
Abstract
This study examines some of the micro-skills associated with the moment-to-moment decisions and actions involved in delivering group formulation sessions in dementia care settings. We discuss the therapeutic framework used by therapists from a number of Challenging Behaviour Services in the UK (Newcastle, Northumberland, South Tyneside, Teesside, Sutton and Merton, Northern Ireland) which is frequently referred to as the Newcastle or Colombo approach. Through a theoretical review and practice illustration, the study pays particular attention to the role of therapists’ questions and questioning styles in group formulation sessions, providing a framework which aims to facilitate care staffs’ understanding, reflection and empathy regarding their residents who are displaying ‘challenging behaviours’. The study also provides a potential guide to the training of therapists working in this area and thereby attempts to benefit clinical practices in an area where pharmacological approaches are usually the treatment of choice.
Introduction
The need for the development of effective psychotherapeutic treatments for people with dementia is reflected in national policy developments and in professional practice frameworks in the UK (National Dementia Strategies England and Scotland; NICE, 2006). For example, the recommendations for interventions for people with dementia presenting with challenging behaviours, suggest that behavioural management has shown some success in single-case trials and that ‘individualised, tailored approaches ought to be considered' (NICE, 2006, p. 230). This view is also supported by the recent Cochrane review of functional analytical approaches for challenging behaviour (Moniz-Cook, Swift, James, Malouf, De Vugt & Verhey, 2012).
However, these guidelines are dominated by general statements about the nature of the therapies (e.g. client-focused, person-centred) or the appropriateness of the content of the therapy and do not describe the specifics of how to conduct an effective intervention when a person presents with challenging behaviour. The guidelines call for holistic assessment and effective care planning, but do not describe the process or strategies required to move from the point of assessment to decisions about care planning. Until this process is described, it is impossible to articulate the reasons for change or to measure the success of interventions. This situation differs substantially from national guidelines (NICE, 2010) on interventions for depression, for example, which stipulate that the treatment of choice is cognitive behavioural therapy – a very specific formulation-driven psychological therapy and a therapy which has been examined extensively in terms of its change mechanisms (Whisman, 1993) and process features (Castonguay, Goldfried, Wiser, Raue & Hayes, 1996).
In many respects, the exchanges occurring within group formulation sessions with staff in dementia care settings are more complex than those occurring within 1:1 therapy. This is due to the fact that the therapist working in care settings is attempting to influence clinical outcomes indirectly through the carers. Further, the success of the intervention is dependent upon all of the care staff implementing the interventions consistently.
We believe that the general level of guidance and analysis for therapists (referred henceforth in this paper as ‘facilitators’) working with care home staff, on interventions in cases of challenging behaviour, needs to be complemented by a more specific or ‘micro-skills’ level of analysis.
The Newcastle approach: a formulation-led approach to working with challenging behaviour in care settings
The Newcastle approach (James, 2011) has been developed in response to a need to offer systematic, model-driven interventions for people presenting with challenging behaviour (CB) in institutional settings. In this approach it is assumed that CB in dementia can be understood within the context of the damage to the brain caused by the dementia but also in the context of other aspects of people’s lives (i.e. physical health, personality, environment, mental health and life history) and so incorporates aspects of the work of Kitwood (1997), Cohen-Mansfield (2000) and Beck (1976). Essentially, there are five stages to the Newcastle approach:
Background assessment Staff and families are asked to provide information relating to the person’s background (e.g. life story, personality, social environment etc). Details are also obtained from case files and relevant data bases. Assessment of triggers Information is obtained to determine the events or situations which are likely to elicit the behaviours. Functional analytical scales are used to help identify the triggers. Assessment of CB It is very important to obtain a rich description of the CB. This is usually conducted via staff completion of behavioural charts, but information is also elicited through observation of the resident. Formulation session This involves organising a group meeting with staff, and sometimes family, to increase empathy and improve understanding of the person’s CB. Interventions Interventions are based on staff suggestions and developed and refined at the end of the formulation session with the therapist’s help.
