
Abstract
Background
The role of beta-blockers after myocardial infarction (MI) in patients with preserved ejection fraction remains controversial.
Methods
We systematically searched PubMed, Embase, Web of Science, and the Cochrane Library from their inception to September 2025 for relevant randomized controlled trials (RCTs). The primary endpoint was a composite outcome comprising all-cause deaths, recurrent myocardial infarction, hospitalization for heart failure, and stroke. Risk ratios (RRs) with corresponding 95% confidence intervals (CIs) were calculated as the primary effect estimates.
Results
Five RCTs involving 23524 patients with MI and preserved ejection fraction were included. Pooled results showed that no significant difference was detected between beta-blockers therapy and treatments with no beta-blockers on the composite outcome (RR,0.93; 95% CI,0.84–1.03). However, metoprolol was associated with a modest but statistically significant risk reduction (RR,0.89; 95% CI,0.80–0.99). Beta-blocker therapy did not confer significant reductions on all-cause death, cardiovascular death, myocardial infarction, hospitalization for heart failure, stroke or compared with no beta-blocker use.
Conclusions
In patients with MI and preserved ejection fraction, beta-blocker therapy did not significantly reduce the risk of composite or individual clinical outcomes compared with no beta-blockers use. Notably, metoprolol showed a modest but significant benefit, suggesting that potential agent-specific effects warrant further investigation.
Introduction
The long-term management of myocardial infarction (MI) focuses on reducing the risk of recurrence and death, and improving quality of life. Since the 1980s, beta-blockers have been widely prescribed for secondary prevention after MI, supported by early randomized trials from the pre-reperfusion era that showed substantial reductions in mortality.1,2 However, with the widespread implementation of contemporary therapies—such as primary percutaneous coronary intervention (PCI), dual antiplatelet therapy, and high-intensity statins—the baseline risk profile and prognosis of modern MI patients have changed substantially.3–5 Furthermore, contemporary MI management is centered on renin-angiotensin-aldosterone system (RAAS) inhibition therapy, with the benefits of angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers (ACEI/ARB) in improving ventricular remodeling and long-term prognosis being well-established, making them standard treatment.6–8 Against this backdrop, the incremental benefit of beta-blockers as another form of neurohormonal antagonism—particularly in populations with preserved left ventricular ejection fraction (LVEF)—may be more limited, thereby casting doubt on their absolute benefit in this specific group.
Current guidelines strongly recommend beta-blockers for patients with MI and reduced LVEF, but the strength of recommendation is lower for those with LVEF ≥40%, reflecting uncertainty in the supporting evidence for this population.9,10 In recent years, several high-quality randomized controlled trials (RCTs), including REBOOT and BETAMI-DANBLOCK, have re-evaluated the efficacy of beta-blockers in this population.11–15 However, the findings have been inconsistent—some trials reported positive outcomes, whereas others were neutral—suggesting potential unrecognized heterogeneity in treatment response.
Several meta-analyses published in 2025 revisited this question, but their conclusions remained inconsistent. Alnemer et al. suggested potential reductions in all-cause mortality, cardiovascular mortality, and major adverse cardiovascular events in patients with preserved LVEF, although their findings were derived mainly from observational studies using variable LVEF thresholds. Chen et al., who included 16 observational studies and 2 randomized controlled trials, found that the apparent mortality benefit was largely confined to unmatched observational studies, whereas no significant reduction in all-cause death was observed in propensity score-matched analyses or randomized evidence; they also suggested that any long-term benefit might be concentrated in patients with an LVEF of 40–50%. Gomes et al., focusing specifically on preserved LVEF, reported that the apparent reduction in all-cause mortality was no longer significant after sensitivity analyses, with no clear benefit for reinfarction, hospitalization for heart failure, or stroke. Taken together, these meta-analyses are informative but remain limited by their heavy reliance on observational evidence, inconsistent definitions of preserved versus mildly reduced LVEF, and incomplete incorporation of the most recent contemporary randomized trials. Consequently, they do not provide a definitive estimate of the effect of long-term beta-blocker therapy based exclusively on contemporary randomized evidence.16–18
Notably, a recent individual patient data (IPD) meta-analysis suggested that the benefit of beta-blockers might be concentrated in patients with LVEF 40–49%. 19 Since this group accounts for a substantial proportion (approximately 25–30%) of the overall MI population, according to registry studies, clarifying their treatment response is crucial for both public health and clinical practice.20,21 These findings further suggest that treatment effects may vary across the spectrum of LVEF ≥40%, and that analyses combining mildly reduced and preserved EF populations may obscure clinically relevant heterogeneity.
To clarify the overall efficacy of beta-blockers in MI patients with LVEF ≥40% in the context of contemporary treatment, we systematically conducted a meta-analysis of relevant RCTs. Unlike prior meta-analyses, the present study was restricted to contemporary randomized evidence and was therefore designed to provide a less confounded estimate of the average treatment effect in current practice. We also explored potential sources of heterogeneity through drug-class subgroup analyses, sensitivity analyses, and trial sequential analysis. Our objective is to evaluate the overall effect of long-term beta-blocker therapy on MI with preserved EF and discuss the implications for clinical practice and guideline development in light of the most recent evidence.
Methods
This meta-analysis was performed in accordance with a pre-registered protocol (CRD420251149074) prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO). The systematic review and meta-analysis were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 22
Data sources and search strategy
We systematically searched PubMed, Embase, Web of Science, and the Cochrane Library from their inception to September 2025 for relevant randomized controlled trials. No restrictions were applied regarding the publication language. The search strategy was developed using the PICOS framework, with a focus on the population (individuals with myocardial infarction and without reduced ejection fraction) and intervention (treatment with beta-blockers, such as bisoprolol, metoprolol, and carvedilol). The complete search terms and strategy are detailed in Supplementary Table 1.
