
Abstract
New knowledge underpins calls for change in approaches to the care of people with dementia. Person-centred care is considered essential, whereas purpose-built facilities and environmental design are reported to enhance safety and to have a positive effect on behaviour. Research findings have highlighted the inappropriate use of antipsychotic drugs and there is debate about their value in ‘managing’ symptoms. This paper presents the combination of approaches used to enable residents of two secure dementia units to live life within their ability and without antipsychotic drugs. Essential to the success of the change process was staff education, knowledge of the person, a varied leisure activity programme and a supportive environment. Evidence of the positive difference these strategies made includes statistics that show a decline in falls and behavioural issues, and feedback from family members. In light of the evidence, this article posits that it is ethically wrong to give people with dementia antipsychotic medications because their behaviour is deemed to be unacceptable, when there are other viable options.
Introduction
This paper outlines the approaches and methods used to make a difference to the provision of care for people living with dementia in a long-term residential care facility. The most significant outcome of the change process, which evolved over a four-year period, was the elimination of antipsychotic drugs. The facility at the centre of this discussion, identified as Haven, enjoys a solid reputation for the quality of care it provides. Established to support frail older people, Haven is a non-profit charitable trust.
The decision to commit to a programme of change developed from knowledge gleaned from research literature reporting that the quality of care within residential facilities could be improved. Although service provision overall was compliant with the Ministry of Health requirements, the literature suggested that residents’ sense of well-being, and thus their quality of life, could be enhanced by using a combination of alternative approaches (Chung, 2004; Kitwood & Bredin, 1992; McGonigal-Kenney & Schutte, 2006; Zeisal, 2005). Undertaking a change process was in keeping with the commitment made by the founders of Haven to provide quality care services for older people. The changes under discussion refer specifically to two secure dementia units, each of which has 15 beds.
Changing perspectives
To bring about change in any organization is an enormous undertaking, especially when staff within the organization, are unaware of the need for change (Bate, 2000). When people are doing their best within their knowledge base, they can be reluctant to accept that what they are doing is not good enough. Viewed from this perspective, change implies something is wrong and therefore it becomes a criticism. Developing awareness of what is wrong, and what needs to change means moving people out of their comfort zone and into a new way of doing things.
Any change has to include all staff from management levels down, because if change is to succeed then the functional circles of influence within an organization have to be involved (Adamson, 2006). Everyone who will be included in the change process has to be drawn in so that they come to work feeling enthused and passionate. This more than anything else will impact positively on quality, safety and productivity, as team work forms the basis of good service provision and is validated and reinforced when passed on to new staff members (Bate, 2000). Interestingly, the change process under discussion adopted the methods of an action research project inasmuch as all staff within the units were involved and progress was monitored by way of an action, reflection and evaluation cycle. However, the project did not start out as a scientific study and so no claim is made under the auspices of research.
To begin with, time was spent observing the routines and practices within the units, before trying new ideas, reflecting on and evaluating the outcome, prior to moving on in still newer directions. Knowledge gleaned from literature, and new understandings gained from research done while travelling overseas was put into practice. That is to say, information on approaches to dementia care gathered from countries such as Scotland, England, Canada and the USA underpinned the project.
Staff training
The first task in the change process was to help staff to understand that in their daily interactions with residents they have the power to develop and improve each person's sense of well-being. By encouraging residents to do what they can for themselves during normal daily activities, staff can facilitate a sense of familiarity, competence and security. In theory, this approach purports that the ordinary and familiar things people do every day promotes and supports a sense of well-being (MacRae, 2007; Yerxa, 2002). In addition, teaching staff to see the person and not the disease (Kitwood, 1993) contributed to a change in the culture of care within the units.
A training programme aimed at increasing staff knowledge of dementia was also undertaken. Training involved a series of in-services run over a six-week period with topics such as: What is dementia? What is person-centred care? Understanding and responding to behaviour; Communicating with people with dementia; The influence of the environment; Developing a sense of well-being for people with dementia; and Nutrition. Participation was mandatory even though some staff felt they had worked with people with dementia for so long they did not need further training. As change is about moving people from the status quo and onto something different, it was necessary for all staff to learn a new way of ‘seeing’ and thus a new way of doing. To understand, that each interaction with a resident is an opportunity to make that person feel good, and to feel valued.
During the course of the change process the resident to staff ratio in the units was increased. That is to say, one staff member to five residents on the morning shift, one staff member to six residents during the afternoon shift, and two staff members overnight.
