
Abstract
This study explored staff perceptions of the role of physical environment in dementia care facilities in affecting resident’s behaviors and staff care practice. We conducted focus groups with staff (n = 15) in two purposely selected care facilities in Vancouver, Canada. Focus group participants included nurses, care aides, recreation staff, administrative staff, and family. Data analysis revealed two themes: (a) a supportive physical environment contributes positively to both quality of staff care interaction and residents’ quality of life and (b) an unsupportive physical environment contributes negatively to residents’ quality of life and thereby makes the work of staff more challenging. The staff participants collectively viewed that comfort, familiarity, and an organized space were important therapeutic resources for supporting the well-being of residents. Certain behaviors of residents were influenced by poor environmental factors, including stimulation overload, safety risks, wayfinding challenge, and rushed care. This study demonstrates the complex interrelationships among the dementia care setting’s physical environment, staff experiences, and residents’ quality of life.
Introduction
The number of people living with dementia worldwide is currently estimated at 35.6 million; this number is predicted to double by 2030 and more than triple by 2050 (World Health Organization, 2013). For decades, the bio-medical care model in dementia care focused on the treatment of pathology and management of “challenging” behaviors (Leibrock, 2000; Zeisel, 2004); the growing movement of culture change in long-term care facilities has pushed for humanization of care, using person-centered care model to improve the living environment and quality of life in people with dementia. Person-centered care is a philosophy that recognizes that each person has equal right to dignity, respect, and to participate in their environment (Alzheimer Society of Canada, 2011; Brooker & Surr, 2005). With the spread of the person-centered care philosophy, the physical environment of a nursing home has been increasingly acknowledged as important in influencing quality of life for older people with dementia living in nursing homes (e.g. Cioffi, Fleming, Wilkes, Sinfield, & Miere, 2007; Jones & Van Der Eerden, 2008; Lee & Dilani, 2012; Scott, Catherine, Perry, & Sam, 2011; Zeisel et al., 2003). The term “environment” is a broad concept, which consists of physical, social, and organizational aspects. Cohen and Weisman (1991) established a conceptual framework to understand dementia care setting as a holistic environment with dimensions of the physical (e.g. building, interior space, and furnishings), social (e.g. relationships between residents-staff and family-staff), and organizational (e.g. facility policies, care philosophy, and staffing structure) contexts. According to this conceptual framework, the physical environment of a care setting affects both its social and organizational domains. This study focuses on the physical environment’s (e.g. architectural layout, furnishing, and sensory qualities) influence on staff care practices and residents’ quality of life, as perceived by the staff.
Several studies have examined the influence of environmental design interventions on people with dementia. Particular environmental design features, such as color contrast, high-intensity lighting, size of the dining room, and noise affect health and behavior of residents (e.g. Chaudhury, Hung, & Badger, 2013; Fetveit, Skjerve, & Bjorvatn, 2003; Hung & Chaudhury, 2011; Jones & Van Der Eerden, 2008; Overman-Dube et al., 2008; Sloane et al., 2007). A recent study suggested that physical environment could alleviate anxiety and promote interest among older adults with dementia by regulating stimulation from their surroundings (Lee & Morelli, 2010). Residents in care units with spaces that provide more opportunities for privacy and personalization were associated with a decrease in anxiety and aggression (Zeisel et al., 2003). Studies also supported the benefits of using wayfinding cues and outside space in care home for people with dementia and their families (Berentsen, Grefsrød, & Eek, 2008; Chalfont, 2008; Innes, Kelly, & Dincarslan, 2011; McGilton, Rivera & Dawson, 2003; Olsson, Lampic, Skovdahl, & Engström, 2013). Another study showed that staff–resident interaction and work efficiency were improved by making nurses station smaller and moving it into one of the hallways (Schwarz, Chaudhury, & Tofle, 2004).
