
Abstract
Background:
The cognitive, emotional, and psychological consequences of dementia are profound and can include memory loss, processing and, communication difficulties, social isolation and agitation. Procedural memory remains fairly intact in people with dementia (PWD) and is readily triggered via sensory cues and prompts. As religious services are often highly structured, it is likely that PWD can participate competently, potentially enhancing their quality of life, and wellbeing.
Aims:
This study aimed to investigate Christian worship leaders’ attitudes and observations of PWD attending religious services, to identify recurring themes, and to generate hypotheses regarding the effects of participation in religious services on PWD.
Method:
The participants were Christian worship leaders experienced in conducting religious services for PWD. The study adopted a grounded theory approach consisting of two phases: a focus group of four worship leaders at Phase 1 and a series of one-to-one interviews with eight worship leaders at Phase 2.
Results:
Five linked themes emerged: familiarity and structure; enhanced sensory cues; significance of worship leader’s approach; social support from and for family and carers; and the personality and characteristics of the PWD. These themes were used to develop a conceptual model, sharing the moderating and mediating factors of wellbeing.
Conclusion:
Religious worship appeared to constitute a naturalistic psychosocial intervention comprised of the service itself and the social context. Further investigation and conceptualisation of the interaction between PWD and their social environment is warranted, and collaboration with those people who constitute the PWD’s social support network.
Introduction
Within the last decade, in accordance with the person-centred approach, commentators have paid increasing attention to the role played by spirituality and religion in meeting the needs of People with Dementia (PWD), and thereby enhancing the lives of PWD and those of their carers (Swinton, 2007; Dakin, 2009; MacKinlay, 2011). It is argued that participation in religious rituals and services by the person with dementia provides an opportunity to address his/her needs. For example, in relation to their pastoral care, where such care is perceived as being ‘… meaningful as a way of manipulating symbols through ritual in order to create a greater sense of security and connectedness despite fragmentation and loss’ (Post, 2006, p. 228). This includes ‘affirmation of God’s presence’, an experience that offers great comfort and meaning for a person of faith (Dakin, 2009, p. 27). These views are based on expert consensus and theoretical perspectives, rather than empirical data.
A Mental Health Foundation research report, which used evidence that drew directly on PWD’s own views and experiences, identified a person’s ability to practise faith or religion as one of 10 key quality of life indicators (Alzheimer’s Society, 2010). From a policy perspective, national guidelines highlight the central role of respect for religious beliefs and spiritual and cultural identity in providing Person-Centred Care (PCC, NICE/SCIE, 2006). A stated principle of care is that it is incumbent on professional carers to identify the religious beliefs and spiritual needs of PWD, to accommodate preferences and to support their faith, spirituality and tradition. Similar guidance has been directed towards the psychiatric profession (Department of Health, 2007). Again, these principles are based on expert consensus and theoretical perspectives, rather than empirical data.
A possible consequence of the lack of empirical data is that a gap exists between policy and practice. For example, Grey (1994) concluded that, among other factors, care staff’s poor awareness of spiritual matters, uncertainty about their personal beliefs, and fear of incompetence, means that care staff often experience difficulties in supporting PWD’s faith needs, and guidance is not implemented (Goldsmith, 2004). Similarly, studies of the psychiatric profession indicate that psychiatrists often fail to accommodate the religious beliefs of patients as a result of their own prejudices and lack of awareness about religious faith (Koenig, 2008). These examples suggest that care staffs’ and psychiatric professionals’ attributions may lead to the development, or maintenance, of malignant social psychology of care (Kitwood, 1997). Within this context, the present authors believe the study of worship leaders’ attitudes and observations of PWD will enhance our understanding of the above processes and therefore is worthy of empirical investigation.
In the present context the term ‘worship leader’ is used to describe those individuals who are the principal coordinators of a worship carried out according to a certain prescribed form within a denomination (e.g. a cleric, celebrant, celebrant, elder, minister, vicar, pastor, priest, etc.).