Person-centred care
By itself, training will not change care practices (Lintern, Woods, & Phair, 2000), and so the concept of person-centred care (Kitwood, 1997) was equally important to the process. The notion of person-centred care is highly regarded; however, it is often ill-defined (Nolan, Davies, Brown, Keady & Nolan, 2003). In this instance, a person-centred approach entailed gathering a detailed description of each resident's physical, mental and cognitive status. Furthermore, self-care habits, leisure interests, personal history, qualifications, productivity, spirituality, attitudinal, physical and social factors were all included in the initial occupational therapy assessment. This level of detail was deemed essential to increase staff awareness of the individuality of each resident. Moreover, these personal characteristics have significance for the ways in which dementia may be manifest. Therefore, this information was important to help staff get to know and understand each resident on a more personal basis.
This approach is endorsed by the World Health Organization's (WHO, 2001) International Classification of Functioning, Disability and Health (ICF) because it acknowledges that each person's characteristics, their personal history, values and interests will impact on their sense of well-being. Indeed, the ICF (WHO, 2001) views health as a dynamic interaction between participation, which concerns the things people do, contextual factors, health conditions and personal functioning. This philosophy endorses the principles of occupational therapy as both emphasize the influence of the environment, participation and activities, on function, health and disability.
An occupational perspective
In the belief that people have an innate need to engage in daily activities (Chung, 2004; Hasselkus, 1997; Öhman & Nygård, 2005), occupational therapists advocate that participating in activities promotes a sense of health and well-being (Wilcock, 2006). In keeping with this theory, opportunities for residents to participate in a range of occupations and/or leisure activities were increased. As the loss of opportunities to engage in daily occupations is associated with depression and declining abilities, the importance of a varied activity programme cannot be overstated (Borell, Gustavsson, Sandman, & Kielhofner, 1994; Warrington, 1996; Zeisal, 2005). Previously, the activity programme was random with options such as baking, reminiscing and word games facilitated on an ad hoc basis. In conjunction with improving staff knowledge, the programme was revamped to provide a greater selection of leisure activities designed to meet individual physical, cognitive, spiritual and social needs.
Academics from various disciplines endorse an occupational approach and studies have found that people eat better, sleep better, feel better and maintain better health when they engage in purposeful occupations (Clark, Jackson, & Carlson, 2004; Csikzentmihalyi, 2004; Glass, Mendes de Leon, Marottoli, & Berkman, 1999; Graff, Vernooij-Dassen, Thijssen, Dekker, Hoefnagels, et al. 2007; Loland, 2004). There is no valid reason to think that this does not apply to people with dementia.
When people enter residential care they lose many of the activities that make up daily routines and give life meaning (Godlove Mozley, 2001; Wood, Womack, & Hooper, 2009), for example cooking, cleaning and laundry are all done for them. Yet people need opportunities to keep their brain active, most especially people who are living with cognitive decline (Bryden, 2005; Clare & Woods, 2004; Taylor, 2007), they should not be left to stare aimlessly at the walls or be parked in front of a television. Science has found that when brain cells are appropriately stimulated, they can be retained (Coulson, Fox, McKenna, & Stathi, 2008). Accordingly, a good activity programme has three important factors: physical exercise, mental challenges and social activities (Gitlin et al., 2009; O'Sullivan, 2005).
Leisure activities
As no two human brains are exactly alike, no one challenge will adequately satisfy all people, and so the provision of a range of interesting activities is essential. For some, physical activity is satisfying; for others, finding and processing information is rewarding; for still more others, working with creative ideas is enjoyable. Regardless of the activity, it is the opportunity to engage and challenge the brain cells that is important (Jakobson Ramin, 2007).
Accordingly, the range and number of leisure activities in the units was increased over the course of the week. As well as group activities twice a day, Monday to Friday, an exercise class was run each morning and a walking group was encouraged late in the afternoon. Timed to start just before dinner, the walking group was intended to offset the occurrence of sundowning by giving residents something to do at the end of the day.
As residents live in a secure environment, outings into the community were deemed to be important to help them retain a sense of normality. For this reason, there were three outings from the units each week and those who were physically and cognitively able also enjoyed an occasional trip to the local coffee shop for morning or afternoon tea or coffee. Engaging people with dementia in activities serves many purposes (Gitlin et al., 2009; Wood et al., 2009). In this instance, leisure activities were used to maximise existing functional abilities, maintain social skills, build confidence and self-esteem, promote physical relaxation and manage agitated and/or restless behaviours.
