Abstract
This pragmatic, exploratory qualitative study, as part of a larger funded research project, sought to explore families’ perspectives on what it means to value a person with dementia and how this value might influence the quality of life of people with dementia. In-depth interviews were conducted with 20 family members who used one long-term care service provider in Australia. Families described the factors influencing a positive quality of life for the person with dementia as being related to the environment and, in particular, to the resident’s room, supportive staff and individualised care that valued the person’s life experience. Family also reported a negative impact on quality of life when staff and the care facility neglected to provide an individualised approach. This study highlights the importance of demonstrating the value of the person with dementia, the family role and partnerships of care.
Background
According to Alzheimer’s Disease International (ADI, 2009) an estimated 35.6 million people globally currently have dementia, and it is predicted that this number will nearly double every 20 years as the population ages. The care and cost of people with dementia puts considerable strain on families, society and the systems of care. A number of behavioural changes are common in dementia, often presenting challenges for staff carers and family involvement in care; they are acknowledged as being linked with negative psychological and physical distress for the family caregiver (Losada et al., 2010). Behavioural disturbance, such as aggression, is acknowledged as one of the main reasons for family placing a family member into long-term care (LTC) (Brodaty, 1996). Caring for a person with dementia can reduce the quality of the relationship between the caregiver and care recipient and, in the case of married couples, this may involve both members having to adjust to new roles (Quinn, Clare, & Woods, 2009). Although the family member may have been the main source of comfort and support when the person with dementia lived in the community, there is a vast literature suggesting that, once the person is placed into care, the family member is challenged by the adjustment to yet another role, and this can result in them becoming disengaged from the family member (Bramble, Moyle, & McAllister, 2009; Gaugler, 2005). Engaging family in a care partnership is important; it has been shown to reduce some of the tensions between family and staff and to support person-centred care (Bramble, Moyle, & Shum, 2011; Pashby, Hann, & Sunico, 2009).
Over the past two decades a number of improvement strategies have taken place in LTC, in particular an improvement of the environment and emphasis on a person-centred approach to care. The question of whether these changes have helped the person with dementia to maintain quality of life (QOL) continues to be explored (e.g. Brooker, 2008; Chenoweth et al., 2009; Fleming & Bowless, 2008; Hancock, Woods, Challis, & Orrell, 2006, Moyle, Venturato et al., 2011). A range of factors have consequently emerged as seemingly influential on QOL in dementia, although the extent of influence does appear dependent upon whether the QOL is rated by the person with dementia or by proxy informants (Moyle, Murfield, Griffiths, & Venturato, 2011a; Ready, Ott, & Grace, 2004). However, the literature is clear that family caregivers are crucial to assisting the person with dementia to live ‘a life worth living’. Furthermore, the way in which the family caregiver sees their role once the person with dementia enters LTC, and the staff approach to their presence, can influence their contribution to care (Bramble et al., 2009).
Dementia impacts on most aspects of daily living, and has the potential to undermine the individual’s self-esteem and feelings of worth (Preston, Marshall, & Bucks, 2007). There is a growing body of literature that suggests valuing people with dementia may be the key to improving QOL (Brannely, 2006; Jennings, 2004; Kontos, 2005). Although an individualised or person-centred approach may assist in this process, it is not clear whether staff or family are always concerned about the enduring value of people with dementia as human beings. There is little evidence to suggest that clinicians or family believe, and convey the belief, that people with dementia retain their moral worth and value throughout the trajectory of the dementia syndrome. Research tells us, however, that judgements about a person’s worth can impair care provision (Cassell, 2004; Moyle, Murfield, Griffiths, & Venturato, 2011b).
Methods
The study aimed to explore family members’ perceptions of what it means to value a person with dementia and how this value might influence the QOL of people with dementia. The study was part of a larger funded research project that sought to inform the development of a new evidence-based model of dementia care.
Design
The study employed a pragmatic, exploratory qualitative approach, situated in the interpretive paradigm (Neuman, 2000). Interviews were conducted between August and December 2007.