LCAPS guidelines for working with care staff
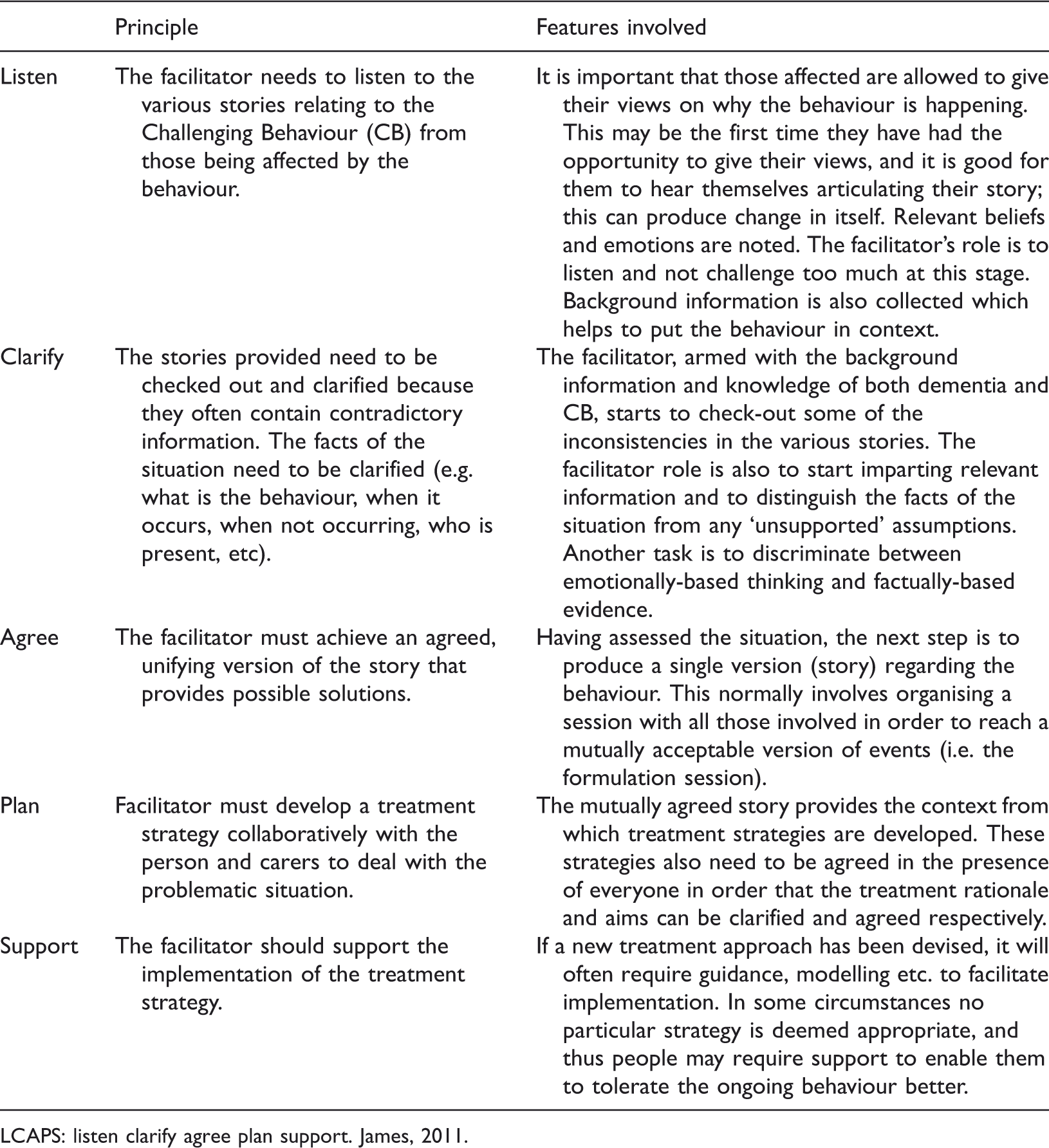
LCAPS: listen clarify agree plan support. James, 2011.
In this paper, we concentrate on describing the elements of the formulation sessions (also called ‘information sharing sessions') which we believe affect the readiness with which staff embrace the approach and their motivation to change.
Formulation sessions are normally guided by the facilitator who highlights key background issues and relates them to the person's behaviour. This individual facilitates the session using effective questioning techniques, feedback, summarising, education, challenging strategies and guided reflection techniques. These methods are designed to get the staff to ‘step back’ from the situation and look afresh at the person's behaviour within its historical and situational context. Collaboration with staff is particularly important when trying to identify the person’s needs and possible thoughts. Therefore, at this stage, as many staff as possible are asked to attend the formulation session, preferably with all levels of staff represented.
