
Abstract
Patients seeking medical care are traveling greater distances for treatment. The globalization of health care has given rise to a thriving global medical services industry. The ability to gain access to more advanced treatments and differences in cost and inflexible national health care systems encourage patients to seek treatment abroad. In the new information age, patients seek information about available treatment opportunities with less regard to national boundaries. International hospitals are seeking new marketing strategies for their services. Today, much of the marketing takes place on the Internet, which is accelerating the internationalization of the medical services industry. This article presents a comparative and interpretative study. We have interpreted the market orientation and degree of specialization of hospitals in Singapore and in Sweden, which in turn are compared to leading hospitals in the United States. In this research, we present evidence of different approaches to medical tourism based on different organizational frameworks for the marketing of medical services to international patients. The study indicates that market orientation results in greater emphasis on superior service quality of health care. This in turn leads to the delivery of improved services to patients.
Keywords
Introduction
Health care is undergoing a process of internationalization, accelerated by information technology (IT) and new communications media. Growing numbers of patients are now seeking planned medical treatment in countries other than their home countries. This represents an export of a service and has led to what is called medical tourism. Medical tourism, defined as travel for the purpose of seeking elective health care (Reed, 2008), has rapidly become a prosperous industry. Our thesis is that increased market orientation can improve the service quality provided to patients. It is primarily, but not exclusively, the private hospitals that can increase their market orientation. International marketing, not least via the Internet, can increase the number of patients seeking international health care.
The aim of the study has been to comparatively interpret hospitals in different countries along two dimensions. We have chosen degree of market orientation and degree of specialization as factors distinguishing hospitals in different regions of the world. Furthermore, the study compares differences between public and private ownership regarding the level of service offered to patients. In this growing global industry, “people travel often long distances to overseas countries to obtain medical, dental and surgical care” (Connell, 2006). IT has an increasingly important role to play in the management and marketing of modern enterprises (Bates & Gawande, 2003; Bhunia, 2005; Borg, 1996, 2006, 2009). Previous research has underlined the role of IT within health care (Goh, Gao, & Agarwal, 2011; Lin, Lin, & Roan, 2012; Pai & Huang, 2011). Medical tourism is often coordinated and promoted through IT-based service solutions. These include logistics, networks, patient information, and Internet-based marketing.
The audience for our research are not only primarily scholars, hospital managers, and marketing managers but also medical service intermediaries, interpreters, physicians, nurses, and other medical staff that come in contact with international patients. These professional groups are essential to the expansion and internationalization of health care and medical tourism.
Reasons for growth in medical tourism
There are several reasons to explain the increase in medical tourism (Connell, 2013; García-Altés, 2005). The population in wealthy countries is aging, giving rise to a growing need for health care. Lifestyles are changing; people travel more and are increasingly prepared to demand treatment abroad. There are new destinations available to tourists, and medical tourism is a growing alternative to domestic consumption of hospital services. Health care systems are often overloaded and have long waiting lists and high costs. Finally, the new knowledge-oriented society is empowering patients who are more informed and able to search for treatment on the Internet. Medical tourism can be seen as both an opportunity and a challenge to existing national health systems (Borman, 2004).
An important reason for medical tourism is to obtain treatment rapidly, without having to wait for many months or even years for health care. Herrick (2007) sees three other vital categories for medical tourism having led to an emerging global competition in the health care industry. One category is patients from countries with limitations in advanced treatment traveling to countries providing more advanced treatment in a specific field. Another category is patients from rich countries saving money by traveling to low cost countries to be treated there. A third category is regions, such as the European Union, agreeing to treat each other’s patients.
Strategic options for the marketing of medical services
Organizations find themselves grappling with two related strategic activities. First, organizations need to formulate strategies to achieve their goals. Second, they will have to implement those strategies (Vorhies & Morgan, 2003). In addition, senior managers are faced with the problems of trade-offs between competing strategic initiatives (Rust, Lemon, & Zeithaml, 2004). The objective of strategy formulation and implementation is to find a strategic fit among many activities (Olson, Slater, & Hult, 2005). In our study of contrasting medical service systems, we have analyzed both strategy formulation and implementation. Hospital administrators may have lofty ideas about how to market their treatment alternatives but have little control over implementation, as medical services are closely tied to the activities of the individual medical service providers. Each team of physicians often has its own ideas about how to approach patients. Hospitals are developing more advanced websites and smartphone applications to interact with current and prospective patients. An essential part of the strategy is to develop a market-oriented interaction strategy and to offer highly specialized care.
