
Abstract
Disordered sleep in persons with dementia is a contributing factor for a range of health problems. The evidence base for non-pharmacological interventions has not been evaluated and clearly presented in the literature. This paper provides a structured Critical Literature Review of the evidence for non-pharmacological interventions to reduce disordered sleep in persons with dementia. The systematic search retrieved 29 studies that were evaluated for methodological quality. The quality of evidence ranged from conclusive for light therapy and activity to inconclusive for most other interventions. There is a paucity of conclusive research for non-pharmacological sleep interventions for persons with dementia. Most of the evidence about effective interventions is anecdotal and untested. There is a need for rigorous scientific inquiry, coupled with tacit knowledge to build a strong evidence base on non-pharmacological interventions for disordered sleep for persons with dementia.
Keywords
Introduction
Although non-pharmacological interventions have been demonstrated to be effective for improving restorative sleep in older persons, there remains a prevalent belief that a decreased ability to sleep is a normal part of aging. As a result, people do not recognize sleep problems as treatable and do not seek help. Also, societal ageism, older adults’ denial of sleep problems, coexisting disabilities related to alcohol misuse, depression, isolation, and poor healthcare provider awareness all contribute to the under-diagnosis and under-treatment of disordered sleep in older persons and, specifically, in those individuals with dementia (Shub, Darvishi & Kunik, 2009).
Persons with dementia often have trouble sleeping. Disordered sleep (DS) is also prevalent in older persons (Foley, Ancoli-Israel, Britz & Walsh, 2004) and has been shown to have significant cognitive, physical, and psychological consequences (Misra & Malow, 2008). People with DS have a range of sleep problems which include the following: hypersomnia (e.g. sleep apnea and narcolepsy), parasomnia (e.g. confusional arousal, night terrors, restless leg syndrome, and sleep walking), insomnia (e.g. difficulty falling and/or staying asleep), and sleep-wake cycle disturbances. These symptoms all share the common outcome of non-restorative sleep.
The rate of falls in older persons with DS is also demonstrated to be higher (Stone, Ensrud & Ancoli-Israel, 2008). The literature shows that falls and a fear of falling have a negative impact on older persons’ self-confidence and continued engagement in social activities. These activities are important because they provide the physical and social stimulation necessary to help maintain cognitive and emotional health (Chou & Chi, 2008; van Haastregt, Zijlstra, van Rossum, van Eijk & Kempen, 2008). British researchers found that DS was a strong predictor of future depression in older community-dwelling adults (Livingston, Blizard & Mann, 1993).
Depression, in turn, is one of the risk factors for dementia (Dudgeon, 2010). Disordered sleep patterns in persons with dementia have been found to accelerate functional decline and contribute to increased caregiver stress (Tractenberg, Singer, Cummings & Thal, 2003). In the home setting, caregiver support and wellbeing is critical for successful management of dementia. However, living with someone who has both dementia and DS often results in sleep deprivation for the caregiver, further decreasing caregiver resilience and coping abilities.
From the literature, we also know that older persons with DS are at increased risk of substance misuse as they attempt to self-medicate for their sleep problems. This behaviour can contribute to a more rapid onset of dementia and decreased functioning. Both intentional and unintentional substance misuse (illicit, prescription, and over-the-counter medication) have been linked to cognitive decline in older persons (Johnson & Breslau, 2001). And while moderate alcohol consumption may delay the onset of dementia, chronic alcohol abuse can be a significant risk factor in some forms of dementia (Culberson, 2006). Culberson and Ziska (Culberson & Ziska, 2008) suggest that in the United States the rate of prescription medication misuse in isolated, elderly women with insomnia may be as high as 11%. Other researchers point out the complexity of the bidirectional nature of substance misuse to self-medicate for DS (Doghramji, 2006; Hartmann, 1995). They highlight that using substances such as alcohol and cough medications to help fall asleep have the side effect of actually reducing restorative sleep. This sets up a cycle of substance misuse to promote sleep, leading to poor sleep, leading to more substance misuse and further sleep problems. Aria et al. (Aira, Hartikainen & Sulkava, 2008) found that of the 699 elderly persons studied in Finland, 26% used alcohol to routinely self-medicate for sleep problems. Self-medication does not seem to decrease with age as evidenced by Johnson’s (Johnson, 1997) finding that the majority of community-living women over the age of 85 studied regularly self-medicate with alcohol and/or over-the-counter medication to improve their sleep.
Individuals who are most at risk for developing dementia (women, living alone, low income, history of clinical depression, obesity, and chronic inflammatory conditions) (Ancoli-Israel, 2009; Dudgeon, 2010) share many commonalities with those older adults at risk of developing disordered, non-restorative sleep (Ancoli-Israel, 2009; Cooke & Ancoli-Israel, 2006; Stone et al., 2008). For example, the estimated 18,000 older adults who immigrate to Canada annually are a subgroup of older individuals at particular risk of poorly managed dementia and DS. As parents and grandparents, they have immigrated primarily to be reunited with their adult children (Canada, 2005). Many of these older persons, often women, take up residence in their adult children’s established households. In their new homes, these older adults can lead isolated lives due to language and mobility barriers. This isolation prevents them from accessing resources in their new community to deal with this complex array of interrelated risks to cognitive, emotional and physical wellbeing (Brown, 2008). As well, risk factors for dementia are often largely unrecognized. These factors include DS, depression, poor nutrition, limited social stimulation and physical inactivity.
