
Abstract
Introduction
To further clarify the association between angiotensin receptor blocker therapy and post-stroke seizures, we analysed a database of patients with acute stroke.
Methods
This single-centre, retrospective observational study included patients with acute stroke admitted to our hospital between 1 January 2019 and 31 December 2023. Patients were allocated into two groups based on whether they received angiotensin receptor blocker therapy. The primary outcome was the incidence of any seizure in the two groups. Predictors of seizure occurrence were assessed in univariable and multivariable logistic regression models.
Results
A total of 2589 patients were enrolled; the mean age was 72 years (SD 13.2), and the majority were female (n = 1306, 50.4%). The median follow-up duration was 18 months (IQR 3–31). A total of 243 patients experienced at least one seizure, including acute symptomatic seizures only (n = 101), post-stroke epilepsy (n = 92), or both (n = 50). The differences in seizure incidence were significant across all three groups (P < 0.05), and angiotensin receptor blocker therapy remained a significant factor in the multivariable logistic regression model (P < 0.001).
Conclusions
Based on our results, angiotensin receptor blocker therapy is independently associated with a lower incidence of both acute symptomatic seizures and post-stroke epilepsy.
Keywords
Introduction
Hypertension and epilepsy have increasingly been recognised as interrelated neurological conditions. Epidemiological evidence consistently demonstrates a higher prevalence of epilepsy among individuals with hypertension compared with normotensive populations. 1 Acute elevations in blood pressure can precipitate epileptic seizures through the development of vasogenic oedema, as seen exemplified by posterior reversible encephalopathy syndrome. 2 In contrast, chronic hypertension may contribute to epileptogenesis via two principal pathways: hypertension-related structural brain injury, including small-vessel disease and post-stroke gliotic scarring, and dysregulation of the renin-angiotensin system (RAS). 3
An extensive body of preclinical and clinical research supports a bidirectional interaction between RAS and epileptogenesis. Hyperactivation of RAS and upregulation of the angiotensin II type 1 receptor (AT1R) have been documented in cortical tissue across several experimental and human epileptic conditions.4,5 Conversely, activation of RAS and AT1R promotes oxidative stress and neurotoxicity, which may enhance neuronal excitability and consequently lead to epileptogenesis. 4
Despite these mechanistic insights, the potential anticonvulsive or anti-epileptogenic effects of AT1R blockade in humans remain uncertain. Retrospective cohort studies based on national health administrative databases have consistently reported an association between angiotensin-receptor blocker (ARB) therapy and a reduced incidence of epilepsy compared with other antihypertensives in patients with hypertension and/or ischemic stroke.6–9 However, these studies did not delineate the underlying aetiology of epilepsy, limiting the interpretation of ARBs mechanistic effect.
Our previous retrospective observational study demonstrated that patients with acute stroke receiving ARB therapy exhibited a significantly lower incidence of acute symptomatic seizures (ASS) than those not treated with ARBs. 10 As ASS represent provoked events rather than a chronic epilepsy disorder, these findings pertain solely to the acute anti-seizure properties of ARBs. Whether ARBs also mitigate the risk of post-stroke epilepsy (PSE) has not been established.
The objective of the present study was therefore to determine whether ARB therapy is associated with a reduced risk of both ASS and PSE in patients with acute stroke compared with no ARB therapy.
Methods
Study setting and design
This retrospective, observational, referral-centre cohort study was conducted with longitudinal follow-up. The enrolled patients were admitted to the Department of Neurology and Stroke, South-buda Central Hospital, Szent Imre Teaching Hospital, Budapest, Hungary, between 1 January 2019 and 31 December 2023. We enrolled individuals aged 18 years or older with neuroimaging-confirmed acute ischaemic or haemorrhagic stroke (n = 3074). We excluded patients with no evidence of stroke on computed tomography (CT) and/or magnetic resonance imaging (MRI) (n = 159), transient ischaemic attack (n = 135), prior diagnosis of seizures or epilepsy (n = 10), potentially epileptogenic comorbidities (i.e., intracranial tumour, history of severe traumatic brain injury or brain surgery) (n = 63), or ambiguous seizure-like events (n = 43). In addition, patients who discontinued their ARB therapy after the stroke during the follow-up (n = 34), and patients who died within 7 days of the acute stroke event (n = 140) were excluded from the PSE analysis (Figure 1).

