
Abstract
The Department of Health has increased the emphasis on earlier detection of dementia among patients aged over 75 admitted to hospital in an emergency in England. Introduction of a Commissioning for Quality and Innovation (CQUIN) payment provides an incentive for NHS Trusts to screen patients for memory problems on admission. This article reports on how improvements were made to the screening process across three wards in a large university teaching hospital.
Introduction
The Department of Health has estimated that only 42% of those living in England with likely dementia have a formal diagnosis and has expressed its commitment to achieving better and more timely diagnosis rates (Department of Health, 2013). Earlier diagnosis is likely to lead to earlier treatment, with some medications associated with greater cost effectiveness than supportive care alone (Nagy et al., 2011), particularly in reducing length of hospital stay, and delaying the requirement for a full-time package of care for some patients(Rive et al., 2010). However, primary care practitioners often feel unable to manage or diagnose dementia, with limited awareness of the National Dementia Strategy (Department of Health, 2009, 2010), with significant numbers of dementia-related admissions to acute hospitals referred via general practitioners (National Audit Office, 2010). Evidence of benefit to justify population screening primary care is lacking (Iliffe et al., 2009). There are criticisms of the proposed dementia screening tool, namely as the screening test is being implemented with a lack of evidence and the UK National Screening Committee suggests the evidence for introducing the screening tool fails to meet acceptable criteria for justifying its use (Fox, Lafortune, Boustani, & Brayne, 2013).
The Department of Health England introduced a target via the Commissioning for Quality and Innovation (CQUIN) framework in 2012 by offering incentives for the identification of patients with dementia and cognitive impairment. This subsequently facilitates referral and follow up following discharge for memory problems (NHS Commissioning Board, 2013).
Funding is allocated based on three indicators:
case finding of patients within 72 h for patients aged over 75 who are admitted in an emergency and ensuring they are assessed and referred appropriately, ensuring sufficient clinical leadership and training of staff and ensuring caregivers of dementia feel adequately supported.
This audit cycle aimed to ensure that eligible patients were screened for dementia within 72 h, assessment, investigation and appropriate referral. Initial results were presented with proposed strategies to improve compliance and then the audit cycle completed to measure the change in compliance.
Method
Case notes of all current inpatients in three care of the older person wards were reviewed on the same day. The clerking proforma was examined to determine completion of the dementia screening tool based on the CQUIN measures. Data recorded on initial assessment were:
Abbreviated Mental Test (AMT) score (Hodkinson, 1972), periodicity of onset of memory problems, documentation of investigations and examination and referral to specialist services/informing the general practitioner.
The clarity of documentation was recorded with the assessor and date of assessment. The initial findings were presented to a departmental meeting, with initial results disseminated to medical staff of all grades responsible for completing the screening tool, recommendations to improve compliance and emphasis on the importance and value of completing the Dementia CQUIN. A second round of data collection occurred 3 months following presentation to determine compliance with the CQUIN and measure the change following initial interventions. Case notes were excluded if patients were aged under 75. Data were analysed in Microsoft Excel.
Results
Initial audit
The case notes of 67 patients were reviewed on the initial audit. Eleven (16%) made no reference to complaints of increasing forgetfulness, 21 (33%) reported that the patient felt they were increasingly forgetful. Thirty-five (52%) patients had not been assessed. Twenty-one (33%) patients had an existing diagnosis of dementia. Two (3%) were unconscious at the time of assessment. Nineteen (28%) patients had a recorded AMT score, ranging from 0 to 10, of which four (6%) had an AMT score greater than 8. Three (4%) patients were considered delirious at assessment. Just two (3%) had the chronicity of the onset of their memory problems documented, with both having occurred gradually over 6 and 9 months. Two (3%) patients had a complete review of medications and clinical examination. One patient (1%) underwent investigations for memory loss at the time of clerking (including haematinics and CT scan), and the same patient was referred to their general practitioner. Thirty-six of the case notes (54%) were signed and dated. The assessments were graded in accordance with having fulfilled the CQUIN requirements. A total of 8 (12%) were deemed to have met the CQUIN requirements, 33 (49%) were partially complete and 26 (39%) had no aspects of the screening completed. Six patients (9%) were considered to have evidence of possible early onset dementia that had not been identified.
Presentation of findings at departmental meeting
At the departmental meeting, a set of recommendations for improvement in compliance with completing the dementia screening tool based on the results from the initial audit included:
highlighting to medical staff the importance for patients of completing the screening tool and its role in patient care, changing the position of the screening proforma within the trust medical clerking booklet to both prompt the attending clinician and ease completion rather than as an ‘add-on’ at the end where it was easily missed, a recommendation for increasing checks by ward staff (either via a dementia ‘champion’ or ward manager) that the proforma has been completed, recommending that a ‘briefing lecture slot’ is included during trust and department induction for all doctors as they rotate between clinical posts during their training and highlighting to the hospital trust board and service lead the completion rate and effects this could have on meeting the CQUIN target.