Disordered sleep can also contribute to a range of other health problems, premature institutionalization, and may be a modifiable risk factor for dementia. Researchers found a relationship between sleep deprivation of as little as three weeks duration and accelerated development of Alzheimer’s disease-associated amyloid plaques in the brains of lab mice (Kang et al., 2009). Other studies reveal a clear link between insomnia and cognitive tasks such as vigilance (Altena, Van Der Werf, Strijers & Van Someren, 2008), concentration, memory, and executive function (Bastien, Fortier-Brochu, Rioux, LeBlanc, Daley & Morin, 2003; Foley et al., 2004). Cricco et al. (Cricco, Simonsick & Foley, 2001) concluded from a study involving more than 6,400 persons over age 65 living in the community that ‘chronic insomnia independently predicts incidence of increased cognitive decline in older men’ (p. 1186).
As the number of people diagnosed with a dementia rapidly grows, so does the burgeoning problem of DS in this population. Although there is an evidence base for non-pharmacological interventions for people with dementia who have trouble sleeping, the methodological quality of this research has not been rigorously evaluated. Evaluation and subsequent synthesis is important as it allows stakeholders to develop evidence-based guidelines and teaching aids to support caregivers in initiatives to improve sleep for persons with dementia. This is a pressing topic to examine given the personal and societal implications of individuals experiencing DS and dementia.
Purpose
This paper provides a structured Critical Literature Review (CLR) of the methodological quality of the evidence for non-pharmacological interventions to reduce DS in older persons with dementia.
Method
Search strategy and selection criteria
We followed the Guidelines for Critical Literature Review (GCLR) developed by the McMaster University Occupational Therapy Evidence-based Practice group and published in Law and MacDermid (Law & MacDermid, 2008). The GCLR also includes data extraction forms to promote ease and consistency of the evaluation process. As part of the review we consulted two medical librarians and developed a comprehensive search strategy to identify outcome studies on the effectiveness of non-pharmacological interventions for older adults with dementia experiencing DS. To validate our search strategy, we contacted five published authors and experts in the field on the topic of DS and dementia to invite them to: (a) confirm that the search terms adequately covered the scope of the topic; (b) recommend additional concepts to include in the search; and (c) alert us to any topical, recently published articles, articles in press, or sources of non-published theses and reports (also known as ‘grey literature’). Following this we finalized and carried out an index term search in each of the selected databases and sources of grey literature.
Index terms relating to dementia, disordered sleep, and general and specific non-pharmacological interventions for older adults 65+, and caregivers were identified using each database’s thesaurus and the exploding term feature when available. The explode command in many databases is useful to expand the search to materials related to the original search terms. Synonyms, broader terms and narrower terms were also included in the search and included terms such as insomnia, non-drug treatment/intervention, and Alzheimer’s.
The following databases were searched: Ageline (1978-2010), AMED Allied and Complementary Medicine, CINAHL Plus with Full Text, Embase (1980–2010), Medline (1950–2010), PASCAL (European health literature), PsycInfo (1987–2010), Citations of International Rehabilitation Research (CIRRIE) Database of International Rehabilitation Research (1990–present), OTDbase, REHABdata. The following systematic review databases were searched: EBMR Reviews (OVID) (OVID Version of Cochrane), Health-evidence.ca (Ranked SRs). Other journal literature databases that were searched were Social Policy & Practice (OvidSP) and Sociological Abstracts (CSA).
Our search of the grey literature included: Agency for Healthcare Research and Quality, Canadian Agency for Drug and Technologies in Health (CADTH) – Sources listed in Grey matters: A practical search tool for evidence-based medicine;, Conference proceedings from major sleep conferences; Google Scholar Institute for Health Economics (IHE); and NHS Evidence.
Finally, we hand-searched all of the references from review articles and followed author links when this feature was included in a database. This allowed us to identify recent or non-indexed publications by known authors in the sleep and dementia field.
Inclusion/exclusion criteria
Search results were limited to English language articles and to research articles in peer-reviewed journals. No date or geographical limits were placed on the original searches. Studies that examined the use of melatonin or other substances, as well as those focused on sleep apnea and continuous passive airway pressure devices were excluded from the search. These studies were outside the scope of the CLR as the aim of the review was to examine evidence for sleep interventions that could be implemented by caregivers. These preliminary searches returned 3306 articles. Each set of database results was separately screened by one or more of the researchers (CB, MT, RB, AK). We reviewed the title and abstract of each article to confirm that it was a human-based outcome study at the level of a case study and above of a non-pharmacological intervention, as well as specific to dementia and sleep. We skimmed the article when we could not determine an article’s relevance through the title and abstract. Studies were excluded for the following reasons: participants with dementia were not included in the study; a non-pharmacological intervention was not delivered; and the studies were published as dissertations and no responses were received after contacting the authors for further information. During our background search we retrieved a systematic review of light-based interventions published prior to 2006 (Forbes et al., 2009). The systematic review excluded all studies that were not randomized control trials (RCTs). Because Forbes’ systematic review did not include non-RCT studies that may have added strength to the evidence base we decided to evaluate the quality of light-based intervention studies of all designs from 2000 forward. We did not extend our search pre-2000 as the existence of RCTs indicated that the state of the science for light-based interventions had moved beyond the theory-building stage where case study is most appropriate. We concluded that looking at older studies would not meaningfully contribute to our findings.
Search results
The above search and screening for exclusion/inclusion was completed in August 2010, and yielded 66 articles. We exported the results of each search to a citation management application and then searched for and removed duplicate records. This yielded 40 records. These articles were organized into two groups: non-light-based interventions (11) and light-based interventions (29).