Although there is considerable growth in the research literature on the impact of the physical environment on residents’ quality of life outcomes, there is limited research on the perceptions and experiences of staff about the physical environmental effects on residents’ behavior and staff care practices. Based on their everyday intimate interactions with residents, the nursing and personal care staff are likely to have in-depth knowledge of residents’ behaviors and mood and the associated or contributing social and physical environmental factors. As Kramer and Schmalenberg (2008) state, the perspective of staff at the front-line as to what constitutes a positive environment is essential if interventions are intended to improve practice settings. Essentially, respecting staff’s beliefs, values, needs, and worth as individuals is key in person-centered care, which in turn, would promote respect and humanity in their interactions with residents (Kitwood, 1997). Surprisingly, empirical studies in exploring staff perception of the characteristics and functionality of a physical setting affecting about the residents’ well-being and their care interactions are scarce. The purpose of this study was to address this gap in the literature and examine staff perceptions on the affect of physical environmental features on residents’ behaviors and their care practices in two care facilities in Vancouver, Canada. This work contributes to the current knowledge base about the role of physical environment in nursing homes on residents’ quality of life and quality of care by providing an in-depth understanding of the staff perspective.
Method
This study was part of a broader investigation on how people with dementia are impacted by the environmental design of dementia care units. The larger study was based on a mixed-method research design involving multiple environmental assessments and comparisons, qualitative fieldwork, and focus group interviews, conducted in 2012–2013. This paper presents the findings from the focus groups as that method was a distinct component in the overall research design. We used focus group method (Krueger, 1998; Krueger & Casey, 2000) to elicit staff’s shared perceptions on the impact of the physical environment on residents’ behaviors and on their own care practice. Discussions in the groups generated rich and inter-subjective accounts via dynamic and interactive exchange among participants, which would not be possible in individual interviews. Participants were explained that the researchers were particularly interested in three aspects of the physical environment: architecture or spatial layout of the setting (e.g. corridor length and bath room size), interior design aspects (e.g. lighting, flooring, and furnishing), and sensory aspects (e.g. noise, smell, and tactile properties). We asked broad questions such as “How does the physical environment affect the behavior and well-being of residents?” “How does the physical environment have an effect on your care practice and interactions with residents?” Other questions focused on staff job satisfaction and recommendations for environmental improvement.
Settings and residents
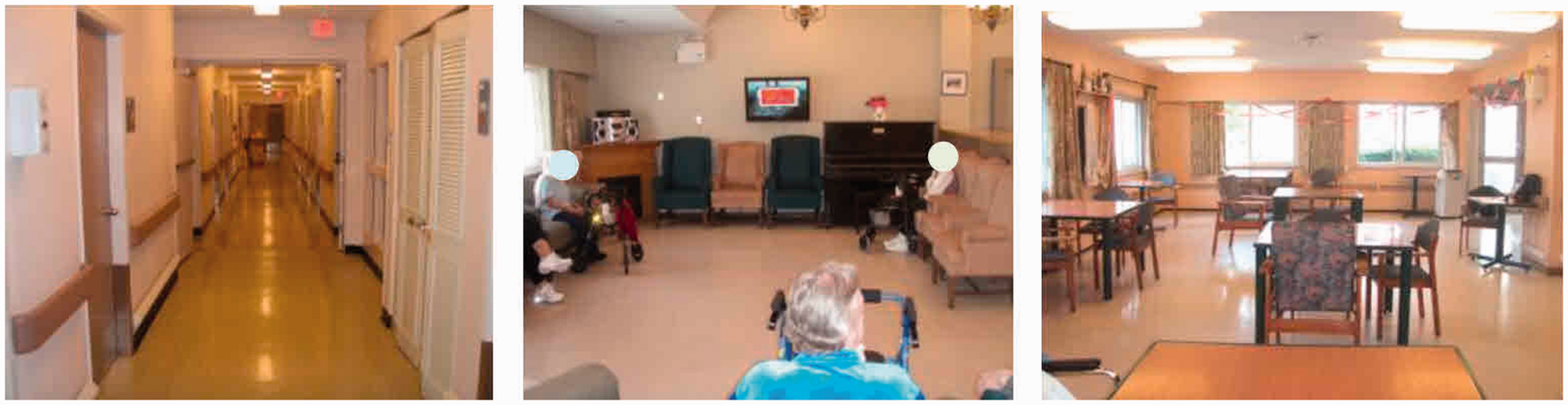
Two dementia care facilities were selected as study sites based on purposive sampling in order to obtain rich data from a breadth of perspectives. The primary selection criterion was to have contrasting physical environmental features between the two care facilities, i.e. one was selected for its traditionally designed large institutional physical setting and the other was selected for its purpose-built physical environmental character. Both facilities were located in Vancouver, British Columbia, Canada. Edgewood Home was a purpose-built dementia care facility, with multiple small units (12 residents on each unit), with relatively short corridors (about 14 m) and all single bedrooms (see Figure 1). Marine Manor was a traditional care setting, with 30 residents on each unit, long corridors (about 41 m), and mixed single/semiprivate bedrooms (see Figure 2).