Study flowchart of patient selection. ARB: angiotensin receptor blockers; ICD-10: International Classification of Diseases Tenth Revision; TIA: transient ischaemic attack. aOnly in group with post-stroke epilepsy. bPatients with acute symptomatic seizures and/or post-stroke epilepsy.
Data source
The study was approved by the Institutional Research Ethics Committee (IKEB) of our hospital (No. IKEB 23/2023). We conducted a retrospective investigation using clinical data from our hospital database (Medworks). Patients with acute stroke were identified using ICD-10 (International Classification of Diseases Tenth Revision) codes: I60-I67 within the study timeframe from our electronic medical records. We collected demographic, diagnostic, interventional and therapeutic data generated during the inpatient and outpatient visits. We reviewed and screened each medical report, and enrolled only those patients who met the enrolment criteria. The statistical analysis was conducted from January 2025 to June 2025.
Exposure definitions
According to the International League Against Epilepsy (ILAE) definition, ASS was defined as provoked epileptic seizure occurring in close temporal relationship with the acquired stroke lesion within seven days. If a seizure occurred more than seven days after the acute stroke, it was classified as PSE. 11 The diagnosis of ASS and PSE was established through an integrated evaluation of clinical findings—specifically eyewitness accounts of seizures—and/or electroencephalographic (EEG) results. If EEG was not performed, or the record was normal, we diagnosed the event when the seizure type was clinically well documented. Further electrophysiological details were beyond the scope of this study, and did not influence the primary outcomes. The ARB therapy was defined as continuous treatment with an angiotensin receptor blocker acting on the AT1R. We enrolled only those patients who were treated with ARB therapy at the time of the acute stroke event and throughout the follow-up period. There was no information on patient treatment compliance in the medical database. The follow-up period was defined as the period during which we had information about the patient in our medical records.
Outcome assessment
We allocated the enrolled patients with acute stroke into two groups. One group received continuous ARB therapy at admission and throughout follow-up. In the other group there was no ARB therapy or it was not continuous. The primary study outcome was to assess the difference in seizure incidence, with ASS and PSE combined, between the two patient groups with and without ARB therapy. The secondary study outcome was to assess the differences between the subgroups with the following characteristics: only ASS, only PSE and any type of seizures.
Covariates
Potential risk factors and clinically relevant variables associated with ASS and PSE were identified at the time of the acute stroke: patient demographic data (sex, age), relevant comorbidities such as diabetes, atrial fibrillation, peripheral arterial disease, carotid atherosclerosis, renal failure measured using laboratory estimated glomerular filtration rate (eGFR) and stroke-related data (aetiology, localisation and severity). In addition, reperfusion treatment (intravenous thrombolysis and/or endovascular thrombectomy) and antihypertensive medication data were collected. We used the World Health Organization (WHO) definitions for stroke. The National Institutes of Health Stroke Scale (NIHSS) was used to define stroke severity. 12 We defined mild (NIHSS ≤ 5) and severe (NIHSS > 5) stroke categories. Stroke aetiology was classified according to the modified Trial of Org 10,172 in Acute Stroke Treatment as ischaemic stroke (large vessel disease, small vessel disease, cardioembolic stroke, cryptogenic stroke), and haemorrhagic stroke. 13 We collected the following antihypertensive drug treatments: ARB, angiotensin-converting enzyme inhibitors (ACEI), α-blockers, β-blockers, calcium channel blockers (CCB), and thiazide-like diuretics.
Statistical analysis
We report the mean and standard deviation of normally distributed continuous parameters, and comparisons between these groups were performed with a t-test for independent samples. The absolute and percentage values of discrete parameters’ frequencies are presented and comparisons between these groups were performed with a z-test and chi-squared test. First, the parameters listed in the baseline table were analysed in univariable logistic models with and without adjustment for age and gender, and then the parameters with significant odds ratio (OR) values (ARB, haemorrhagic stroke, hypertension, NIHSS score ≥ 5 points, carotid atherosclerosis, ACEI, CCB, and thrombolysis) were further tested in a multivariable model. The results of the above-mentioned parameters from both logistic regression models are presented in tables. P < .05 was considered statistically significant. The statistical analysis was performed using the R statistical program, version 4.2.3, and reporting our results were in accordance with EQUATOR STROBE guidelines for observational studies.