We used Forbes’ (Forbes et al., 2009) systematic review as a final filter because it included published light-based intervention studies up to 2006 (with a few exceptions our search retrieved). We excluded the 10 studies already reviewed by Forbes from our own CLR although the conclusions from that systematic review are incorporated into the discussion section of this paper. Forbes (Forbes et al., 2009) found overall weak, poor-quality evidence and, consequently, we continued to search for any light-based interventions and dementia-related research articles published after Forbes’ review. This retrieved an additional 11 pre-2000 light-based intervention studies. Preliminary review of these studies revealed extensive methodological flaws in the eight non-RCTs. Consequently, we excluded these eight non-RCT studies and retained only the three RCTs not included in Forbes’ review for full review with the GCLR guidelines and data extraction forms. In the final CLR, a total of 29 quantitative outcome studies were included of non-pharmacological interventions for DS in individuals with dementia. Although we searched for qualitative studies none were retrieved.
Methodological quality evaluation strategy
We conducted the systematic CLR based on the GCLR (Law & MacDermid, 2008). These guidelines are structured to evaluate the methodological quality of qualitative and quantitative outcome studies. The broadness of studies is important when addressing complex, non-linear health problems such as DS in persons with dementia. The GCLR were first published online in 1998 and updated in 2007 (Law & MacDermid, 2008). These protocols are used extensively in rehabilitation research and have been translated into four languages. The GCLR data extraction tools focus on assessing the methodological quality of research in the following categories for studies with quantitative design: study purpose; background literature review; design; sampling; outcome tools; description of intervention; results; and conclusions. For studies of qualitative design the evaluation categories included: study purpose; background literature review; design; sampling; data collection methods; procedural rigour; data analyses; auditability; theoretical connections; and overall rigour. The data extraction tools are accompanied by clear guidelines and definitions of the components of each evaluated category. Each study was assessed by two of four reviewers (CB, RB, MT, and AK) using the GCLR data extraction review forms (Law & MacDermid, 2008). Disagreements were resolved through consensus and included a third reviewer as necessary. We also used the Jadad scale for quality of randomization in control trials (Jadad, Moore & Carroll, 1996).