Study selection
This analysis aimed to identify and include RCTs evaluating the effect of beta-blocker therapy, as compared with no beta-blocker therapy in the management of myocardial infarction without reduced ejection fraction. Eligible studies met the following criteria: (1) adult patients aged ≥18 years; (2) prospective randomized clinical trial design; and (3) availability of outcome data, including all-cause deaths, cardiovascular deaths, myocardial infarction, hospitalization for heart failure, or stroke. The exclusion criteria included: (1) studies involving patients under 18 years of age; (2) non-randomized study designs; and (3) trials lacking the specific outcomes of interest.
The screening of titles and abstracts for all retrieved records was performed independently by two reviewers (QS and ZZ) using NoteExpress software (v3.9.0; AegeanSoftware Corp, Beijing, China). Subsequently, the full texts of potentially eligible articles were assessed by the same reviewers to determine final inclusion. Any disagreements that arose during either stage were resolved by consensus, with consultation of a third reviewer (XT) when necessary.
Data extraction and quality appraisal
Two investigators (QS and ZZ) independently extracted data from the eligible studies using Microsoft Excel 2017 (Microsoft, Redmond, WA, USA), following a predefined and standardized data extraction form. The form included study characteristics (author, study design, study region, study period, sample size, duration of follow-up, LVEF threshold, and Beta-Blocker Type), baseline characteristics (mean age, sex, body mass index (BMI), LVEF, rate of ST-segment elevation myocardial infarction (STEMI), medical and medication history), intervention (treatment with beta-blockers or no beta-blockers), and outcome measures (all-cause deaths, cardiovascular deaths, myocardial infarction, hospitalization for heart failure, and stroke.). The methodological quality of the included trials was independently assessed by the same two investigators using the Cochrane Risk of Bias Tool 2 (ROB2). 23 Any discrepancies were resolved through discussion and, when necessary, by consultation with a third investigator (XT).
Clinical outcomes
The objective of this analysis was to assess the effect of beta-blocker therapy compared with no beta-blocker use in patients with myocardial infarction and preserved ejection fraction. The primary endpoint was a composite outcome comprising all-cause deaths, recurrent myocardial infarction, hospitalization for heart failure, and stroke. Secondary endpoints included the individual components of the primary outcome as well as cardiovascular deaths.
Statistical analysis
A study-level meta-analysis of randomized controlled trials was performed to compare beta-blocker therapy compared with no beta-blocker use in patients with myocardial infarction and preserved ejection fraction. Risk ratios (RRs) with corresponding 95% confidence intervals (CIs) were calculated as the primary effect estimates for dichotomous outcomes. Owing to anticipated clinical and methodological heterogeneity across studies, a random-effects model was applied to obtain conservative pooled estimates. Between-study heterogeneity was assessed using the Q statistic (p < 0.05 indicating significant heterogeneity) and quantified with the I2 statistic, with values of <25%, 25%–50%, and >50% interpreted as low, moderate, and high heterogeneity, respectively.
To explore potential sources of heterogeneity, we conducted several sensitivity analyses. First, subgroup analyses were performed according to the type of beta-blocker used. Second, a leave-one-out analysis was undertaken, sequentially omitting each study to evaluate the robustness of the results. Third, account for the potential confounding effects of renin-angiotensin-aldosterone system-related diseases and medication use, we performed a meta-regression analysis based on age, female ratio, PCI ratio, hypertension, diabetes, ACEI/ARB use and Calcium channel blockers use.
Publication bias was assessed using both visual and statistical approaches. Contour-enhanced funnel plots were generated to assess the symmetry of effect estimates and to distinguish asymmetry potentially due to publication bias from that attributable to heterogeneity or chance. In addition, Egger's regression test was performed to quantitatively evaluate small-study effects, with p < 0.05 considered indicative of significant asymmetry.
To evaluate the robustness of the pooled estimates and control for the risk of random errors due to sparse data or repeated significance testing, trial sequential analysis (TSA) was conducted using the TSA software (version 0.9.5.10, Copenhagen Trial Unit, Denmark). A two-sided type I error (α) of 5% and a type II error (β) of 20% (power 80%) were applied. Because previous meta-analysis showed no statistically significant association, 24 a relative risk reduction (RRR) of 20% was assumed, representing a moderate and clinically meaningful effect size. To address uncertainty regarding this assumption, additional sensitivity TSA analyses were conducted using more conservative RRR estimates of 15% and 10%.
The certainty of the evidence was appraised using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework, with evidence quality categorized as very low, low, moderate, or high. GRADEpro GDT software (McMaster University and Evidence Prime, Hamilton, ON, Canada) was employed to generate the summary of findings tables.
Meta-analyses were performed using Review Manager version 5.3 (Cochrane Collaboration, Copenhagen, Denmark) and R version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria). The “metafor” package in R was applied to generate contour-enhanced funnel plots and to conduct Egger's regression test. Statistical significance was defined as a two-sided P value < 0.05.