Hospitals are often non-profit organizations, even in the United States, and these organizations regularly find a middle way in which to meet social needs without resorting to the profit motive of the private sector or the bureaucracy of the government sector (Kotler, 1979). Health care providers are increasingly focusing on the customer needs of the patient and thereby becoming more market-oriented (Bhuian, Bulent, & Bell, 2005). This in turn increases the administrative cost of health care. An effective strategy which includes a pricing strategy takes into consideration the increased cost of internationalization. In the United States, public hospitals had 22.9% in administrative costs, while private hospitals, which are likely to pay more attention to customer demands, had an astonishing 34.0% in administrative costs (Woolhandler & Himmelstein, 1997). By comparison, figures for Europe and Asia are between 5% and 10% administrative costs. Greater market orientation together with a wider definition of the needs of patients is likely to increase overall administrative costs associated with treatment. In general, international patients generate more administrative costs than local patients. International patients need more help at hospitals with activities such as translation, accommodation, and transportation. These services are supplied at the destination where patients seek care.
International destination branding in medical tourism
Medical tourism destinations are being marketed as places where patients receive high-quality treatment while also having access to amenities and services such as interpreters and concierge services. Destinations seeking to attract international patients have a tendency to focus on the augmented needs of patients. This is often achieved through destination branding.
Treatment destination plays an important role in the marketing of medical services. Treatment opportunities can be marketed using destination marketing. Medical tourism can be promoted by the use of destination branding, which can be conveyed through Internet-based communication. The destination, region or city where the medical treatment is to be provided, can be branded in conjunction with the hospital that performs the treatment. A place is usually branded together with a slogan (Pike, 2005). Branding can be used in connection with various geographical entities ranging from countries and towns, and it identifies stakeholder engagement from organizations other than the one delivering the service (Hanna & Rowley, 2008).
Branding a destination as a place in which to obtain medical treatment indicates that the city or region is engaged in making the treatment a valuable alternative for the patient. Many destinations have developed logos in line with their destination management organization (Blain, Levy, & Brent Ritchie, 2005). This logo can be used by the individual organizations that are located at the same destination. A partnership between the stakeholders involved in the destination branding is seen as crucial to the success of the brand (Morgan, Pritchard, & Piggott, 2003). Disease is closely associated with fear and insecurity, thus influencing our feelings, attitude, and behavior. Holiday and spare-time activities are positively loaded phenomena. The right combination can influence the treatment in a positive way. Trust, confidence, and reliance with regard to the destination are strengthened by a structure and organization featuring an individual, empathic approach and acceptance. To win such confidence, communication and language are of interest in this context. Confidence in the organization and the individuals providing treatment is required by those prepared to undergo medical treatment abroad. A cornerstone of trust is a readiness to communicate with the medical care provider’s staff, and a fundamental requirement for this is finding a common language, if possible the mother tongue of the patient. It is also for this reason that so many hospitals in a large number of countries use a language or interpreter service to assist their patients. Most websites of hospitals that offer treatment to international patients have web pages in different languages. It is essential that patients can receive information online that they are able to understand and relate to. The second stage of an international online strategy is therefore to communicate in the patient’s mother tongue and to translate all relevant information about the patient’s treatment into a language that the patient can understand.
Methodology
In this study, we have conducted a comparative, qualitative study consisting of two fundamental dimensions to our empirical material. We have chosen an interpretative research paradigm, as this enables richness, nuances, and depth regarding the understanding and description of the phenomenon we are studying. Constructivist and interpretivist theory suggests that to understand our world of meaning, we have to interpret it (Schwandt, 1998, p. 26). Furthermore, Denzin and Lincoln (1998) argue that all research is interpretative. This claim has merit, in particular in connection with the analysis and concluding part of a study. However, interpretation is not always the dominating element in all kinds of research. Our research is interpretative when it comes to interpreting and understanding what the dominant direction is concerning how patients are perceived and the way of working in the hospital. Thus, our article examines whether there is a predominantly market-oriented or production-oriented view and whether it is mostly routine-based standard economies-of-scale thinking or a more specialized and tailor-made philosophy that prevails regarding the practical treatments provided for patients.