Findings
Data categorization of search results
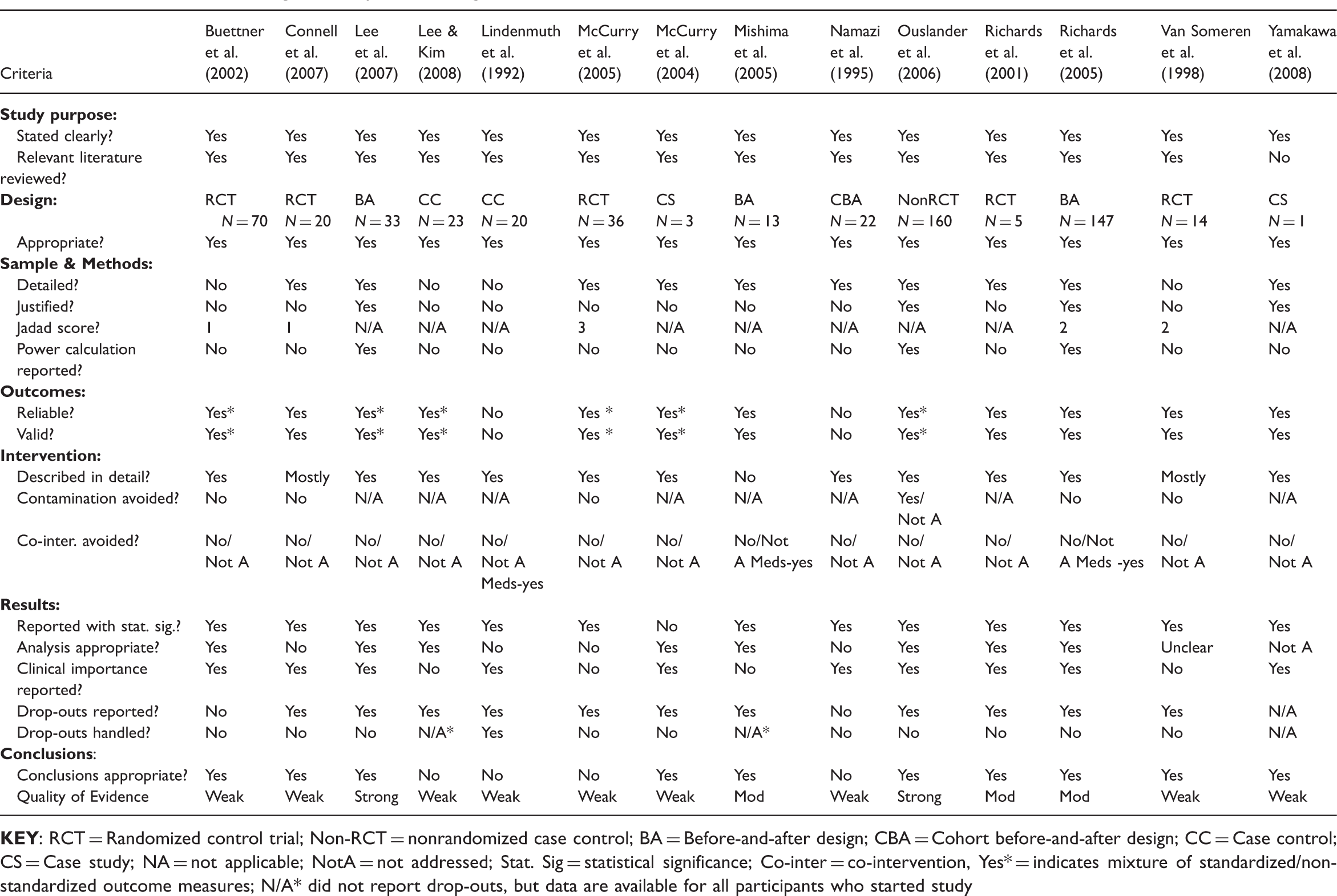
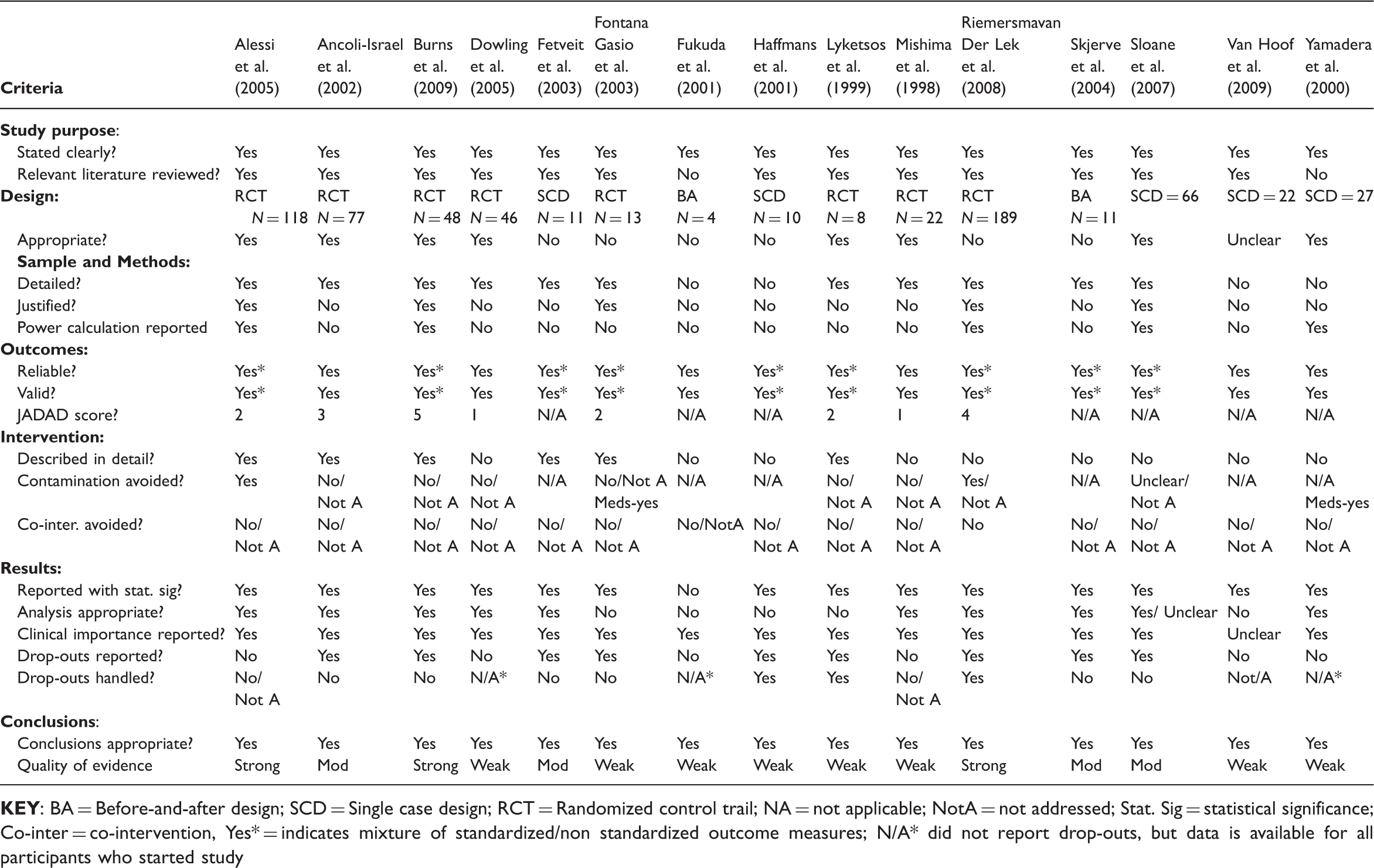
The 29 studies were categorized into non-light-based interventions (14 studies) and light-based interventions (15 studies) for ease of comparison and presentation of the findings. The non-light-based sleep interventions for persons with dementia included the following: music (Lindenmuth, Patel & Chang, 1992); exercise (Namazi, Zazorozny & Gwinnup, 1995); transcutaneous electrical nerve stimulation (TENS) (Van Someren, Scherder & Swaab, 1998); individualized activities (Richards, Sullivan, Phillips, Beck & Overton-McCoy, 2001); therapeutic biking (Buettner & Fitzsimmons, 2002); sleep hygiene and dementia education (McCurry et al., 2006); passive body heating (PBH) (Mishima, Hozumi, Shimizu, Hishikawa & Mishima, 2005); individualized social activity (ISAI) (Richards, Beck, O’Sullivan & Shue, 2005); outdoor activity (Connell, Sanford & Lewis, 2007); respite care (Lee, Morgan & Lindesay, 2007); indoor gardening (Lee & Kim, 2008); and environmental controls (Yamakawa, Shigenobu & Makimoto, 2008). The 15 light-based studies for persons with dementia included the following: social interaction accompanying bright-light therapy (BLT) (Mishima, Hishikawa & Okawa, 1998); morning BLT (Dowling, Mastick, Hubbard, Luxenberg & Burr, 2005; Fetveit, Skjerve & Bjorvatn, 2003; Lyketsos, Lindell Veiel, Baker & Steele, 1999; Skjerve, Bjorvatn & Holsten, 2004; Yamadera et al., 2000); lunchtime BLT (Fukuda et al., 2001); BLT in combination with melatonin (Haffmans, Sival, Lucius, Cats & van Gelder, 2001); comparison of BLT at different times in the day (Ancoli-Israel, Martin, Kripke, Marler & Klauber, 2002); dawn-dusk simulation (Fontana Gasio et al., 2003); multi-dimensional intervention including bright-light exposure (Alessi et al., 2005); comparison of high-intensity ambient light at different times in the day (Sloane et al., 2007); bright light and melatonin (Riemersma-van der Lek et al., 2008); late morning to noon BLT (Burns, Allen, Tomenson, Duignan & Byrne, 2009); and ambient bright-light exposure (van Hoof, Aarts, Rense & Schoutens, 2009).
