
Abstract
Introduction
Previous research has shown that people with dementia and caregivers derive wellbeing-related benefits from viewing art in a group, and that facilitated museum object handling is effective in increasing subjective wellbeing for people with a range of health conditions. The present study quantitatively compared the impact of two museum-based activities and a social activity on the subjective wellbeing of people with dementia and their caregivers.
Methods
A quasi-experimental crossover design was used. People with early to middle stage dementia and caregivers (N = 66) participated in museum object handling, a refreshment break, and art viewing in small groups. Visual analog scales were used to rate subjective wellbeing pre and post each activity.
Results
Mixed-design analysis of variances indicated wellbeing significantly increased during the session, irrespective of the order in which the activities were presented. Wellbeing significantly increased from object handling and art viewing for those with dementia and caregivers across pooled orders, but did not in the social activity of a refreshment break. An end-of-intervention questionnaire indicated that experiences of the session were positive.
Conclusion
Results provide a rationale for considering museum activities as part of a broader psychosocial, relational approach to dementia care and support the use of easy to administer visual analog scales as a quantitative outcome measure. Further partnership working is also supported between museums and healthcare professionals in the development of nonclinical, community-based programs for this population.
Introduction
There is growing evidence for the efficacy of nonpharmacological interventions in dementia care aimed at improving functioning, quality of life, and increasing wellbeing (Kaufmann and Engel, 2014). Recent research has shown that older adults who are cognitively impaired are significantly less likely to be socially and cognitively active than older adults without a cognitive impairment (Johnson, Whitlatch, & Menne, 2014), and that engaging in meaningful activity in the early stages of dementia can help people to focus on their residual abilities and offset a sense of loss (Genoe & Dupuis, 2014). This also includes the arts, which have increasingly been shown to have cognitive, emotional, and wellbeing benefits for people with dementia (Young, Camic, & Tischler, 2015; Zeilig, Killick, & Fox, 2014). Argyle and Bolton (2005) have argued that it is possible to be ill and still be in a state of wellbeing, and other authors have highlighted the crucial impact the social context can have on the wellbeing in dementia. For example, Kitwood (1997) rejected a solely biomedical deficit-based model of dementia so that the person does not become defined by their illness but retains a sense of “personhood.” Despite diminished cognitive function, relational needs such as social contact remain intact, as well as creativity and self-expression (Kitwood & Benson, 1992). A definitive consensus on defining wellbeing has yet to emerge, although it is agreed to be a complex and multidimensional construct (Dodge, Daly, Huyton, & Sanders, 2012). Some have argued in favor of emphasizing the subjective nature of wellbeing, elevating the capacity of the person themselves to assess their own state of health and happiness (Keyes, Shmotkin, & Ryff, 2002). Hedonic wellbeing has been conceptualized as one’s own pleasure and happiness and may be seen as a relatively straightforward way in which to quantify subjective wellbeing using self-report measures (Swindells et al., 2013). The present study drew on a definition of wellbeing as the subjective state of experiencing pleasure and happiness (Swindells et al., 2013).
The arts in dementia care
Empirical studies have begun to investigate the impact of the arts in dementia care through group-facilitated art viewing (e.g. Camic, Tischler, & Pearman, 2014; MacPherson, Bird, Anderson, Davis, & Blair, 2009; Rosenberg, 2009). Results have indicated positive outcomes in terms of increased subjective psychological wellbeing, a sense of broadening of horizons, and social inclusion (Flatt et al., 2014; Young et al., 2015). Other findings showed increase in sustained attention and intellectual engagement (Camic et al., 2014) and stimulation of episodic memories and communication (Eekelaar, Camic, & Springham, 2012). There is also evidence to suggest that new learning occurs in people with dementia (Clare et al., 2000; Eekelaar et al., 2012). Mell, Howard, and Miller (2003) proposed that new skills can emerge after the onset of dementia, and that artistic development can continue even when language abilities deteriorate. Graham, Stockinger, and Leder (2013) demonstrated that, for people with Alzheimer’s, esthetic judgments are similar to those of healthy adults, providing further evidence that art-based interventions may draw on residual abilities even when cognitive impairment is present. The involvement of caregivers in art-viewing studies was deemed to be an important aspect, as art viewing formed a vehicle of relational communication within the dyad giving the caregiver new insights into the person with dementia’s abilities (Greenwood, Loewenthal, & Rose, 2002; Zeilig et al., 2014) and how dementia itself is conceptualized (Zeilig, 2014). As evidence suggests that the wellbeing of many people in caregiving roles may be adversely affected, it is highly pertinent to offer psychosocial support for caregivers as well as the people they care for (Department of Health, 2008). Previous research has suggested that art gallery-based interventions can provide social and psychological support to caregivers in ways different from traditional support groups (Roberts, Camic, & Springham, 2011). Focusing on residual abilities and meaningful activities may help to offset a sense of loss for both the person with dementia and the caregiver, and can potentially help throughout the course of illness. Several authors have argued for the emphasis of the importance of “in-the-moment” subjective experience of the person with dementia, with a focus on meaningful personal experiences for participants (De Medeiros & Basting, 2014) and person-centered outcomes (Patel, Perera, Pendleton, Richman, & Majumdar, 2014). Reviewing evidence for visual arts interventions, Salisbury, Algar, and Windle (2011) concluded such interventions were shown to reduce isolation, promote communication, encourage residual creative abilities, and enable expression of a sense of identity. A further review of art therapies in dementia care strongly argued for consistent inclusion of participants’ subjective experience in research rather than the imposition of normative, outcomes-based expectations that do not adequately capture the enrichment and enjoyment derived from these activities (Beard, 2012).