Results
The study included 2589 patients; mean (SD) age was 72.0 (±13.2) years; 1306 (50.4%) were women and 1283 (49.6%) were men; the median follow-up duration was 18 months (IQR 3–31). The baseline characteristics of the patients are shown in Table 1. Patients receiving ARB therapy were significantly older and had higher rates of diabetes and hypertension, lower mean NIHSS scores, and lower mean eGFR values. In the ARB-treated group, significantly more patients had ischaemic stroke and significantly more patients were on antihypertensive therapy. Other variables were similar between the two groups.
Baseline characteristics of the study population at time of the acute stroke.
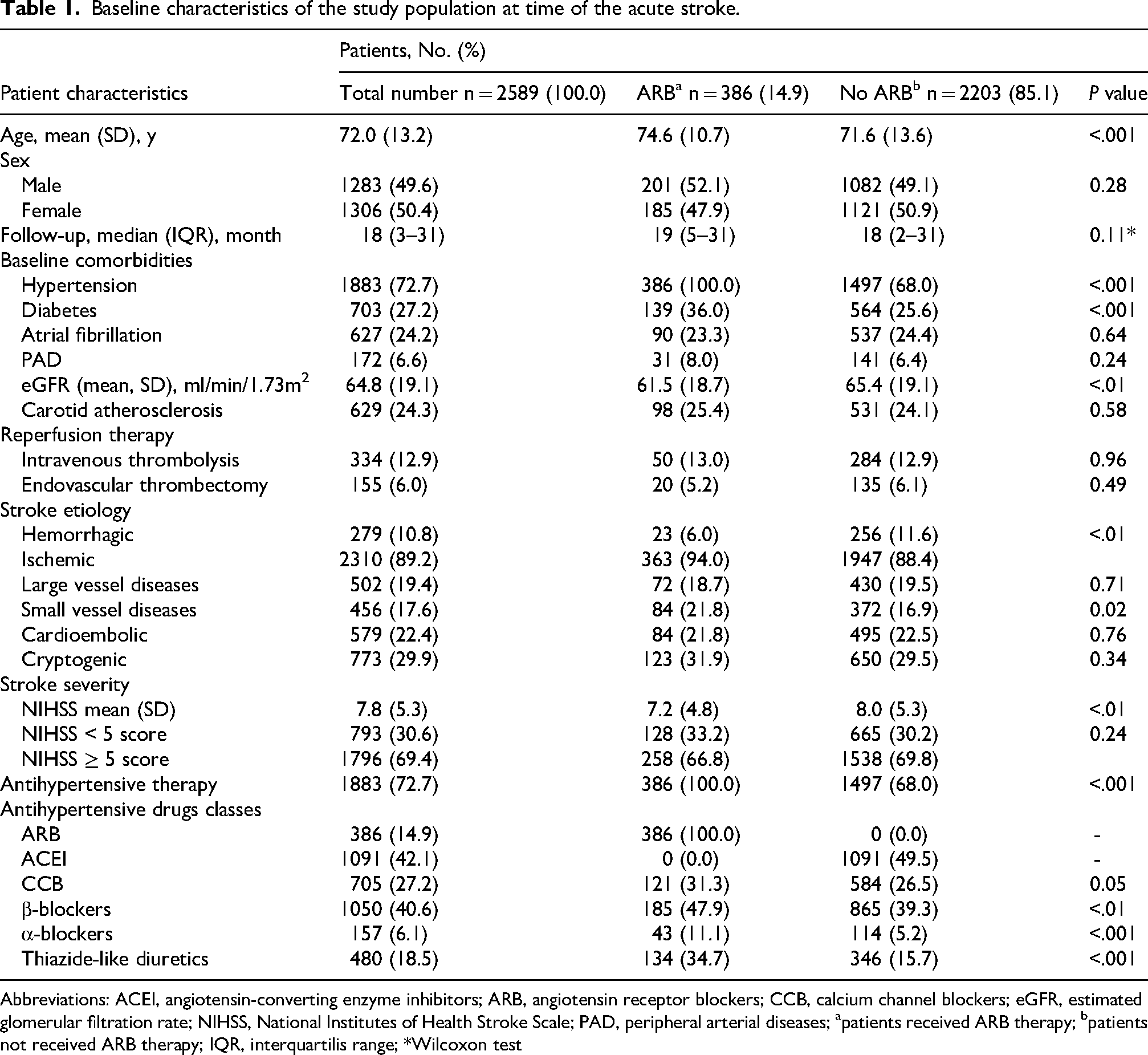
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CCB, calcium channel blockers; eGFR, estimated glomerular filtration rate; NIHSS, National Institutes of Health Stroke Scale; PAD, peripheral arterial diseases; apatients received ARB therapy; bpatients not received ARB therapy; IQR, interquartilis range; *Wilcoxon test