Reassessment of performance
Three months after the departmental meeting, the case notes of 70 inpatients on the same three wards were reviewed. Forty-four (63%) referred to patients having become more forgetful over the preceding 12 months, with 18 (26%) not noticing memory impairment. Figure 1 shows the number of patients complaining of memory problems. Thirty-one (44%) had an existing diagnosis of dementia. No patients were unconscious at time of admission on re-assessment. Thirty-two (46%) had an AMT calculated at time of admission, ranging from 0 to 10 with 4 (6%) considered to be delirious at time of admission. Ten patients (14%) had the chronicity and onset of their memory problems documented. Among these, 4 (the same 4 considered delirious) had an acute onset of memory problem. For the remainder, the range of onset of memory problems was between 3 months to 1 year.
Perceived change in memory over the preceding 12 months.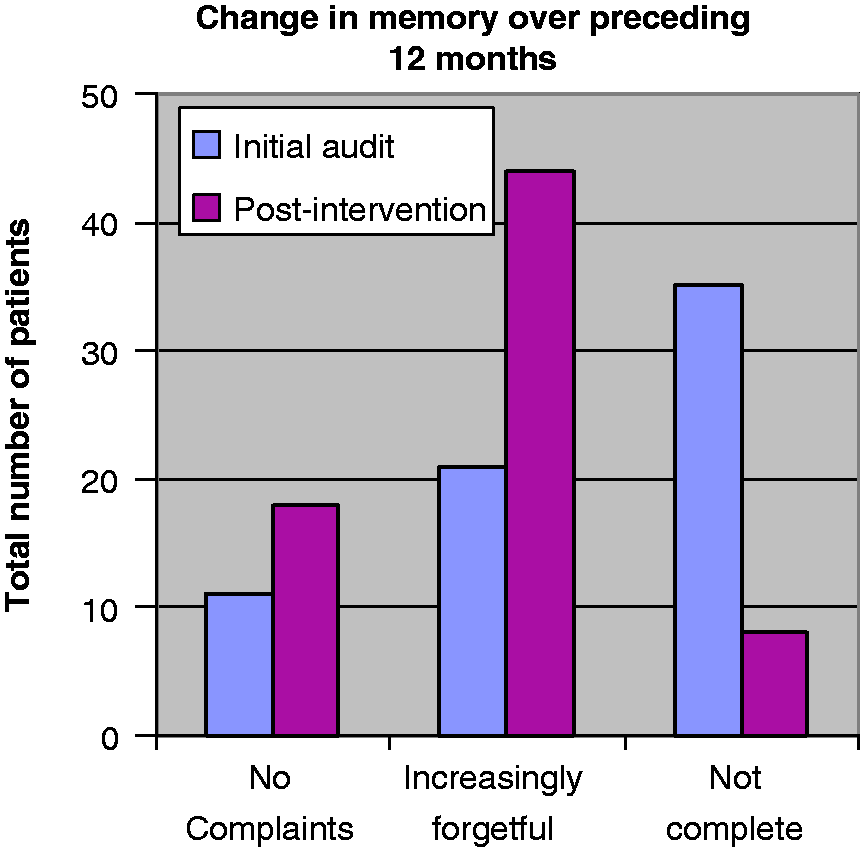
Eleven of the 44 (25%) patients who answered ‘yes’ to worsening memory problems over the preceding 12 months underwent full examination, review of medications, investigations for dementia and their GP was informed of the outcome. Fifty-three (76%) of screening assessments were signed and dated by the completing clinician. A total of 23 (33%) were deemed to have fulfilled the CQUIN requirements, 31 (44%) were partially complete and 16 (23%) were uncompleted. This represented an overall increase of 21% in appropriate completion of the dementia screening tool and a reduction of 16% in non-completions. Fourteen patients (20%) were considered to have evidence of possible early onset dementia that had not been identified, compared with 9% in the first audit, suggesting that better form filling has resulted in an improved identification rate. Figure 2 shows the change in proformas that fulfilled the CQUIN requirements.