Phase One – The focus group consisted of four participants, three male and one female with a range of 2–33 years experience of working with PWD. Three participants were ordained ministers, one was an Honorary Chaplain. All were currently employed as NHS Chaplains, all defined their ethnicity as White British and were drawn from four denominations of the Christian faith: Roman Catholic, Church of England, Methodist, and Baptist.
Interview participants’ demographic information for Phase 2.
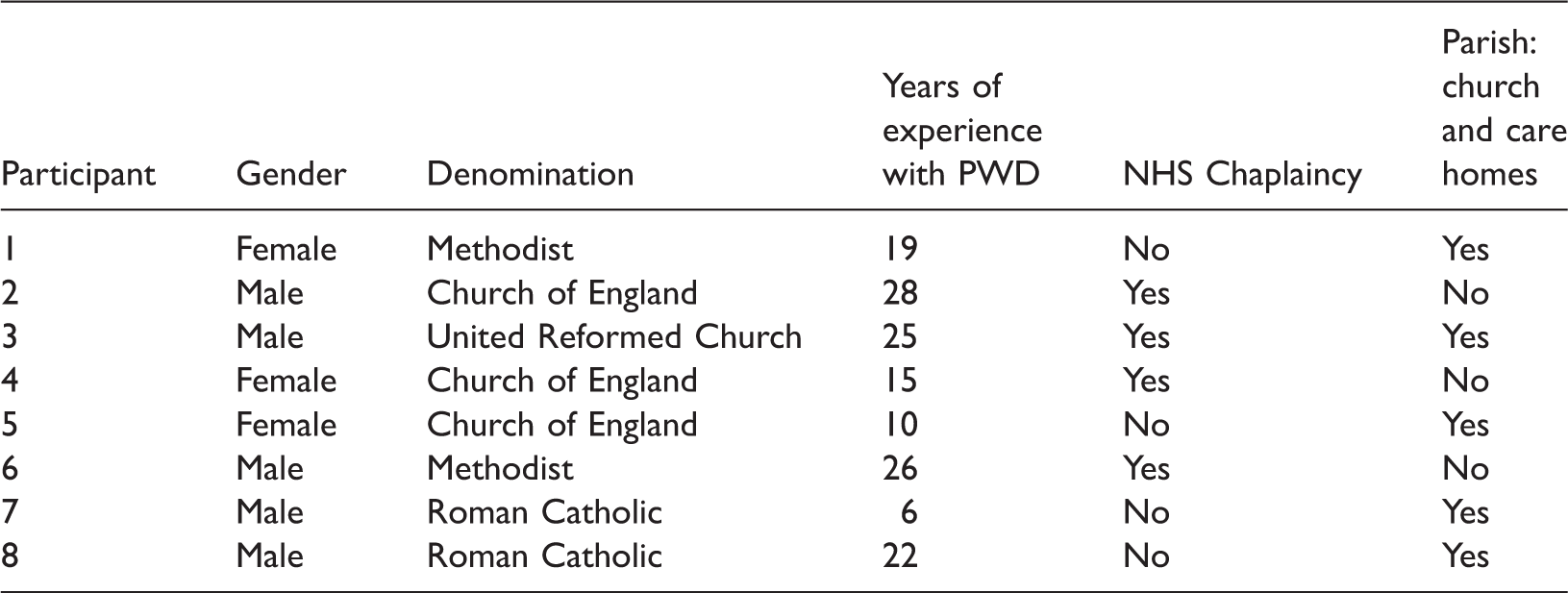
Design: An hour-long focus group was held with four participants. Themes arising from the focus group were used to develop the initial semi-structured interviews. Eight individual one-to-one interviews were held with participants lasting approximately 1 h each. The contents of each interview were guided by the emerging themes from the earlier stages of data analysis and thus the interview schedule evolved as more interviews and analyses occurred. All individual interviews were audio taped, transcribed and a thematic analysis was undertaken using Computer Assisted Qualitative Data Analysis Software (CAQDAS) NVivo8 (QSR International, 2009).