Since several hospitals are included in this study, it also includes a comparative component. Comparative research design uses almost identical methods to compare two or more cases, with cross-cultural studies being an obvious example (Bryman & Bell, 2013). Silverman (2000, p. 85) argues, “Comparative method is the basic scientific method”. We are therefore combining these two fundamental approaches into our method, thereby obtaining a comparative interpretative study. Our methodology involves semi-structured interviews conducted between May 2013 and September 2014, and parallel interviews and observations made on-site in Stockholm, Singapore, Bangkok, Boston, New York, Baltimore, Washington, and Rochester (Minnesota). Over this time span, several interviews were conducted in Stockholm. More specifically, interviews in Singapore were conducted in May 2013 and July 2014, in Bangkok in July 2014, and in the United States in November 2013 and September 2014. The principal interviewees and informants were hospital managers, physicians, researchers, and consultants.
Market orientation or production orientation
An efficient medical care provider should provide as much care as possible for the limited resources available. In economic terms, this is strongly related to the profitability of the company. Profitability is an essential goal in a market-oriented company. However, a lot of hospitals and medical care providers are publicly owned or non-profit organizations, and do not therefore have profitability as an objective. How does this affect the relationship between the patient and the medical care provider’s personnel? What are the implications for private hospitals pursuing a more market-oriented path compared to a more production-oriented medical care provision from major publicly owned hospitals?
It could be expected that a market-oriented medical care provider would be more likely to put considerably greater effort into building up good relationships with patients, giving them an advantage that puts them ahead of the more production-oriented public hospitals—and that it would be more accustomed to doing so. This is an assumption however. To answer these questions, we will consider what market orientation means and what its implications are in the countries studied here, Sweden and Singapore.
A market-oriented strategy has long been considered to be associated with improved economic outcomes (Day, 1990, 1992; Deshpande & Webster, 1989; Narver & Slater, 1990; Shapiro, 1988), and a significant relationship between market orientation and business performance has been established (Deshpande, Farley, & Webster, 1993; Jaworski & Kohli, 1993; Slater & Narver, 1994). The marketers of medical services in Singapore have long been able to actively market their services internationally, while their counterparts in Stockholm have been more reluctant to adopt a market-oriented approach and have instead been dominated by a production orientation.
The contrast between market orientation and production orientation can be related to research that has been conducted on the impact of private or public ownership of hospitals. However, market orientation is not exclusively associated with private hospitals, with public hospitals also attempting to apply a more market-oriented approach. The not-for-profit hospitals have a large market share even in the United States (Pauly, 1987). It has been found that hospitals that do not have an explicit profit motive are able to pursue goals other than cost minimization (Register & Bruning, 1987). Public or not-for-profit hospitals may have more freedom to choose output specifications and to choose less profit-oriented measurements of their output (Magnussen, 1996). Public hospitals may, for instance, when adopting a production orientation, maximize a different definition of utility (Lee, 1971). Within health care, improved utility can be defined as the output of care, such as increasing survival rates, higher quality of life, and other successful treatment outcomes. In other words, differences in ownership may lead to differences in best practice objectives (Grosskopf & Valdmanis, 1987).
Market orientation with a customer focus
In comparisons between private and public hospitals, differences in five service dimensions were studied: empathy, tangibles, assurance, timeliness, and responsiveness. The study shows that private hospitals score higher in these service dimensions than public hospitals (Irfan & Ijaz, 2011). A similar study looked at the service dimensions of empathy, tangibles, reliability, administrative responsiveness, and supporting skills, with ownership playing a less significant role in determining patients’ perceived service quality (Jabnoun & Chaker, 2003).
According to Sharp (1991), in a market-oriented perspective, the customer is put at the very top of the organization chart, whereas both the company and the customer are given the same weight in a production orientation perspective. Furthermore, for market orientation to achieve its strategic goals, its markets have to be well chosen and the productive capabilities well managed. Market orientation has evolved as a response to the shortcomings of a production and sales orientation. Sharp (1991) finally argues for a balanced and holistic development with respect to both customers and production.
Medical tourism is in many ways related to specialization, focusing on a number of specific treatment areas, thereby limiting their potential markets. This choice of care provider in a few specific areas has also been confirmed in interviews we have conducted with executives of other Swedish care providers working outside the Stockholm area. Among the people requiring the kind of treatment provided by the clinic, it would be possible to target the group that can afford it by virtue of their insurance policies or by paying privately upfront. At the same time, patients’ demands in terms of services, as well as other factors such as differences in culture and geographical distances, would be considered. This could further limit the targeted market.
