
Abstract
This paper outlines an intervention protocol used to educate carers in a project that implemented and evaluated a capability model of dementia care (CMDC) in three long-term aged care facilities. It outlines an evaluation of the content of the education and processes used to deliver the intervention through an analysis of surveys and reflective field notes. The education protocol was designed for adult learners and grounded in the six assumptions of Knowles' learning theory. Results suggest the education protocol positively impacted on the knowledge, skills and attitudes of participants towards providing quality dementia care to residents in long-term care. The paper also acknowledges the challenges involved in sustaining a practice change through an educational intervention.
Introduction
Caring for people with dementia is a very demanding and complex task and while there are examples of excellence in dementia care there are many more examples where provision of care is of a low standard. Increasing staffing in some care homes may improve quality of care; the evidence, however, suggests that it is the quality of staff, in particular the level of their skill and training, which contributes to quality dementia care and resident quality of life (Burgio et al., 2002; Commission for Social Care Inspection, 2008; Zimmerman et al., 2005).
The aged care sector and care of older people continue to be challenged by the increasing number of unregulated care staff employed in the sector. In Australia, the number of personal care workers ((PCW), i.e. assistants in nursing) in long-term care continues to rise (89.5% increase in PCW numbers between 2000 and 2005), while the number of qualified staff declines (Australian Institute of Health and Welfare, 2006). A large ratio of skilled staff to unskilled staff has the potential to affect the quality of care. As such, improving the knowledge, skills and attitudes of staff and their perceived value in the workplace is an important starting place for shifting the standard of care from the minimum to the highest possible potential (Nakahira, Moyle, Creedy, & Hitomi, 2008).
The role of staff in providing quality dementia care and enhancing resident’s quality of life cannot be overstated. The ability of staff to provide ethical and quality care is related to the level of commitment a person makes or is prepared to make and the way they view the care recipient (Edvardsson, Winblad, & Sandman, 2008; Jennings, 2004). The beliefs, values and life experience of the caregiver inform their judgments and thus their potential to impact the person with dementia either negatively or positively (Moyle, Murfield, Griffiths, & Venturato, 2011a). Education is a valuable tool in challenging beliefs and values that have the potential to compromise the sense of value experienced by the person with dementia (Foreman & Gardner, 2005). Aylward, Stolee, Keat, and Johncox (2003), in their literature review of studies conducted with long-term care staff, argue that: (1) there is minimal evidence that continuing education programs are effective; (2) the critical issue in successful knowledge transfer and behaviour change is staffs’ understanding of the relevance of these to their practice; and, (3) a program that incorporates organisational and system factors is needed to sustain change.
This paper outlines an education protocol used for carers as an intervention in a project that implemented and evaluated a capability model of dementia care (CMDC) in three long-term aged care facilities in Queensland, Australia. The CMDC (developed by Moyle and then reviewed by an international panel and pilot tested (Moyle et al., 2011a,2011b, 2012)) incorporates principles underpinning the model as well as providing an approach to implementation and evaluation of dementia care. The CMDC theoretical framework values and integrates the capabilities approach, person-centred, relationship-centred and strengths-based care (Moyle et al., 2013). The aim of the CMDC is similar to person-centred care in that it aims for optimal care and the development of opportunities to improve quality of life of people with dementia living in LTC facilities. The CMDC aims to do this through a focus on the strengths and capabilities of persons with dementia using structured care cycle that incorporates multi-sourced care assessment, planning opportunities, facilitating care needs and care review and evaluation. Furthermore, the CMDC uses a set of values, which guide care and also aim to develop a culture of value within the organisation so that the person with dementia is given the opportunity to do the things they deem as being important in their life.
This paper also reports on an evaluation of the content of the intervention and the processes of delivering the intervention through surveys and reflective field notes. The education protocol was designed for adult learners and grounded in the following assumptions set out in Knowles’(1980) theory: a need to know; a responsibility for own learning; the role of experience in learning; a readiness or applicability of the information to a real life situation; a motivation to learn; and problem-centred learning with real life problems.
