
Abstract
Patients with type 2 diabetes (T2D) are at high risk of developing hypertension and related cardiovascular disease. The renin-angiotensin system (RAS) plays a central role in regulation of blood pressure (BP). Accordingly, each component of this system represents a potential candidate in the etiology of hypertension. This study investigated the impact of polymorphisms within the RAS on ambulatory and central BP in T2D subjects. A cohort of 761 subjects (55–65 years) with T2D was studied. Ambulatory and central BP were measured, and ACE I/D genotype, angiotensinogen M235T, renin rs6693954 and ATR1-A1166C polymorphisms were analyzed. Women carrying the AA-genotype had lower 24-hour and day-time systolic and diastolic BP (p<0.05), and lower night-time and central diastolic BP (p<0.05), compared to T allele carriers. In men, the AA-genotype was instead associated with higher central diastolic BP (p=0.018) and higher augmentation index (p=0.016). Further, the associations between the renin rs6693954 SNP and diastolic BP were strongly gender dependent (p≤0.001). In T2D patients, there is a gender-dependent association of the renin rs6693954 SNP with central and ambulatory BP. Women carrying the renin rs6693954 AA-genotype may be protected against the higher BP seen in men with the same genotype.
Introduction
Patients with type 2 diabetes (T2D) are at high risk of developing hypertension and related cardiovascular disease (CVD). In clinical routine, blood pressure (BP) measurements are usually performed at the brachial artery using an auscultatory technique. However, measurement of ambulatory BP gives additional information regarding the patient’s total cardiovascular risk 1 and is more accurately related to microvascular 2 and macrovascular 3 complications compared to traditional office BP measurements. In addition, recent evidence has shown that BP measured in central arteries (e.g. in the aorta) more strongly relates to cardiovascular outcome, than the peripheral BP. 4
It is well known that the renin-angiotensin system (RAS) plays a central role in salt and water homeostasis and maintenance of vascular tone. Consequently, each component of this system represents a potential candidate in the etiology of hypertension. Recent studies have also suggested a role of RAS in the pathogenesis of T2D, as angiotensin-converting enzyme (ACE) inhibitors have been shown to protect against new onset of T2D. 5 These findings emphasize the need for studies elucidating the connection between RAS, T2D and cardiovascular risk.
The inactive peptide angiotensinogen is released from the liver and converted to angiotensin I (Ang I) by renin, which traditionally represents the rate-limiting step in RAS. Ang I is further converted to the vasoactive peptide angiotensin II (Ang II) by ACE. Ang II acts on the Ang II receptor type 1 (ATR1), which is widely distributed within the cardiovascular system. 6 The genetic regions encoding the components of RAS are highly polymorphic, and several RAS gene polymorphisms have previously been associated with CVD. 7 However, most previous studies investigating the association between RAS gene polymorphisms and hypertension have studied non-diabetic patients and have been limited to traditional office BP recordings. The present study aimed to investigate the impact of RAS polymorphisms (angiotensinogen M235T, renin rs6693954, ACE insertion/deletion (I/D) and ATR1 A1166C) on ambulatory BP and central hemodynamics in subjects with T2D. As each component in RAS is central for regulation of cardiovascular homeostasis, we hypothesized that genetic polymorphisms within this system may affect BP.
Methods
Study population
The study population consisted of 761 T2D subjects (498 men and 263 women) aged 55–65 years included in the Cardiovascular Risk Factors in Patients with Diabetes – a Prospective Study in Primary care (CARDIPP).8,9 Subjects were recruited from 22 healthcare centers in the counties of Östergötland and Jönköping, Sweden, from 2005 to 2008. The healthcare centers are located in different demographic areas and differ in size. However, the management and care of type 2 diabetes was organized similarly and followed the same national guidelines for diabetes care. All clinical data were collected during an extended yearly examination of the patients. The participants were asked about medical history and on-going medical treatment. Diabetes duration was defined as the time from diagnosis until the time for the examination.
Blood sampling and laboratory analyses
Blood samples were drawn at the local healthcare centers following overnight fasting. Glycated hemoglobin (HbA1c) and creatinine were analyzed according to general primary healthcare routines. HbA1c was calculated according to the Swedish Mono-S HPLC standard, which is approximately 1% below the Diabetes and Control Complications Trial (DCCT) standard. Levels of apolipoprotein A-1 (ApoA1) and apolipoprotein B (ApoB) were analyzed in plasma by immunoturbidimetric assays (Bayer HealthCare and Siemens Diagnostics Medical Solutions, Tokyo, Japan). The ApoA1/ApoB ratio was used as this is considered a better estimate of cardiovascular risk compared to conventional lipids. 10 Glomerular filtration rate (GFR) was calculated according to the Cockcroft-Gault equation.