Outcomes
A total of 3066 records were identified through the literature search, and 2604 remained after removing duplicates. After thorough screening of titles, abstracts, and full texts, five studies were ultimately included in the final analysis.11–15 (Figure 1)
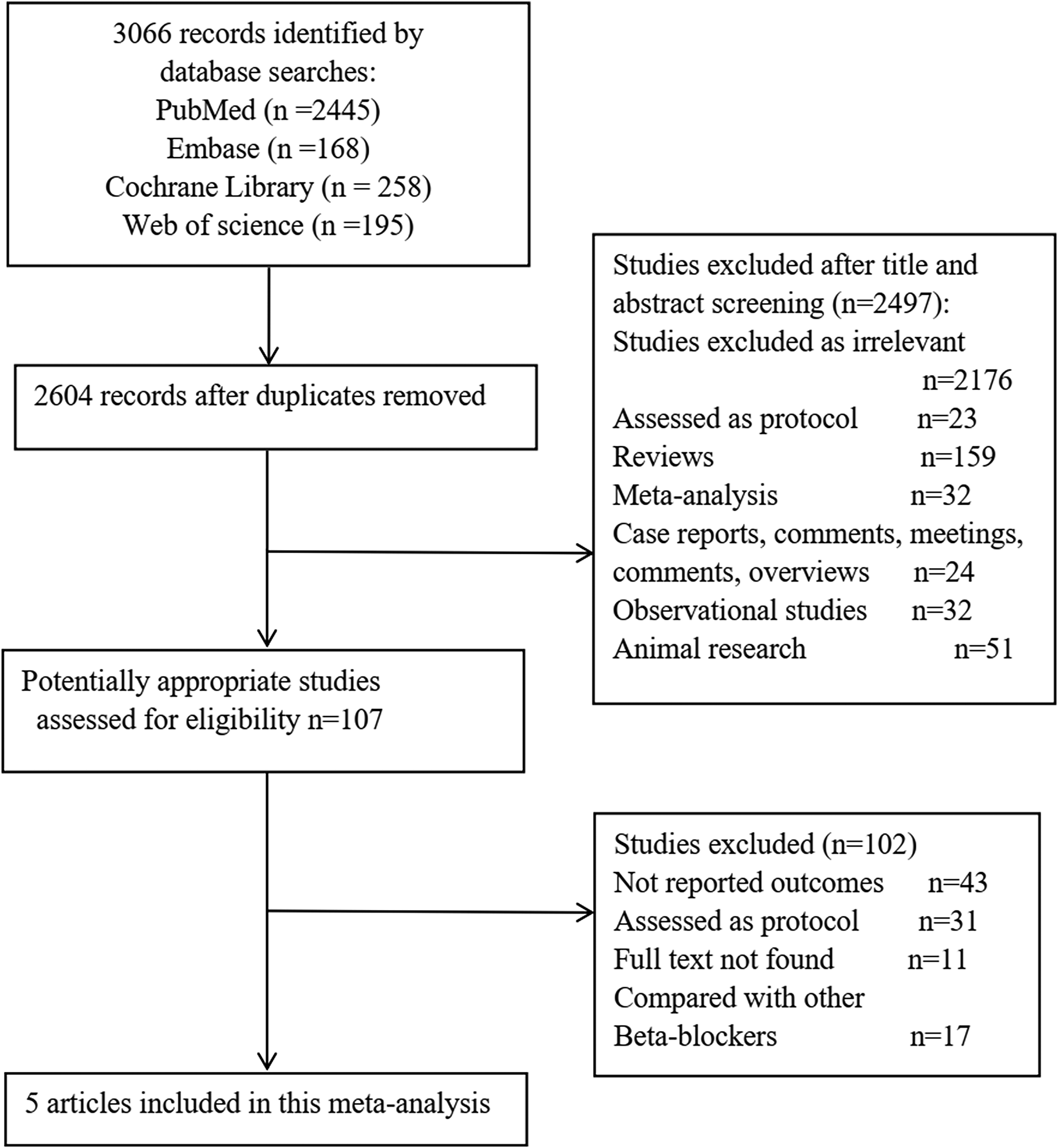
Selection process of included studies. RCT, Randomized Controlled Trials.
Characteristics of the eligible trials
All included trials were conducted in developed countries across Europe and Asia, including Spain, Italy, Norway, Denmark, France, Sweden, Estonia, New Zealand, and Japan. The study period spanned from 2010 to 2024, with a median follow-up duration ranging from 3.0 years in the ABYSS trial to 3.9 years in the CAPITAL-RCT. The LVEF inclusion threshold was ≥40% in four trials and ≥50% in the REDUCE-AMI trial. The types of beta-blockers used varied across studies, with bisoprolol and metoprolol being the most commonly prescribed. The main study characteristics are summarized in Table 1.
Characteristics of the included studies.
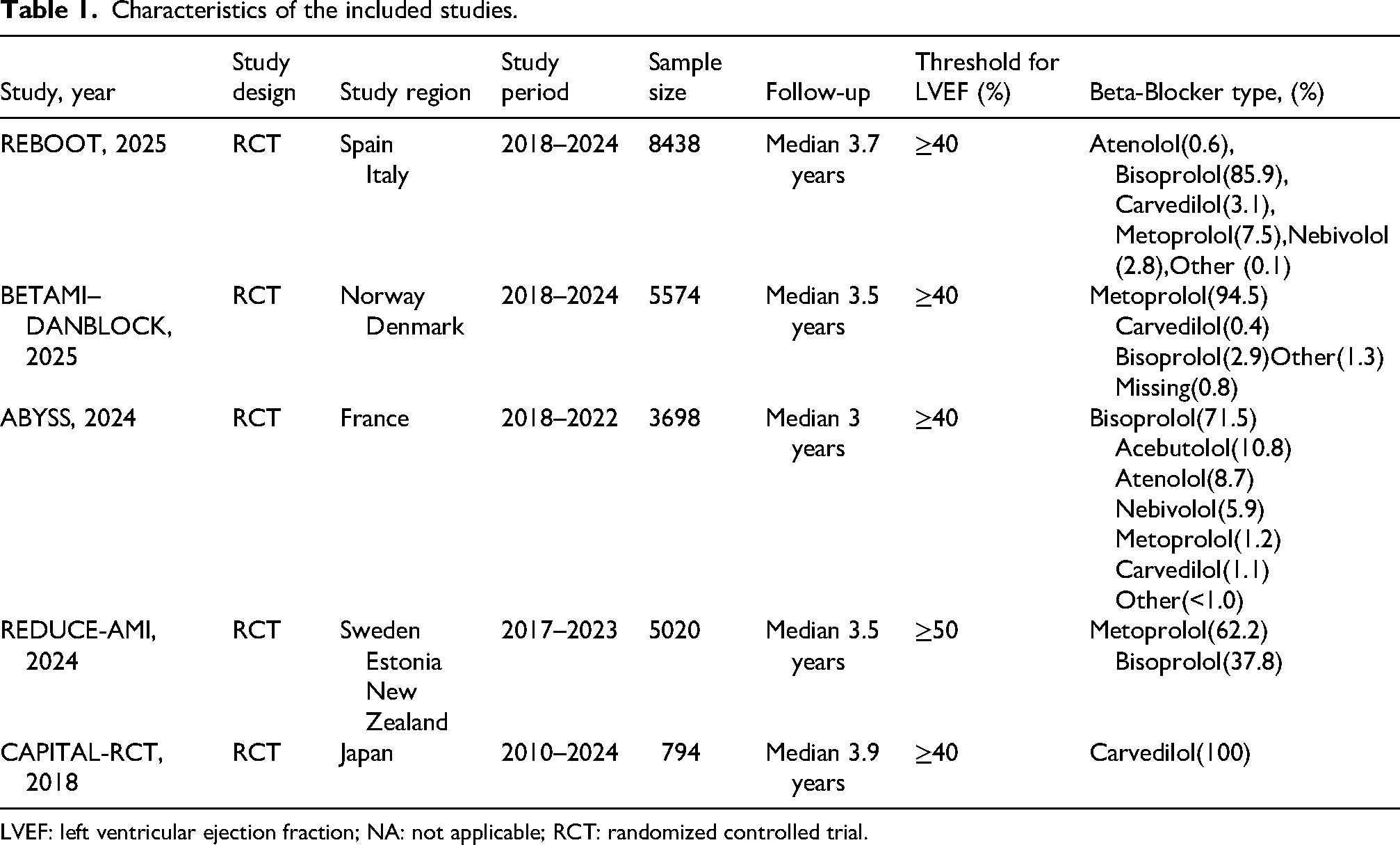
LVEF: left ventricular ejection fraction; NA: not applicable; RCT: randomized controlled trial.