A conceptual literature review of museum object handling has found this activity to be effective in achieving significant short-term increases in subjective wellbeing (Solway, Camic, Thomson, & Chatterjee, 2015). Object handling sessions comprise tactile, visual, and conversational exploration of authentic museum artifacts. Neuropsychological evidence suggests that certain types of cutaneous touch implicated in this activity may invoke a sense of wellbeing through being linked to emotional and motivational systems in the brain (e.g. the insula cortex: Critchley, 2008). It has also been argued that the stimulation of multiple sensory modalities facilitates a deeper level of encoding in working memory (Baddeley & Hitch, 1974) and thus may facilitate learning (Paddon, Thomson, Menon, Lanceley, & Chatterjee, 2014). Evidence exists suggesting that older adults may particularly benefit from the simultaneous presentation of congruent information via multiple sensory modalities (Laurienti, Burdette, Maldjian, & Wallace, 2006). Other authors have emphasized that holding museum objects can trigger memories, projections, and associations that may invoke a meaning-making process beneficial to subjective wellbeing (Dudley, 2010; Rowlands, 2008).
Arts interventions have frequently been criticized for lacking a comparison group (Clift et al., 2009) meaning that limited inferences can be drawn regarding the importance or necessity of the art component. This has led critics to suggest that benefits obtained from these interventions can be accounted for by social interactions alone (Simmons, 2006). Art viewing and object handling as group activities have not yet been compared to each other, nor have they been assessed in relation to non-art-focused social activities.
The present study
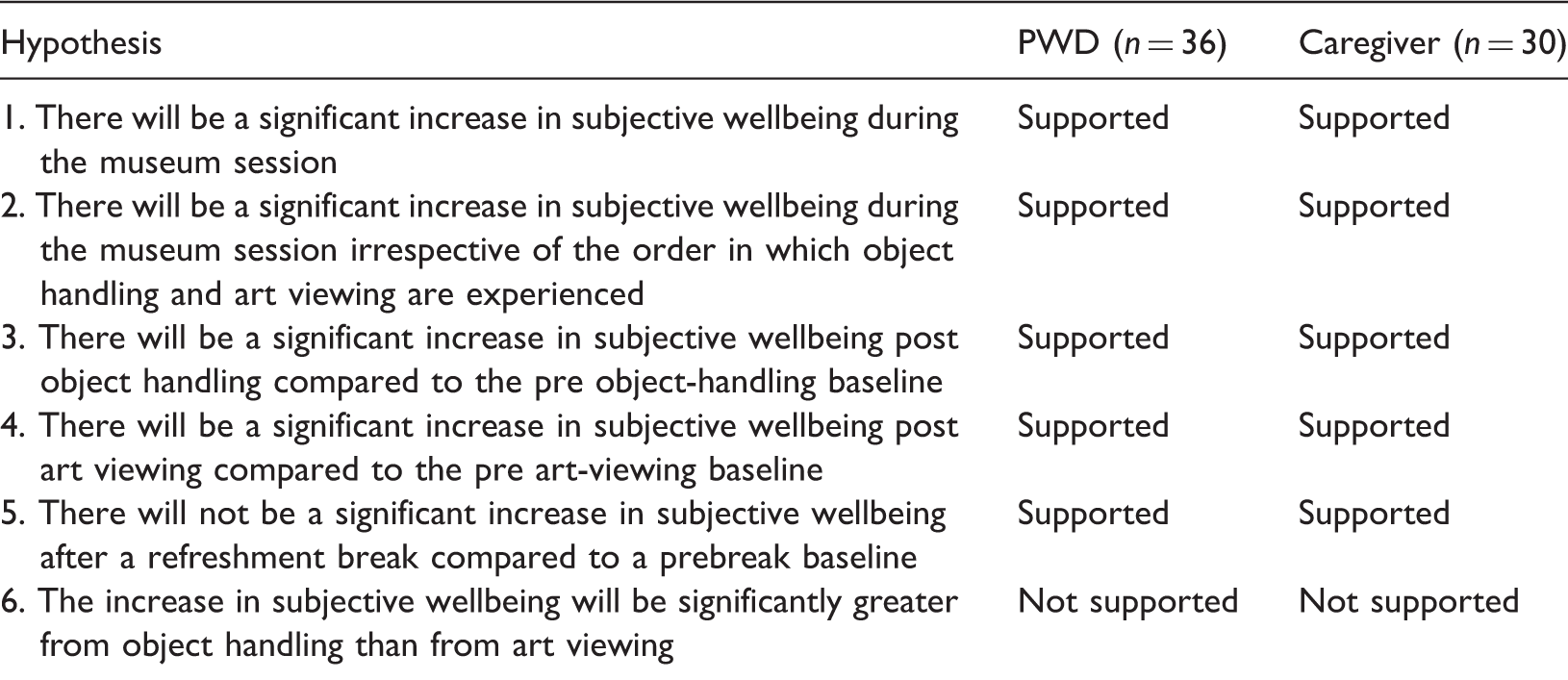
The present study investigated the impact of three museum-based activities on the subjective wellbeing of people with dementia and their caregivers. These comprised two interventions (art viewing and object handling) and a usual social activity in the form of a refreshment break. H1: There will be a significant increase in subjective wellbeing during the museum session. H2: There will be a significant increase in subjective wellbeing during the museum session irrespective of the order in which object handling and art viewing are experienced. H3: There will be a significant increase in subjective wellbeing post object handling compared to the pre object handling baseline. H4: There will be a significant increase in subjective wellbeing post art viewing compared to the pre art-viewing baseline. H5: There will not be a significant increase in subjective wellbeing after a social refreshment break compared to the prebreak baseline. H6: The increase in subjective wellbeing will be significantly greater from object handling than from art viewing.