Genotyping
Genomic DNA was isolated from peripheral blood using automated Maxwell® 16 DNA isolation kit (Promega, Madison, WI, USA), following the manufacturer’s instructions.
The ACE I/D polymorphism was determined as previously described. 11 In brief, DNA was amplified with polymerase chain reaction (PCR) using three primers: 5'-CTGCAGGTGTCTGCAGCATGTGGC-3', 5'-GATTACAGGCGTGATACAGTCACTTTT-3' and 5'-GCCATCACATTCGTCAGATCTGGTAG-3' (Invitrogen, Paisley, UK). Each primer was used at a concentration of 0.4 µM. DNA amplification started with an initial denaturation at 94°C for 5 five minutes (min) followed by 30 cycles of the following thermal profile: 94°C for 45 seconds (sec), 65°C for 45 sec and 72°C for 45 sec, followed by a final extension at 72°C for five minutes (min). Amplified DNA was separated by gel electrophoresis using a 1.5% agarose gel stained with ethidium bromide and visualized by ultraviolet (UV) light. The determination of ACE genotype was based on length and number of DNA fragments.
The ATR1 A1166C single nucleotide polymorphism (SNP), the angiotensinogen M235T SNP, and the renin rs6693954 SNP were analyzed using Taqman® SNP genotyping assay (Applied Biosystems, Foster City, CA, USA) and the 7900HT Fast Real-Time PCR system (Applied Biosystems), according to the manufacturers’ protocols. A sample volume of 20 µl was used. All SNPs were amplified with an initial denaturation at 95°C for 10 min, followed by 40 cycles of 92°C for 15 sec and 60°C for 1 min.
Clinical evaluations
Ambulatory BP measurement devices (Spacelab 90217, Spacelabs, Redmond, WA, USA) were used to measure the brachial BP every 20 min for 24 hours (h). Night-time BP was defined as the time between when the patient went to bed until the patient got out of bed the following morning. Central aortic BP was estimated from recordings of the radial pressure waveforms using a Millar pressure tonometer and the SphygmoCor CvMS system (version 7.0, model MM3, AtCor Medical, Sydney, Australia). The SphygmoCor system uses a validated generalized transfer function 12 to calculate aortic pressure waveforms from 11-sec recordings of the radial pressure waveforms, and enables estimations of central aortic BP and aortic augmentation. 13 Brachial BP, determined using an oscillometric technique (Dinamap model PRO 200 Monitor, Critikon, Tampa, FL, USA), was used for calibration. Pulse pressure amplification was calculated as the ratio between the brachial and central aortic pulse pressure. Augmentation pressure represents the pressure boost caused by wave reflection, while augmentation index (AIx) is the augmentation pressure expressed as a percentage of the aortic pulse pressure. Carotid-femoral pulse wave velocity (PWV) was calculated as the aortic pulse wave transit time, determined by electrocardiograph (ECG)-gated recordings of the carotid and the femoral pulse waves, divided by the distance between the measure sites at the suprasternal notch and the carotid and femoral arteries, respectively. Mean values of two consecutive recordings were used for statistical analysis. Only recordings with a quality index >74% were included.
Intima media thickness (IMT) of the carotid arteries were determined by B-mode ultrasound, using a digital ultrasound system (HDI 5000, ALT, Bothell, WA, USA) equipped with a broadband linear transducer (L12-5), as previously described. 8 Mean values of IMT from both the left and the right carotid arteries were used. Measurement of central hemodynamics and IMT of the carotid arteries were performed at the Department of Physiology, Linköping University Hospital and at County Hospital Ryhov, Jönköping, at different times throughout the day. All measurements were carried out by experienced technicians after at least 10 min of rest. Subjects refrained from smoking and alcohol for at least four hours prior to the examinations. There were no restrictions regarding food intake, and no changes in the patients’ daily intake of medications were made.