The Challenging Behaviour Service
Over a six-month period in 2010, members from three specialist CB teams analysed their performances during formulation sessions, and this paper presents their current understanding of the skills they employed in conducting the sessions.
The teams’ experiences of working in the care sector with staff suggest that assessment and advice are insufficient to help staff identify relevant aspects of people’s experience or for staff to alter their behaviour to manage situations. In the Newcastle approach, a team member facilitates sessions with care staff in order to reach a collaborative understanding of how the identified person with CB might be thinking and feeling during episodes of challenge. This understanding is reached through the facilitator sharing information about the many aspects of the person’s experience that could be affecting their behaviour. The information shared is represented in the diagrammatic model of the formulation framework used in the Newcastle model (see Figure 1).
Newcastle model formulation framework.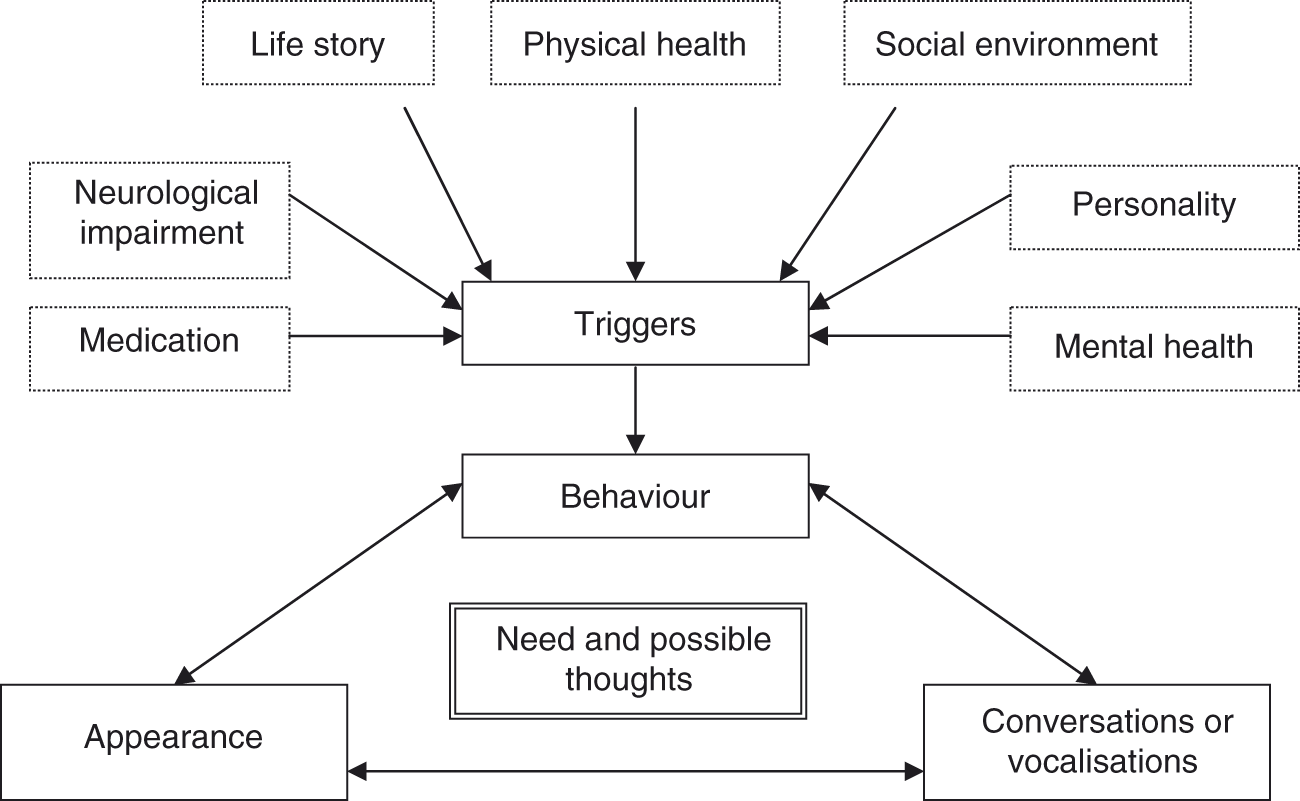
The Newcastle approach involves working with staff to make connections between the way a person behaves and their thoughts and feelings at the time; this reflects the approach used in cognitive therapy. In this type of therapy, the therapist aims to help the patient identify and change unhelpful ways of thinking. Similarly, the Newcastle approach aims to identify and change unhelpful thoughts staff might hold about a person with CB in order influence practice in a positive way. In the formulation session, the facilitator aims to replace the care staff’s previous (unhelpful or erroneous) understanding or thinking about the CB with a new set of ideas. Similarly to the mechanism of change proposed in cognitive therapy, it is assumed that this new understanding of the problem behaviour will lead to different interpretations and thus care-giving practices.