Corridor, living room, and dining room in Edgewood Home Corridor, living room, and dining room in Marine Manor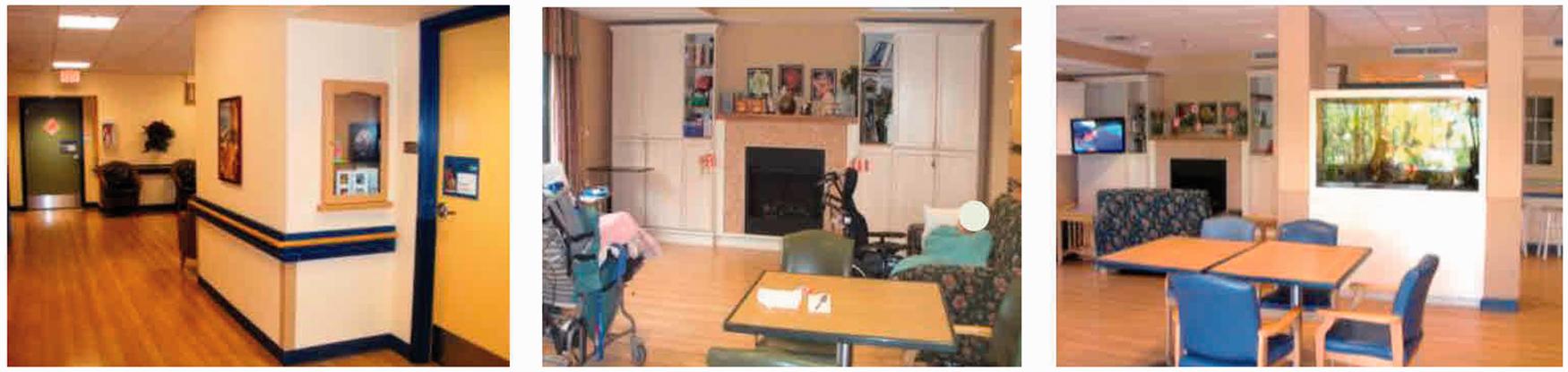
The two units were segregated from other wings of the facility, and doors that connected to the main building were unlocked by using a keypad. The number of staff working in the daytime was 1.5 nurses and 2 care aides in Edgewood Home and 1 nurse and 4 care aides in Marine Manor. Ethical approval for the study was obtained from Simon Fraser University’s Office of Research Ethics. Permission from the care homes was granted by administration at each site. Written consent was obtained from all participants’ family members or legal guardians. All names in the study documents were changed to pseudonyms to provide anonymity and confidentiality.