Statistics
The data are presented as mean values ± SD or number of subjects (%). Pearson’s χ2 test was used to analyze discrete variables and to evaluate whether genotypes were in accordance with the Hardy-Weinberg (HW) equilibrium. Student’s t tests or one-way analysis of variance (ANOVA) were used to compare continuous data between groups. Adjustments for potentially confounding factors were made using general linear models. Adjustments were made for HbA1c, ApoB/ApoA1 ratio, body mass index (BMI) and gender (model 1), with additional adjustments for age, diabetes duration and smoking in model 2. For AIx, adjustment for heart rate and height were also included. To address whether associations were gender dependent, a gender-genotype interaction was included in the adjusted model. Data were analyzed in the entire study population, in men and women separately, in three genotype models as well as in recessive and dominant models of inheritance. Two-tailed p values <0.05 were considered statistically significant. Statistical analyses were carried out using SPSS 17.0 for Windows (SPSS Inc, Chicago, IL, USA).
Ethics
Written informed consent was obtained from all participants. The study was approved by the Regional Ethical Review Board in Linköping, Sweden and was conducted in accordance with the principles stated in the Declaration of Helsinki 1975, revised Hong Kong 1989.
Results
The mean age of the study population was 60.7 ± 3.1 years and mean diabetes duration was 7.3 ± 6.2 years. Two-hundred and fourteen subjects (28%) used only diet and exercise as anti-diabetic treatment. The remaining subjects were treated with oral agents (n=308, 41%), or insulin alone or in combination with oral agents (n=238, 31%). A total of 493 subjects (68%) were treated with BP-lowering drugs (ACE inhibitors, angiotensin-receptor blockers, beta-receptor blockers, calcium channel blockers or diuretics) and 414 subjects (54%) were treated with statins. There was no significant difference in the number of BP-lowering drugs between genotypes for all of the studied polymorphisms, either in men or women. Genotyping was successful in 724 subjects (95%) for the ACE I/D polymorphism, 706 (93%) for the angiotensinogen M235Thr polymorphism, 715 (94%) for the ATR1 A1166C SNP and 719 (94%) for the renin rs6693954 SNP. Genotype distributions of all studied polymorphisms were in accordance with the Hardy-Weinberg equilibrium.
Association between the renin rs6693954 SNP and hemodynamics
The genotype distribution for the renin rs6693954 polymorphism was TT 60%, AT 36%, AA 4% (HW p=0.37). Hemodynamic characteristics according to the renin rs6693954 SNP in women and men are shown in Tables 1 and 2, respectively. In men as well as women, there were significant associations between the renin rs6693954 SNP and BP. Specifically, women carrying the AA genotype had lower 24-h systolic and diastolic BP, lower day-time systolic and diastolic BP and lower night-time diastolic BP, compared to carriers of the T allele. These associations remained after adjustment for potentially confounding factors. In addition, women carrying the renin rs6693954 AA genotype had lower central diastolic BP compared to carriers of the T allele (TT 73 ± 8, AT 70 ± 8, AA 64 ± 11 mmHg, p=0.013). This association was significant after adjustment for HbA1c, ApoB/ApoA1 ratio and BMI (p=0.019), while a tendency was seen (p=0.059) after additional adjustment for age, diabetes duration and smoking. Lower BP among female AA carriers was also seen in recessive models of inheritance (AA vs AT/TT) (data not shown). In addition, AIx and carotid IMT was lower among women carrying the AA genotype, but the difference was not statistically significant.
Characteristics according to the renin rs6693954 SNP in women.

Values are mean ± SD, or number of subjects (%). Genotypes are in accordance with the Hardy Weinberg equilibrium. aAdjusted for HbA1c, ApoB/ApoA1 ratio and BMI. bAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, age, diabetes duration and smoking. cAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, height, heart rate. dAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, age, diabetes duration and smoking, height, heart rate. ep < 0.05, TT compared with AA, determined by Bonferronis’ post-hoc test. fp < 0.05, TA compared with AA, determined by Bonferronis’ post-hoc test. p values < 0.05 are indicated in bold.
SNP: single nucleotide polymorphism; BMI: body mass index; HbA1c: glycated hemoglobin; GFR: glomerular filtration rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; AIx: augmentation index; PWV: pulse wave velocity; IMT: intima-media thickness; ACEi: angiotensin-converting enzyme inhibitors; ARBs: angiotensin II receptor blockers.
Characteristics according to the renin rs6693954 SNP in men.