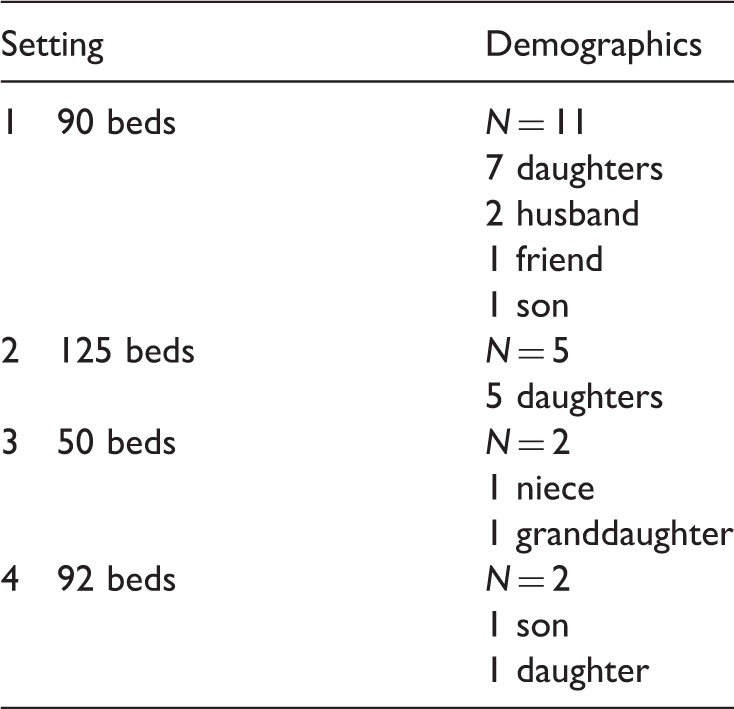
Sample and setting
Demographic profile.
Data collection
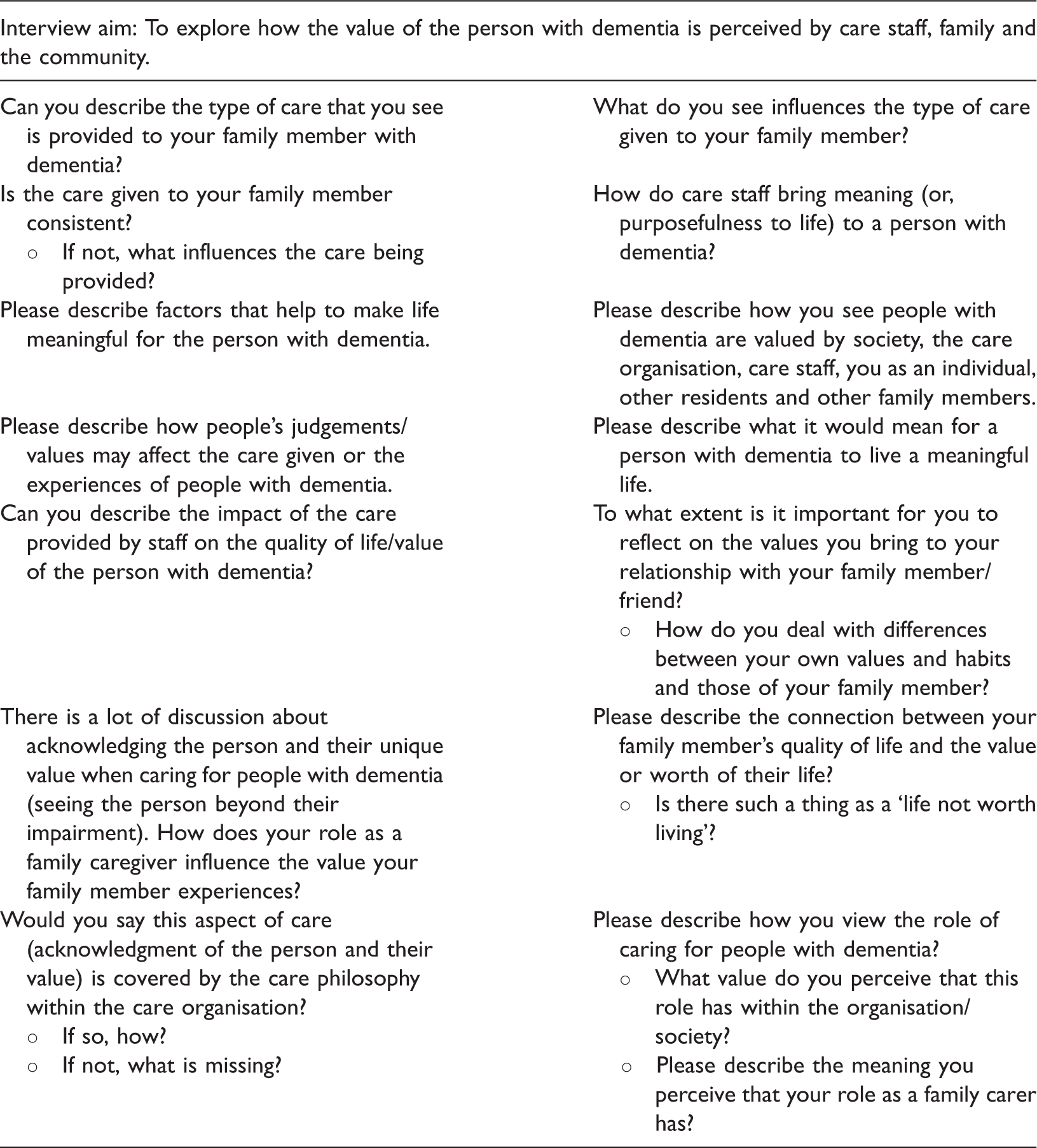
Interview schedule.
Data analysis
Analysis of the qualitative data was undertaken with the assistance of Leximancer (2009), a computer-assisted concept-mapping programme which enables mathematics-based text mining and information extraction from interview data and identifies key concepts or themes and their inter-relationships. The concepts identified by the software are rank-ordered in terms of importance – which, for this paper, were the concepts of most importance to family members’ perceptions of what it means to value a person with dementia. For ease of writing, people with dementia will be referred to in this manuscript as residents. Although the approach used for data analysis can be read in other papers (Moyle et al., 2011c), as the terminology used is specific to this study, the approach will be articulated below.
In preparation, the typed family interview data was initially tagged to indicate interviewer statements as ‘Int’ and statements by family interviewees as ‘Family’. In general, interviewer data (i.e. their questions and responses) is not considered in qualitative data analysis, but in this case the interviewer data was included because it helped to provide an audit trail to check the interviewer was staying true to the interview protocol. The