Design and methods
Participants
Gender and age of participants.

The average length of time since diagnosis was nine months (range: 2–24 months). Inclusion criteria were a diagnosis of any type of dementia in the early to middle stages, living at home, and capacity to give informed consent. Two people with dementia had a comorbid diagnosis of Parkinson’s disease; one had a lateral visual impairment. Caregivers had to be over the age of 18 and could be a spouse, relative, or friend. People with dementia could attend without a caregiver if they wished. Recruitment took place over 13 months; 134 participants initially registered their interest in participating (64 dyads and six people with dementia who did not identify a caregiver). Nine dyads were unable to attend due to illness; 15 dyads changed their mind about participating in the study without giving a reason; 10 dyads no longer wished to participate due to other life events taking precedence. The study was approved by the UK National Research Ethics Service (reference 13/LO/1353).
Design
This quasi-experimental study had a mixed 2 × 4 repeated-measures crossover design with two separate groups: people with dementia and caregivers. The first factor (between subjects) was the order in which participants experienced the interventions, with one level as object handling first and art viewing last (summarized as order 1: MOH-AV) and the other level as art viewing first and object handling last (summarized as order 2: AV-MOH). The second factor (within-subjects factor) was the time point at which self-report measures of subjective wellbeing were administered (Figure 1). This factor had four levels: time 1 (prefirst intervention), time 2 (post first intervention and pre refreshment break), time 3 (post refreshment break and pre second intervention), and time 4 (post second intervention). Control measures implemented included using the same facilitator for all sessions and use of a repeated-measures crossover design, which counterbalanced the order to account for any order effects. Additionally, the facilitator and volunteers were not aware of the directionality of the hypotheses. An a priori power calculation using G*Power statistical software (Erdfelder, Faul, & Buchner, 1996) indicated that to detect a medium effect size (f = .25) with 80% power and alpha .05 two-tailed, the between-subjects factor required N = 82; the within-subjects factor required N = 24; the interaction required N = 24.