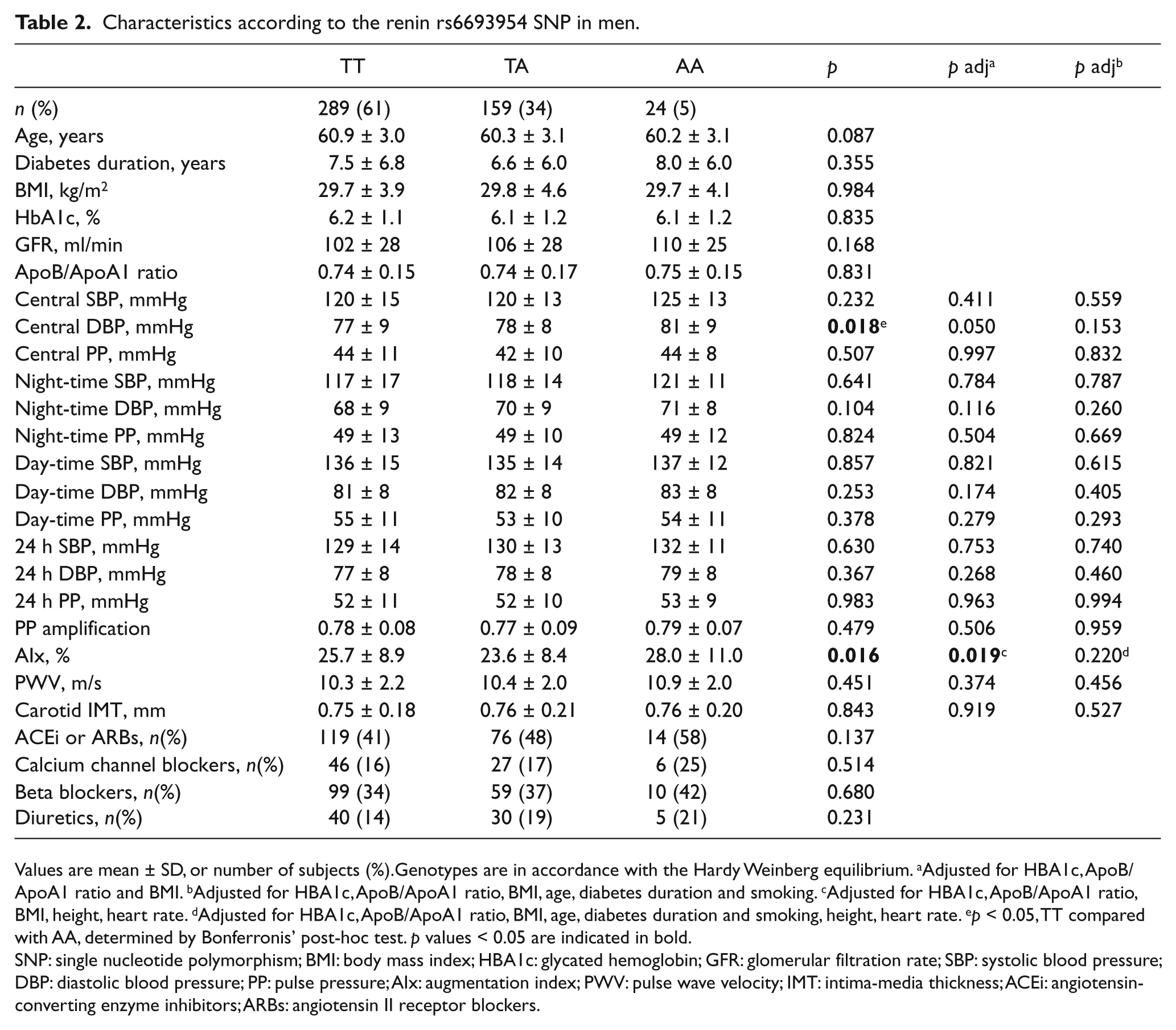
Values are mean ± SD, or number of subjects (%).Genotypes are in accordance with the Hardy Weinberg equilibrium. aAdjusted for HbA1c, ApoB/ApoA1 ratio and BMI. bAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, age, diabetes duration and smoking. cAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, height, heart rate. dAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, age, diabetes duration and smoking, height, heart rate. ep < 0.05, TT compared with AA, determined by Bonferronis’ post-hoc test. p values < 0.05 are indicated in bold.