Ethics
Ethical approval was granted by Northumberland Tyne and Wear NHS Foundation Trust Research and Clinical Effectiveness Department and by County Durham and Tees Valley 2 Research Ethics Committee.
Results
The focus group provided topic headings to discuss in the initial interview, such as memory triggers (e.g. hymns, prayers); visual aids and objects (e.g. cross, candles); relationship with family and community; denomination; clergy; practical dilemmas (e.g. suitable environment); sensory stimulation. In Phase 2, five themes emerged: Familiarity and Structure, Enhanced Sensory Cues, Worship Leader’s Approach, Social Support, Personality and Characteristics of the person with dementia. The following section presents the five themes and their sub-categories, with illustrative quotes from participants.
Theme 1: Familiarity and Structure
This category constitutes the factors that were most salient for participants. Traditional ‘age appropriate’ hymns and prayers were observed by all participants to be a primary means of facilitating engagement. (Participant 3): ‘If we gave them the familiar hymns they were very much part of worship experience. They were able to join in with what they were familiar with when they were younger’.
The Lord’s Prayer was reported as most accessible for PWD. (Participant 6): ‘There was one lady I visited, all she could say was the word ‘visitor’ … except The Lord’s prayer. She could say The Lord’s Prayer with me, and as soon as we finished she was unable to say any other word’.
All participants perceived that set pieces of wording acted as trigger phrases for engagement. (Participant 6): ‘Even just saying “let us pray” is a trigger phrase for them to adopt a certain posture … their eyes closed, hands go together, even among people who appear not to be engaged at all’.
Four participants observed that familiar hymns and prayers elicited engagement of PWD who were traditionally non-churchgoers. Familiarity was perceived by all participants to create security. Hymns were observed to be an important means of creating a structure for experience within worship and sustaining people’s engagement. Participants considered the consistency (eight participants) and simplicity (six participants) of the hymns to be important: (Participant 4): ‘I always try to have that little framework, something to open, something to listen to, something to join in, something to explore, and something to finish with. You need a structure and just explore what works, what doesn’t work’.
Many participants felt that giving a set structure to a Service provided a familiar pattern which a person could identify with, particularly for individuals in an advanced stage of dementia. However, the ability to provide flexibility in the form of one-to-one worship was necessary at times for those who were either very frail or extremely agitated. Engagement was perceived by all participants as creating a sense of normality, a sense of belonging for the person with dementia, and an opportunity for self-expression and self-efficacy. (Participant 7): ‘They fit in, they know when to kneel and stand, they’ll sing and they’ll answer’.
All participants observed changes in emotional state during services, and five described PWD as ‘more relaxed, at ease and peaceful’ within the context of a service.
Theme 2: Enhanced Sensory Cues
For all participants, sensory stimulation was critical to providing an experience that people would find meaningful on a spiritual level. For all participants music and visual cues such as colour and symbols, the Bible, the cross and clerical collar, facilitated orientation to place and time: (Participant 2): ‘Music is so important… it clicks in people “Oh, yes, I’m in church now, this is where I am”. (Participant 1): ‘I would usually wear my cassock … the symbolism would be important, it sets the scene’. (Participant 7): ‘Colour will be evocative of the season’. (Participant 4): ‘Lighting a candle can be such a significant moment, you can see it in people’s eyes … giving someone with dementia a candle to hold can be like giving them a lottery winning … eyes open and start to sparkle. Linking sound with colour and movement … using coloured scarves and flags, and simply moving around the room with those to particular music tracks, and seeing the response on people’s faces, as, if you drift a flag gently over their heads, the whole face would just come alive. A lady sat absolutely entranced and rapped, and wanted to hold a flag and move it herself and engage’.
They were perceived to act as memory triggers (all participants) with layers of meaning for the PWD and to elicit changes in emotional state. (Participant 8): ‘Whether it’s linking into memory of when they were at school or church, or saying the rosary back home … but it can be a source of making them more peaceful. The receiving of Communion … the physicality of that … getting something to eat and the memory of that from childhood).