Time points at which self-report measures of subjective wellbeing were administered.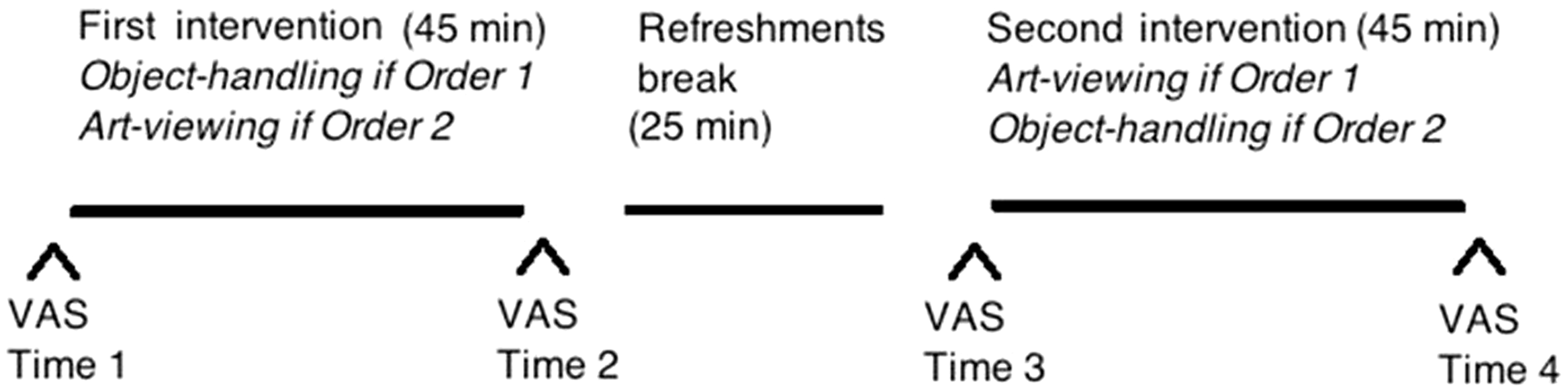
Measures
Visual analog scales (VAS)
VASs were selected to measure subjective wellbeing (EuroQol Group, 1990). VASs are suitable for assessing change across a short period of time, have validity within subjects, and are usually easily administered (Wewers & Lowe, 1990). People with dementia use VAS in a way that is conceptually similar to the general population (Arons, Krabbe, van der Wilt, Olde-Rikkert, & Adang (2012) while Thomson and Chatterjee (2014) successfully trialed VAS measuring happiness and wellness with people with mild, moderate, and severe dementia. Since many researchers agree that wellbeing is a complex, multifaceted construct, the present study used five subscales in an attempt to capture dimensions of wellbeing outcomes pertinent to this group and setting, yet also sought not to overly burden participants with lengthy and cognitively challenging measures. Participants self-reported on vertical scales of 0–100 how happy/sad, well/unwell, interested/bored, confident/not confident, and optimistic/not optimistic they were feeling at that moment in time. Their previous ratings were not made available to them at any time as an attempt to control for demand characteristics to report an improvement. Ander et al. (2011) suggested that engagement may be a key aspect of wellbeing relevant to a museum context and there is theoretical and empirical support for the benefits of engaging people with dementia in activities they find interesting (Genoe & Dupuis, 2014). Engagement was conceptualized as a continuum between interested and bored to avoid confusion from other common uses of the word. The dimension of confidence was included, since research has indicated this can decrease over time in people with dementia (Miller & Butin, 2000). The dimension of optimism sought to measure hopefulness about the future and is included in other measures of wellbeing (e.g. Stewart-Brown & Janmohamed, 2008). The interested, confident, and optimistic subscales were piloted with people with dementia and caregivers by Weiner and Camic (2014).
Evaluation questionnaire
A brief open-ended feedback questionnaire aimed to elicit responses about participants’ experiences was given at the end of the intervention.
Procedure
A museum in the southeast of England was the site for the study. Its permanent collection includes artifacts from ancient Egypt; the Anglo-Saxon period; as well as a wide range of paintings, taxidermy, and other curiosities from the 17th to 20th centuries.