Study aims
The study aimed to evaluate, using two methods, an educational intervention implementing the CMDC. Firstly, through analysis of survey responses to face-to-face workshops and secondly through analysis of reflective notes to explore the perceptions of the on-site facilitators regarding how the educational intervention enabled staff to meet the objectives of the education, that is:
To work collaboratively in care teams which include the person with dementia and their family member; To contribute to and be guided by a new model of care that involved a Capabilities Care Plan; To use a strengths-based and relationship-centred approach to care; and, To practice reflective thinking and/or reflective writing.
Design
The study used an exploratory mixed method approach to evaluate the content of the intervention and the processes of delivering the intervention through surveys and reflective field notes.
Method
Forty-eight staff in the three LTC facilities received education and training that incorporated a range of teaching methods in the CMDC for 8 months. The staff involved in the education program included registered nurses (RNs) (n = 7), enrolled nurses (ENs) (n = 8), personal care workers (PCWs) (n = 30), and diversional therapists (DTs)/activity therapists (n = 3). Participation in the education and training was voluntary although the organisation encouraged all staff to attend.
Following initial face-to-face education sessions comprising of six two-hour sessions conducted over 2 months with staff, the facilities were provided with on-site mentorship to facilitate the development of staff skills and assist in the implementation of the training into clinical practice. Two registered nurses (facilitators) were employed 21.45 hours a week to provide both the face-to-face sessions over the first two months and the on-site mentorship across the three facilities for 6 months. Both these nurses had some experience in clinical education; however, neither had a background in dementia care. As such, members of the research team (WM, LV & MC) provided extensive education for these two facilitators before the education protocol was implemented and this consisted of workshops on dementia, mentorship, the CMDC, leadership and change, reflective journaling, and orientation to the facilities and staff participating. The facilitators worked with two members of the team (WM & LV) to construct the education materials and to update support materials such as education tip sheets developed in a previous project. Two of the research team (WM & LV) also met with the facilitators once a fortnight to discuss any issues with the mentoring role, help with understanding the context of the situation and to keep the facility senior staff engaged in the project. Ethical approval for the study was granted by the university human research ethics committee, and the partner aged care organisation formally endorsed the three facilities involvement in the research. All participants provided written informed consent.
Intervention
Knowles’ (1980) theory and content and process of education protocol.

Data collection
The six, 2-hour face-to-face workshop education sessions were evaluated to ensure they met the needs of the participants. This was completed via an eight-item survey, developed by the research team. The first six items were pre-determined closed response questions, employing a 5-point Likert rating scale (items one–four: 1 = ‘strongly disagree’ to 5 = ‘strongly agree’; and items five–six: 1 = ‘needs improvement/poor’ to 5 = ‘very effective/excellent’). The final two items were open response; allowing participants to comment on what they perceived were the most valuable aspects of the session and provide any suggestions for improvement. Participants were asked to complete the survey anonymously after each of the six education sessions, and return it to the facilitator.
The extensive reflective field notes, recorded over the course of the study by the two facilitators who were the on-site mentors, were qualitatively analysed. Facilitators were asked to keep a journal for reflective comments about their perceptions of how the intervention protocol met the aims of the CMDC educational program. They followed Gibbs’ (1988) framework when writing their reflections: Description; Feelings; Evaluation; Analysis; Conclusion; and Action Plan.
Data analysis
Survey evaluation data from the six education workshops, undertaken at each of the three facilities, were entered into PASW Statistics Version 20.0 (SPSS Inc., Chicago, IL, USA) for analysis. Twenty per cent of the data was randomly checked against source to confirm input accuracy. For all categorical items (one–six), basic frequencies were established and the two open response items (seven–eight) were thematically coded. A mean score was computed to provide an overall workshop evaluation score, with two, one-way analyses of variances (ANOVAs), with Bonferroni pairwise comparisons, then undertaken to test for differences in mean scores by workshop session number (one–six). A pairwise deletion strategy was employed because there were minimal points of missing data (Tsikriktsis, 2005). All statistical tests were considered significant at the level p < 0.05.
A critical appraisal of the content of the field notes was undertaken. The process was informed by Norwood’s (2010) approach to thematic analysis. The pattern of categories and the relationships between categories were identified and systematically considered using an inductive analysis process to allow themes to emerge from the data (Norwood, 2010). Themes were refined as the analysis process progressed through in-depth research team discussions until distinct themes emerged. The names of the themes were chosen based on their clarity to represent the overall sense of the reflective notes (Norwood, 2010). Four themes emerged from this inductive content analysis.