The primary study outcome was ASS and/or PSE; these occurred in 16 of 386 patients (4.1%) with ARB therapy and 227 of 2203 patients (10.3%) without ARB therapy (P < .001). If we further divided the patients according to seizure types we also found significant differences between the subgroups. In patients with only ASS (n = 101), there was a significantly lower percentage of seizures in ARB treated group (2.1% vs. 4.2%; P = .045). Similarly, in the ARB-treated group there was a significantly lower incidence of seizures in the PSE (1.6% vs. 3.9%; P = .017) and combined PSE and ASS (0.5% vs. 2.2%; P = .026) groups (Table 2).
Incidence of the seizure types in patients with acute stroke.
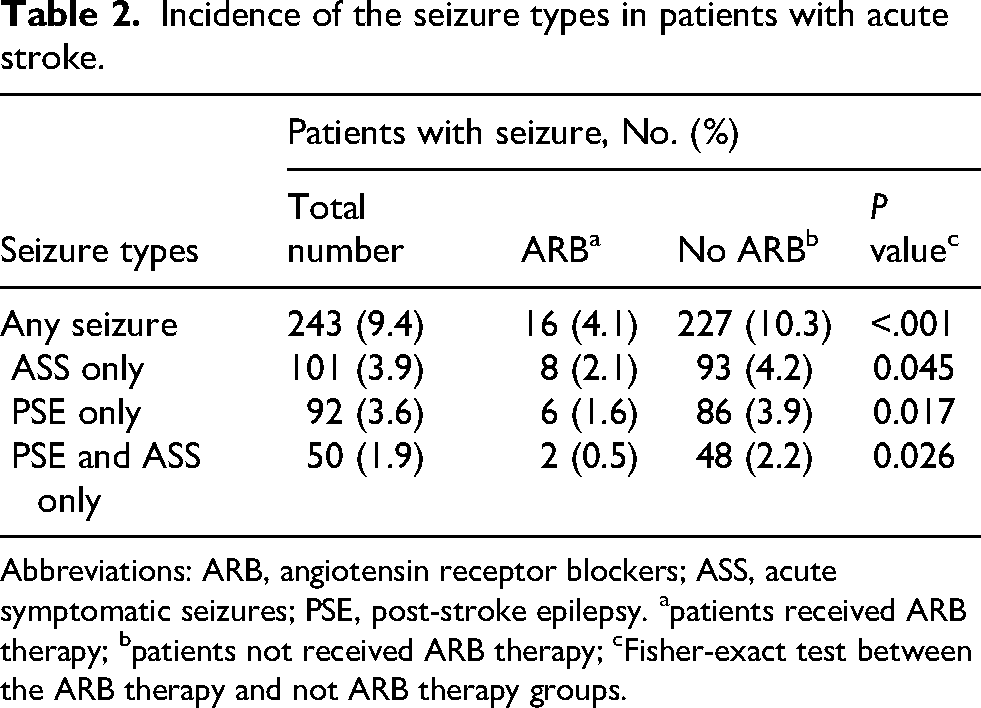
Abbreviations: ARB, angiotensin receptor blockers; ASS, acute symptomatic seizures; PSE, post-stroke epilepsy. apatients received ARB therapy; bpatients not received ARB therapy; cFisher-exact test between the ARB therapy and not ARB therapy groups.