Although the understanding of care staff can often change during the initial assessment period, the main vehicle of change in the Newcastle approach is the formulation session facilitated by a member of the specialist Challenging Behaviour Service. These formulation sessions require skilful facilitation in order to change the understanding of care staff in a supported and non-threatening way. We refer to the techniques and strategies used in facilitating these sessions as ‘micro-skills’.
Micro-skills within the formulation session
Micro-skills are the moment-to-moment activities that facilitators use within formulation sessions to promote learning, understanding and empathy. These skills may be verbal or non-verbal in character, involve the imparting of facts, the promoting of reflection, action planning and the using of experiential exercises (Kolb, 1984). In the current paper we aim to examine the role of some of these micro-skills, particularly the function and sequencing of questions (i. e. the placement of specific questions within a section of dialogue) and the relationship of questions to other aspects of formulation dialogue. Therefore, we start by outlining the rationale for micro-skills and then provide an illustrative dialogue with comment on the key aspects of the process of effectively conducting the formulation session. However, before discussing micro-skills in relation to dementia care, we shall review its relevance to the general literature on therapy and learning.
Micro-skills in therapy
It is clear that the various therapeutic approaches, while differing in the assumptions that might underlie each therapy, have a number of commonalities in the process of delivering therapy. Therapists in training learn about body posture, eye contact, managing silence and reflection. It is recognised that the micro-skills involved in delivering one-to-one therapy can be measured and taught through the process of clinical supervision. In a series of empirical studies, Milne and colleagues have developed a useful list of activities engaged in by supervisors during clinical supervision. This list has been packaged into a tool called ‘Teachers PETS’ (Process Evaluation of Training and Supervision: Milne, James, Keegan & Dudley, 2002; Milne, Pilkington, Gracie & James, 2003). The PETS tool is an observational instrument that provides a system for coding the speech of trainers and their trainees. It identifies 14 activities typically engaged in by a cognitive behavioural therapy (CBT) supervisor. These are: listening, gathering information, managing, supporting, summarising, feedback, checking theoretical knowledge, challenging, educating, experiential learning (e.g. modelling, role-play), self-disclosing, disagreeing, video observation, other (e.g. social chat, paper work, setting-up equipment). The PETS tool can also be used to examine the impact of these activities on the trainee. We believe that the PETS tool is particularly useful in the context of group formulation sessions as the process of these sessions mirror, to a large degree, the processes we see taking place in supervision sessions. Effectively, the group facilitator (i.e. Challenging Behaviour Service team member) takes on a temporary role as a trainer of the group. In other words, the activities highlighted and defined within the PETS tool represent some of the micro-skills required when providing a good formulation session. However, competent group formulating in the context of CB in the residential care setting not only requires the presence of such micro-skills; the facilitator also needs to be sensitive to other issues that will affect the staffs' ability to contribute to, and learn from, the formulation session. For example, facilitators need to take into account the group members' education, culture and intellectual and language skills. It is important that the functions in formulation are sequenced in an order that promotes the most effective learning. Owing to the limited scope of this paper, the following section will focus mainly on a specific set of micro-skills relating to questioning styles, termed ‘scaffolding’.