Results
Evaluation of workshops
Workshop attendee responses to categorical items (one–six) on the evaluation survey (n and %).
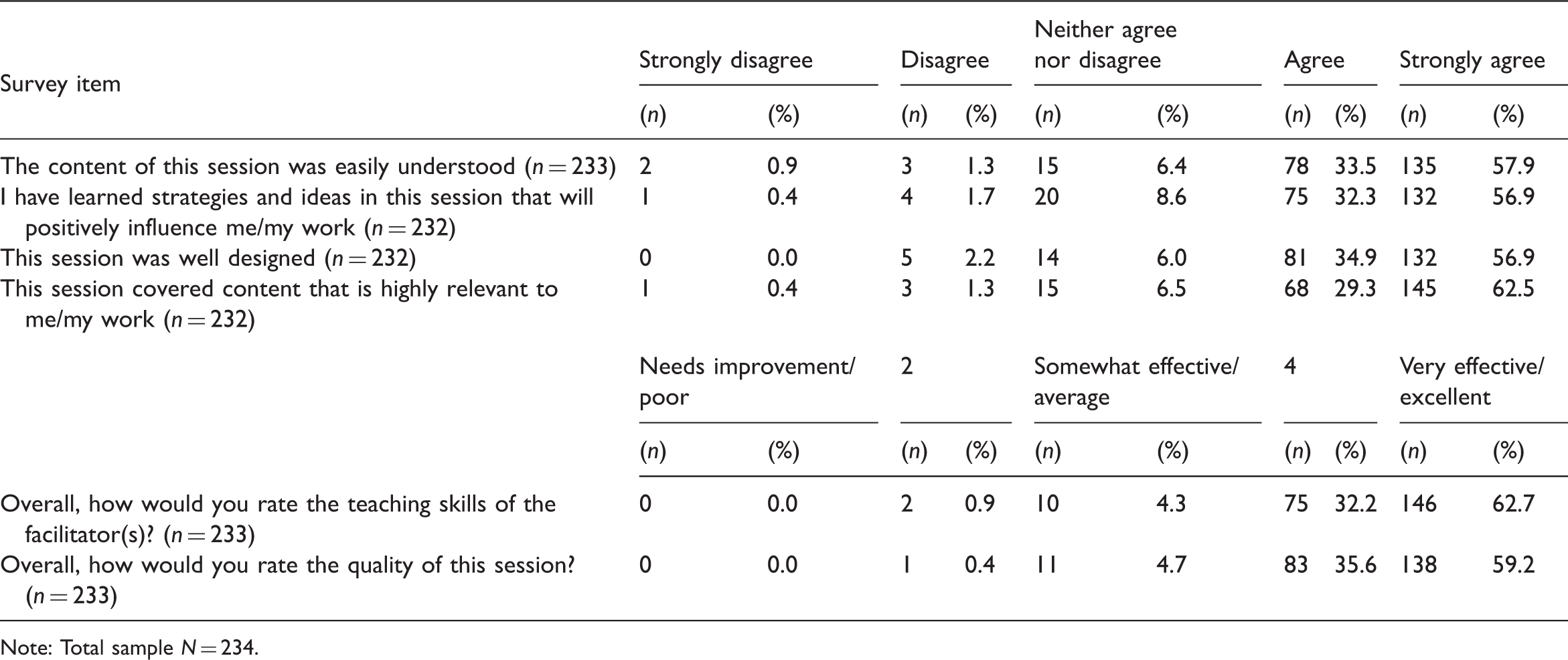
Note: Total sample N = 234.
When exploring whether workshop attendees’ overall mean evaluation scores differed according to facility and workshop education session number, no statistically significant differences were apparent (F(2, 230) = 2.476, p = 0.086 and F(5, 227) = 1.289, p = 0.269).