Narver and Slater (1990) maintain that an organization has to create sustainable value for its customer, giving it a competitive advantage. They argue that the market orientation entails two criteria: long-term orientation and profitability, and also three components. The first component is customer orientation, that is, understanding the customer’s entire current and future value chain. The second component is competitor orientation: understanding the current strengths and weaknesses, as well as the strategies and long-term capabilities, of current and future competitors. The third component is inter-functional coordination using the company’s resources in such a way as to create superior value for its customers. Narver and Slater (1990) find that for both commodity and non-commodity businesses, market orientation, and market growth are important for profitability.
By its very nature, medical care is in many ways long term, starting with patient reception, through surgery, to aftercare, while also seeking to cure or improve the patient’s health. This long-term orientation probably applies to both market-oriented private clinics and publicly owned hospitals. The customer’s value chain corresponds in many ways to the patient’s medical care chain, which has to be well understood by the medical care provider. Both private and public hospitals will probably have to look much more closely than before at how global competition evolves. In addition, medical care providers also have to focus their resources on a number of specific areas in which they have the personnel, traditions, equipment, and facilities that allow them to excel.
A classical view of market orientation
Kohli and Jaworski (1990) provide the following definition of market orientation: “Market orientation is the organisation-wide generation of market intelligence pertaining to current and future customer needs, dissemination of the intelligence across departments, and organisation-wide responsiveness to it.” It is thus a question of gathering, distributing, and managing information about customers. To be market-oriented as a company or an organization requires an emphasis on being very well informed about what is going on in the market. That might seem obvious, but they also present some interesting findings regarding when market orientation might not be so advantageous. They found that, although market orientation is profitable in general, under conditions featuring limited competition, stable market preferences, booming economies, and technology turbulent industries, there might not be a strong relation between market orientation and commercial profit.
On the other hand, Kohli and Jaworski (1990) come up with many other findings. To strengthen market orientation, their interviews with executives suggest that close coordination between top managers in their communication about market orientation is vital, as is low-risk aversion and a positive attitude toward change. They also argue that there is a correlation between greater interdepartmental connectedness within the company, greater interest in ideas from other departments, greater reliance on market-based factors for evaluating and rewarding managers, and the ability of top marketing managers to convince top managers in other departments on one hand, and greater market orientation on the other hand. Furthermore, they find that greater market orientation of an organization is reflected in better business performance, and better employee job satisfaction and organizational commitment. Customer satisfaction is also greater, as is repeat business from customers. The greater the competition and market turbulence, the stronger the relationship between market orientation and business performance; the weaker the general economy and the greater the market turbulence, the stronger the relationship between market orientation and business performance. Thus, there are many arguments for the advantages of market orientation when running a company, but how do these arguments fit in with running a hospital where the patient is the customer?
Comparisons of hospitals in different countries
We have found that, in Sweden, a national or even an intra-national or regional view of medical care has prevailed and dominated, with little competition and with rather stable patient preferences strengthening production orientation in medical care. This is largely due to the fact that regional authorities are responsible for medical care, with the municipalities taking care of elderly people in geriatric care facilities. However, we argue that the development of worldwide medical tourism brings in more and more marketing thinking with a global competitive market, forcing hospitals to adapt to a new situation if they want to survive and prosper in the future. Furthermore, the demographic development, with an aging population in many countries around the world and highly indebted states, calls for a combination of creative solutions and efficient management. This requires a sensitive ear to patients, personnel, and society at large. Consideration of the benefits of market orientation as listed above has drawn us to conclude that more market-oriented management, focusing on patients and their needs while being creative and cost-efficient, could be a fruitful path to choose for the future of medical care.
From this more general and global outlook, we have focused on medical care in the two main cities selected for our study. A major difference between Stockholm and Singapore in terms of the treatment of international patients is the level of market orientation that prevails in the two systems. Singapore is far more market-oriented when it comes to medical tourism.
At the same time, there is a difference between Karolinska University Hospital, co-located with the Karolinska Institute in Stockholm, and the hospitals in Singapore. The Karolinska complex in Stockholm is far more research-intensive, while the Singapore hospitals mass-produce more routine procedures. The differences can be summed up in the following two-column matrices, starting with the theoretical matrix (see Figure 1).