Descriptive summary of reviewed bright light intervention and non-light intervention studies

Critique of Methodological Quality
Results of methodological critique of non-light-based intervention studies
Results of methodological critique of light-based intervention studies
Purpose and design
All of the studies clearly identified the purpose of the research and, with the exception of one non-light-based (Yamakawa et al., 2008) and two light-based reports (Fukuda et al., 2001; Yamadera et al., 2000), justified the need for research on sleep and dementia. The inclusion of a study justification in a research report is important as it identifies a need or gap in the current evidence base (Greenhalgh, 2006).
Five of the 29 studies utilized a before-and-after design which is useful when the researcher does not want or feels it is unethical to withhold treatment from the participants. Two of the studies used a case study design yielding descriptive information. Seven of the 29 studies used a single case control or a case control (with multiple participants) study design. These studies evaluated participants for the outcome(s) of interest at baseline and after the intervention. This allows the individuals in the study to serve as their own control. However, similar to before-and-after studies, it is difficult in studies using this case control design to conclude that the treatment alone resulted in any differences (Law & MacDermid, 2008). Five of the 14 non-light-based intervention studies and 8 of the 15 light-based intervention studies were RCTs. RCTs have traditionally been perceived to set the gold standard for design because of their ability to provide the highest internal validity which enhances confidence that the difference observed between the groups can be attributed to the manipulated variable (usually the treatment). As such, RCTs have an increased likelihood of demonstrating a causal relationship between the non-pharmacological intervention and sleep disturbances (Law & MacDermid, 2008). However, only two studies (Burns et al., 2009; Riemersma-van der Lek et al., 2008) achieved a Jadad score for randomization greater than three. The total possible Jadad scores ranged from zero (very poor) to five (rigorous) and this indicates that the randomization of participants in the 14 RCTs studies was moderate at best and most often poor.
RCTs are not always the most appropriate design for a study. For example, Sloane et al. (2007) employed a cluster-crossover design, which can be considered a form of case control design. A cluster-crossover design can be used for clinical trials comparing two or more interventions in a naturally occurring study population where the treatment sequence is allocated at the cluster level (Parienti & Kuss, 2007). The use of the cluster-crossover design can be considered more suitable than attempting an RCT in a clinical setting where randomized trials are not feasible. Sloane’s study was carried out in a psychiatric hospital and dementia residential care facility, where the use of cluster-crossover design was well suited (Parienti & Kuss, 2007). Similarly, single case, case control and case studies are considered appropriate when little is known about a topic and theory-building is still ongoing. Case studies cannot demonstrate causality but contribute important preliminary observational data to inform the next level of experimental testing (Greenhalgh, 2006).
Sampling
In regards to sample selection, only two studies (McCurry et al., 2005; McCurry et al., 2004) recruited participants from the community and the other studies were carried out in institutional settings. This makes generalization of the findings to community settings problematic and highlights a gap in the research. A range of recruitment and purposeful sampling strategies were used by researchers across the range of studies. These strategies included posting advertisements in the community, nurses identifying individuals with sleep disturbance symptoms, and other attempts to recruit individuals with cognitive impairments. Seven of the studies lacked sufficient detail about the sampling and the majority failed to justify their sample size. In general, the studies recruited through third parties and reported no efforts to match participants or achieve a representative group. We concluded based on our reading that, overall, sampling bias was poorly controlled. This highlights the challenges of recruiting participants from vulnerable populations such as those individuals with dementia (Greenhalgh, 2006).
Three non-light-based intervention studies (Lee et al., 2007; Ouslander et al., 2006; Richards et al., 2005) and five light-based intervention studies (Alessi et al., 2005; Burns et al., 2009; Riemersma-van der Lek et al., 2008; Sloane et al., 2007; Yamadera et al., 2000) reported using a power calculation to justify sample size. The other studies were less clear in how they determined sample size. Lack of a justified sample size (for example with a power or number-needed-to-treat calculation) is a fundamental concern limiting the validity of statistical analysis and generalizability of findings (Greenhalgh, 2006). Consequently, it was difficult to place a high confidence in the statistical findings of many of the reviewed studies.
The sample sizes ranged from 1 to 189 participants. Using a sufficiently large sample detects treatment effects (Law & MacDermid, 2008) and strengthens internal validity. Internal validity is important as it demonstrates that there is evidence that the outcomes of the study were related to the variable that was manipulated (Trochim, 2006). Although case control and single case studies establishing possible relationships typically have small samples, it was concerning that a number of the RCT studies for non-light-based interventions (Connell et al., 2007; McCurry et al., 2005; Van Someren et al., 1998) and light-based interventions (Fontana Gasio et al., 2003; Lyketsos et al., 1999; Mishima et al., 1998) also had small samples which possibly weakened internal validity.