In the univariable logistic regression model, the following variables were significantly associated with seizures: ARB therapy (odds ratio [OR], 0.38; 95% CI, 0.22–0.63; P < .001), thrombolysis (OR, 0.55; 95% CI, 0.34–0.89; P = .014), haemorrhagic stroke (OR, 2.69; 95% CI, 1.93–3.75; P < .001), hypertension (OR, 1.63; 95% CI, 1.17–2.27; P < .01), higher NIHSS score (per 5-point increase), (OR, 1.23; 95% CI, 1.10–1.39; P < .001), ACEI therapy (OR, 1.82; 95% CI, 1.39–2.37; P < .001). After adjustment for age and gender, the following parameters remained significant as protective factors: ARB therapy (OR, 0.39; 95% CI, 0.23–0.65; P < .001), thrombolysis (OR, 0.53; 95% CI, 0.33–0.86; P = .011). Risk factors that remained significant were hypertension (OR, 1.96; 95% CI, 1.38–2.78; P < .001), haemorrhagic stroke (OR, 2.66; 95% CI, 1.86–3.63; P < .001), higher NIHSS score (OR, 1.29; 95% CI, 1.27–1.30; P < .001), ACEI therapy (OR, 1.96; 95% CI, 1.49–2.57; P < .001), CCB therapy (OR, 1.35; 95% CI, 1.01–1.79; P = .04) (Table 3). In the multivariable logistic regression model, ARB therapy remained a significant protective factor (OR, 0.38; 95% CI, 0.21–0.68; P < .001) together with thrombolysis (OR, 0.54; 95% CI, 0.33–0.89; P = .016) and age per 5-year increase (OR, 0.91; 95% CI, 0.86–0.96; P < .001). In contrast, significant risk factors were haemorrhagic stroke (OR, 2.20; 95% CI, 1.54–3.15; P < .001), hypertension (OR, 2.28; 95% CI, 1.44–3.11; P < .001), and higher NIHSS score (per 5-point increase) (OR, 1.26; 95% CI, 1.12–1.43; P < .001) (Table 3).
Logistic regression analysis of predictors associated with seizuresa in patients with acute stroke.
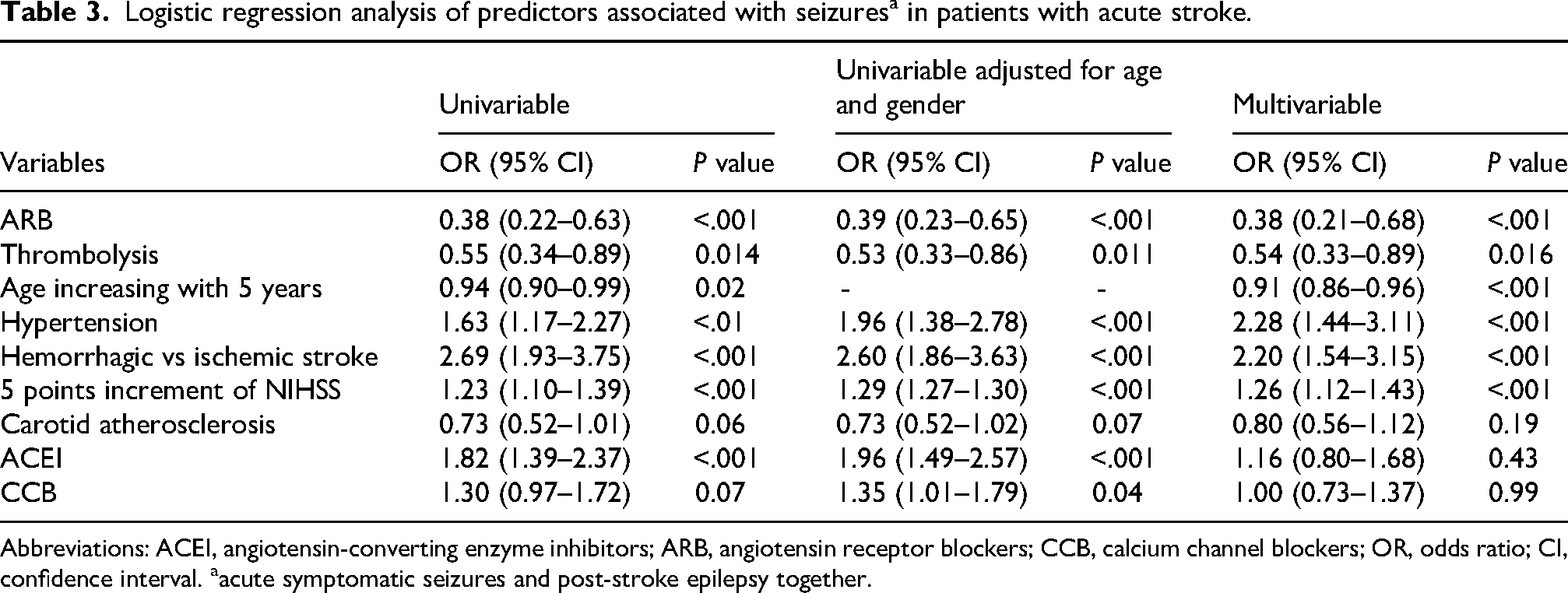
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; CCB, calcium channel blockers; OR, odds ratio; CI, confidence interval. aacute symptomatic seizures and post-stroke epilepsy together.