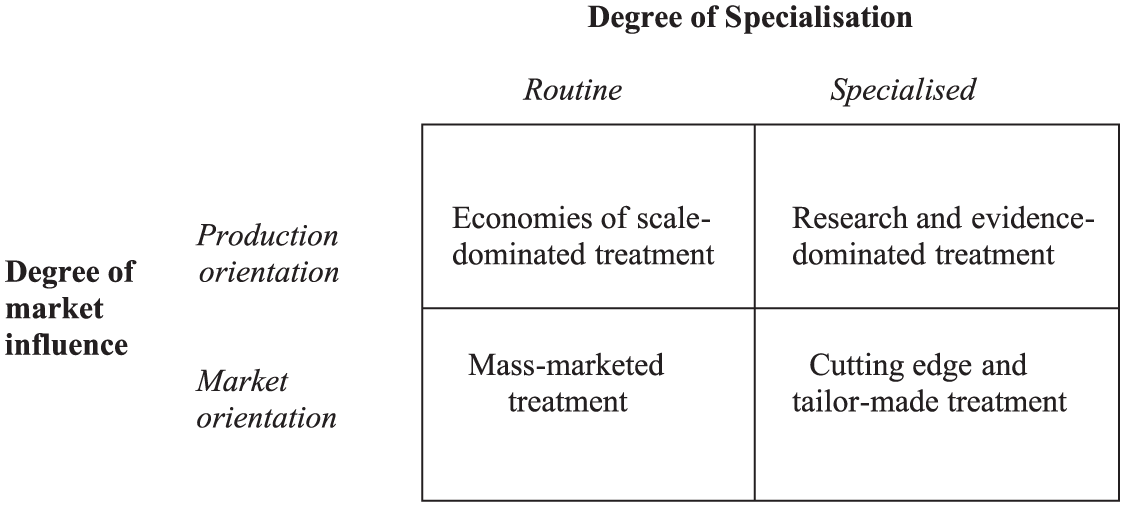
A theoretical matrix: describing the degree of market orientation and degree of specialization in medical care.
If we apply the above model to two hospitals in Sweden, Karolinska University Hospital and another major, though less research-oriented hospital in Stockholm, Södersjukhuset (The Southern Hospital), and to Singapore and the United States, represented here by two of its top US hospitals, the Mayo Clinic in Rochester, Minnesota and Johns Hopkins in Baltimore, we obtain the model shown below. In this matrix, we see how some hospitals are arranged in terms of the degree of market influence and their degree of specialization (see Figure 2).
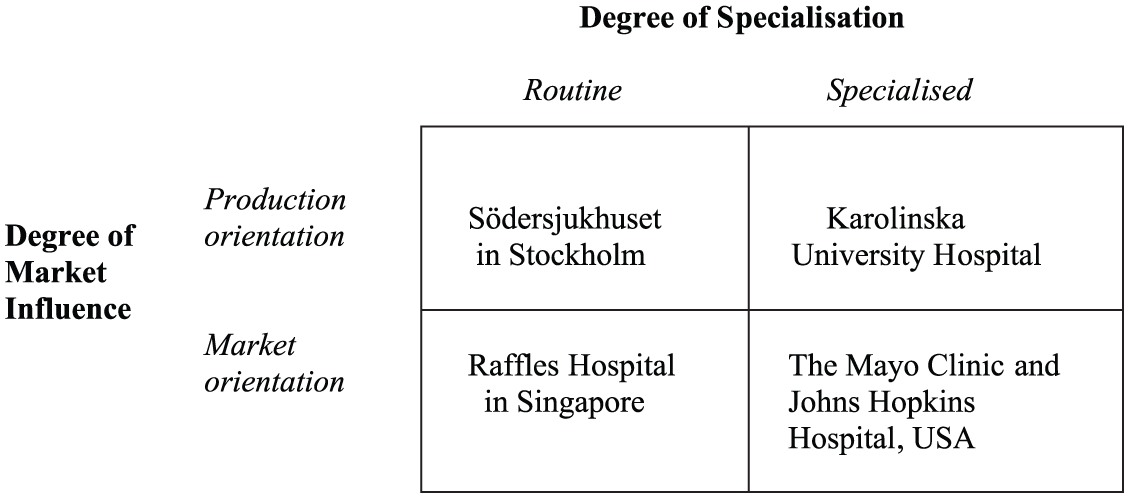
An empirical matrix: describing market orientation and specialization in medical care in selected hospitals in Sweden, Singapore, and the United States.