All participants perceived the importance of touch in providing comfort and attachment. Touch included physical contact, the holding of objects (hymn cards, holding cross) and anointing with oil or holy water. Tears (often perceived as joy, relief) were frequently observed.
Theme 3: The Significance of the Worship Leader’s Approach
This theme was the most developed in terms of its properties and dimensions. It comprises several key sub-categories: relationship, monitoring, wellbeing, insecurity and ethical, practical and theological dilemmas. All participants identified the relationship between the worship leader and PWD, and knowledge of the people as being central to eliciting engagement. Within this, careful use of non-verbal communication (eye contact, eye-level, touch) (eight participants) and a contemplative stance (being attuned to the person, an unspoken connection between people) (three participants) were considered essential. (Participant 1): ‘You have to make a relationship with people. You have to project your personality’.
All participants perceived themselves as having a ‘special relationship’ with parishioners, that operated on both a symbolic and an emotional level and provided for PWD a sense of connection with God and a sense of security, of being in safe hands. (Participant 2): ‘People see the collar and you do represent something almost that feeling “we’re in safe hands”’.
Four participants described monitoring well-being, recalling incidents of distress for PWD, and of responding in a low key manner. Participants regarded distress as a positive effect, providing an opportunity for the processing of difficult emotions, provided the emotions were contained and validated. Most participants were reluctant to draw conclusions about the causes of the PWD’s distress or failure to engage in the worship, without fully understanding the wider context of the PWD.
Worship leaders’ insecurity was reported by three participants to impact negatively on their willingness and ability to conduct services with PWD. The insecurity seemed to be about not feeling able to cope with the unpredictability of the situation: (Participant 2): ‘There was a degree of nervousness amongst those clergy at going into a unit for PWD …there was a fear, what will people do, will they be able to join in with things and respond to it?. It’s not unusual for my feeling at the beginning of the service … I wonder how we’re going to do here today … that’s quite frequent, the fear at the start’.
All participants perceived that worship leaders’ personality and flexibility were key factors in successful ministry to PWD: (Participant 6): ‘I talk about busking in that you don’t know until you get there which approach is going to be needed, because it depends on the congregation, but the busker isn’t making it up as they go along, they’re using pre-practised chords and songs they’ve used in other situations’.
Seven participants described undergoing standard training for ministry, but no training in working with PWD. However, some felt that aspects of their training for ministry and reflective practice provided guidance. (Participant 6): ‘All training for the last thirty years has included psychological elements to it …Training for person centred care,… that’s very high on the agenda’.
Participants reported that ministering to PWD was an experience of personal growth. All participants reported conflicts and dilemmas that impacted on their ability to provide PCC. Six participants reported concerns about failure of care staff to gain the consent of the person with dementia to participate in acts of worship, two reported concerns about failure of care staff to accommodate religious needs, and all experienced these as ethical dilemmas. Often these arose due to the practicalities of the care environment: (Participant 6): ‘I’ve always felt uncomfortable with taking services in a communal lounge where everyone is, because people don’t have the opportunity to opt out’.
Three participants expressed great concern that staff attitudes often (unintentionally) led to bad practice. (Participant 5): ‘They felt that they had to get me a good congregation, so they would say “Come on, are you coming to the service?” as if it was like the pictures … it was as if they were all being herded in to this thing happening … that created confusion for them’.
Three participants reported examples of good practice including care home residents being taken to the local church service, or ministers being provided with an appropriate room and invited to give Communion to identified residents. Three participants reported dealing with these dilemmas directly: (Participant 6): ‘I’ve always said to a home if I’m offering worship, “Can we have a separate room for this?”’.
adaptations to practice (specially devised hymn cards), or on-the-spot problem-solving (allowing a PWD to make an offering). Communion was perceived by all participants as the most significant ritual for churchgoers, and was the most frequently cited example of adapting practice to the needs of PWD: (Participant 1): ‘If you use wafers, they give it back to you. They receive by intinction, which is dipping the bread, and then by the time it reaches their mouth it’s nearly dissolved, so they don’t give it back’.