Focus group participants
To obtain information-rich cases among the research participants, the Director of Care at each care home was requested to recommend participants among the staff who worked closely with the residents. At Edgewood Home, six staff members participated in the focus group discussion: one administrator, one nurse, one recreation assistant, and three care aides. Nine members participated at Marine Manor: one administrator, two nurses, five care aides, and one family member. All participants were women. Participants in Edgewood Home had been working at the facility from 12 to 30 years with an average of 23.3 years and in Marine Manor from 2 to 34 years with an average of 14.4 years. The result of t-test indicated that there was no significant difference in length of working period for the staff between the two care homes.
Data collection
The focus group interviews were conducted to gather qualitative data with open-ended questions. The sessions took place in a conference room at each care facility. An interview guide was developed to explore staff’s perception on how the facility’s physical environment may affect residents’ behavior and well-being as well as staff work and job satisfaction. The interview guide questions were given to the participating staff members a week before the focus group interviews to provide them an opportunity to reflect on the questions in advance. One researcher (LH) moderated the interviews and another researcher (SY) took notes about non-verbal reactions, group dynamics, and asked follow-up questions. Throughout the focus group interviews, photographs highlighting the physical environment of the facility were shown in a slide loop to prompt responses from the group. Each focus group session lasted approximately 1 h, was audio-recorded, and fully transcribed by a professional transcriptionist. The authors verified transcriptions against the original audio recording for accuracy.
Data analysis
The analysis was driven by a broad question—how does the facility’s physical environment affect residents’ behavior and well-being as well as staff’s everyday work and job satisfaction? Each researcher began with reading the whole interview transcriptions independently several times to gain an initial understanding of the content. Afterward, the research team members searched for patterns of meanings—data related to similar concepts within and across cases to explore commonalities and differences, which were then sorted into clusters of themes and sub-themes. The authors repeatedly discussed the themes and challenged each other until consensus was reached; emerging interpretations and themes were rechecked back and forth with the original text. This iterative and systematic process in data analysis was purposefully carried out to establish credibility of the study findings.
Results
Schematic overview of themes and subthemes
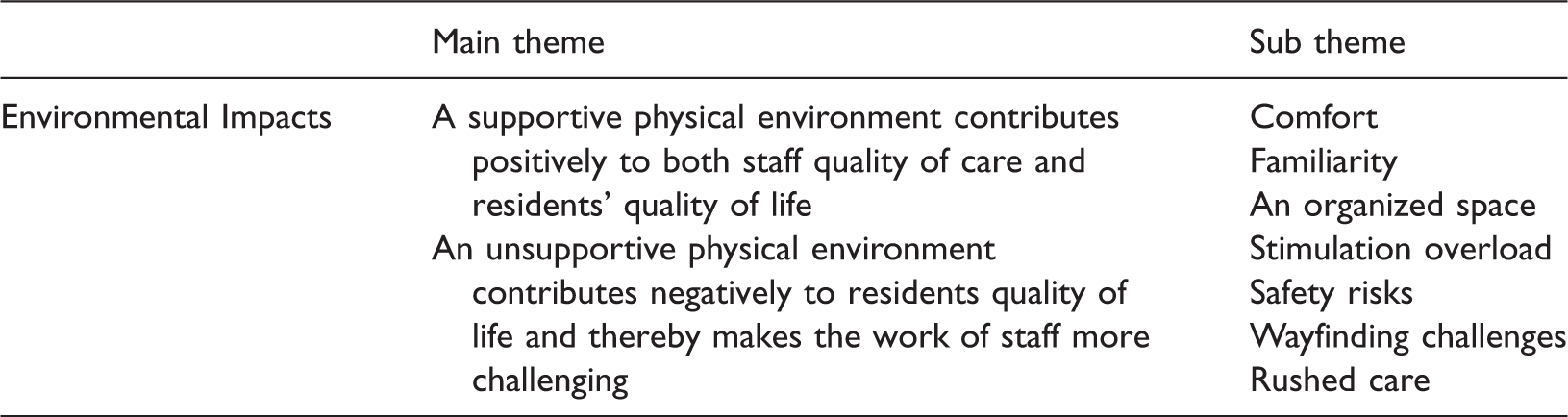
Theme 1: A supportive physical environment contributes positively to both quality of staff care and residents’ quality of life
Staff members frequently emphasized the utmost importance of creating a calm and homelike environment for residents with dementia. They expressed that a comforting environment not only kept residents happy, but it also made easier for staff to connect with and care for the residents, which led staff to be more effective in their work and have higher job satisfaction. A participant summarized it well: What I find about my working environment is the home-like feel and I can reach my residents quickly. I don’t need to walk miles to get to them. Also what I find is I don’t know who enjoys the place more, I do or the residents, just because of the comfort, the big windows, the bright lights. It’s such a nice environment to work. When I feel good, I can be more beneficial to give care to the residents (Ursula, Edgewood)
Comfort
The staff considered offering appropriate activities to comfort residents as extremely important. Both groups stressed music as a particularly positive stimulation for residents with dementia. One staff, Polly, commented on how music therapists were able to make a difference in transforming residents’ mood.