This matrix is somewhat nuanced, however. The least market-oriented hospital in the above matrix is Södersjukhuset in Stockholm, while Raffles Hospital in Singapore is the most market-oriented of the hospitals in this study. The two matrices can be viewed in light of the context of the subtle differences between the study objects.
Medical tourism in Singapore
Singapore is a significant hub for medical patients and a center for medical treatment in Asia. According to Bloomberg (2014), Singapore has the most efficient health care system in the world. In the same rating, Sweden is ranked 19 and the United States 44 out of 51 countries. Highly advanced medical care at competitive prices is provided in the city state, where medical tourism is booming. Singapore is a preferred destination for patients from all over Asia, as well as from all over the world. Prices for treatment are higher than those of India, Thailand, and Malaysia, but at the same time almost half of those in the United States. Singapore therefore competes with the United States on price and geographic closeness to Asian markets, and on better quality of health care with many other Asian countries.
Health care for non-residents is provided at about 20 different public and private hospitals. The Singapore government is heavily engaged in promoting incoming international patients. Singapore regards medical tourism as a means of increasing the overall standard of health care and minimizing differences between public and private health care (Leng, 2010). Although private hospitals dominate this market, many of the public hospitals have liaison offices that deal with international patients. Singapore has an infrastructure that is well-suited to handling traveling patients. The Changi Singapore airport, which is rated number 1 in the world, is a large Asian air travel hub, with flights from over 220 cities and from 60 nations around the world. Singapore is located in a small geographical area and all hospitals are easily reached from the airport. The city state is known for being well organized and clean. Heavy fines are issued for littering and other types of misbehavior.
The Singapore health care industry is encouraged by the national government to grow and to take in more international patients, while the government tightly regulates the industry. Before a hospital can be opened, a license must first be obtained from the government, which then continuously monitors the quality of the activities provided by the hospital. The way in which medical treatment is marketed is subject to strict regulations that have recently been tightened.
Two hospital clinics in Singapore: Raffles Hospital and Johns Hopkins Hospital
To look more closely at health care facilities in Singapore, we have studied two hospitals and conducted interviews at these two sites. Raffles Hospital, which is the largest private hospital in Singapore, was opened more than 30 years ago. Today, about half of the patients come from abroad. The hospital covers all major medical specialties and is housed in modern facilities centrally located in downtown Singapore. Raffles has a modern website which provides patients with advanced information about the treatment options available at the various clinics. The hospital is accredited by the highly recognized Joint Commission International accreditation and is ISO 9001:2001 certified. Raffles Hospital is named after Sir Thomas Stamford Raffles, who established a British port in Singapore in 1819. Under British rule, Singapore grew in importance as a major port.
At Raffles Hospital, international patients are received and handled by a professional international service staff. The liaison officers speak several languages, including Arabic, Mandarin, English, Russian, and Vietnamese. All staff are particularly good English speakers, a skill that dates back to the time of British rule. Raffles Hospital has its own marketing department. Medical reports are regularly translated by the in-house staff. The aim of the staff is to become friends with the patients and establish long-term relationships. Many patients come back regularly for checkups and continuous treatment. Health screening is one of the main medical services that are offered. The support staff can help with accommodation and solve practical problems for patients. The hospital offers an airport pickup service and helps with apartment rentals. A prayer room is provided for religious patients, and a range of specialty foods such as Halal and vegetarian meals are available from the in-house kitchen.
The pricing of Raffle’s medical services is transparent. Patients and insurance companies know in advance what a standard medical procedure will cost, though the cost may vary with complications and other factors occurring during treatment. Prices can at times be higher for international than for local patients because they incur higher costs for extra services such as concierge services, airport pickup, interpreters, and special food menus. A so-called second opinion is offered at 125 Singapore dollars, which is about US$100. A follow-up is offered at US$70.
The hospital is dedicated to treatment only and does not conduct any research. Raffles Hospital is expanding rapidly and is currently building a new hospital wing. There is an emphasis on good testimonials from patients, and all patients are asked to fill in a detailed questionnaire at the end of their treatment. Word-of-mouth marketing is important and many patients are referred to the hospital by doctors in many other countries. The naming of the hospital after the icon Sir Thomas Stamford Raffles is an important marketing tool, which, along with being located in Singapore, helps to market the hospital. Singapore is known internationally and especially in Asia as a major medical hub and the home of first-class hospitals.