Theme 4: Social Support from and for Family, Community and Professional Carers
This category pertains to the role of social support from worship leaders, relatives and carers for PWD, and support of relatives and carers by worship leaders. Social support for PWD included the shared experience of worship within community congregations, with care staff, residents, relatives in homes and hospital wards, and one-to-one with clergy. (Participant 1): ‘It felt like a service … about half a dozen visitors from the local churches came to support as well as staff’.
All participants perceived the act of worship as providing social support for the person and their relatives. Seven participants described it as a source of strength and comfort to the person with dementia and carers and reported changes in their emotional state. (Participant 2): ‘If the person’s partner comes along it can be a very important time … it may be that it’s something they’ve lost the ability to share as a couple … to be able to participate in worship together … is moving for the partner and the person themselves’.
The shared experience was perceived by all participants to have layers of meaning and to create a sense of belonging for the person. (Participant 1): ‘It could be that it reminded them of times they went to church and took Communion with their family and friends, and that community.
Six participants described how church members, staff and volunteers provided practical support within services and offered containment when PWD became distressed, often this involved moving closer to the person and offering soothing touch. Supporting the identity of the PWD (five participants) and remembering on their behalf (three participants) was reported as an important aspect of social support. (Participant 5): ‘Relatives find comfort knowing that their Mum, Dad, whichever, is receiving this’. (Participant 1): ‘What do you do when you can’t remember? How are you still part of a community of faith? So obviously we have to remember for them’. (Participant 5): ‘They wanted somebody who actually knew their Mum… in an area that was very important‘.
Theme 5: The Personality and Characteristics of the Person with dementia
This category was the least developed of the five themes, but was considered important by participants. It comprises two sub-categories: the personal history of the person, and his/her stage of dementia. Both impacted on worship leaders’ ability, and choices about how, to elicit engagement, enjoyment and a sense of connection. (Participant 1): ‘All the time she was saying “God help me” and the staff thought it was just a loop she’d got into, but somebody did some digging about her past life. She used to be a churchgoer until she got married, her husband wasn’t a churchgoer so she didn’t go anymore, and as soon as we started bringing her to the service … she stopped saying it’. (Participant 6): ‘If someone was in an advance state of dementia and I couldn’t do anything else with them I would sing a hymn with them and they would join in’.