interviewer statements also helped to clarify the focus of the family members’ ‘talk’, thereby enhancing understanding of what was meant in their responses. Leximancer was set to analyse a single line at a time. The method adopted included:
Findings
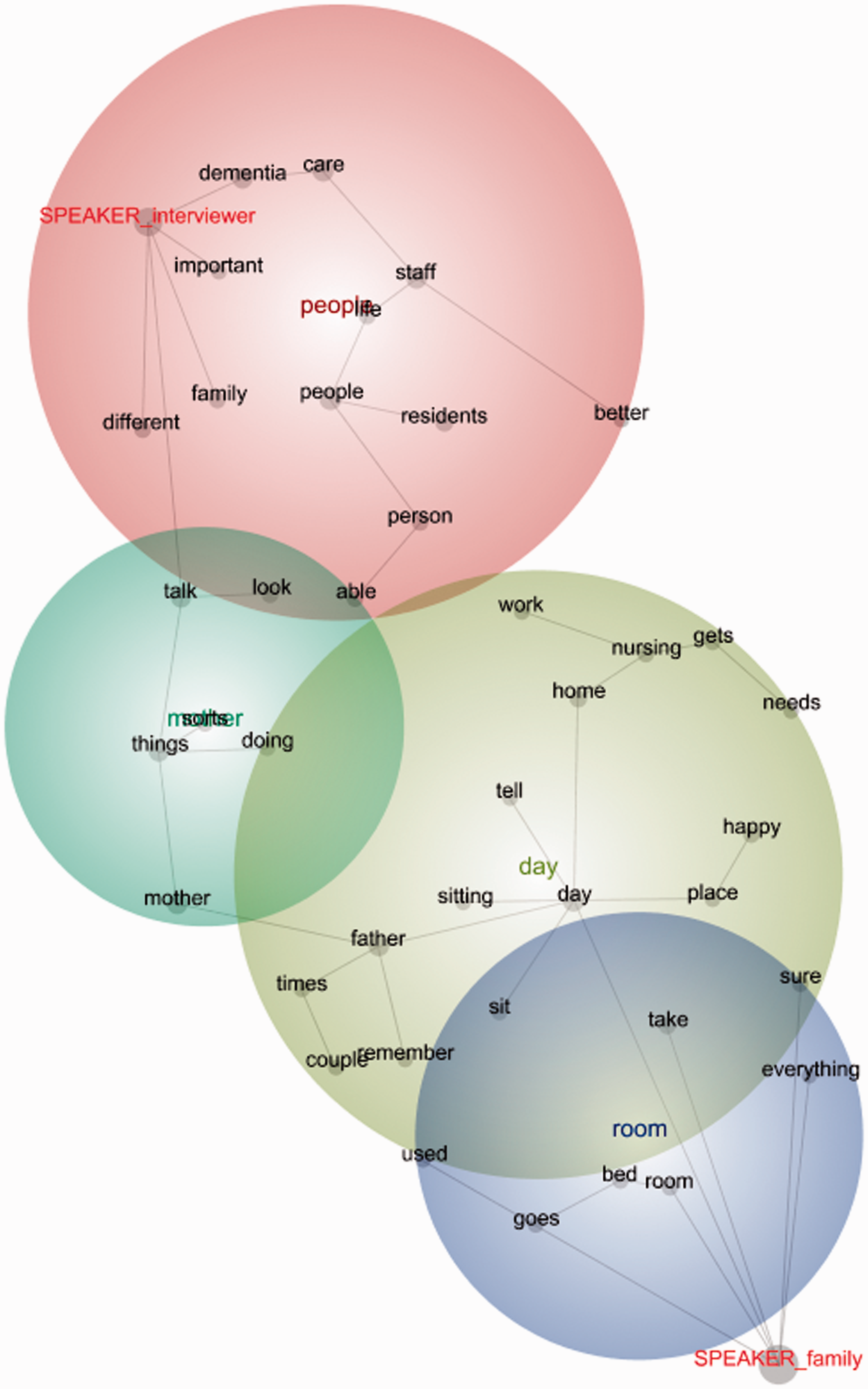
The Leximancer concept map outlines the thematic concepts that were borne out of family members’ and the interviewer’s words (talk) during the qualitative interviews.
The family interview concept map, with intermediate concepts, depicted below shows that family members’ talk was most closely associated with the thematic concept of room, and this was in relation to the two thematic concepts of day and Mother (including Mum and Dad) (see Figure 1). Interviewer talk, however, was most closely associated with the thematic concept of people, although this was again in relation to both day and Mother (including Mum and Dad). Families spoke about the room the resident went to, or sat in, and its relationship to QOL as being either a pleasant or unpleasant room. A further manual thematic investigation aimed to explore the links between the three key thematic concepts (room, day and Mother), and through an interpretative lens, the key factors influencing being valued and QOL are identified. Quotations generated by Leximancer software to give textual context to the thematic concept map are used to illustrate the general consensus of opinion that emerged from the family member interviews.
Influencing factors on being valued and QOL
The resident’s room
When discussing the resident and the factors that influence being valued and their QOL, the family member frequently talked about the importance of the long-term care environment and, in particular, their relative’s room. This conversation was directly linked to the concept of day, or the time of day when they visited. For many, the bedroom was where they spent time when visiting or was the place they returned to after being on an outing or walk with the resident. Some family members highlighted the importance of the resident’s single or private bedroom as providing an opportunity for the person with dementia to maintain a sense of self and dignity; somewhere they could continue to place their ‘mark’ on the environment through familiar objects such as furnishings and photographs. Furthermore, the private bedroom also provided a place of stability or a place of refuge in an at times chaotic environment. A typical example of family conversation includes: ‘There are some frustrating things happening sometimes, some of the residents scream for no reason and it goes on for an hour, so that can annoy Mum, she might just go to her room’. The bedroom, therefore, offered both privacy and a sense of control over what could be a noisy and stressful environment.