The environment
Further to staff training and the activity programme, the person–occupation–environment ‘fit’ (Townsend et al., 1997) was taken into consideration. That is to say, the influence of the environment was also acknowledged. Until the final stages of dementia rob them of the ability to engage with their surroundings, people with dementia will either be helped or hindered by the environment in which they live (Marshall, 1998; Zeisal et al. 2003). The less competent the person, the more the environment can affect the way they feel and that in turn shapes their behaviour (Wood, 2005). Based on insights gained overseas, the two units were refurbished to make them less clinical and more comfortable. The previously locked doors between the units were opened and the single-storey layout made barrier-free, yet safe and secure. Other ‘security’ doors were unlocked wherever possible so that residents are free to wander both indoors and out.
Independent way finding was facilitated by visual cues and theme landmarks in the corridors. Bedroom doors were made visually distinctive with easy-to-read nameplates, photos and pictures of personal significance. Toilet doors were painted red and given a sign with two visual indicators, the word toilet in large black capitals and a picture of a toilet for easy identification. Small lounges were created and fitted with home-like furniture to produce a warm and inviting environment, with easy listening music playing softly in the background. A storage room was made into an arts-n-crafts centre because creative activities are an important part of the activity programme. Seating niches and theme nooks were added to offer a destination for restless residents.
Furthermore, places of interest include a nursery, complete with a selection of soft toys and a chest of drawers with baby clothes for folding. This familiar environment facilitates reminiscing and allows nurturing instincts. An unused cupboard was transformed into a sewing nook complete with treadle sewing machine, and sewing cabinet. With safety a key consideration, drawers and shelves contain fabric, threads, elastic and zips for residents to tinker with while a mannequin displays the current sewing creation. Another large cupboard was made into a sailing nook and furnished with a collection of yachts, a captain's chair and a desk complete with writing tools.
Sensory stimulation
Research indicated that a soothing, yet stimulating, multi sensory environment can be reassuring and so a Snoezelen room was created for people who are prone to anxiety (Baker et al., 2001; McGonigal-Kenney & Schutte, 2006); however, the room was not considered a success. Although one-to-one sensory intervention in the Snoezelen room was therapeutic with activity staff, those same interventions were successful in other areas of the units. What is more, when activity staff were not on duty, care staff did not always have time to engage with residents in the Snoezelen room. Eventually, it became apparent that residents seldom ventured into the room alone. Occasionally, some might stand at the door and look at the visual sensory stimulants, or perhaps listen to the sounds of nature playing on the sound system. The point is, with a decline in behavioural issues the room was considered ineffective and as a result it was replaced with a rummage room. Reminiscent of a second-hand shop, the room now contains age-appropriate memorabilia. Diverse pieces of furniture display all sorts of colourful bric-a-brac and pictures on the walls are an added interest. The residents appear to enjoy browsing and tinkering with the various bits and pieces, and, although the contents often go missing, they are not valuable. In due course, staff invariably find the missing ‘treasures’ and return them to the rummage room.
To be effective, the environment must promote independence not dependence with homeliness and normalization a key consideration (Marshall, 1998). The changes adopted in this project are innovative in their simplicity yet they have made a tremendous difference to residents, staff and family members. What is more, the combination of these approaches formed a framework to support the elimination of antipsychotic drugs.
Antipsychotic drugs
During the course of these changes the author came across literature warning of the inappropriate use of antipsychotic drugs to manage the behaviour of people with dementia (Aschenbrenner, 2005; Ballard & Howard, 2006; Banerjee, 2009; Fossey et al., 2006; U.S. Food and Drug Administration, 2005). Upon checking resident medications in the dementia units, it was found that nearly two-thirds were being given either risperidone or quetiapine. In most cases the drugs had been prescribed before the resident came into care, but in some instances antipsychotics had been prescribed because staff experienced difficulty in coping with resistant behaviours.
Reflecting on the literature prompted the question of how best to take heed of the warnings. With management support, the issue was raised during an interdisciplinary team meeting. In discussion, one GP indicated s/he wanted to see scientific evidence of the potential for negative side effects from antipsychotic drugs before agreeing to support the initiative. Consequently, a selection of research from prestigious universities was provided to enable an informed decision.