Synthesis of the findings
A conceptual model was developed on the basis of the above results (Figure 1).
Moderating and mediating features of spiritual wellbeing.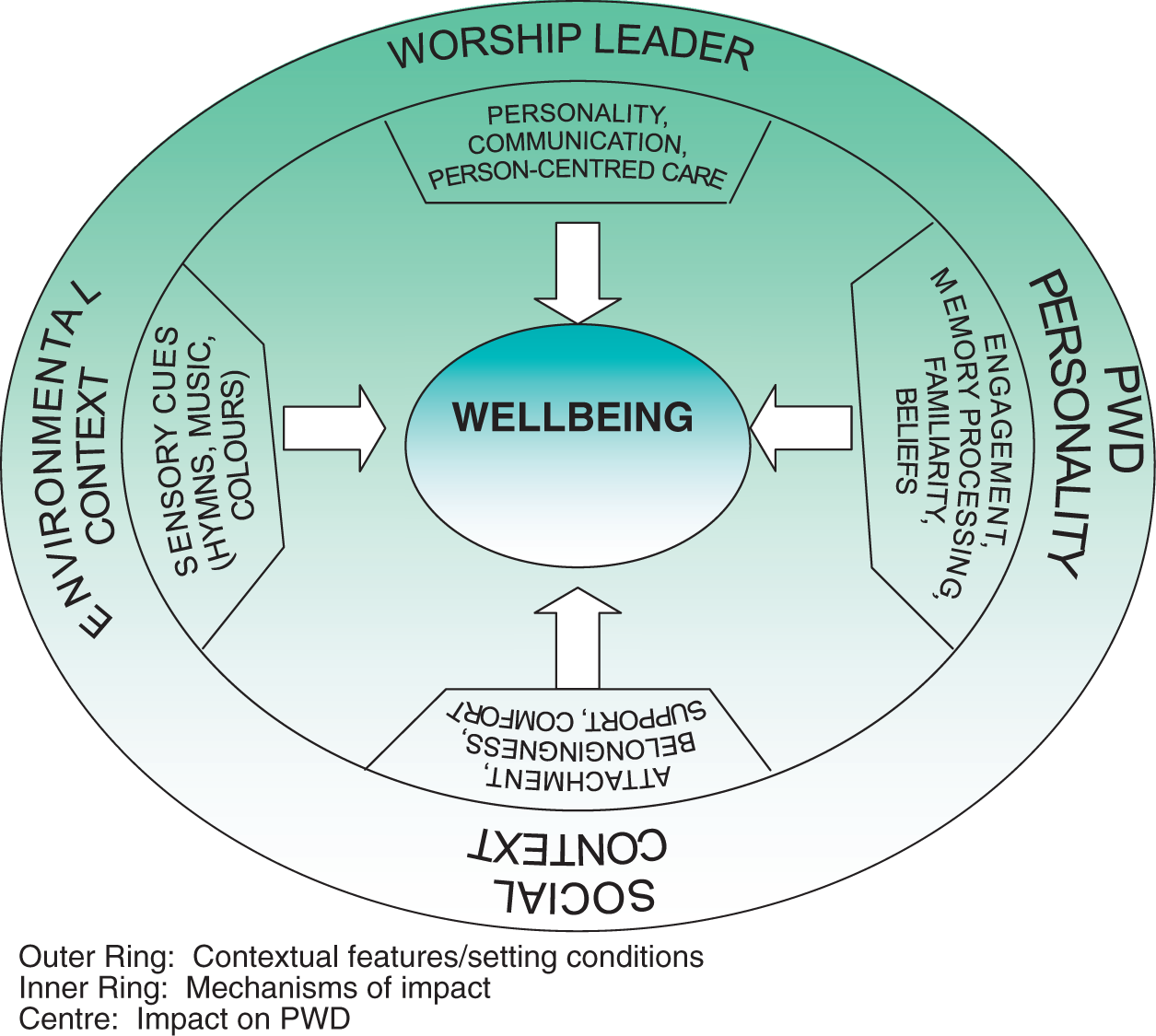
This model attempts to describe the moderating and mediating factors implicated in the wellbeing of the person with dementia. As such the model is data driven, describing the interaction between moderating factors such as the PWD’s personality, worship leader’s style and the contextual and environmental features and mediating factors such as use of sensory cues, fostering of attachment and support, attitudes, use of routines. At the centre of the model is wellbeing, set within the context of the whole person. Further, the personality and characteristics of the person with dementia are perceived to determine their cognitive appraisal of, and emotional response to, the service and its components, while the PWD’s needs are perceived to be met through the process of engagement, experiences of attachment, and a sense of support and belongingness. It is relevant to note that the outer layer of the model is represented as both enveloping the model and as operating at every level of the model to influence wellbeing.
Discussion
The findings suggest that religious services provide a socially supportive environment in which the various components of the service contribute to a ‘stress buffer effect’ for PWD by meeting fundamental psychological needs (Coyne & Delongis, 1986). For example, participants perceived that the familiarity and structure that worship services offer (through the use of traditional rituals and symbols) engendered feelings of security, normality, a sense of belonging and self-efficacy in the PWD attending. The use of sensory cues as part of worship was perceived to facilitate comfort, attachment and a sense of connection (to other worshippers, and to God).
The presence of, and interaction with, worship leaders, carers and relatives was perceived to offer the person with dementia a shared experience incorporating containment, validation of emotions, security, inclusion and validation of the identity of the person (both as an individual for whom relationship, attachment and belonging is important, and as a person of faith, for whom religious expression and ritual were perceived as central).