SNP: single nucleotide polymorphism; BMI: body mass index; HbA1c: glycated hemoglobin; GFR: glomerular filtration rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; AIx: augmentation index; PWV: pulse wave velocity; IMT: intima-media thickness; ACEi: angiotensin-converting enzyme inhibitors; ARBs: angiotensin II receptor blockers.
In men, a significant association was seen between the renin rs6693954 SNP and central diastolic BP, but in contrast to women, male AA carriers were the ones with the highest BP. This association was significant in the three-genotype model (Table 2) as well as in a recessive (AA vs. AT/TT) and a dominant (AA/AT vs. TT) model of inheritance (data not shown). The renin rs6693954 SNP was also associated with AIx in men, carriers of the AA genotype having the highest values. The association between the renin rs6693954 SNP and AIx as well as central diastolic BP did not remain statistically significant in the fully adjusted model. There was no significant difference in the number of BP-lowering drugs between genotypes either in men or women. Furthermore, the associations between the renin rs6693954 SNP and diastolic BP were strongly gender dependent, as indicated by significant gender-genotype interactions (p<0.001 for night-time, day-time and 24-h diastolic BP, p=0.001 for central diastolic BP, Table 3).
Renin rs6693954 SNP, gender-genotype interaction.
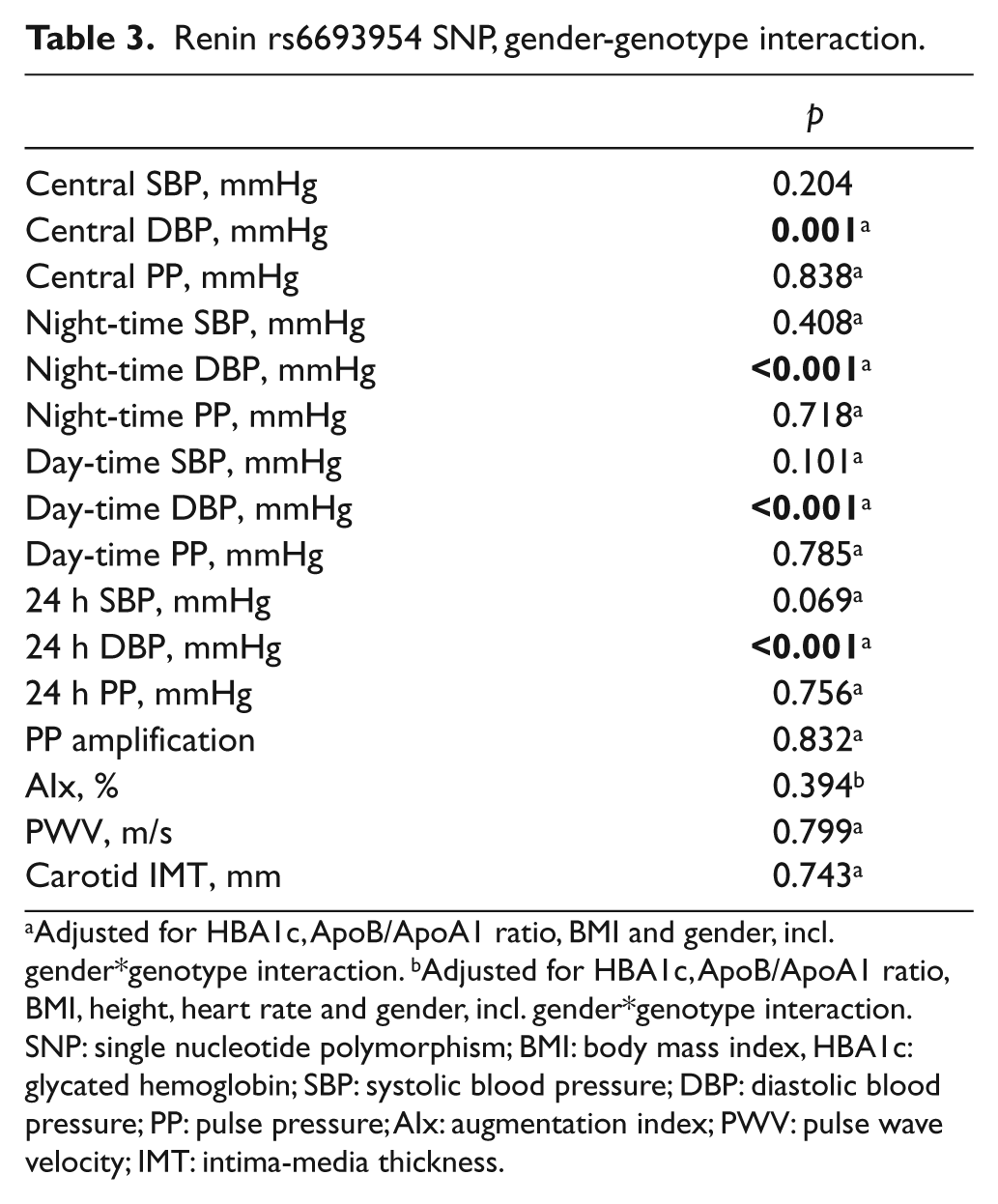
Adjusted for HbA1c, ApoB/ApoA1 ratio, BMI and gender, incl. gender*genotype interaction. bAdjusted for HbA1c, ApoB/ApoA1 ratio, BMI, height, heart rate and gender, incl. gender*genotype interaction.