The museum session
The average size of each museum group was six people (three people with dementia and their caregivers) ranging from four to eight people. The facilitator and two volunteers were present at each session. Sixteen sessions were scheduled and 11 were run in total (five were cancelled due to dropout; remaining participants were transferred to a subsequent session). Sessions were counterbalanced: six sessions began with object handling and five with art viewing with the social activity between them (Figure 1). Objects were presented one at a time and people had the opportunity to hold, examine, and talk about them as a group as they were passed round. Questions about impressions of the objects included sensory descriptions, preferences, and reflections; associations and anecdotes were encouraged. A wide range of objects were used (e.g. Victorian carbolic soap, ancient Egyptian scarab stone, Iron Age axe head, geode, 19th-century African headdress rest, fossilized shark’s tooth, 18th-century tinderbox). The social intervention consisted of general conversation with refreshments. Art viewing comprised viewing selected paintings in the gallery and the facilitator’s use of open questions to discuss color, texture, esthetic preferences, and speculation on the artist’s intent. Paintings were selected which had different content and styles, and a potential for visual discovery. At the conclusion of the museum session, participants completed the evaluation form and were given a pack containing a debriefing letter, a museum brochure, a postcard of one of the paintings, and a list of questions similar to ones asked by the facilitator to use on future museum visits if desired.
Data analysis