A total of 23,524 participants were included across the five trials, with 11,744 randomized to the beta-blocker group and 11,780 to the control group. The mean or median age of participants ranged from 61.3 to 65 years. The proportion of female participants varied between 17.0% and 22.6%. The prevalence of STEMI ranged from 35.0% to 100%, and PCI was performed in 92.5% to 97.4% of patients across the trials. Common comorbidities included hypertension (40.5%–61%), diabetes (11.9%–25%), dyslipidemia (28.9%–53.7%), and current smoking (18.5%–47%). Medication use at baseline was high for aspirin (94.8%–98.6%), P2Y12 inhibitors (88.2%–98%), ACEI/ARB (41.2%–79%), and statins (86%–98.5%). The baseline characteristics are presented in Table 2.
Baseline characteristics of the included studies.
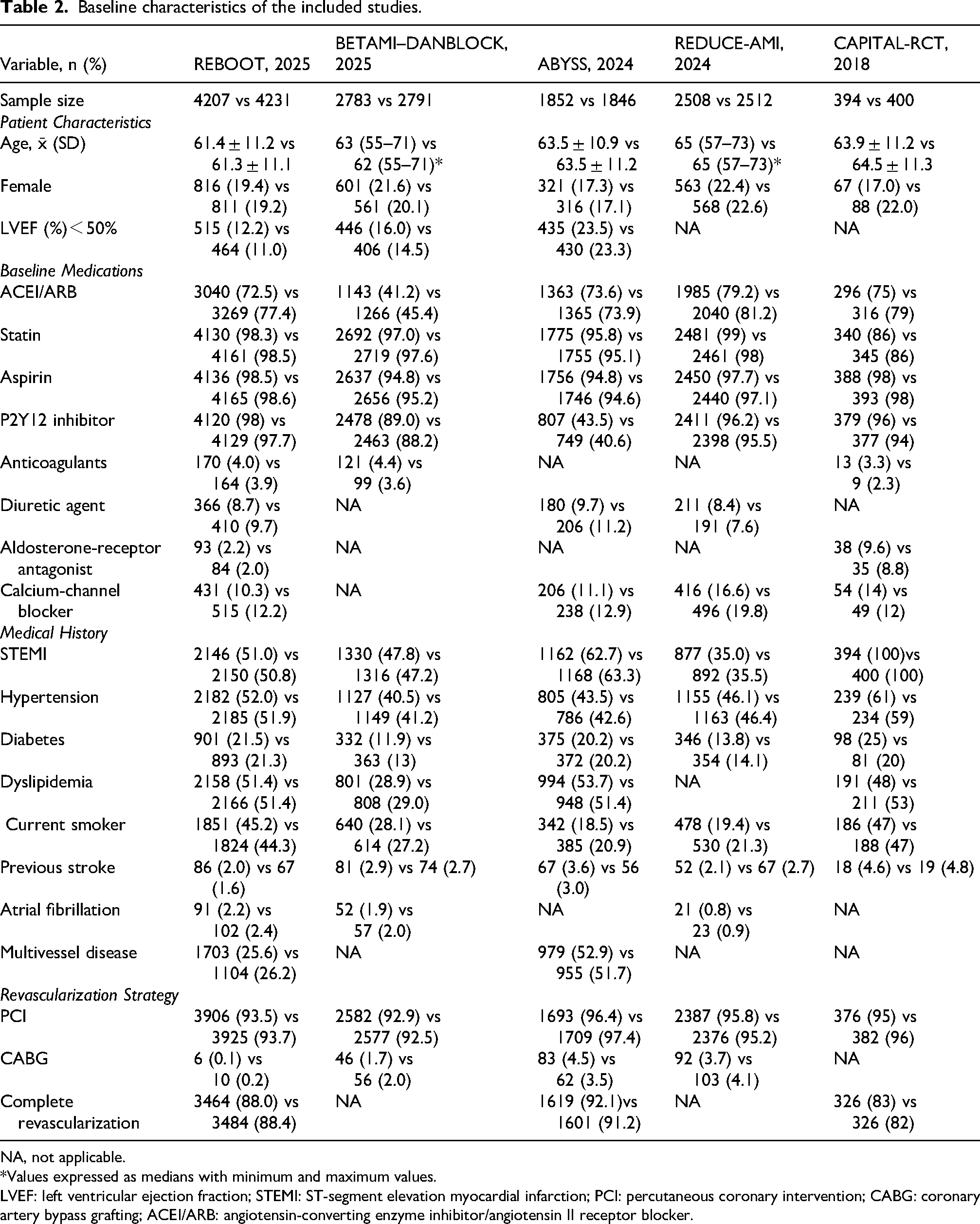
NA, not applicable.
*Values expressed as medians with minimum and maximum values.