Regarding the secondary study outcome, we entered separate patient subgroups into age- and gender-adjusted multivariable models to test whether ARB therapy remained a significant parameter in the different types of seizure subgroups. In this model, ARB therapy remained a significant protective parameter in all three subgroups: only ASS (OR, 0.40; 95% CI, 0.19–0.84; P = .016), PSE only (OR, 0.16; 95% CI, 0.14–0.76; P < .01) and combined PSE and ASS (OR, 0.22; 95% CI, 0.05–0.93; P = .04). Furthermore, in the only ASS group the protective factor was thrombolysis (P < .01), while the risk factors were hypertension (P < .01), haemorrhagic stroke (P < .021), and increased NIHSS scores (P < .01). In the only PSE group, thrombolysis lost its significance, and in patients with combined PSE and ASS, only ARB therapy and haemorrhagic stroke remained significant parameters (Table 4).
Multivariablea logistic regression analysis of predictors associated with different type of epileptic seizures in patients with acute stroke.

Abbreviations: ARB, angiotensin receptor blockers; ASS, acute symptomatic seizures; CI, confidence interval; OR, odds ratio; PSE, post-stroke epilepsy. aadjusted for age and gender.
Discussion
The results of our retrospective, observational cohort study with longitudinal follow-up demonstrated that lower incidences of ASS and PSE were significantly associated with ARB therapy in patients following acute stroke of ischaemic or haemorrhagic origin. Among other risk factors, hypertension, haemorrhagic stroke, and higher stroke severity were significantly associated with an increased risk of epilepsy, while thrombolysis and older age were associated with a decreased risk. Notably, while ACEI therapy was significantly associated with a higher seizure incidence in the univariate analysis, it did not remain an independent predictor in the multivariate model. According to the current concept, epileptogenesis is increasingly understood as the dysfunction of the neurovascular unit, which induces potential epileptogenic lesions in the brain. 14 The neurovascular unit is a highly specialised structure in the central nervous system and is composed of multiple cell types including neurons, astrocytes, microglia, brain vascular endothelial cells and vascular pericytes that work in harmony under physiological conditions. In the context of post-stroke epileptogenesis, disruption of the blood-brain barrier following endothelial damage causes extravasation of albumin and other substances, which activate astrocytes and microglial cells. As a consequence of these processes, the brain undergoes progressive structural and functional changes, leading to increased excitability in the affected area and a higher possibility of recurrent spontaneous seizures.14–18 Therefore, protecting the neurovascular unit is one of the priorities in acute stroke care. Revascularization therapy, such as thrombolysis can reduce hypoxia in acute stroke, which may also attenuate damage to the cerebral vessel wall. According to our findings, thrombolysis may be a protective factor for seizures, probably by protecting the integrity of the neurovascular unit and reducing the infarct size.
The RAS is a fundamental system regulating electrolyte and water balance in the body and its elements are found in almost all organs, even in the brain. Furthermore, the central nervous system has its own RAS, which plays an important role as a physiological neuromodulator and regulates various pathophysiological brain processes.4,19,20 Although several mechanisms have been proposed for the association between ARBs and epilepsy, the exact explanation remains unclear. 21 The results of preclinical research can be outlined in three main areas regarding the association between ARBs and epilepsy.