VAS subscale scores (happiness, wellness, interestedness, confidence, optimism) at each time point were summed to derive a composite overall wellbeing score. Overall wellbeing scores were used as the dependent variable for inferential statistics; SPSS version 22 was used for all analyses. Since VASs are deemed to be interval scales (Paul-Dauphin, Guillemin, Virion, & Briancon, 1999), data were checked for normality in order that parametric analyses could be conducted where possible. Mixed-design analysis of variance (ANOVAs) was conducted to test for main effects of time and order for people with dementia and caregivers as separate groups. The size and significance of the differences between time 1 and 2 (pre and post first intervention), time 2 and 3 (pre and post refreshment break), and time 3 and 4 (pre and post second intervention) were then tested by performing bootstrap paired-sample t-tests. Bonferroni corrections (Bland & Altman, 1995) were applied to reduce the risk of inflation of Type I error: alpha levels were adjusted accordingly (α = .05 / 3 = .017). These procedures were applied to all t-tests reported.
Results
Shapiro–Wilk’s statistics showing normality of distribution for overall wellbeing scores.
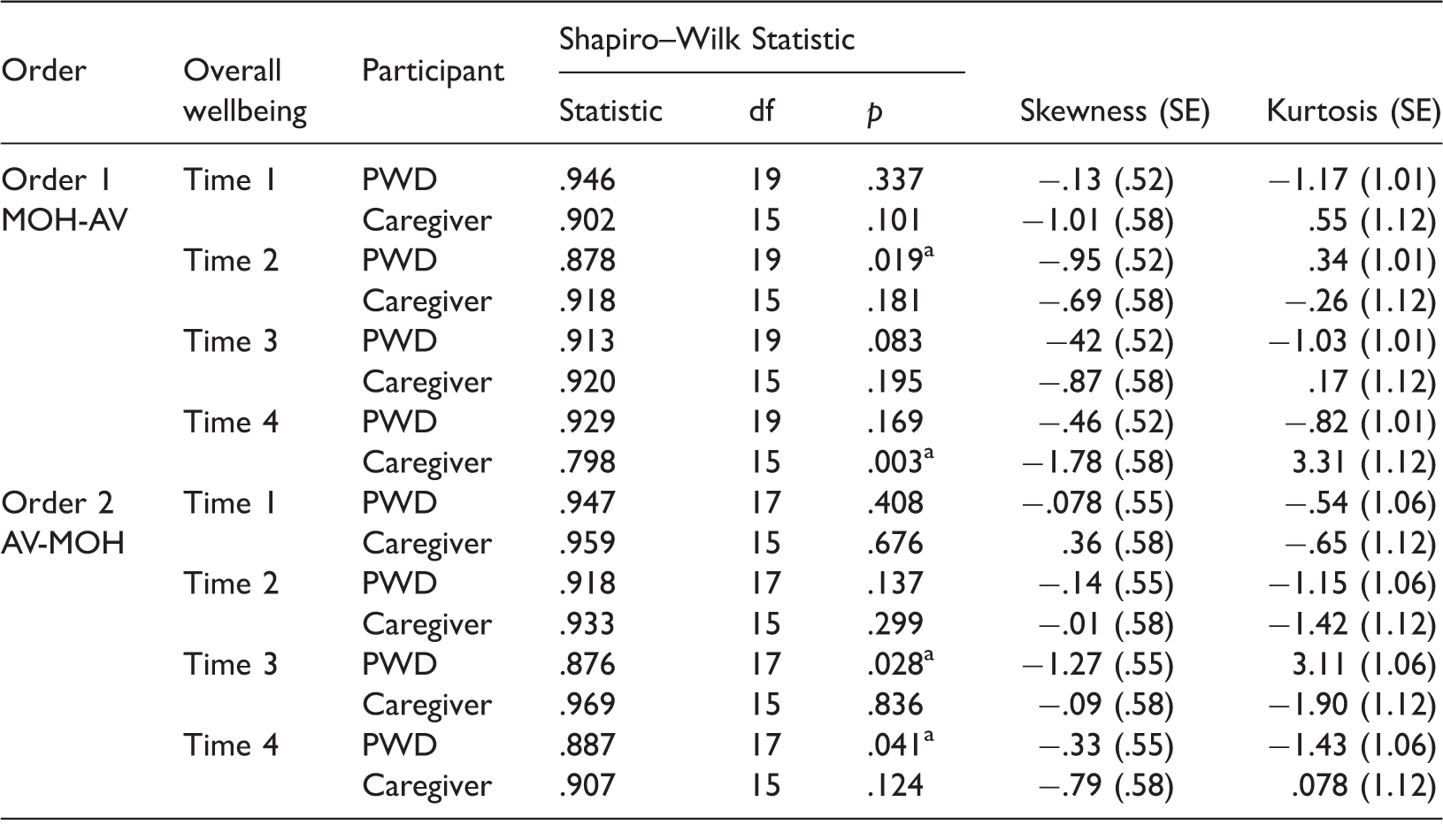
AV: art viewing; MOH: museum object handling; PWD: people with dementia; SE: standard error.
denotes data that deviated significantly from a normal distribution. Bootstrapping procedures were later used to compensate.
Mean (SD) overall wellbeing scores at time 1, 2, 3, and 4.
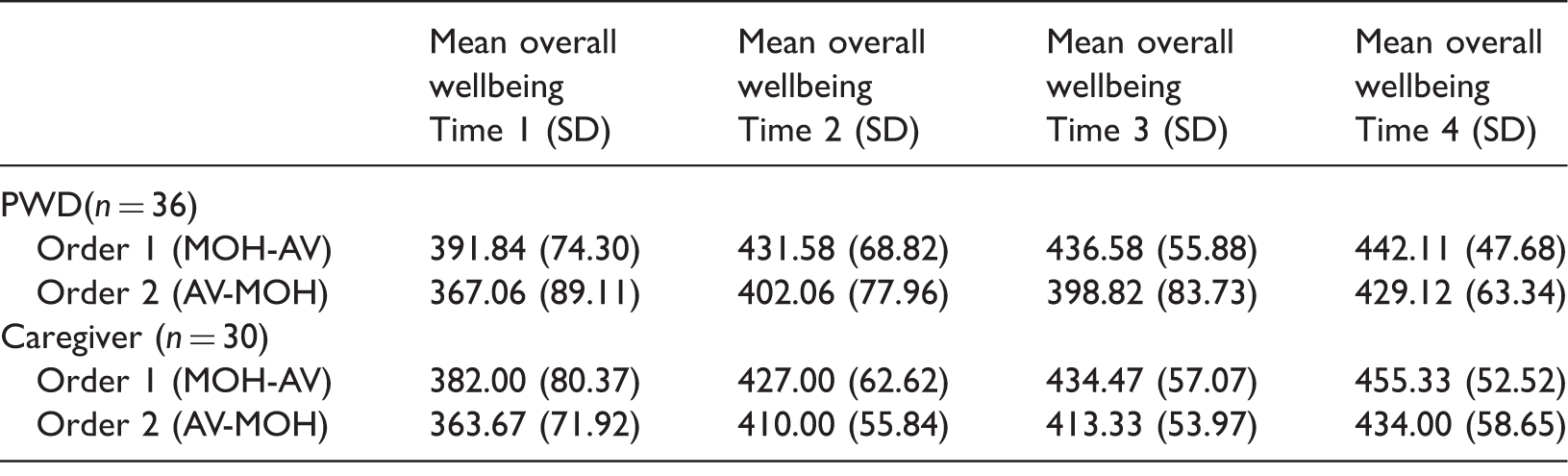
AV: art viewing; MOH: museum object handling.
Note. Maximum overall wellbeing score = 500.
Mean (SD) overall wellbeing change scores.