The effects of these forms of support were reported to be observable and evidenced in the improved functioning of PWD within the environment of the worship service. For example, in PWDs’ direct responses to sensory cues and prompts (e.g. praying, singing); in their active engagement with aspects of the service and with the worship leader, carers and each other (making eye contact, smiling, holding hands); and in changes in their emotional state (e.g. enjoyment).
Stimulation of memory, both verbal and non-verbal, was seen as a key process through which many of the positive effects were obtained. The participants noted that familiarity and sensory stimulation triggered specific memories of events from the past (i.e. episodic memories, Tulving, 2000) and that retrieval was aided by the structures within the service. In this context, negative affect was not perceived by worship leaders as a negative outcome of the service for PWD, but potentially as a positive outcome, in terms of emotional release and emotional processing leading to resolution of internal conflicts.
In relation to non-verbal forms of memory (e.g. memories for actions, procedural memories, Baddeley, 2002), the use of familiar hymns and prayers and traditional visual symbols were perceived to act as automatic triggers to long-term, well-established memories (i.e. an automatic awareness of when to stand, sit, kneel, make a response, recite a prayer, etc). It was commonly perceived that many of the long-term memories elicited had been learned in childhood and/or at school, and therefore had resonance for non-churchgoers too.
Clinical implications
Worship services comprises certain intrinsic components and qualities that appear to have particular meaning and positive effects for PWD and their carers. Though some components are specific to religious rituals (e.g. hymns, prayers, iconic symbols), many components are present in, and transferable to, other contexts (e.g. enhanced sensory cues, positive social support). In this respect, many of the components identified in the course of this study can be used to inform other forms of psychosocial intervention in other settings.
The findings of the present study suggest that worship services constitute a naturalistic and meaningful psychosocial intervention in their own right, comprised the service itself and the social context, effectively supporting the needs of PWD. As such, these findings lend support to existing policy directives regarding the central role of religious observance in relation to the identity and wellbeing of people of faith. Further, the findings of the present study can inform training programmes (e.g. for worship leaders, health professionals, care staff, relatives) to increase understanding, not only with regard to the value of identifying and accommodating religious and spiritual needs, but also of the application in other settings of components/interventions such as sensory stimulation and person-centred approaches. Within the curriculum of such training we would recommend the inclusion of the writings of people like Swinton (2007) and MacKinlay (2011) and their views on what it means to be human and live humanly within the contexts of faith, personhood and dementia. Finally, the findings may be of value in helping to ensure that the religious and spiritual needs of PWD are incorporated within assessment and care plans, an omission highlighted by Koenig (2008).
The study has several limitations, including the fact it interviewed a small sample of worship leaders. However, saturation was achieved after the eighth participant. A further potential problem was that no additional method of data collection was used to validate the findings. Indeed we are aware that if another method had been used, a different perspective may have been achieved, serving to either corroborate or challenge our findings (Green & Thoroughgood, 2009; Pope & Mays, 2006; Willig, 2008). Options for triangulation that were considered included conducting interviews with carers (e.g. care staff and relatives) and direct observation of religious services by the researcher. However, for ethical and pragmatic reasons it was not possible to apply these methods of data collection and analysis to the present study.
In relation to future research, this project is exploratory, representing the first stage of the research cycle. Possible directions for future research include the development of appropriate guidelines and training for worship leaders. It would also be interesting to investigate the views of carers and PWD. Furthermore it would be useful to examine peoples’ views across different faiths.
Conclusions
Participation in religious worship by PWD appears to constitute a naturalistic psychosocial intervention comprised the service itself and the social context that brings together a range of supports and cues in a meaningful way for the person with dementia. If these efforts are to be effective and productive in terms of developing understanding and implementing appropriate interventions, this process demands collaborative engagement with those people who make-up the PWD’s social support network. In summary, the results of the present study will be helpful in informing the work of worship leaders, potentially contributing to the development of further guidelines and flexible ways of working. The findings may also contribute to care assessment and planning for PWD, and also direct future research in the area.
Footnotes
Funding
The author(s) received no financial support for the research and/or authorship of this article.