In contrast to Raffles Hospital, the Johns Hopkins Hospital’s joint venture in Singapore was established based on a joint research program between Singapore researchers and scientists at Johns Hopkins University in Baltimore in the United States. Johns Hopkins Singapore Hospital provides cancer treatment only. It is a recognized Asian center for oncology treatment, which attracts patients from all over the world. The Johns Hopkins name gives the hospital clinic a boost in its marketing efforts. In terms of destination branding, the Singapore location, together with its American affiliation, provides the hospital with effective marketing tools. The Johns Hopkins Singapore Hospital was first located in the National University Hospital in the 1990s, and it was here that the initial research cooperation was started. In 2005, the hospital needed more space and so it was relocated to the Tan Tock Seng public hospital. Being located within a larger hospital gives the Johns Hopkins clinic the opportunity to consult other specialties as required.
The medical service team of five people that receives international patients speaks Arabic, Russian, Mandarin, and English, which helps in communicating with foreign patients. All doctors at the clinic are assistant professors or above, which indicates a high level of competence among the medical staff. The hospital provides both inpatient and outpatient care. Most of the patients are insured and select this hospital for its good reputation in its field.
Stockholm Care
Stockholm Care, which was established in 1991, is a fully owned subsidiary of the regional government in Stockholm. The company is responsible for coordinating the hospital care of international patients who are treated at Stockholm’s four major hospitals or at several other associated clinics. Our research interviews show that Stockholm Care sees its primary market as being countries located within a 2-hr flight from Stockholm, but it also provides treatment for patients from further away. A major part of the marketing is Stockholm’s reputation as a center for medical research and treatment. It places emphasis on the famous Karolinska Institute, which selects the winner of the annual Nobel Prize in medicine via the Nobel Assembly.
The health care provided through Stockholm Care is normally priced on completion of the treatment. However, patients are expected to pay part of the treatment cost in advance. Stockholm Care cooperates with insurance companies to collect payment for treatment provided. A preliminary treatment plan and an estimated cost of treatment can be provided. The clinics associated with Stockholm Care can provide a second opinion, and the price for this can be deducted from the hospital bill if the patient chooses to be treated in Stockholm. Before the treatment is started, medical records that are as complete as possible are first obtained and translated. The information is transferred to the clinic that is treating the patient. A total of about five people are in charge of the reception of all patients from abroad and who are treated at all hospitals in the Stockholm region. When patients need to communicate in languages other than English and Swedish, interpreters are used.
Differences and similarities between Stockholm and Singapore
A major difference between Stockholm and Singapore is that Stockholm is situated within a not-for-profit health care system. In Stockholm, it is not so common, therefore, for hospitals to accept patients who pay for the treatment they receive. Politically, this paid-for treatment is controversial and several political parties have been skeptical about private money entering into medical care. At the same time, of hospitals has taken place privatization of hospitals taken place. And Sweden is home to the international private medical company Capio, which is another care provider we have interviewed. Capio, however, receives public funding for the medical treatment they provide. Profitable companies in the health care sector are thriving in Stockholm but are not particularly encouraged by the government. Stockholm Care works under a regional government that sets objectives for its profitability but not for its future growth. Swecare is a rather small networking industry organization that encourages growth among companies in the life sciences sector and in incoming medical tourism to Sweden.
The Singapore hospitals, in contrast to those in Stockholm, are well established within a private for-profit economic context. Expansion of the medical services industry is strongly encouraged by the Singapore government and there is strong annual growth. The government regulates the industry and stipulates rules for how it operates and how it markets its medical services. Singapore has both private and public hospitals that all participate in the medical tourism industry. The public hospitals, however, focus more on meeting the needs of the local population and receive substantially fewer international patients.
With both Singapore and Stockholm, the location plays a major role in the marketing of medical services. Having a good general reputation as a location for medical services is an asset. Fewer patients want to travel to a country or city that does not have a hospital sector with a good general reputation. The city name combined with a hospital brand, such as Karolinska University Hospital or Johns Hopkins Hospital, helps to market the medical treatment provided by these hospitals.