Firstly, AT1R antagonists have been shown to have direct anticonvulsive effects in various epilepsy models, similar to antiepileptic drugs.22–24 Experimental and clinical studies have shown the hyperactivation of RAS and AT1R signalling pathways under epileptic conditions.4,5,25 The AT1R hyperactivation increases neuronal excitability by enhancing Ca2+ currents, modulating potassium and sodium ion channels and glutamate release.4,5,25 ARBs block the AT1R and consequently the free angiotensins can stimulate the remaining angiotensin receptors, including angiotensin II type 2 receptor (AT2R), Mas receptor, angiotensin II type 4 receptor and MrgD.26,27 When angiotensin II binds to AT2R, it can suppress neuronal excitability by reducing calcium influx and facilitating potassium outflow, which results in hyperpolarization of neurons and increases the seizure threshold.26,27
Secondly, in stroke, blood-brain barrier dysfunction can induce epileptogenesis by triggering a complex cascade due to albumin passing from the serum into the brain interstitial tissue, binding to astrocytes and activating astrocytic TGF-β receptors, which induces transcriptional changes in astrocytes. This transcriptional signalling changes cause astrocytic decoupling and downregulation of K+ and glutamate buffering capacity. The latter leads to the degradation of extracellular matrix, development of new excitatory synapses, and reorganisation of neural networks, which together promote epileptogenesis.28–30 These changes are the major hallmarks of epileptogenesis across animal models of acquired epilepsy. SJN2511, a specific ALK5/TGF-β inhibitor, can block the maturation of excitatory synaptogenesis and epilepsy. 31 In a rat model of vascular injury, losartan blocked astrocytic TGF-β-induced signalling and prevented epileptogenesis. 32 In a mouse model of paediatric epilepsy, candesartan treatment enhanced seizure freedom, diminished blood-brain barrier permeability and partially reversed disease-induced genome-wide gene expression profiles, which was associated with inhibition of TGF-β and other cytokine signalling. 33 Furthermore, pathway analyses revealed that candesartan, an AT1R antagonist, is also a peroxisome proliferator-activated receptor γ agonist. 33
Thirdly, ARBs have been shown to have neuroprotective effects in various animal models which may have an impact on epileptogenesis. ARBs protect against neuronal injury induced by oxygen–glucose depletion in a model of ischaemic injury, 34 improve functional recovery and reduce infarct volume in experimental models of stroke, 35 protect against oxidative stress by augmenting the levels of glutathione and superoxide dysmutase enzymes in a neurotoxic rat model 36 and suppress activated microglia-induced neurotoxic A1 astrocyte conversion through p65 degradation. 37 Considering these results there is great interest in whether human astrocyte–microglia crosstalk may activate the brain renin–angiotensin system during neuroinflammation. 38
In addition to the above mentioned data, the results of our study may support a hypothesis that ARBs are acting to reverse the pathogenic mechanisms leading to seizure occurrence. Since ASS (which is a provoked seizure due to acute electrolyte imbalance)39,40 and PSE (which is epilepsy disease due to epileptogenesis) were associated with a lower incidence in patients receiving ARB therapy, this suggests that blocking AT1R may modify neuronal excitability via multiple processes. It can be assumed that ARB therapy may play a role in reducing the risk of ASS by increasing the seizure threshold in acute stroke (anti-seizure effect) and reducing the risk of PSE by inhibiting neuroinflammatory processes (mainly TGF-β signalling) in astrocytes and microglia (anti-epileptogenic and neuroprotective effect) in patients after stroke.
The novel aspects of our study are as follows. We used a clinically confirmed stroke cohort rather than an administrative health insurance database. The majority of previous investigations based on national healthcare data also showed an association between ARB therapy and a lower incidence of seizures compared with other antihypertensive drugs in patients with hypertension.6–10 However, these studies did not provide information about the nature of the seizures. We included patients with haemorrhagic stroke, because it has a twofold greater risk of seizures compared with ischaemic stroke. 41 Therefore, the risk of seizures was higher in our study population than in patients with ischemic stroke only. To our knowledge, we are the first to analyse data by seizure type for both ASS and PSE, because these subgroups of seizures differ significantly. We found a significant and independent association between ARB therapy and the incidence of seizures, including both subgroups. In contrast to a previous study in which the authors reported a benefit of RAS antagonists for both ACEIs and ARBs together 8 in our cohort, ACE inhibitor (ACEI) therapy was associated with a higher seizure incidence in the univariable analysis. However, this association did not remain significant in the multivariable model. Therefore, ACEI therapy was not an independent predictor of seizures in our study. This contrasts with ARB therapy, which remained a robust protective factor across all models. The lack of association for ACEI can be explained by the fact that ARBs provide complete AT1R blockade and enable AT2R activation, which may offer greater neuroprotection. In addition, ACEI increase bradykinin levels and influence the concentrations of other ACE substrates, which may theoretically enhance neuronal excitability. Since ASS belongs to the class of provoked seizures, it might be worthwhile to investigate the association between ARB therapy and other provoked seizures (e.g., trauma, infections, tumours) in the future.