A third (33.8%, n = 79) of workshop attendees provided detail on which aspects of the sessions were most valuable to them, with the largest proportion stating that everything/all was of value (35.4%, n = 28). When particular aspects of the sessions were highlighted, comments chiefly focused on the structure of the workshop sessions, specifically the perceived value of the interactive, scenario-based, open-discussion format, which enabled attendees to work with colleagues, share ideas, reflect and hear different perspectives (22.8%, n = 18). Other aspects considered of value, but more disparately noted by three or more attendees, focused on: how to maintain and achieve a sense of feeling valued (7.6%, n = 6); how changes in the approach to care of people with dementia can be made to enhance their sense of value (i.e. taking the time to sit and talk) (3.8%, n = 3); symptoms of dementia (3.8%, n = 3); more/new knowledge (3.8%, n = 3); and morals and ethics (3.8%, n = 3).
When asked how the education sessions could be improved for the future, just over a fifth of attendees provided comment (21.8%, n = 51). Whilst the largest proportion of these stated that no improvements were required (52.9%, n = 27), there were three main suggestions, noted by three or more attendees. These were: more handouts/prints of the presentation slides (11.8%, n = 6); more simplified explanations to aid greater understanding (5.9%, n = 3); and more time to process the information during sessions (5.9%, n = 3).
Facilitator reflective field notes
To explore the perceptions of the two facilitators regarding how the intervention enabled staff to achieve the aims of the CMDC education program a thematic analysis of their written reflective notes was undertaken. Four themes emerged from this analysis and included: on-hand application and guidance, teaching and mentoring methods, visible progress, and organisational support.
On-hand application and guidance. The understanding of and approach to care within the CMDC model were reinforced well through the application of concepts and principles at the coalface with the facilitators on-site. Facilitators identified that they were able to address concerns and issues quickly to reduce any negative concerns: ‘I would sit down with her and help her with where and how to write it and I saw the strain visibly lift from her’ (facilitator A). This on-hand support and guidance also provided staff with instant feedback that promoted their understanding of the CMDC model and its importance to improving care through its strength-based approach. Facilitator B wrote: ‘Worked with [a staff member] after her having been to 4 hour workshop. She has great ideas but is hesitant to try for herself so we sat together and wrote the care plan to her ideas’ and an on-site meeting with staff led the facilitator to conclude that this enabled them ‘… starting to think of ways to utilise [resident’s] strengths to help her to be occupied’.
Teaching and mentoring methods. The reflective notes identified that a varied approach to the teaching of the CMDC was particularly valued by the participants in helping them understand the model. The content of and methods used in the initial workshops enabled ‘plenty of interaction … with the activities’ (facilitator A), the group to ask ‘lots of questions and … think about strengths that may be available … [and] reflect on residents and how they changed when given opportunities’ (facilitator B). This was confirmed by the survey results. The facilitators identified that using a combination of group and individual teaching moments was effective. Group meetings provided opportunities ‘which work well in helping the staff to gain information about the residents and build relationships with each other’ (facilitator A) that fostered ‘collaboration … [and] a willingness to share that can be built on’ (facilitator B). On the other hand, one-to-one sessions whether ‘on the floor’ or in the training room, provided focused teaching moments specific to the individual participants need: ‘7 staff members came [to training room] for a good period of time and all wrote in a care plan and were happy to have a chance to talk one-on-one about the CMDC’ (facilitator A). The tip sheets that often incorporated an appropriate scenario were developed for each of the values in the CMDC and proved to be a valuable teaching tool with facilitator A’s notes identifying the sheets as ‘helping people to focus … [and] clarify the capability for them’, and read with ‘great enthusiasm’.
Many of the staff participants were PCWs (assistants in nursing) with little formal education and little confidence in their abilities to write both in care plans and reflective notes. The facilitators agreed that strategies to build confidence did prove to be positive overtime as this excerpt illustrates: She feels her ideas will not be good enough or right. In an effort to encourage her to gain confidence to branch out on her own, I encouraged her to make some notes in her journal for this week and I would check them before she transcribed them to care plan. She suggested I look at her care plan as maybe something she had in there already might be appropriate – it sure is! … The positive feedback I was able to give her about her writing must have given a boost to her confidence and it really brought joy to my day (facilitator A).