Their voices are very soft; they come with their guitar and sit down. A lot of times, I noticed that even if residents were really cranky. The therapist would sing, then residents started to settle; then they (residents) just sit there and watch and listen. The therapist had such a calming voice!
Both groups also pointed to the need to keep the outdoor environment safe and accessible. For example, Joanne at Marine Manor stated:
I would like to have a nice outdoor walking space, level. Like all the walkway being accessible for wheelchair and people with mobility devices like walkers and stuff would be nice, plants that obviously are not poisonous so residents can break it, chew it if they want to. Maybe some raised garden beds so they can dig in them as well if they wanted to have a little pot and things like that.
It’s really nice that there’re different colors because residents see a different color, they’d turn and come back, and then there’s different stuff on the walls so they are constantly seeing something. And they’d stop sometimes and look at some of the memory boxes (Polly, Edgewood).
Familiarity
According to the staff, the residents needed familiarity in their environment. It was noted that residents were in better mood and more receptive to care when there were personal items in the environment or when the environment was arranged in a personalized way. Diane expressed, “Allowing them (residents) to have personal items in their room is a way for you (staff) to associate and talk with them and see their pictures.” Another participant shared a similar view, “The resident is calmer knowing familiar stuff around. It’s their room and they are not feeling threatened. You’re in their house and I think it really does help with the care.” (Joanne, Edgewood).
New technology was not always deemed as helpful. The group at Edgewood shared their experience of using automatic faucets in the special care unit. The administrator Diane at Edgewood said, “With the automatic faucets we thought that by putting those in that we would have less leaks but it turned out that it ended up being a problem.” A nursing staff further explained: I have one resident when he wants to wash his hands after going to the washroom he’s like trying to find where it is and he gets really ticked and just starts swearing sometimes. It really seemed like a really good idea to start with. Now it’s total frustration. It takes a lot of time to do our care because we use a face cloth, wet it and then we have to hang it over top of the facet until the water is running warm enough. (Polly, Edgewood).