Outcome measures
Outcome measures and screening tools used in critiqued studies

Eleven studies (Alessi et al., 2005; Ancoli-Israel et al., 2002; Burns et al., 2009; Fontana Gasio et al., 2003; Haffmans et al., 2001; Lyketsos et al., 1999; McCurry et al., 2005; Ouslander et al., 2006; Skjerve et al., 2004; Sloane et al., 2007; Yamakawa et al., 2008) used a mixture of observational, standardized, and psychometrically tested outcome tools. Of concern, two non-light-based studies (Lindenmuth et al., 1992; Namazi et al., 1995) only used sleep logs completed by nurses as their outcome tools. The potential for inconsistent reporting exists and the researchers presented little information about inter-rater reliability and evaluator training. These limitations further undermine the quality of the outcome measures and make it difficult to replicate or generalize the results from both studies.
Intervention details
All but one non-light-based intervention study (Mishima et al., 2005) provided sufficient intervention details to be replicated in practice. Insufficient details about the intervention reduces the quality of the study as this makes it difficult to evaluate if the study can be replicated and to determine if the intervention is applicable to different clinical contexts. In comparison, nine of the 15 light-based studies (Dowling et al., 2005; Fukuda et al., 2001; Haffmans et al., 2001; Mishima et al., 1998; Riemersma-van der Lek et al., 2008; Skjerve et al., 2004; Sloane et al., 2007; van Hoof et al., 2009; Yamadera et al., 2000) did not provide sufficient detail about procedures, settings, and description of the persons carrying out the intervention. As such, the studies are of a weaker quality because the relevance, replicability, and transferability to other clinical settings are unclear.
Bias
The potential for contamination bias did not appear to be considered in five of the non-light-based intervention studies (Buettner & Fitzsimmons, 2002; Connell et al., 2007; McCurry et al., 2005; Richards et al., 2005; Van Someren et al., 1998). This bias occurs when members of the control group inadvertently receive the study treatment, thereby reducing the difference in outcomes between the two groups (Law & MacDermid, 2008). This same problem existed in the light-based intervention studies and only two studies (Alessi et al., 2005; Riemersma-van der Lek et al., 2008) reported efforts to avoid contamination bias. Contamination may be particularly difficult to control in institutional settings where the majority of these studies were carried out.
Attention bias was also a consideration as all of these interventions were delivered or assisted by individuals throughout the duration of the study. These daily interactions between researchers/research assistants and participants whilst providing the intervention in addition to the usual care could have negatively or positively influenced the results. Additionally, co-intervention bias was not adequately addressed in any of the applicable studies. Co-intervention bias is the influence of results based upon participants receiving another form of treatment at the same time as the study treatment (Law & MacDermid, 2008). Although several non-light-based intervention studies (Lindenmuth et al., 1992; Mishima et al., 2005; Richards et al., 2005) discussed trying to control for medication, the researchers failed to report if all the other variables (such as alternative programs, daily schedules, and other forms of treatment) were kept consistent. Two applicable light-based intervention studies (Fontana Gasio et al., 2003; Yamadera et al., 2000) discussed medication control, whilst the other studies failed to address other influencing variables that may have impacted the results.
Results
Although 13 of the 14 non-light-based studies presented their findings in terms of statistical significance, only seven studies (Buettner & Fitzsimmons, 2002; Lee et al., 2007; McCurry et al., 2004; Mishima et al., 2005; Ouslander et al., 2006; Richards et al., 2005; Richards et al., 2001) described their statistical analysis with sufficient detail to justify the appropriateness of the analysis methods. McCurry et al. (2004) used descriptive statistics appropriate to the study design and sample. The matching of statistical analysis formulae to study design and sample size was better demonstrated in the light-based intervention studies and only five of the 15 studies (Fontana Gasio et al., 2003; Fukuda et al., 2001; Haffmans et al., 2001; Lyketsos et al., 1999; van Hoof et al., 2009) failed to justify the appropriateness of their statistical analysis.
In the evaluation of the studies with questionable matching of analytical methods, a common concern was the use of parametric statistical tools in the absence of evidence that the study population demonstrated a normal distribution (see Table 2 and Table 3). For example if an RCT had a small sample this generally precludes achieving the normal distribution required to confidently use parametric statistical techniques (e.g. paired samples t-test). For a small sample without a normal distribution, the non-parametric alternative to a t-test (e.g. the Wilcoxon Signed-Rank test) would be indicated. A number of the studies did not report whether their sample achieved a normal distribution. Statistically significant findings generated without a normal Gaussian distribution are of weaker value with a higher probability of a type 1 (false positive) error (Trochim, 2006) and so clear matching of parametric and non-parametric analysis based on the sample distribution is required.
Summary and synthesis of the methodological quality
The number of met/unmet criteria for each study entered into the GCLR data extraction forms was considered regarding the strength of the evidence of each study. However, each of the GCLR criteria is not of equal weight. For example, the data extraction question in the guidelines ‘was there a review of relevant background literature?’ is not as significant an indicator of research rigour and validity as the question ‘is the sample size justified?’. Issues such as a low Jadad score and poor randomization procedure, lack of a justified sample size or power calculation, insufficient detail for sampling and sample size, insufficient intervention detail to allow for replication, and inappropriate selection of statistical analysis formulae were frequently occurring problems.