However, not all family member interviewees referred to their relative’s room in positive terms. In these instances, comments appeared to reflect an association between the room of the person with dementia and his/her isolation from the community of care and, therefore, subsequent lack of involvement in any outside activities at the facility. In such circumstances the private bedroom was considered to have a negative impact on the resident’s QOL. Indeed, one family member stated: ‘ … I try to say to [staff], please get Dad out to anything you possibly can because I don’t think it is good for him to be sitting in his room by himself all the time’. The families in similar examples were of the belief that the person with dementia needed stimulation and opportunities for social engagement. Although the resident lived in communal facilities, there was a perception that the resident was isolated from other residents and this may have encouraged feelings of loneliness.
Some family members also mentioned the concept room in relation to the care their relative received in the facility, and this was specifically in terms of staff not being attentive enough in tidying the room or keeping it presentable. For example: Mum would benefit from closer care in that sometimes I go and see her in her room and it is a tip. It is not dirty but she puts stuff in odd places, piles of clothes that aren’t hung up
and ‘When the [staff] that work there go in and out of his room in a day, they don’t even straighten the towels’. The untidy bedroom in what appeared to be a chaotic environment was perceived as showing a lack of respect and, therefore, limited valuing of the resident. The bedroom seemed to be a place in which the family felt there could be more structure and care provided, as a result demonstrating the resident’s importance and value within the community.
The resident’s day
Family members predominately referred to the concept day in relation to care staff at the facility and the importance of their role in the everyday life of their relative with dementia; one interviewee’s statement that ‘It is the only highlight of their day really, the people that work around them’ aptly addressed this. Comments frequently centred on the importance of care staff taking the time in the day to get to know the resident and spending time talking to them; something which they considered was not done enough or regarded as a priority by the facility. As an example, one family member explained that ‘the management don’t see it as important for staff to talk to the people and they have to hurry off all the time’ and another emphasised: ‘It is hard to understand why people can’t stop and spend some time to talk, that should be part of the employment, not just doing the work, even just for a couple of minutes talking with the elderly’. As well as the need for conversation, there were also comments about the importance of care staff providing activities and opportunities tailored to the preferences and likes of the individual, which perhaps provided a way of showing that the person was valued. Such comments included: ‘So for the caregivers … they will see that she may like to wipe the tables down after lunch and give her that particular job to do because she was always housekeeping at home’; and ‘one of the diversional therapists had sat with Mum and [name of resident] and a couple of others and they sang every song in the book and picked out their favourites to copy them to go into the song book’. The important concepts here relate to residents engaging in meaningful activity that connects them to their social biography.
Family members’ references to the thematic concept of day were also related to the deteriorating course of dementia, such as failing lucidity, memory and changing behaviour, and the influences this has on what was considered to be a deteriorating QOL. Comments that best reflected this included: ‘Mum wakes up in the morning and says to whoever is there, what day is it and what date is it?’ and I am concerned about the response I am going to get from Mum whether is it going to be a good day or whether it is going to be a bad day’. For many family members, this deterioration was clearly painful and difficult to experience as it forced a change in the nature of their relationship and, ultimately, the perception of their relative. One family member stated: ‘I said to my sister, I have done my grieving. I feel like I am losing my mother on one level. We were very close and spoke together every day on the phone’. These changes in behaviour were seen by some interviewees to directly impact on how the person with dementia was valued, with the inference that as the person’s health deteriorated, the less they were valued or understood by facility staff. As an example, one family member stated that ‘some people are not valued at all because they seem to be, without being rude, away with the fairies all the time’ and said ‘she is in the same clothes from one week to the next, Mum hasn’t had a shower and we have told them so many times that we would like them to shower her, but different staff on, different nurses’. This perceived lack of attention to everyday things resulted in the view that the resident was not deemed worthy of respect.