LVEF: left ventricular ejection fraction; STEMI: ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; ACEI/ARB: angiotensin-converting enzyme inhibitor/angiotensin II receptor blocker.
The risk-of-bias assessment for each trial is summarized in Supplementary Figure 1. Overall, three studies were judged as having some concerns, whereas two studies were considered at high risk of bias. All included trials were rated as low risk in the domains of the randomization process (D1), missing outcome data (D3), and selection of the reported result (D5). Some concerns were identified in all studies regarding deviations from intended interventions (D2). In addition, two studies were judged as having some concerns in the measurement of outcomes domain (D4). No study was considered at high risk in any individual domain; however, according to the ROB2 overall judgment algorithm, two studies were classified as high risk of bias due to concerns across multiple domains.
Primary outcome
The primary outcome was a composite outcome of all-cause deaths, myocardial infarction, hospitalization for heart failure, and stroke. Pooled results showed that no significant difference was detected between beta-blockers therapy and treatments with no beta-blockers on the composite outcome (9.6% vs 10.2%; RR,0.93; 95% CI,0.85–1.03; I2=31%) (Figure 2(a)). The certainty of evidence was deemed moderate (Supplementary Table 2). In the subgroup analyses, bisoprolol showed a neutral effect (RR 1.01, 95% CI 0.86–1.18), while metoprolol was associated with a modest but statistically significant risk reduction (RR,0.89; 95% CI,0.80–0.99). Carvedilol demonstrated a non-significant trend toward benefit (RR,0.74; 95% CI,0.49–1.14) (Figure 2(a)). In the leave-one-out sensitivity analysis, exclusion of the REBOOT-CNIC trial rendered beta-blocker therapy significantly associated with a reduced risk of the composite outcome, with no statistical evidence of heterogeneity (I2 = 0%). Exclusion of any other individual study did not materially alter the overall effect estimates (Supplementary Table 4). Meta-regression analysis did not identify any significant moderators of the treatment effect. (Supplementary Table 10)
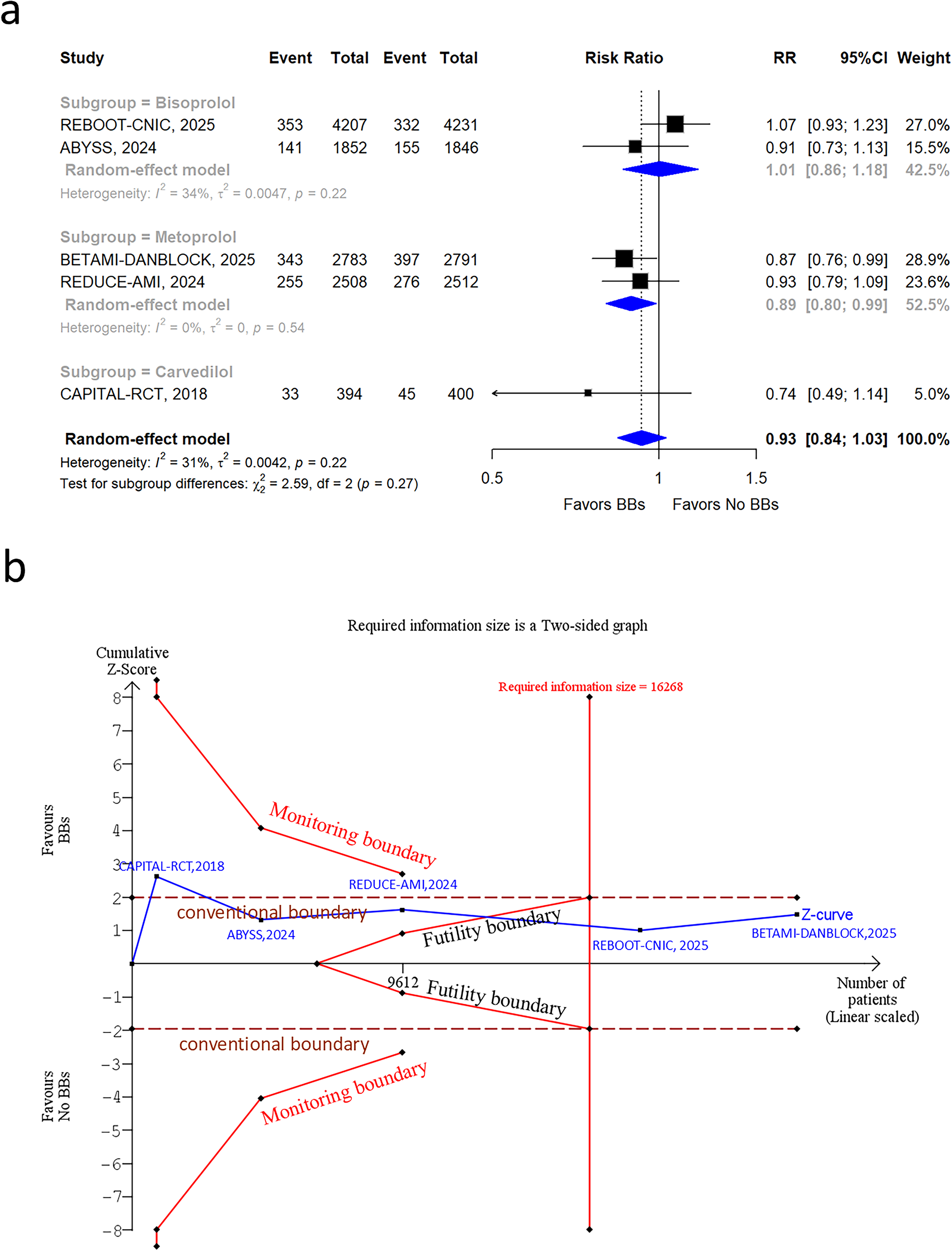
(a) Forest plot illustrating the association of BBs therapy and no BBs with the primary composite outcome. (b) Trial sequential analysis for BBs therapy on the primary composite outcome. BBs: Beta-blockers; RR: risk ratios; CI: confidence interval.