Challenges with organisational systems. Both facilitators identified various challenges impacting on the progress and maintenance of the education throughout the 6 months on-site program. Despite staff positive evaluation of the teaching program and the outcomes of the application of the Model, lack of time, resources and at times organisational support impacted on their perceptions of the success of the education protocol. The three sites proved to be quite different with facilitators indicating both environmental and management factors as challenging. The design of the oldest of the facilities incorporated separate blocks of accommodation that was seen to ‘influence workload with the blocks being separated and if they need assistance from a co-worker it is much further to walk and the … distance and steep incline’ (facilitator B) also limited the ability to gather groups of residents together for activities. All participants reported to the facilitators that lack of time and some staff hindered their abilities to often apply the principles and concepts of the Model, and in one particular facility it was perceived that ‘no support from the top’ (facilitator A) left participants discouraged, resistant and negative.
Limitations
A limitation of this study was that the evaluation is based on the perceptions of the facilitators who provided the workshops and on-site mentoring through their reflective notes (although survey results from the 6 workshops are based on participant responses). However, as the reflections were based on Gibbs’ (1988) framework, the notes provided detailed observations and examples to support conclusions drawn by the facilitators.
Discussion
Overall, the results indicate that the education protocol based on Knowles’ (1980) assumptions around adult learning met the identified aims. Time pressure, environmental challenges and some staff and supervisors’ attitudes impacted upon the extent to which staff could actively engage in the education and its application to practice. The education process and methods stimulated thought and reflective practice regarding the importance of individualised strengths based care and facilitators identified that staff particularly found the on-site mentoring for 6 months provided on-hand guidance, support and feedback that was helpful in applying their knowledge about the Model to practice. Russell (2005, p. 203) argues reflective practice ‘can and should be taught—explicitly, directly, thoughtfully and patiently’. As such, the importance of the abilities of the facilitators as mentors to facilitate learning and reflection was crucial to the success of the education protocol in that many of the staff members involved had not formally been involved in reflecting on their practice. Spouse (2001) has argued that the promotion of the integration of theory and practice through mentorship is dependent on the learning environment and resources. It is clear that the facilitators were able to create a safe and conducive learning environment using teaching and mentoring strategies that guided staff to understand, apply, practice and reflect on the concepts inherent in the Model and this was particularly important given the challenges around time, and staff attitudes.
In line with Spouse’s (2001) argument, it was found that the activities organised to meet identified learning needs within the face-to-face weekly sessions and the on-site mentorship assisted in the application of theoretical aspect of the Model to practice. Although the facilitators found it challenging to encourage the PCWs (majority of participants) to document in the resident’s assessment and care plan and write their reflections, positive reinforcement and providing safe practice strategies (notes to discuss, writing together) proved successful. Changes in staff perspectives of care through their learning and witnessing the difference applying the Model made to care are heartening and provide opportunity for continued developments in the application of the capabilities-based care in the future.
In addition, the results of the present study highlight a number of issues, in relation to supportive management and organisational practices. The importance of managerial support is highlighted by Aylward et al. (2003) who argued from their review of the literature that any sustained practice change through education can only occur when there is organisational support. Although this support was planned to be achieved in this current study through management ‘buy-in’ in the development and implementation phases of the education intervention, and staff ‘buyout’ to attend education sessions supported by study funds, high staff turnover and management practice changes meant that maintenance of this support ‘on the ground’ in the long-term was extremely challenging. Edwards et al. (2003) also found that despite a variety of strategies to gain organisational support, commitment ‘on the ground’ to education programs was variable and suggested that this was linked to high care needs of residents and inadequate staffing levels.
Conclusion
By focusing on ‘on-site’ staff education and continuous guidance, support and feedback through mentorship, the developed protocol maximised the potential of staff to sustain quality dementia care over time, despite challenges regarding time, workloads, environment and attitudes. Continued long-term practice change through an educational process, however, needs to be sustained through the commitment of substantial resources (both human and fiscal) and long-term organisational and management support. It is argued, however, that long-term benefits of an application of an on-site mentorship education protocol to improve staff knowledge and practice has enormous potential to improve care for people with dementia living in long-term care. As such, future research specifically focussing on organisational level approaches to changing models of care practice in aged care that include economic evaluation are needed.
Footnotes
Funding and Acknowledgements
The research team would like to acknowledge Wicking Trust for grant funds, and support and assistance from RSL Care (QLD), staff, and Susan Griffiths as project manager.