Both Singapore and Stockholm have access to advanced computer services, and much of the destination marketing is done via the Internet. Patients seeking information about treatment options increasingly use electronic media to obtain more information. Web-based information is a major source of the globalization of the medical services industry. Patients are not stopping at obtaining information about the local hospital when seeking treatment, and searching the Internet produces a more complete picture of different alternatives and the costs of various treatments. People who are sick are vulnerable and are likely to grasp the last straw when faced with a complicated diagnosis. As a result, patients are willing to travel long distances to seek treatment when the local alternative is not seen as a sufficiently good alternative.
Concluding remarks
Stockholm and Singapore both have credibility as medical tourism destinations, and both can build on this in their destination branding for medical tourism. However, they differ in their marketing strategies. The Stockholm hospitals are more conservative and production-oriented, while the Singapore hospitals, particularly the private ones, are more responsive to change and far more market-oriented toward international incoming patients. They also seem to have much stronger political support for this industry from their local political leaders. A market orientation entails a greater emphasis on the provision of superior service quality. A production orientation, on the other hand, can enable the hospital to define objectives for their provision of utilities to patients and to provide better health care for patients. Empirically, we have seen this in our comparative studies. As a consequence of their market orientation, Singapore hospitals place greater emphasis on service to patients, while Karolinska in Stockholm maximizes utility to patients. Both private and public hospitals can improve their level of service to patients through market orientation. Our two sets of figures show that both private and public hospitals can either be market- or production-oriented and focus either on specialized or routine treatment. Traditionally, private hospitals have been more market-oriented, but the development of international medical tourism also provides incentives for public hospitals to strengthen their market orientation.
Singapore has rapidly expanded its capacity as a health care provider and has built new modern hospital wings to accommodate a growing number of international patients. The hospitals are welcoming, with large lobbies and reception areas. The first impression is that the hospitals are advanced, clean, and efficient and they project a feeling of being in good hands. In contrast, the Stockholm hospitals are older and less modern. Many of the hospital buildings are from the 1970s or older and have less generously spaced reception areas. The hospital buildings are well maintained, but they do not project the high-tech and advanced medical care that they provide. An increased intake of international patients could finance an expansion and modernization of the hospitals in the Stockholm area. Stockholm, as a medical tourism destination, could benefit from an expansion of its medical services and competition for the approval of current and prospective international patients. In contrast, Singapore is able to expand and improve its hospital facilities and can welcome new patients to a constantly improving health care system. However, the strong research activities in Stockholm could give its hospitals a cutting edge if they became more market-oriented and the architecture were more welcoming, providing a warmer atmosphere with better and more advanced services for patients.
Sweden has many successful and large exporting companies, but the public sector is huge and with medical care at its core, especially in the minds of many politicians and a substantial part of the local population. Nevertheless, there are quite a lot of private hospitals and private physicians in Sweden. However, implementing a new strategy is never easy for an organization. Steering a hospital and its personnel from a clearly production-oriented to a more market-oriented approach therefore involves confronting many challenges and forces of inertia, both among politicians and personnel at the hospital, who, for ideological or practical reasons, might prefer to continue their current, more production-oriented approach. This is a potential obstacle to implementation of a stronger market orientation aimed at medical tourism patients coming to Sweden, with the occasionally long waiting lists for medical treatment for local patients potentially making the task of obtaining acceptance of such implementation even harder. In this respect, the hospitals in Singapore seem to be in a much more favorable position, having made much more progress in terms of the level of market orientation for incoming international patients.
Key findings
There is a rapid increase in the internationalization of medical care and movements of patients across national boundaries.
The national context plays an essential role in the organization of international health care.
When analyzing health care, it is essential to distinguish between routine and specialized care as well as production-oriented and market-oriented provisions of medical services.
Health care that adopts a stronger market orientation will be inclined to focus more on providing superior services to patients.
Stockholm and Singapore both feature advanced medical care, providing a credible basis as destinations for international patients. Private Singapore hospitals are more market-oriented, while Stockholm’s hospitals are more production-oriented.
Strong brands generated through attractive destinations and acclaimed hospitals play an important role when establishing competitive treatment alternatives for international patients.
Language proficiency in patients’ mother tongue among treatment and support personnel is a vital asset in international medical tourism. Multilingual Singapore has an edge in this respect.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Authors would like to thank the Knowledge Foundation for financial contributions to this research. Prior to this funding we are also thankful for funding from Ragnar Söderberg foundation, which enabled the initial research and international interviews.