SNP: single nucleotide polymorphism; BMI: body mass index, HbA1c: glycated hemoglobin; SBP: systolic blood pressure; DBP: diastolic blood pressure; PP: pulse pressure; AIx: augmentation index; PWV: pulse wave velocity; IMT: intima-media thickness.
Association between the ACE I/D polymorphism and hemodynamics
The genotype distribution for the renin ACE I/D polymorphism was II 23%, ID 49% and DD 27% (HW p=0.80). Among men, the ACE I/D polymorphism was associated with PWV, II carriers having the highest PWV. This association was significant in the three-genotype model (II 10.8 ± 2.4, ID 10.3 ± 2.1, DD 10.2 ± 2.0 m/s, adjusted p=0.010), as well as in the recessive model of inheritance (II 10.8 ± 2.4 vs. ID/DD 10.2 ± 2.0 m/s, adjusted p=0.003). In addition, in the recessive model of inheritance (II vs. ID/DD), men carrying the II genotype had higher central systolic BP than carriers of the D allele (II 123 ± 15 vs. ID/DD 120 ± 14 mmHg, p=0.043). This association did not, however, remain after adjustment for potentially confounding factors.
Association between the angiotensinogen M235T polymorphism and hemodynamics
The genotype distribution for the angiotensinogen M235T polymorphism was MM 36%, MT 47% and TT 17% (HW p=0.46). Male carriers of the M235T M allele had higher central systolic and diastolic BP compared to men carrying the TT genotype (systolic BP: MM/MT 121 ± 15 vs. TT 117 ± 14 mmHg, p=0.044, diastolic BP: MM/MT 78 ± 9 vs. TT 75 ± 8 mmHg, p=0.027). However, this difference did not remain after adjustment for potentially confounding factors. No association between the angiotensinogen M235T SNP and hemodynamics was seen in women.
Association between the ATR1 A1166C SNP and hemodynamics
The genotype distribution for the ATR1 A1166C SNP was AA 53%, AC 39% and CC 8% (HW p=0.71). No significant associations between the ATR1 A1166C polymorphism were found in the entire population, in men and women separately, in the three-genotype model, or in recessive or dominant models of inheritance.
Discussion
The present study was conducted to investigate the impact of RAS gene polymorphisms on ambulatory BP and central hemodynamics in a population of middle-aged T2D patients. We show, for the first time, a gender-dependent association of the renin rs6693954 SNP with central and ambulatory BP in patients with T2D.