Family members were consulted during care reviews. This involved informing them of research findings that had raised concerns over the use of these drugs and asking why the drugs had originally been prescribed when the resident was at home. Responses were varied: to help the person sleep, to make him/her easier to manage or to help the caregiver to cope. In some instances the resident had been on the drugs for so long that their family did not know, or could not remember why the drugs had been prescribed (O'Sullivan, 2011). With family support, the consulting psychiatrist and/or general practitioner (GP) was asked to review residents who were being given these medications with a view towards gradually weaning them off the drugs.
To begin with, the drugs were withdrawn from residents on a low dosage and their behaviour was monitored over several weeks. Initially, some of the care staff were afraid of the potential consequences but when nothing untoward happened staff gradually became more confident. With the passage of time, both staff and family members began to notice a positive difference, and over the following 12–18 months the use of antipsychotic drugs was eliminated altogether (O'Sullivan, 2011). Eventually, when a new resident was admitted, their drug chart was automatically checked to see if antipsychotics had been prescribed. After a period of adjustment to allow time for the person to adapt to a new environment and equally, to allow staff to get to know the person, the need for these medications was reassessed by a psychiatrist or GP.
A positive difference
Eliminating the use of antipsychotic drugs was the most rewarding outcome of the change process because it made such an obvious difference to residents. People who came into the unit often commented on how alert and contented everyone looked. In addition, the residents were more cooperative, and interested in what was going on around them. What is more, families were very supportive of the proactive stance taken. In fact, one man's son specifically came in to voice his appreciation. He wanted staff to know that during a weekend visit, for the first time in over two years, he felt he had not only been able to connect with his father, but to have a conversation of sorts.
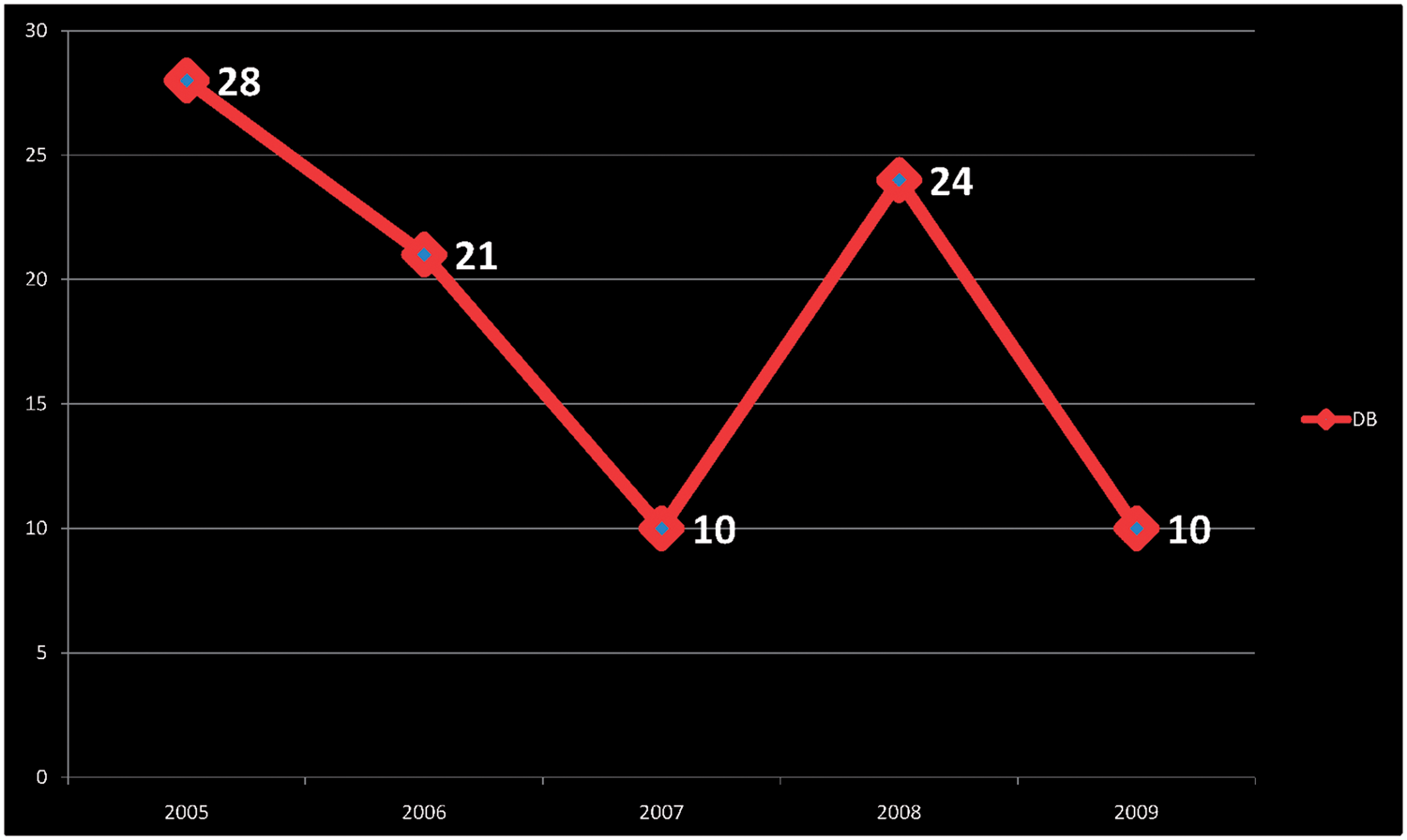
A further consequence of removing these specific drugs is the statistics, which show that the number of falls in the units went down by more than 50% from 123 falls to 55 falls in one year (see Figure 1). Those numbers stayed down, as the following year only 62 falls were recorded. Other positive outcomes from the overall change process include a decline in behaviour management issues (see Figure 2). An upsweep in 2007/2008 is connected to the admission of a resident who had been prescribed both risperidone and quetiapine prior to admission. Due to the unpredictable nature of this person's behaviour, other residents were deemed to be at risk and so the GP would not reduce the medications. In the interests of other residents’ safety, the person was eventually transferred to another facility. Following his/her departure, as shown in Figure 2, behavioural issues declined again.
