out of the bone marrow, apoptosis and functional capacity of these cells. As summarized above, survival and functional improvement of EPCs by blocking MR has been shown in-vitro already.
Our study has several limitations. First of all, the sample size is limited. Second, it is an observational study without randomization or adjustment to patient characteristics before initiation of eplerenone treatment. Therefore, we understand the current study as hypothesis generating suggesting a randomized placebo-controlled trial. However, our patient population is well characterized and represents a real-life scenario in an academic referral centre for CHF.
In conclusion, eplerenone treatment positively affects EPC numbers in patients with CHF, an effect that has been already described by in-vitro studies. The demonstrated benefit of eplerenone treatment might be mediated by this effect. Further studies are warranted to confirm these findings and to elucidate the exact underlying mechanisms.
Footnotes
Acknowledgements
We thank Annett Schmidt for excellent technical assistance.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None.