One of the most important clinical implications of our study is that the results are closely linked to the highly prevalent condition of arterial hypertension, a major risk factor for cardiovascular diseases, including stroke. Epidemiological data indicate that globally one in four individuals over the age of 25 will experience a stroke during their lifetime. 42 Stroke is the most common cause of seizures and epilepsy in the elderly population. 43 The incidence of ASS and PSE ranges between 3–6% among stroke patients, although this varies according to aetiology, lesion location, disease severity, and diagnostic accuracy. 44 It is important to emphasise that ASS does not in itself indicate epilepsy; however, the ten-year risk of developing PSE is 33% in patients who have experienced a previous acute provoked seizure. 45 Current guidelines for the management of arterial hypertension recommend combination therapy as the firs-line approach in the most cases, typically involving a RAS blocker (either ACEI or ARB), together with CCB or thiazide-like diuretics. 46 Our results should therefore draw clinicians’ attention to the potential additional benefits of ARBs in reducing the risk of PSE among stroke patients. It would be highly valuable for these to be examined in further studies, which could ultimately support their incorporation into future hypertension management guidelines. Such developments may offer more effective protection for affected patients against adverse neurological outcomes, including ASS and PSE.
Limitations
Our study has several limitations. First, the study is a retrospective, single-centre observational study, which limits generalisability to other healthcare systems or populations. Second, we collected data from all consecutive patients in our medical records; as a result, the two analysed groups differed in several parameters, including epidemiology, comorbidity and antihypertensive use. Despite these differences, ARB therapy remained a significant parameter in the multivariable model. Third, the majority of patients were managed according to recent local and international guidelines and received combination antihypertensive therapies in both groups; therefore, our results refer primarily to combination therapy. A further limitation is that we had no data on treatment compliance. Fourth, although the number of patients with stroke was relatively high (n = 2589) and the frequency of ASS and PSE corresponded to international data, the number of epileptic cases was relatively low (n = 243). If we had enrolled more patients or followed the patients for a longer period we would have increased the number of patients with seizure and the statistical power. However, the incidence of seizures occurs mostly within one year after acute stroke. Fifth, we collected data on comorbidities including treatment of hypertension but we do not know the blood pressure values of the patients. There may be further differences in comorbidities or socioeconomic factors between the subgroups. Sixth, additional bias-reduction approaches (e.g., propensity-based methods) were considered but were not feasible because of the small number of seizure events in the ARB group.
Conclusions
To sum up, the results of our study demonstrate that ARB therapy is independently associated with a lower incidence of ASS and PSE in patients following acute stroke. These findings suggest potential anti-seizure, neuroprotective and anti-epileptogenic properties of this antihypertensive drug class. Further basic research and prospective, randomised clinical studies are needed to elucidate the anticonvulsive and anti-epileptogenic effects of ARB medications and to determine whether these benefits should be incorporated into future clinical guidelines.
Footnotes
Acknowledgements
The authors thank András Paksy, MD for his invaluable help in the statistical analysis.
Ethical approval
The study was approved by the Institutional Research Ethics Committee (IKEB) of our hospital (No. IKEB 23/2023).
Author contributions
All authors contributed to the conceptualization and design of the study. All authors performed the literature search and data extraction. The first draft of the manuscript was written by ZK and ZSz, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The statistical analysis was supported by a research grant from the Hungarian Hypertension Society (HHS-2025 Research Grant).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and analysed during the current study are not publicly available due to patient confidentiality and local regulation but are available from the corresponding author on reasonable request. This study is reported in accordance with the STROBE statement.