As the rate-limiting step in RAS, renin plays a central role in regulation of BP. Alterations in renin activity have been associated with BP 14 and responsiveness to antihypertensive treatment. 15 Previous data have indicated that the expression of renin is under genetic control; 16 however, the exact identity of such polymorphisms is unknown. Although our study was limited to a low number of AA carriers, we showed, for the first time, an association between the renin rs6693954 SNP and BP in diabetic men and women. Women carrying the renin rs6693954 AA genotype had lower central, night-time, day-time and 24-h BP than carriers of the T allele. Among men, on the other hand, the AA carriers had slightly higher central diastolic BP as well as higher AIx, compared to T allele carriers. One previous study in non-diabetic subjects has reported that the renin rs6693954 A allele is associated with a higher risk for hypertension, 17 which is in line with our findings in male diabetic patients. The same study also reported an association of the haplotype containing the renin rs6693954 A allele with plasma renin levels and vascular response to ang II. 17 The molecular mechanism underlying the association between the renin rs6693954 polymorphism and BP is unknown; however, high linkage disequilibrium with another hypertension-related polymorphism within the renin gene (rs2368564) has been reported.17,18 The latter polymorphism has also been suggested to affect the expression of renin. 19
In addition, our study showed that the association between the renin rs6693954 SNP and diastolic BP was strongly gender-dependent. No gender analysis was performed in the previous study; however, the study population included more men than women (61% of the hypertensive subjects were men). 17 Gender has previously been reported to affect plasma renin levels; postmenopausal women have lower plasma renin levels than men of corresponding age, and it decreases further with estrogen.20,21 Thus, women carrying the renin rs6693954 AA genotype may be protected against the increase in BP seen in men with the same genotype, as a consequence of lower renin levels.
While renin is responsible for the formation of ang I, the subsequent conversion of ang I to the vasoactive peptide ang II is catalyzed by ACE. The ACE gene contains a common I/D polymorphism (ACE I/D) that is strongly linked to circulating levels of ACE, explaining 10–50% of the variation in ACE activity in general populations.22,23 The ACE I/D polymorphism is probably one of the most frequently studied candidate genes in CVD, and has been associated with a wide range of cardiovascular complications. 24 The present study showed an association between the ACE I/D polymorphism and aortic stiffness among T2D men, II carriers having higher carotid-femoral PWV than D allele carriers. In addition, male carriers of the II genotype had higher central systolic BP, which may be a result of an increased arterial stiffness. Higher aortic PWV in II carriers has previously been reported in T2D, 25 hypertensives 26 and healthy subjects; 27 however, those studies did not consider the gender aspect. The fact that the II genotype repeatedly has been associated with increased PWV is rather surprising as the DD genotype, rather than II, has been linked to increased risk for CVD. 24 However, when measured locally, higher abdominal aortic 28 and carotid stiffness 29 has been reported in DD carriers. Thus, it seems as genetic determinants may have different outcomes in different arterial regions, and that different methods may reflect different aspects of vascular function.
Besides changes in the enzymatic activity of RAS, alterations in the circulating level of angiotensinogen have also been recognized as a determinant of systemic BP. 30 The angiotensinogen gene contains a functional substitution polymorphism encoding a threonine instead of a methionine (M235T). As this polymorphism is known to affect plasma angiotensinogen levels, 31 it is not surprising that the polymorphism also has been associated with BP. 32 In our diabetic population, the angiotensinogen M variant was associated with higher central systolic and diastolic BP among men; however, after adjustment for confounders, no difference remained. In most previous studies, the T variant rather than M has been associated with higher BP.32,33
The final step in RAS consists of the binding of Ang II to its receptor Ang II receptor type 1 (ATR1), which is widely distributed within the cardiovascular system. The ATR1 gene contains a A→C transversion polymorphism (ATR1 A1166C) located within the binding site of a regulatory microRNA, 34 leading to downregulation of the ATR1 protein in the presence of the A but not the C allele. 34 The CC genotype of the ATR1 A1166C SNP has previously been associated with hypertension 35 and increased arterial stiffness. 26 To our knowledge, our study is the first to report data regarding the impact of the ATR1 A1166C SNP on ambulatory and central BP in diabetic patients. Although no effect of the ATR1 A1166C SNP on BP was seen in our study, this polymorphism may affect BP in non-diabetic subjects, as previously suggested, 35 but may be concealed by other, more important regulators in diabetic patients, related to vascular alterations induced by dysglycemia.
In summary, the present study investigated the impact of RAS gene polymorphisms on ambulatory BP and central hemodynamics in a population of middle-aged T2D patients. We show, for the first time, a gender-dependent association of the renin rs6693954 SNP with central and ambulatory BP in patients with T2D. Women carrying the renin rs6693954 AA genotype may be protected against the development of higher BP seen in men with the same genotype.
Footnotes
Conflict of interest
None declared.
Funding
This work was supported by the Medical Research Council of Southeast Sweden (FORSS-12478, FORSS-88091); the Swedish Heart Lung Foundation (20110571); County Council of Östergötland, Sweden (LIO-28471) and Lars Hierta Memorial Foundation, Sweden (FO2009-0696).