As shown in Figure 2(b), the cumulative Z-curve crossed the required information size (RIS = 16,426) but did not cross the trial sequential monitoring boundaries for benefit or harm. This indicates that the accrued sample size was sufficient, and the current evidence supports a robust conclusion that β-blocker therapy did not significantly reduce the composite outcome compared with no β-blocker therapy. However, for more conservative assumptions (RRR 15% and 10%), the required information size was not reached, and no boundary was crossed, indicating insufficient evidence. (Supplementary Figure 2 and 3)
The contour-enhanced funnel plot revealed a relatively symmetrical distribution of studies around the pooled effect estimate, with no apparent small-study effects. This suggests a low likelihood of substantial publication bias. Consistently, Egger's regression test did not indicate significant asymmetry for the composite outcome (p = 0.476). (Supplementary Table 3 and Supplementary Figure 2)
Secondary outcomes
All included trials consistently reported data on major clinical outcomes, including all-cause death, myocardial infarction, hospitalization for heart failure, and stroke. Overall, beta-blocker therapy did not confer significant reductions compared with no beta-blocker use. Specifically, no significant differences were observed for all-cause deaths (4.0% vs. 4.1%; RR 0.98, 95% CI 0.87–1.11; I2 = 0%) (Figure 3(a)) or myocardial infarction (3.8% vs. 4.3%; RR 0.89, 95% CI 0.72–1.04; I2 = 10%) (Figure 3(c)). Similarly, although a numerical reduction was noted for hospitalization for heart failure (1.1% vs. 1.4%; RR 0.80, 95% CI 0.64–1.01; I2 = 0%) (Figure 3(d)), this did not reach statistical significance. Conversely, stroke occurred slightly more often in the beta-blocker group, but the difference was not significant (1.3% vs. 1.1%; RR 1.16, 95% CI 0.88–1.53; I2 = 0%) (Figure 3(e)). In addition, four trials (17,950 patients; beta-blockers: 8,961, no beta-blockers: 8989) reported cardiovascular death, again showing no significant between-group difference (1.5% vs. 1.4%; RR 1.06, 95% CI 0.83–1.36; I2 = 0%) (Figure 3(b)).
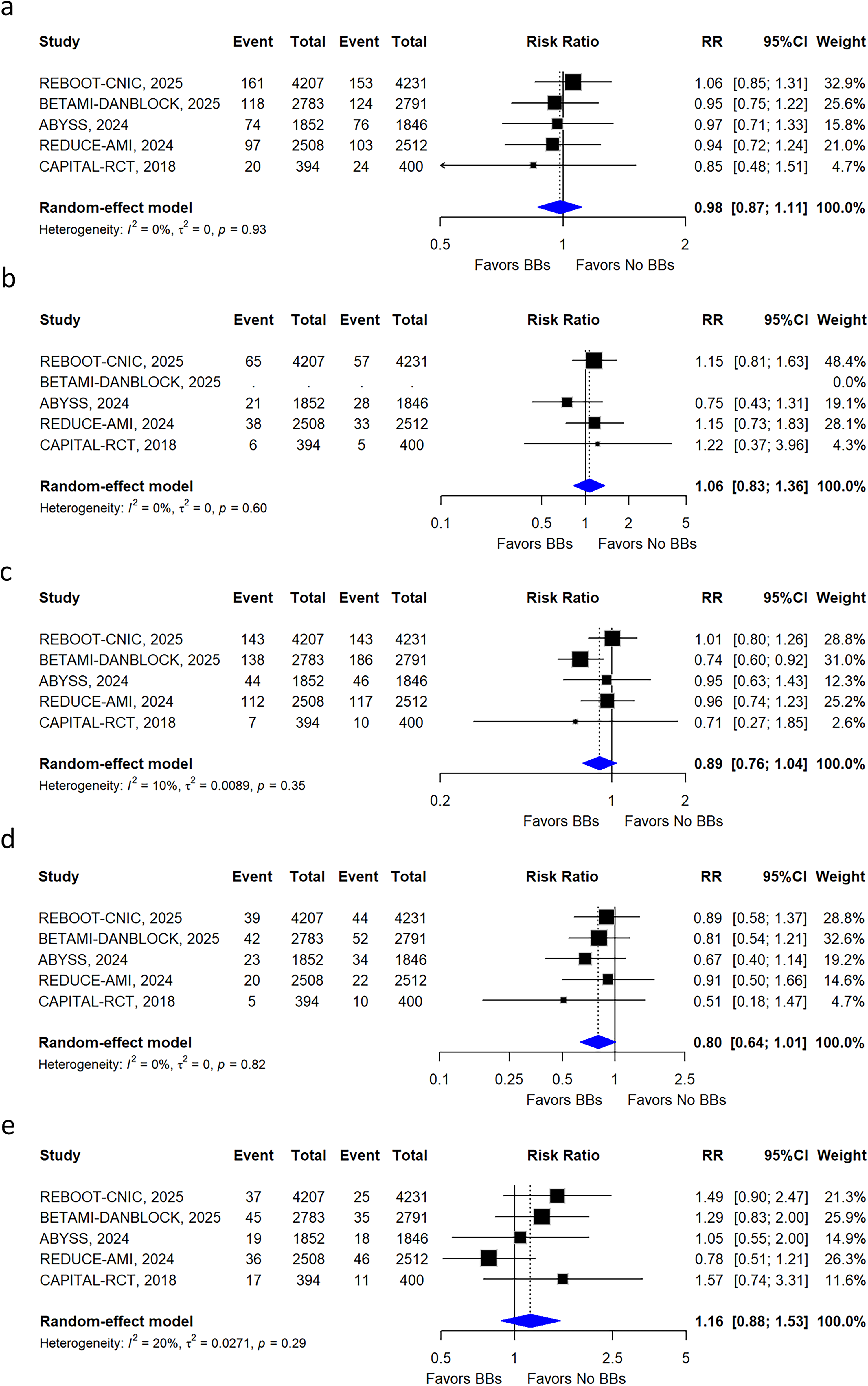
Forest plot illustrating the association of BBs therapy and no BBs with (a) all cause deaths, (b) cardiovascular deaths (c) MI (d) hospitalization for heart failure and (e) stroke. BBs: Beta-blockers; MI: myocardial infarction; RR: risk ratios; CI: confidence interval.