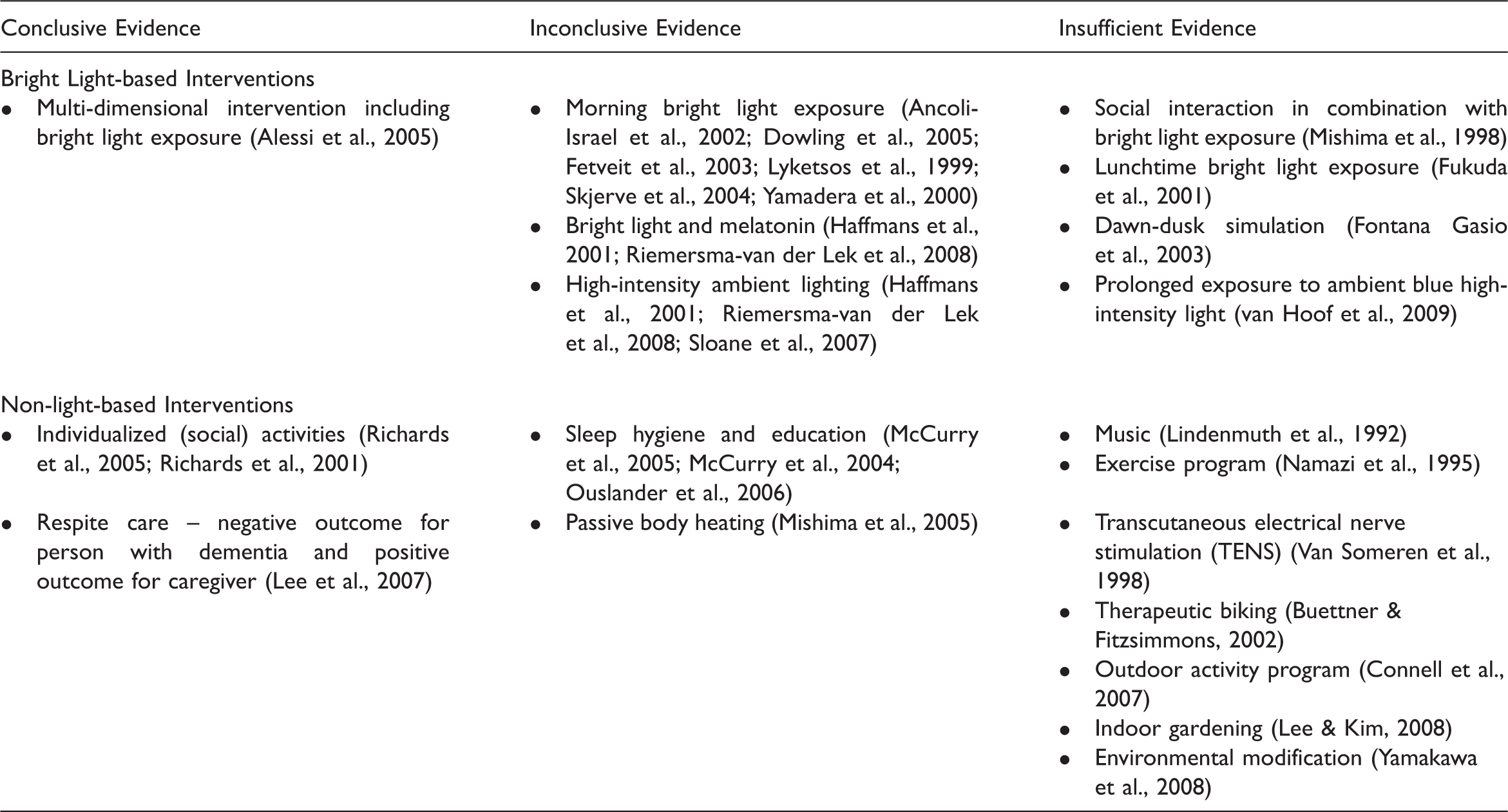
Our overall CLR of the non-light-based intervention studies determined there was strong methodological quality in the studies of sleep hygiene techniques (Ouslander et al., 2006) and respite care (Lee et al., 2007). Moderate methodological quality was found in the studies of individualized activities (Richards et al., 2005; Richards et al., 2001) and passive body heating (Mishima et al., 2005). The remaining non-light-based intervention studies of music (Lindenmuth et al., 1992), transcutaneous electrical nerve stimulation (TENS) (Van Someren et al., 1998), exercise (Namazi et al., 1995), therapeutic biking (Buettner & Fitzsimmons, 2002), sleep hygiene and dementia education (McCurry et al., 2004), sleep education (McCurry et al., 2005), outdoor activity programs (Connell et al., 2007), and indoor gardening (Lee & Kim, 2008) showed evidence of promise but lacked sufficient methodological quality to confidently implement the findings.
The CLR of the light-based sleep intervention studies determined there was strong methodological quality in the studies of multi-dimensional interventions including bright light exposure (Alessi et al., 2005), bright light and melatonin (Riemersma-van der Lek et al., 2008), and late morning to noon BLT (Burns et al., 2009). Moderate quality was found overall for studies of bright light exposure at differing times of the day (Ancoli-Israel et al., 2002), morning BLT (Fetveit et al., 2003; Skjerve et al., 2004), and high-intensity ambient light (Sloane et al., 2007). The remaining studies were of insufficient methodological quality to implement findings with confidence prior to further research. These studies included social interaction in combination with BLT (Mishima et al., 1998), morning BLT (Dowling et al., 2005; Lyketsos et al., 1999; Yamadera et al., 2000), lunchtime bright light exposure (Fukuda et al., 2001), BLT in combination with melatonin (Haffmans et al., 2001), dawn-dusk simulation (Fontana Gasio et al., 2003), and prolonged exposure to ambient blue high-intensity light (van Hoof et al., 2009).