The resident (Mother, including Mum and Dad)
Given that the interviews concerned a family member’s perception of the care, value and QOL of their relative with dementia, it is not surprising that there were numerous references to Mother. However, in addition to these general conversational references, there were also times when the thematic concept was used to reflect how the family member perceived and valued the person with dementia. Typically, interviewees again lamented their relative’s deterioration because of the disease, which was painful for them to observe and be part of: ‘When I say to people about my mum they say my parents died really young and I say you are so lucky because you don’t have to see them deteriorate’. Many considered the course of dementia to be cruel and essentially to be reducing their relative’s QOL: ‘Yesterday I spent some time talking … I said it is a shit of a disease we all know that, it is not what we would want for Mum but this is the way it is and we can’t change it’. A number of references were made to the tension of wanting to terminate the disease while also recognising that this would result in a loss of the person. An example is: ‘[a] horse going crazy and biting people you put it down, but she is my mum and will always be’. Some relatives also expressed guilt over placing their family member in the LTC facility, feeling that they had somehow left them there alone. For instance: I still hate it with a passion, I hate that walking out the door every time, but it certainly makes me feel like they are caring enough that they will go and see Mum and see that she is not just sitting there waiting for me to come back when I have already gone.
Family members also used the thematic concept of Mother when comparing their relative’s behaviour with another person with dementia in the LTC facility. In some instances, these comparisons provided reassurance that ‘… there are probably worse people than Mum’. However, in other instances they showed the extent of the relative’s deterioration: ‘The majority of the people that are here, they are all happy and wander around and talk with the other residents but Mum doesn’t talk to even the nurses’. Such comparisons may have served to help the family member process and understand the changes seen in their relative by potentially placing it in the context of others with a diagnosis of dementia.
Discussion
This study identified that when discussing what it means to value a person with dementia, family members most often made reference to three main concepts: room, day and Mother (including Mum and Dad). Although each of these concepts can be considered separately, the interrelationship between them is a result of the need for the resident to be treated with respect and dignity and, therefore, to be valued as an individual rather than thought of as a collection of symptoms of a disease process. To provide context and illustrate the general consensus of opinion that emerged from the interviews, analysis of extracted ‘talk’ in which reference to these three concepts was made was undertaken using Leximancer software.
The environment was important to family members who identified the provision of a personal space, such as a private bedroom, as one way of continuing to value a person with dementia. A private room enabled the person with dementia to be able to take pride in their own space and, when the room was perceived as clean and comfortable, family perceived that their family member was being appropriately cared for. In addition, the private bedroom also offered welcome refuge and a place for solitary time away from other residents and care staff when needed. This suggested that a private space enabled the person with dementia to maintain a sense of self and to maintain their dignity whilst living in a facility and requiring care. However, family members also perceived that valuing a person with dementia also involved staff getting residents out of their room, offering opportunities to participate in outside activities and providing appropriate stimulation. In this sense, family members considered it important not to isolate the person with dementia and confine their world to just their bedroom, or the rooms of the LTC facility. Sharing with others with, and without, dementia and being with other residents was assumed to help normalise the situation (Preston, Marshall, & Bucks, 2007). Furthermore, family members considered that an outward expression of valuing the person with dementia was respecting their personal space. Thus, care staff could show that they valued and respected the person with dementia by keeping the resident’s room tidy and presentable.
Family members perceived care staff to be central in how a person with dementia was valued as, for many, staff were ‘the only highlight of their [the residents’] day’. Family members identified two main ways in which care staff could show they valued the person with dementia. This included firstly taking the time to talk and/or sit with the resident and, essentially, moving away from a task-orientated focus. Secondly, care staff could provide opportunities and activities specifically tailored to the interests and preferences of the person with dementia. By doing this, care staff could show that they recognised the person with dementia as an individual and valued them enough to provide activities of particular interest to them. The findings also support other studies which suggest that the staff focus is often predominately on residents’ physical, rather than emotional, needs and that residents spend a large part of their day alone (Harmer & Orrell, 2008; Moyle et al., 2011c).
Family members also identified that the way in which the person with dementia was valued was inherently linked with the course of the disease and the extent of deterioration. For many family members, the changes in lucidity, memory and behaviour forced them to change their perception of their relative, and this was often painful, upsetting and similar to a grieving process. Some relatives also expressed guilt over placing their family member in the LTC facility, feeling that they had somehow left them there alone. Such findings are supported by other research demonstrating that the loss and grief experienced by family caregivers at the time of diagnosis continues even when people are placed into LTC (Bramble et al., 2009; Moyle et al., 2002).