Questioning processes
In the training literature there are a number of frameworks that describe how learners learn; one of the most useful in the present context is Vygotsky’s (1978) notion of how learning can be promoted via the use of scaffolding strategies (Wood, Bruner, & Ross, 1976). Scaffolding strategies take the form of verbal and non-verbal statements (questions, cues, reminders, prompts and contexts) that guide the learner’s development. In a training project examining some of the micro-skills involved in the supervision of a neuropsychology case (James, Allen & Collerton, 2004), it was suggested that this notion of scaffolding (Wood et al., 1976; James, Milne, Morse, & Blackburn, 2007; James, Milne, & Morse, 2008) was a helpful way to understand how the facilitator promoted reflection and knowledge acquisition. Scaffolding is defined as the process by which a trainer provides temporary support to the learner in order to help him/her learn something new based on the foundations of what is already known (Graves & Braaten, 1996). For example, when conducting an educational session on the nature of Lewy body dementia, instead of asking staff the rather confrontational question, ‘What do you know about Lewy body dementia?', one could ‘scaffold’ the learning as follows: ‘Mr Smith has been diagnosed with Lewy body dementia, have you noticed anything particular about how he behaves or appears?’. This question is less direct, and puts the staff in a powerful position, as they are likely to be the experts about Mr Smith’s presentation. Furthermore, as the staff respond with appropriate responses, the trainer is able to reinforce the correct answers via the use of praise and non-verbal gestures. Of note, at the end of the sequence, the trainer should then summarise the characteristics generated in order to consolidate the learning.
Essentially, the scaffolding procedure takes the form of questions and directions (gestures, questions, instructions, cues and prompts) from the trainer. The directions are contingent on the observed interaction of the participants with the learning material. Hence, if the learners start to look confused or anxious, this may cue the trainer to use simpler language, reiterate key issues or tackle the situation from a new perspective.
One of the chief functions of questions is to drive learning forward, causing the participants to access new information, reflect on past experience, etc. Sometimes the questions may be simple and direct and at other times they may be provided within a context. The context is often made up of scaffolding statements which function either to help focus the participants with respect to a particular issue or to facilitate ease of response. To illustrate, take the following two questions which are essentially asking the same thing:
Trainer: Why do you think Mrs Jones is so aggressive?
Trainer: OK, let’s look at Mrs Jones' formulation. I see that she is 85, has a history of chronic back pain and arthritis. Can anyone tell me Staff: She was hitting out this morning and yesterday morning … also when I told her I needed to ‘lift’ her to take her to the toilet. Trainer: Thanks, and I see from your charts, she is only hitting out at staff, and this behaviour occurs almost exclusively in the morning and when you’re hoisting her. OK, has anyone got an idea why a woman with these physical difficulties might hit out?
Although the trainer is essentially asking the staff to do the same thing in both examples, the second question provides a rich, yet focused, context (i.e. it has been scaffolded); thus, increasing the likelihood that the staff will integrate the relevant information and generate appropriate hypotheses about Mrs Jones’ presentation.
As outlined above, the use of information to promote learning is called ‘scaffolding’. We suggest that there are at least two aspects of the scaffolding process (i.e. the statements spoken by the trainer), namely questions and ‘platforms’ (James et al., 2008). A platform is defined as the supportive information (summaries, reminders or statements) used to set-up a question or to give it an appropriate context. Thus, the platforms serve to guide and direct the participants’ responses. In the first example (Question 1) a platform was not provided and thus the participants may have struggled to select an answer, as there were so many potential reasons, and they may have perceived, from the direct nature of the question, that there was a ‘correct’ answer. However, in the second example (Question 2) it is anticipated that the presence of a platform helped the staff to focus better, thereby facilitating the selection of the most relevant and appropriate response from a number of possibilities.
Case illustration
In order to illustrate how some of the concepts discussed above relate to the context of formulation sessions, we present two sequences of formulation dialogue. In the first sequence we hear how a facilitator uses self-disclosure to demonstrate empathy with staff working with a gentleman whose sexually-disinhibited language and behaviour was causing great distress and threatening his placement in the care home (corresponding to self-disclosure function in PETS). Also, although staff are initially reluctant to admit to feeling shocked or upset by the resident’s behaviour, the facilitator provides cues in the form of visual imagery and reflection to prompt staff to make connections between their feelings and how those feelings affect their provision of care for Mr Brown. The facilitator uses a scaffolding process to encourage these links.