Fall Statistics. Behavioural statistics.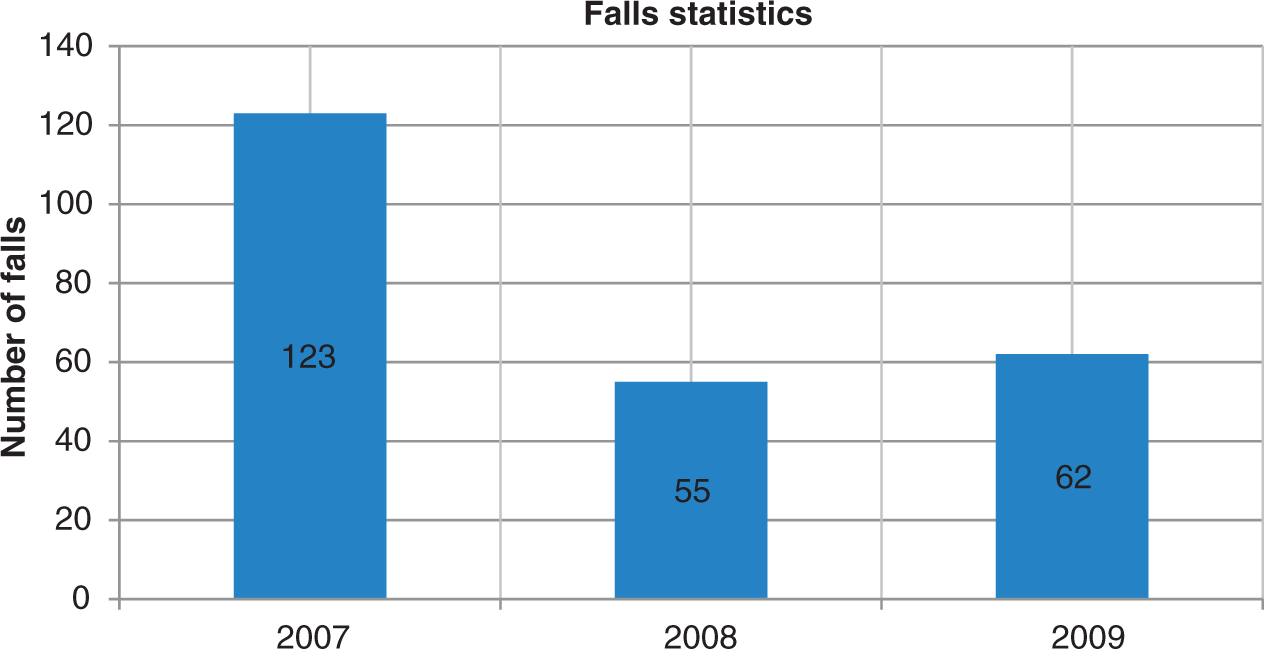
Family approval
Further evidence to support the change process came in the form of an email received from a family member approximately six months after the resident was admitted: Grace, I wanted to record both my, and my family’s appreciation for the professional guidance and the level of care that we have received for our mother … She was accepted into the Dementia Care ward in February of this year, after 3 years of care at another Rest Home … , and I have to say that the turnaround in her personality and behaviour has been unbelievable. While there are a number of factors at play in Mum’s improvement, my wife (who is a registered physiotherapist) and I put a large part of it down to your suggested regime of removing all drugs from her daily routine, apart from those required for specific physical care, such as pain relief. Mum has had a number of problems over the past 30+ years, including depression and alcoholism, some of them exacerbated by caring for our Dad as he suffered through three years of cancer treatment. While she was living in her own home … , and then in the Rest Home … , Mum was on a series of anti-psychotic drugs and other medicines. However, personal experience from regular visits, and feedback from my siblings, indicated that Mum was a rather unpleasant person to be with. She was forgetful, quite irrational, and frequently very rude, aggressive and hurtful. i.e., visits were a filial duty, rather than a family pleasure! However, since being weaned off all her drugs, she has once again become the Mum that I remember from my youth. Her wonderful sense of humour has returned, her enjoyment of her extended family is evident, and she is a joy to be with. She remains very forgetful, and has her share of physical problems still, but she is no longer the scornful and vindictive old woman that neither my wife nor my children would ever gladly visit. So thank you … for your approach to treating dementia patients. We are 100% sold on it! (O'Sullivan, 2011).
This feedback highlights the detrimental effects of antipsychotic drugs and, moreover, that drugs may actually exacerbate problems. Clearly, using these medications to manage the behaviour of people with dementia is ethically wrong.
Discussion
The goal of the change process presented in this article was to try and ensure residents live each day to the best of their ability and thus, achieve a sense of life satisfaction. Haven has come a long way towards achieving that goal. The steps taken and the resulting outcomes clearly show that much can be done to support people with dementia who live in residential care, to help them retain a sense of well-being and experience life satisfaction.