CQUIN completion.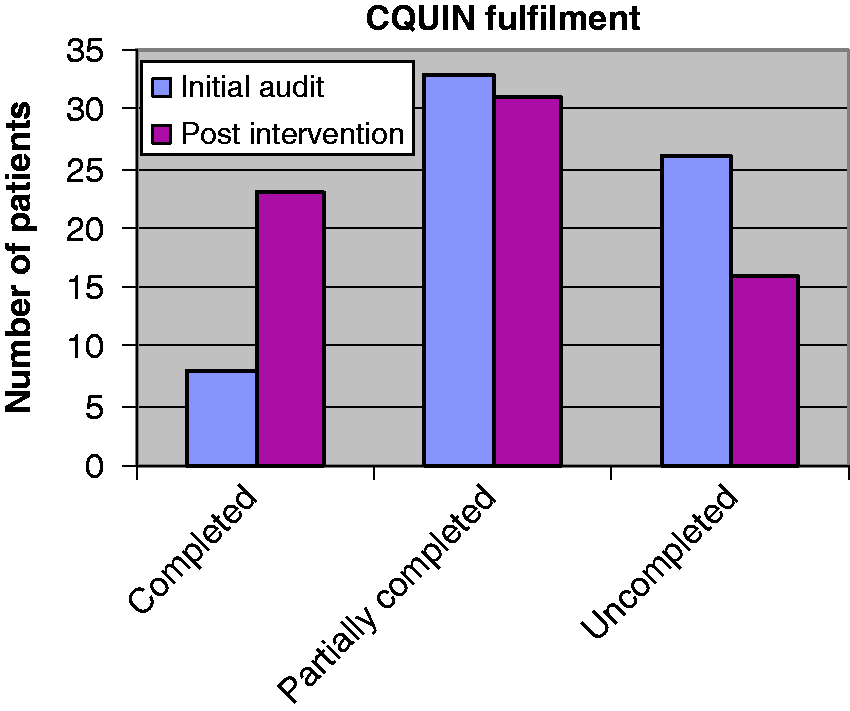
Discussion
The results of the initial audit showed an initially poor completion rate. While a third of patients had a previous diagnosis of dementia, the high proportion of uncompleted proforma suggests this could be an underestimate. A high proportion of older people in acute hospital settings have dementia, with one study suggesting that it may be as high as 42.4% (Sampson, Blanchard, Jones, Tookman, & King, 2009), with associated higher rates of mortality approaching nearly a quarter of admissions with those afflicted with dementia. Our results are comparable, with 44% of patients included in the audit having an existing diagnosis of dementia, though the proportion of incomplete proformas may mean that the actual prevalence rate was slightly higher. AMT scores were rarely calculated at admission, meaning an objective measure could not be compared with previous cognitive scores or even within the admission. Patients are at risk of cognitive decline following hospitalisation (Ehlenbach et al., 2010), with those having been an inpatient with a critical illness in the preceding few years prior to onset of symptoms having an increased risk of progressive cognitive decline (Sukantarat, Burgess, Williamson, & Brett, 2005). Calculating AMT scores should be encouraged to allow objective demonstration of cognitive trends over time. Although there was an improvement in the number of patients being investigated for dementia who indicated memory problems in the preceding year, three quarters were not investigated. While this is unacceptable, it may be that investigations were ordered at a later date, or the clerking doctor considered screening for dementia ‘a side line’ rather than part of the contributing factors leading to admission. The authors’ worry is that the CQUIN is viewed as a ‘box ticking’ exercise by clerking doctors, and that its value in helping identify dementia earlier leading to timely investigations and treatment is still underrated. Documentation was considered unacceptable, with a quarter of clerking doctors failing to sign and date the screening proforma. There is widespread consensus among the medical royal colleges that all entries in patient notes should be signed and dated legibly, so the person writing in the notes can be identified (Academy of Medical Royal Colleges, 2008; Royal College of Physicians, 2007). Inadequate documentation can have financial (Lawrence & Hinchliffe, 2012), legal (Mangalmurti, Murtagh, & Mello, 2010) and patient care (Schiff & Bates, 2010) implications. However, excessive time with paperwork and administrative tasks is associated with lower clinician satisfaction (Mechanic, 2003). While there was an improvement in records that would meet the standard for receiving the CQUIN payment, this remained below the threshold which could result in loss of the payment, and reduced funds to invest in the services.
The paper adds to the literature through clear demonstration of an improvement in compliance with the dementia CQUIN across multiple elderly care wards within the Trust and overseen by multiple medical teams. While this paper did not examine the results of screening investigations and examinations to determine how many patients identified as ‘possible early onset dementia’ actually went on to receive a formal diagnosis (true positive rate), it does highlight how in the reality of clinical practice how many patients on an elderly care ward admitted acutely who have not been diagnosed with dementia formally, may in fact be showing the early signs of memory difficulties. Further work may wish to determine the sensitivity of the dementia screening tool. The authors believe this to be one of the first completions of the audit cycle published on improving CQUIN compliance. This audit demonstrated a 21% increase in case notes that would fulfil the requirements of the CQUIN. Making clinicians aware of the benefits of routinely recording information about memory problems on admission in addition to providing evidence of the use of the screening tool can identify patients with the early signs of dementia appears to have resulted in a moderate improvement.
The authors suggest that a multifaceted approach to overcoming the barriers to completion of the dementia screening tool is needed in hospitals to improve compliance. Our approach included highlighting to medical staff the potential patient care benefits of using the screening tool, repositioning the screening tool to a more favourable and convenient location on clerking documents and highlighting to the hospital trust board the completion rates and CQUIN target implications. Further suggestions include routine checks by ward staff (either a nominated dementia champion or ward manager) that the proforma is completed appropriately and including in the induction training of doctors a lecture on how to use the dementia screening tool and why it is important.