Facilitator: So now, I’d like to find out how you feel when Mr Brown says things like ‘Give me a ‘f..ck'. How does it makes you feel and how do you deal with it? Does anybody want to comment? Carer 1: I don’t feel anything, its part of the job. It doesn’t really affect us. Facilitator: OK, do you think it changes the way you behave towards him? Carer 1: No, I don’t think so, we’re all professionals … and just ‘do what we have to do’. Facilitator: Just to get things clear in my own head. I’d like to get you to think through the last time you helped Mr Brown get dressed … and what happened when you opened the bedroom door … how you felt. Now remember how he looked, and recall if he said anything to you. Just stick with that image for a minute. OK, any comments? Carer 2: Actually, I can remember … he asked me to rub his penis … I remember feeling embarrassed … it was really disgusting. Carer 3: I hate it when he says things like that … the way he looks at you … makes me feel a bit frightened … I don’t like to go in then … I think I probably avoid going in. Facilitator: Embarrassed. Yes. [writes onto flip chart]. And you said you ‘hated’ what he said and felt frightened. Anything else? Carer 4: I’m shocked when I see that written down like this … ‘cause he’s never said things like that to me … he just says some inappropriate things but nothing as disgusting as these. [At this stage, the facilitator is not going to investigate why Mr Brown behaves differently towards this carer. This feature can be examined later.] Facilitator: So you are shocked? [writes on flip chart] … Any other emotions when you see these words written down like that … and recall the image? Carers 4 and 5: Sad … sick … [facilitator notes on flip chart]. Facilitator: I mean, when I showed the comments from the diaries you kept to my team we were all upset too. Carer 1: You know in truth, when he is like this it really puts you off going into his room. If you have to go in, you end up doing things really quickly to get out. [Other carers agree, facilitator writes comments onto flip chart.] Facilitator: So these are the sorts of emotions you’re feeling and these are the sorts of things you’re doing as a consequence of these emotions? Carers: Yes. Facilitator: So you don’t want to go into his room any more. You don’t really want to do the sort of tasks that may trigger him to say these things? … As I said, when we heard about it, we were upset by what he was saying. It made me wonder how you were coping … and why he would say such ‘out of character’ things.
In the second sequence (Dialogue 2) the facilitator reiterates information previously learned during a short teaching session (corresponding to information-giving in PETS) in order to lead the group to use that information to form new inferences about why Mrs Mackay may be parcelling and hiding faeces. Once again, the facilitator accepts and examines the suggestions of staff by reiterating previous learning and, through general questions (‘I wonder why…?’) invites them to synthesise that learning with their knowledge of the resident to help them understand why she may be acting in this way. In this case the staff are meeting to discuss why Mrs Mackay has started wrapping her faeces in a paper parcel and placing it behind the radiator in her room. One of the most vocal members of staff (Carer 2) believes that Mr Mackay is becoming lazy and cannot be bothered going to the toilet.
Facilitator: I’m aware you know a lot about dementia already. I just want to go through some aspects that may help us understand Mrs Mackay’s behaviour. We know that dementia leads to memory problems, linked with word finding difficulties … there’s confusion, with mood swings … and we know it’s progressive. And some people have great difficulty working out quite simple problems. So have you noticed Mrs Mackay experiencing any of these problems? Carer 1: Yeah, she is really slowing down. When she first came in to the home she could make herself a sandwich. She gets confused doing this now. The other day she put the butter in the washing machine by mistake … she got really, really embarrassed. She seemed to know it was wrong, but couldn’t work out what to do. In the end she took the butter out of the machine and hid it in her bedside cupboard. Facilitator: OK, so we know that she’s getting confused, and tends to get embarrassed about things. How do you think these features might relate to her parcelling her faeces and placing the parcel behind the radiator? Carer 2: Well I think she’s a becoming lazy. She is asking for a lot more help these days. Facilitator: OK, that’s one possibility. Any other possible reasons? Carer 3: I don’t think she is lazy, because why would she go all the way back to her room, wrap the ‘poo’ in paper and then put it behind the radiator … that’s much more work! Facilitator: That’s a good point. So you’re saying when she wants to do a ‘poo’, she goes all the way to her room to do it. I wonder why she doesn’t go to the toilet? Carer 1: Well, I don’t think she likes going to the toilets here. They’re often smelly and usually dirty. Anyway she gets lost easily, and I am not sure she can always find the toilet.
Summary
In this paper, we describe important aspects of the process of facilitating a formulation session with staff who are having difficulty managing CB in care environments. The facilitation of these sessions is an integral part of the Newcastle or Colombo approach to working with staff groups. The suggestions in this paper have emerged as a result of project work by the teams using this approach which is intended to identify and articulate the processes involved in effecting change through formulation sessions. The process of delivering formulation sessions requires many of the skills also used in conducting clinical supervision and in delivering effective training. Hence, the latter areas have provided useful frameworks within which to consider the micro-skills involved in successful facilitation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest statement
None declared.