The certainty of evidence for the secondary outcomes were deemed moderate (Supplementary Table 2). Subgroup analyses, leave-one-out sensitivity analyses, and meta-regression analysis yielded results that were largely consistent with the secondary outcomes (Supplementary Table 5–9, 11–14 and Supplementary Figure 3–7). The contour-enhanced funnel plots suggest a low likelihood of substantial publication bias, and Egger's regression test did not indicate significant asymmetry for the secondary outcomes(Supplementary Table 3 and Supplementary Figure 8–12).
Disscusion
This meta-analysis of five contemporary randomized controlled trials evaluated the effect of long-term routine beta-blocker therapy in MI patients with a LVEF≥40% at discharge, all of whom had received modern revascularization and guideline-directed secondary prevention. The pooled analysis showed that beta-blocker therapy did not significantly reduce the risk of the composite endpoint, which included all-cause death, myocardial infarction, hospitalization for heart failure, and stroke. Furthermore, no statistically significant differences were observed for any individual component of the composite outcome. Taken together, these findings support a neutral overall effect of routine long-term beta-blocker therapy in this broad contemporary population.
This conclusion differs from earlier meta-analyses reporting survival benefits, reflecting the evolution in MI management. Earlier studies often included trials from the era of incomplete reperfusion or incorporated substantial observational data, involving higher-risk patients not receiving contemporary optimized therapy.25,26 With the widespread adoption of primary PCI, high-intensity statins, and dual antiplatelet therapy, patient outcomes have substantially improved, and baseline event rates have markedly declined.3,27,28 Recent meta-analyses focusing on populations with preserved LVEF similarly indicate that the survival benefit signal for beta-blockers has significantly attenuated or disappeared; weak trends observed in observational data failed to translate into statistically significant benefit in randomized trials or after adjusting for heterogeneity.16–18 In this context, the present study is important because it is based exclusively on contemporary randomized evidence and therefore provides a less confounded estimate of the average treatment effect in current practice.
Critically, a recently published individual patient data meta-analysis provides an important framework for interpreting our overall neutral findings. It demonstrated that beta-blocker therapy significantly reduced the risk of the primary composite endpoint in patients with an LVEF of 40–49%. 19 This observation does not necessarily conflict with our results; rather, it suggests that considering patients with LVEF ≥40% as a homogeneous population may obscure clinically relevant heterogeneity in treatment response. In our study-level meta-analysis, patients with mildly reduced EF were pooled together with those with LVEF ≥50%, and this broader grouping may have diluted a benefit that is concentrated in the 40–49% subgroup. Because our analysis was based on aggregate trial-level data, we were unable to directly test treatment-by-EF interactions at the individual-patient level. Accordingly, our pooled estimate should be interpreted as the average effect across a mixed LVEF ≥40% population, rather than as direct evidence against benefit in the mildly reduced EF subgroup.
This pooled neutral estimate reflects an integration of seemingly contradictory signals from the five contemporary RCTs. Neutral primary outcomes from the REBOOT, REDUCE-AMI, and CAPITAL-RCT trials constitute the foundation of the overall estimate.11,14,15 However, the positive findings from the BETAMI-DANBLOCK trial and the potential risks associated with beta-blocker discontinuation observed in ABYSS suggest important underlying heterogeneity.12,13 Therefore, a more detailed analysis of the overall findings is essential to identify potential effect modifiers and beneficiary subgroups, prompting the exploration of our pre-specified drug-class subgroups and sensitivity analyses.
The pre-specified subgroup analysis suggested heterogeneity among beta-blockers: bisoprolol showed a neutral effect, metoprolol was associated with a significant reduction in the primary endpoint, and carvedilol showed a non-significant trend toward benefit. These differences are unlikely to be explained solely by source-trial populations and probably reflect a combination of pharmacological distinctions, EF distribution, and trial design. Metoprolol and bisoprolol are both β1-selective antagonists, whereas carvedilol is a non-selective beta-blocker with additional α1-blocking and antioxidant properties.29,30 These pharmacological differences may influence afterload, myocardial perfusion, and ventricular remodeling,29,31,32 although available comparative evidence does not support a simple conclusion that one agent is uniformly superior to another after MI. 33
Within our dataset, the apparent benefit observed with metoprolol should be interpreted cautiously, because it was driven predominantly by the BETAMI-DANBLOCK trial. 12 This is notable in light of the recent IPD meta-analysis showing that benefit may be concentrated in patients with LVEF 40–49%. 19 By contrast, the “neutral” effect observed with bisoprolol was primarily driven by the REBOOT and REDUCE-AMI trials, both of which enrolled lower-risk populations characterized by higher LVEF thresholds (>40% or ≥50%) and individually reported neutral findings.11,14 These results suggest that in contemporary, revascularized, low-risk patients with well-preserved LVEF, the additional benefit of long-term β1-selective blockade may be limited.
For carvedilol, our findings are best interpreted as hypothesis-generating. A post-hoc analysis of the CAPITAL-RCT supports a possible benefit in patients with mildly reduced LVEF (41–55%),15,31 and the direction of effect in our pooled analysis is also broadly consistent with the benefit observed in the CAPRICORN trial, which enrolled patients with left ventricular dysfunction. 34 However, the confidence intervals were wide, and the number of carvedilol-treated patients was relatively small. Accordingly, carvedilol should be described as showing a non-significant trend toward benefit rather than the “greatest magnitude of benefit.” Overall, these findings suggest that beta-blockers should not be regarded as a fully homogeneous therapeutic class, and that future studies should more carefully evaluate agent-specific effects within prespecified EF-defined subgroups. 35
Leave-one-out sensitivity analysis revealed that excluding the REBOOT trial rendered the beta-blocker effect statistically significant and eliminated heterogeneity (I2 = 0%), identifying REBOOT as the primary source of the overall heterogeneity and the neutral pooled result. This trial exerted disproportionate influence not only because of its large sample size, but also because it enrolled a pivotal contemporary low-risk population and was dominated by bisoprolol exposure, with substantial crossover that may have diluted any true treatment effect. 11 Once REBOOT was excluded, the favorable signal from BETAMI-DANBLOCK became more apparent, 12 further supporting the view that the pooled neutral estimate is highly sensitive to differences in trial design and patient selection.