To ensure an optimum level of care and a strong team spirit, everyone from management levels down, or from grass roots up, has to be genuinely involved in a change process. Ongoing staff training and support is required to ensure standards of care are maintained. A person-centred approach enables staff to get to know unique personality traits and in this way to preserve each resident's sense of identity, dignity and self-respect. Equally, a varied activity programme provides opportunities for residents to engage in occupations and/or leisure activities of choice and to enjoy positive daily experiences. There is be no doubt that the impact of the physical and social environment can have a positive or negative influence on people with dementia. An unrestricted, albeit secure and homely environment, in which there is a general sense of safety, security and order, promotes a sense of autonomy.
Any one of the aforementioned interventions will go some way to improving resident's well-being, contentment and quality of life, but one intervention is not enough. It was the combination of approaches that was the real key to making a significant difference to the quality of care services provided in the two dementia units under discussion in this article. Eliminating the use of antipsychotics was an unexpected bonus, one that was highly praised by residents’ family members and others in the community.
Challenging the use of antipsychotic medications involved a degree of courage. This was offset by confidence in occupational therapy knowledge, management support, and understanding of dementia and the relational decline in functional ability. In the belief that many of the behavioural issues people with dementia exhibit stem from frustration and a sense of uselessness and/or incompetence, opportunities for engagement in occupation or activities are a cost-effective alternative to medications. Therefore, this article posits that ethically, it is very wrong to medicate people with dementia when alternative ways of treating the cause of behaviours are more appropriate and rewarding for all concerned.
Conclusion
This article has described a change process undertaken in two secure units within a residential care facility for people with dementia. It has reported the steps taken to improve the quality of care provision and the outstanding benefits for residents and their family, as well as staff. There can be no doubt that these alternative approaches to care offset the sometimes unpredictable behaviours of people with dementia and enhanced their life satisfaction. Therein lays a challenge for all residential facilities offering care services for people with dementia.
There have been numerous calls to improve standards of care for this vulnerable population of people and to stop the inappropriate use of antipsychotic medications. The combination of approaches outlined in this article proved to be an effective response to that call. I hope the course of action depicted will encourage others to adopt similar approaches.