There was also a suggestion that the greater the deterioration in health, the less the person with dementia was valued or understood by care staff, and this was visible when residents were in ‘the same clothes from one week to the next’. Family members were challenged by the identity of their family member being eroded and, when the individual and their characteristics were ignored, the perception was that the person was being treated as if they were of little value to society. In this sense, the person and their abilities were positioned negatively, as they were only considered in terms of the symptoms of dementia. The acknowledgement of negative attitudes toward and stereotypes of older people with dementia is important to understand because, if treated with disrespect, the person with dementia may come to believe that they are unworthy and incapable, and such feelings may have a crucial effect on self-esteem and subsequent care provision (Dein & Huline-Dickens, 1997).
Finally, family members often compared their relative’s course of dementia with that of others in the LTC facility, and this may have been a way in which they sought to process and understand the changes and place them in context. For some, the comparisons provided reassurance that their relative was perceived to have a better QOL than others with dementia. However, in other instances the comparisons served to show the extent of the person with dementia’s deterioration.
The importance of role
On one level, this study shows us what families see from their perspective. However, it could also be hypothesised that some of the family caregivers, through their change of role, have lost a sense of attachment to the person with dementia and, in so doing, relied on staff to maintain the highest possible care; they may therefore have felt a sense of dissatisfaction when the care provided was substandard. Others appeared to subsume themselves within the care situation and were concerned with every aspect of life, as they were not yet able to separate or define their new role (Ingebretsen & Solem, 1998).
The importance of these findings lies in understanding the families’ perspective, as the factors of importance to them may provide opportunities for staff to work with families and, therefore, assist in integrating family into the LTC community as a partner in care. Incorporating families into the care environment will, no doubt, meet the needs of residents who benefit from the meaningful connections that families can bring into their lives (Moyle et al., 2001c). In order to further consider the findings of this research, it would be helpful to explore additional interventions to assist the family caregiving role following the transition of the person with dementia into nursing home care.
Determining preferences
There is an increasing body of research indicating that family and staff are relatively inaccurate in determining the preferences of people with dementia (Mesman, Buchanan, Husfeldt, & Berg, 2011). It is important, therefore, that the voice of the person with dementia is included in planning such interventions. As previously indicated, this project was part of a larger one that explored QOL and value. The findings suggest that the person with dementia and family caregivers had different perceptions about QOL and value. The person with dementia reported that factors influencing positive QOL were related to relationships with family and other people and ‘things’ such as needing to feel some control over the decisions made about their life, including care (Moyle et al., 2011c). Joint interviews may assist families and staff to understand the needs and perceptions of people with dementia (Keady, Nolan, & Gilliard, 1995; Thein, D’Souza, & Sheehan 2011). Furthermore, formal, participatory partnerships between staff and families may also assist in this endeavour (Bramble et al. 2011).
The results from this qualitative investigation highlight a number of practical ways in which care staff and family members can show that they value a person with dementia. In particular, the importance of family–staff partnerships in care may help to reduce staff–family tensions and improve QOL for people with dementia. In terms of care staff, this includes: taking a few minutes each day to talk and/or sit with the person with dementia; providing regular activities that are tailored to the individual preferences and likes of the person with dementia; respecting the person with dementia’s personal space by keeping their bedroom tidy and presentable; and engaging with family members on a regular basis. As regards to family, they should encourage their relative to become involved in activities within the facility so as to reduce feelings of isolation and loneliness and also, facility policy permitting, encourage the person with dementia to make their bedroom feel personal and ‘homely’, so that they can express their individuality and maintain a sense of self. It is especially important to provide such ways in which the person with dementia is valued when the course of dementia is more severe, given that this study found that family members perceived the value of a person with dementia to be inversely related to the extent of deterioration.
Footnotes
Acknowledgements
The research team gratefully acknowledges the help and support of the residents, family and staff at the four RSL Care facilities. Also acknowledged is Ms Debora Osborne for her help with the conduct of interviews, Mr Kris Roobottom for his assistance with the initial Leximancer analysis and Ms Deborah Oxlade for her help as liaison between the facility staff, residents and family and the research team.
Funding
This paper reports on an outcome of a larger collaborative research project funded by the Australian Research Council (LP0775127) under the Linkage Project Scheme for 2007–2009 and RSL Care, the industry partner. Family interview concept map with intermediate level thematic concepts. Notes. SPEAKER_int = interviewer; SPEAKER_family = family member.