An organized space
Having resources and equipment close by was regarded as important in making work easier for staff in both groups and participants described it as “an organized space.” In Edgewood, a recreation staff member expressed her gratitude of the environmental design on her unit: “I appreciate having all my things, resources right at my fingertips, so close by, the way the cupboards were designed…. I always have what I need to do my programs.” However, when “things are not together,” a participant shared her bitterness about the problem of not having a toilet near the bathtub: I think I like the other unit better because they have a toilet beside the bathtub. It’s very good this way because if the person, the resident wants to go to the toilet, it would be easy. Now, for us, we need to take the person out the bathing room and to the washroom. It’s very frustrating. So it would be very nice if everything were together. (Nelli, Marine Manor)
Participants used strong emotional descriptors such as “over-stimulating,” “agitated,” “rushed,” “too many people,” “too loud,” and “aggravated” to depict how negative environment aspects may contribute to residents’ behavior; they also articulated how the environment could lead a reciprocal effect on residents and staff. A staff explained: When you are not fighting against things like, I’ve got to protect this person from this and that’s going to be annoying to my residents, when you are not constantly having to work around things, it just makes your job easier. It makes what you are able to do much more effective. When you are able to do better work, you feel better, right? (Kelly, Edgewood)
Stimulation overload
The staff at Marine Manor voiced a number of stimulation issues regarding the physical environment of their facility, including noise, overcrowding, and high traffic of people coming and leaving the units. I find that the spaces of our units are quite confined and there’re a lot of people in one area like we have 29 or 30 residents on our units, in the special care unit. That has a big impact on how people behave because they just basically get on each other’s nerves sometimes. (Colleen, Marine Manor) If there is no air and if we’re hot and we feel like we are in a stuffy environment, it makes us feel tired and, you know, you just sometimes if it’s really bad, you can be less patient and, so it does affect how we feel, and how we feel directly impacts the residents as much as you try to not allow it to. It does. So I mean if we have a nice open area environment it’s going to make us feel better and that will be passed on to the residents. The environment has an impact on how we respond to people. (Colleen, Marine Manor)
Safety risks
Staff members in Marine Manor discussed the facility’s traditional long hallway layout, and large-scale environment made it difficult for staff to supervise and protect residents from safety risks. Mary gave an example, “Trying to keep them (residents) away from the exit where people are always coming and going is quite a challenge especially after lunch.” Celine further explained, “I’m scared that if residents would follow visitors to leave… and the resident there who is standing in the door could get hurt… it’s so difficult for us to call them all the time.” Another staff, Colleen, mentioned Like in the evenings, for example, if we are putting people to bed it can also be like a safety issue because if there is whole bunch of people still in the lounge and the staff are putting somebody to bed that’s at the end of the hallway, for example, the people down here are left unattended. And, you know, it has happened. People have fallen or there’s been an altercation between residents and there hasn’t been anybody there right at that moment. So the layout is such that, you know, it’s difficult to monitor everybody. (Colleen, Marine Manor) I think that because it is a small unit, I personally feel safe. I can holler and someone is going to hear you because it is small enough that even if you are in the lunchroom or in the nurses’ station, you can hear pretty well. The same with residents, if somebody happened to fall or something nine out of ten times you are going to hear them yell out. (Polly, Edgewood)
Wayfinding challenges
Difficult in wayfinding due to the large scale of unit was reported as another important stressor for residents with dementia. Julie at Marine Manor stated, “Because there are so many rooms that escalate the frustration because they are going around asking—This is my room? Not my room? It’s frustrating and our rooms are mostly unlocked, so the residents wander into each others’ rooms which again cause conflicts.” Staff also felt that the layout of the unit could cause frustration in residents: “I mean with our hallways being very long, you know, the residents will always end up at a dead end. It becomes kind of frustrating for them. They cannot find the exit. Because they have nowhere to go and they try the doors and everything’s locked of course.” (Mary, Marine Manor)
Rushed care
A few staff members at Marine Manor were deeply concerned about the care experiences of their residents. One staff gave an example of mealtimes that were quite problematic, rushed, and not meeting special needs of residents with dementia who needed to move in a slower pace. A few other participants echoed the same concern. One made a comment: I wouldn’t want to sit down to a meal in our dining area myself because it just would not be a pleasurable experience for me, it’s very quick, very rushed. And it should be a pleasurable experience because it’s a very important part of life, of our life, you know. So I can imagine for the residents. We start at seven in the morning, check our residents, get the report. Then we run back to residents’ rooms and do their care, wash them, dress them, comb their hair, head to the bathroom, take each resident to go to the dining room and go back to get other residents in the rooms. So we have to rush, residents have to be in the dining room by 8:30. We have 29 residents (Jan, Marine Manor)
Discussion
Findings from this analysis lend support to Kitwood (1997)’s theory of person-centered care, which asserts that when the personhood of individual staff is supported, “staff will take their own sense of well-being into their day-to-day work” (p. 103). The staff members at Edgewood Home were happy about how the small units and homelike environment supported their abilities to meet residents’ needs. Being able to stay close with residents, having familiar positive stimulations (e.g. music, memory boxes, and personal items) empowered staff to connect with residents. This is consistent to the work of Cioffi et al. (2007), which found small dementia care unit improved the work for staff. In contrast, a sense of feeling drained and exhaustion was clearly evident within staff at Marine Manor; they were tired of dealing with the heat, poor ventilation, unsafe exits, resident conflicts, confusing large layout, and high level of legwork. Participating staff in both groups strongly believed how outdoor areas were useful for comforting residents. Bengtsson and Carlsson (2006) had similar findings in their research that found outdoor gardens provided residents with restorative experiences and temporary escape from negative situations.