Clinical relevance
Clinically relevant evidence for non-pharmacological sleep interventions with dementia
Limitations of the review
Some of our exclusion/inclusion and search term decisions may have resulted in overlooked studies. However, our confidence was improved that this was not a significant problem by continued input from medical librarians and experts in the field who provided feedback on new literature. Hand-searching reference lists retrieved some relevant studies where the authors had omitted any words indicative of cognitive impairment from their key words, title or abstract. Possibly some studies with similar problems were overlooked in our hand search. Our categorization of the quality of the evidence (conclusive, inconclusive, and insufficient evidence) exercised clinical judgement in combination with the objective findings from the CLR. Other researchers, using different tools than the GCLR, may arrive at slightly different rankings.
We attempted to minimize concern about rating the quality of the evidence through a process of multiple reviewers with a wide range of clinical and research experience. The study search was completed in August 2010 and there may be more recent higher-quality studies that have not been included in the CLR. Finally, the comprehensiveness may be limited as only English language studies were included in the review.
Discussion
Similar to Forbes (Forbes et al., 2009), we found that a range of interventions based on light exposure were supported by moderate to strong quality of the evidence (see Table 5). Our review also determined that there is conclusive evidence to apply the intervention of bright light as a component of a multi-dimensional intervention (Alessi et al., 2005) and individualized social activities (Richards et al., 2005; Richards et al., 2001) to reduce DS in persons with dementia. It is important to note that although the principles of light-based therapies have been established, there is no current consensus about the time of day, frequency, duration or specific wavelength required for effective and safe light exposure intervention (Deschenes & McCurry, 2009). As Deschenes and McCurry point out, one size does not fit all; the intervention must be selected based on a deeper knowledge of the presenting sleep problem, diagnosis, and other contextual factors. There is also conclusive evidence that whilst institutional respite care has positive sleep outcomes for caregivers, this care has a negative impact on the sleep of people with dementia (Lee et al., 2007). Although less conclusive, there is additional preliminary promising evidence for light-based interventions at various times of the day (Ancoli-Israel et al., 2002; Dowling et al., 2005; Fetveit et al., 2003; Haffmans et al., 2001; Lyketsos et al., 1999; Riemersma-van der Lek et al., 2008; Skjerve et al., 2004; Sloane et al., 2007; Yamadera et al., 2000), sleep hygiene and sleep education (McCurry et al., 2004, 2005; Ouslander et al., 2006), as well as passive body heating (Mishima et al., 2005).
The search revealed that although a number of authors provided a clear, theoretically grounded rationale for their study, the studies did not build on each other and the body of previous clinical research. Most studies were unique with little design and/or intervention consistency between studies. Replication of intervention across a number of studies and with consistent, more rigorous research design, would strengthen the evidence. As David et al. (David et al., 2010) identified, research seems to be more focused on light-based interventions and the current evidence base for these other practical, non-pharmacological interventions is limited. However, it should be a strong incentive for non-light-based, non-pharmacological research as many of the interventions with insufficient evidence are pragmatic and could easily be implemented by family caregivers. For example, the use of music at bedtime (Lindenmuth et al., 1992), indoor gardening (Lee & Kim, 2008), and decreasing ambient nighttime light and noise through simple environmental modifications are relatively easy to implement and can be confidently carried out by most family caregivers. Building the evidence base supporting or refuting these simple interventions should be a priority considering the cost, complexity and potential side effects of medication and more elaborate non-pharmacological interventions (Yamakawa et al., 2008). Encouragingly, our review identified a range of standardized and in some cases psychometrically tested outcome measures available to dementia and sleep researchers. For example, as technology advances, the use of actiographs is becoming more routine and much less expensive. The actiograph is an objective form of sleep measurement. It is important to use an objective measure to enhance the validity of conclusions that should not be based solely on standardized third-party reporting tools.
Importantly, we found that researchers regularly raised the issue of a lack of awareness amongst healthcare providers about the range of non-pharmacological sleep interventions available. Although not part of the formal methodological review, this is important because without awareness of the range of evidence-based non-pharmacological options available, healthcare providers are left managing complex sleep and dementia problems with only pharmacological interventions. These pharmacological interventions have little empirical evidence to demonstrate they are safe for long-term use in persons with dementia (Deschenes & McCurry, 2009) and have associated clear and significant adverse effects (Shub et al., 2009).
Lastly, our search retrieved some promising research into the related area of technology to promote nighttime safety for the person with dementia. Although outside the scope of this study, Carswell et al. (Carswell et al., 2009) provide a comprehensive review of the existing technologies to help monitor safety and undesired mobility and to trigger audiovisual technology to entice the viewer to stay safely in the bedroom instead of wandering at night. These innovations will continue to evolve and become another source of practical, affordable strategies to help decrease the impact of poor sleep for persons with dementia.
Conclusion
With the rapid global rise in numbers of people who will have some form of dementia, identifying effective sleep interventions to promote health for both them and their caregivers is clearly urgent. This anticipated rise in dementia presents unique challenges as the accelerating demand for services is coupled with the need for healthcare providers to quickly develop the requisite skills to respond with best practice and evidence-based interventions.
Currently there is a paucity of methodologically rigorous research in the area of non-pharmacological sleep interventions for persons with dementia. While the literature clearly identifies the magnitude and clinical, functional, and economic significance of this issue for persons with dementia, their caregivers and society, most of the evidence about the effectiveness of non-pharmacological interventions is anecdotal and untested.
The small body of research that does exist shows much promise and serves to highlight emerging and extensive opportunities for further study. It is important to note that while methodological weakness in a study’s design may result in a lack of evidence for the intervention, it does not follow that the intervention has no merit and should be discarded. Rather, we need to couple tacit knowledge about effective interventions derived from clinicians’ and family members’ experience with what we know about good research design. In this manner we can build a strong evidence base for the high need and growing area of non-pharmacological sleep interventions for persons with dementia.