To further investigate sources of heterogeneity, a meta-regression was performed on several study-level covariates, with a focus on evaluating the potential influence of RAAS-related factors. The covariates included age, proportion of females, primary PCI rate, prevalence of hypertension and diabetes, and usage rates of ACEI/ARB and CCB. The results showed that none of these factors significantly modified the treatment effect of beta-blockers on the primary composite endpoint.
This null finding is informative. It suggests that the overall neutral effect is unlikely to be explained simply by differences in major baseline characteristics or background pharmacotherapy. More importantly, it may reflect a defining feature of contemporary post-MI care: the widespread and standardized use of RAAS inhibition as foundational neurohormonal blockade. Under such conditions, convergence in background therapy across trials may reduce the ability of study-level analyses to detect any incremental benefit of beta-blockers using aggregate data. 36 Future IPD-based analyses would therefore be valuable for clarifying whether these apparently negative interaction analyses conceal true patient-level effect modification.
A non-significant trend toward increased stroke risk was observed with beta-blockers, consistent with findings from other studies. 19 The underlying mechanism may involve hemodynamic effects that reduce cerebral perfusion. 37 A large observational study from the NCDR registry also found beta-blocker use was not associated with lower stroke risk in heart failure patients with preserved EF. 38 However, no RCT evidence confirms a significant association, suggesting this finding is likely due to chance or residual confounding. Nevertheless, because stroke remains a clinically meaningful safety outcome, continued monitoring in higher-risk populations appears warranted.
Through meta-analysis and trial sequential analysis of randomized controlled trials, we obtained robust evidence showing that universal long-term beta-blocker therapy does not significantly improve composite outcomes in MI patients with LVEF ≥40%. However, these results should not be interpreted as evidence against beta-blockers in all such patients. Rather, they challenge the current “one-size-fits-all” prescribing model and support a more individualized approach. Beta-blockers should remain indicated for patients with clear clinical indications such as heart failure with reduced ejection fraction (HFrEF) or arrhythmias. 9 For patients without strong indications, the priority for future research is to determine which EF range, clinical profile, and beta-blocker type are most likely to derive net benefit. TSA findings suggest that while a large treatment effect (RRR of 20%) is unlikely, the current evidence is still underpowered to exclude more modest effects (RRR of 10–15%). These results underscore the importance of interpreting non-significant findings with caution, particularly when the accumulated sample size is insufficient under more conservative assumptions. This will require prespecified EF-stratified analyses or dedicated trials that distinguish patients with LVEF 40–49% from those with LVEF ≥50%, and that more directly compare different beta-blocker agents. Such work would provide a stronger basis for precision therapy and for more nuanced guideline recommendations.
Several limitations should be acknowledged in this analysis. First, a key limitation of this study is the inability to perform stratified analyses according to LVEF categories (e.g., 40–49% vs ≥50%) due to the use of aggregate study-level data. Furthermore, variations in LVEF inclusion thresholds across trials (≥40% vs ≥50%) may have introduced clinical heterogeneity and limited the ability to assess differential treatment effects across LVEF strata. Second, combining trials of ‘de novo initiation’ and ‘discontinuation’ introduces inherent conceptual limitations, although sensitivity analyses confirmed the robustness of our findings. Second, the open-label design of most trials and crossover use of medications may introduce bias and attenuate true effects, potentially leading to underestimation of benefits or harms. Third, variation in beta-blocker types and dosing limits conclusions regarding a class effect or dose-response relationship, although it provides a real-world perspective. Fourth, the inability to directly compare LVEF ≥50% versus 40–49% subgroups, coupled with low event counts in other subgroups, renders all subgroup findings exploratory. Fifth, the meta-regression was based on study-level covariates and therefore cannot exclude unmeasured patient-level confounding or true effect modification, particularly for variables such as background neurohormonal therapy, treatment intensity, and temporal changes in ventricular function. Finally, low baseline event rates hinder detection of small yet potentially clinically meaningful risk reductions, necessitating larger sample sizes or extended follow-up.
Conclusion
In patients with myocardial infarction and preserved or non-reduced ejection fraction, beta-blocker therapy did not significantly reduce the risk of composite or individual clinical outcomes compared with no beta-blocker use. A signal favoring metoprolol was observed in subgroup analysis, but this finding was driven largely by one major trial and should therefore be regarded as hypothesis-generating rather than definitive evidence of agent-specific superiority.
Supplemental Material
sj-docx-1-jra-10.1177_14703203261466278 - Supplemental material for Beta-blockers after myocardial infarction with preserved ejection fraction: A meta-analysis with trial sequential analysis
Supplemental material, sj-docx-1-jra-10.1177_14703203261466278 for Beta-blockers after myocardial infarction with preserved ejection fraction: A meta-analysis with trial sequential analysis by Qingchun Song, Zilong Zheng, Xiaokang Tu, Haoyu Tan, Qinwei Tang and Chengming Fan in Journal of the Renin-Angiotensin-Aldosterone System
Footnotes
Acknowledgements
Everyone who contributed significantly to the work has been listed.
List of abbreviations
Ethical considerations and consent to participate
Not applicable.
Consent for publication
Not applicable.
Author's contributions
CF is the corresponding author. QS, ZZ and CF had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: QS, ZZ and CF. Acquisition and interpretation of data: QS, ZZ, QT and XT. Statistical analysis: QS, XT, HT and CF. Drafting of the manuscript: QS, ZZ, XT and QT. Critical revision of the manuscript for important intellectual content: QS, ZZ and CF. Study supervision: QS and CF. All authors have read, provided critical feedback on intellectual content and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Hunan Provincial Health High-Level Talent Scientific Research Project (R2023017 to CF), and the Natural Science Foundation of Hunan Province (2026JJ20069 to CF).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
Transparency
The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.