The findings of this study shed new light into the significance of the physical environmental characteristics role on the interrelationship between residents’ behaviors and staff care practice. The study also gives voice to a group of nursing home staff, a marginalized workforce in long-term care to express their opinions regarding the environment in which they worked. Findings suggest that design of the physical environment in a care home setting is significant in influencing staff’s quality of work, as well as their job satisfaction, which are related to residents’ care experiences. When staff felt supported by the environment, they were happier and more effective in caring for residents. Since dementia care involves empathic skills and relational work, our findings raise an important question on how emotion, well-being, and quality of work life of staff may affect them using empathy in care provision. Staff in Edgewood took pride of their work that meet the challenging needs of the residents with dementia. A sense of reward and meaningful accomplishment may sensitize and reinforce staff to provide and/or maintain quality care. However, when the physical environment restricts staff to meet residents’ cognitive, behavioral, and emotional needs, staff members have the potential of increased work-related stress and reduced job satisfaction. Therefore, a deeper understanding of staff perspective is necessary in creating an environment that works for staff and effective in meeting the needs of residents in care facilities.
The results in the focus groups were consistent with the findings in our larger study (manuscript under review) that showed the smaller scale environment was more effective in creating a homelike feel and promoting social engagement in residents. Future studies need to ask specific questions to explore how the built environment may affect teamwork, which can have important consequences on the quality of care and social interaction, and in turn, in residents’ experiences.
While previous studies focused on the association between physical environment and resident outcomes, to our knowledge, this is the first study that makes the connection among the physical environment, staff-care practice, and resident’s well-being, as perceived by the staff in dementia care settings. The findings of this study have potential to contribute to informing improvement of the physical environment in care facilities.
Finally, it is important to acknowledge the limitations of the present study. This was a small-scale study, and our results may not reflect the care experiences of residents and perspectives of staff in other settings. Also, a few staff members might have hesitated to fully share their opinions in the presence of their supervisor (Director of Care) in the focus group. Although a heterogeneous group can bring together people with job roles at different levels of an organizational hierarchy to share diverse perspectives, power imbalance can potentially be a challenge for candid sharing of views. To address this issue, during the focus group sessions, our second moderator paid careful attention to the participants’ nonverbal behaviors and explicitly encouraged the relatively quieter participants to share their views. The only one family participant did not say much in the Marine Manor focus group. Because families have unique and invaluable perspective to contribute, future studies need to identify effective ways to recruit families in research. Family is likely to be more comfortable to express their opinions in separate family focus group.
Conclusion
Findings of this study suggest that a well-designed physical environment can lead to higher morale, closer relationship between staff and residents and work-effectiveness in staff, potentially resulting in better care in enhanced well-being of residents. Specifically, it has shown that a small-scale homelike setting gives dementia care homes more resources to improve quality of life for residents and more supportive work environment for staff. Prior research offers insights as to the impact of physical environment on residents. This study adds to the current body of literature by providing evidence that demonstrates the interactive relationship among the physical environment, staff work practice, and residents’ quality of life outcomes in dementia care settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Acknowledgement
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (NRF-2011-0009776).