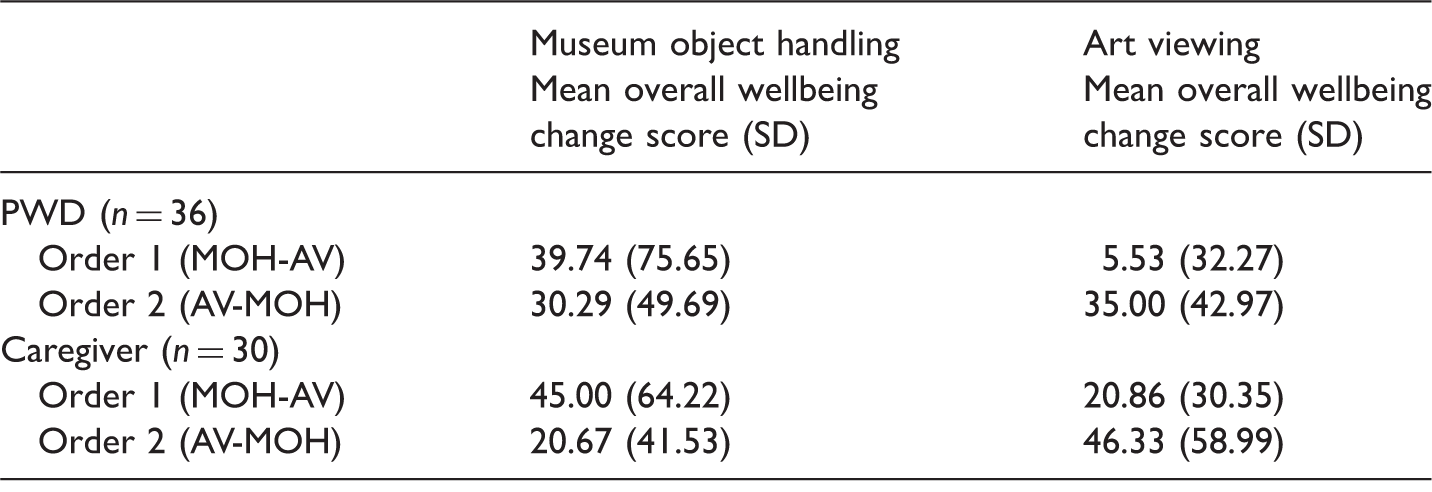
AV: art viewing; MOH: museum object handling.
People with dementia
A mixed-design ANOVA with time (time 1, 2, 3, and 4) as a within-subjects factor and order as a between-subjects factor revealed a significant main effect of time for people with dementia (F(3, 102) = 13.54, p < .001, ηp2 = .285). There was no significant main effect of order (F(1, 34) = 1.583, p = .217, ηp2 = .044). There was no significant interaction between time and order (F(3, 102) = .65, p = .585, ηp2 = .019). Therefore, Hypotheses 1 and 2 were supported for people with dementia (Figure 2).
Plot showing main effect of time on overall wellbeing for people with dementia with separate lines for order.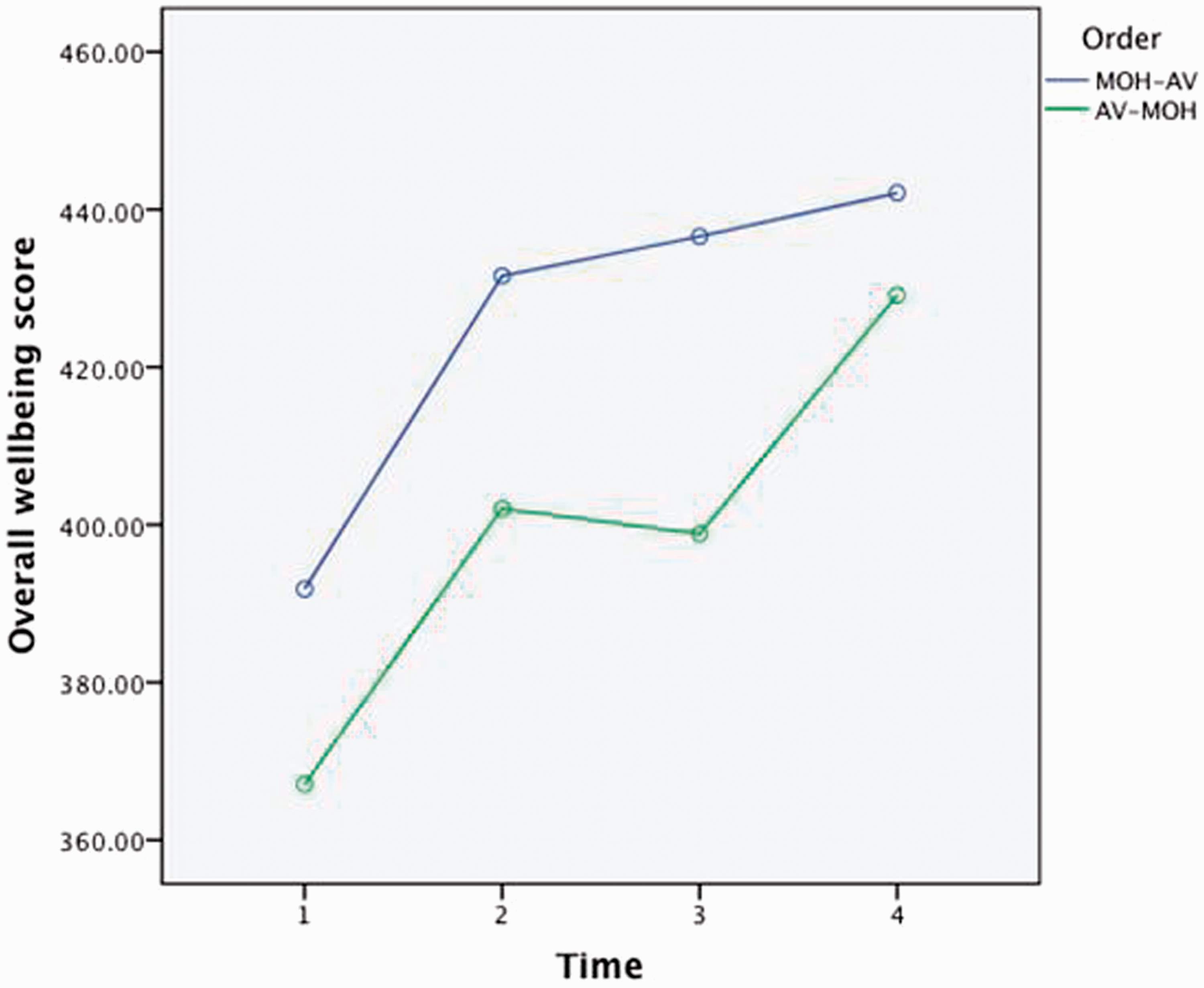
Collapsing scores across order but maintaining time measurements aligned allowed further exploration of the main effect of time. Paired sample t-tests indicated that overall wellbeing scores were significantly higher at time 2 (M = 417.64, SD = 73.74) than at time 1 (M = 380.14, SD = 81.40), t(35) = 3.65, p = .001, d = 0.61. There was no significant difference between overall wellbeing scores at time 2 (M = 417.64, SD = 73.74) and time 3 (M = 418.75, SD = 71.95), t(35) = .133, p = .895 nor were scores significantly higher at time 4 (M = 435.97, SD = 55.19) than at time 3 (M = 418.75, SD = 71.95) with the Bonferroni corrections applied: t(35) = 2.42, p = .021, d = .40. Hypothesis 5, that there will not be a significant increase in subjective wellbeing from a refreshment break, was supported for people with dementia.
Since no significant main effects of order were found for people with dementia, results for object handling and art viewing were pooled across both orders for this analysis (Cohen, 2007) to test Hypotheses 3 and 4 (Figure 3). This was achieved by averaging time 1 scores for participants in order 1 with time 3 scores for participants in order 2, and averaging time 2 scores for participants in order 1 and time 4 scores for participants in order 2 and so on. Subsequently, paired sample t-tests indicated that overall wellbeing scores were significantly higher post object handling (M = 430.42, SD = 65.35) than pre object handling (M = 395.14, SD = 77.82), t(35) = 3.308, p = .002, d = .51. Hypothesis 3, that there will be a significant increase in subjective wellbeing from object handling, was supported for people with dementia when scores were pooled across both orders. Paired sample t-tests also indicated that overall wellbeing scores were significantly higher post art viewing (M = 423.19, SD = 66.02) than pre art viewing (M = 403.75, SD = 80.47), t(35) = 2.194, p = .006, d = .26. Hypothesis 4, that there will be a significant increase in subjective wellbeing from art viewing, was supported for people with dementia when scores were pooled across both orders.
Plot showing main effect of time on overall wellbeing for people with dementia across pooled orders.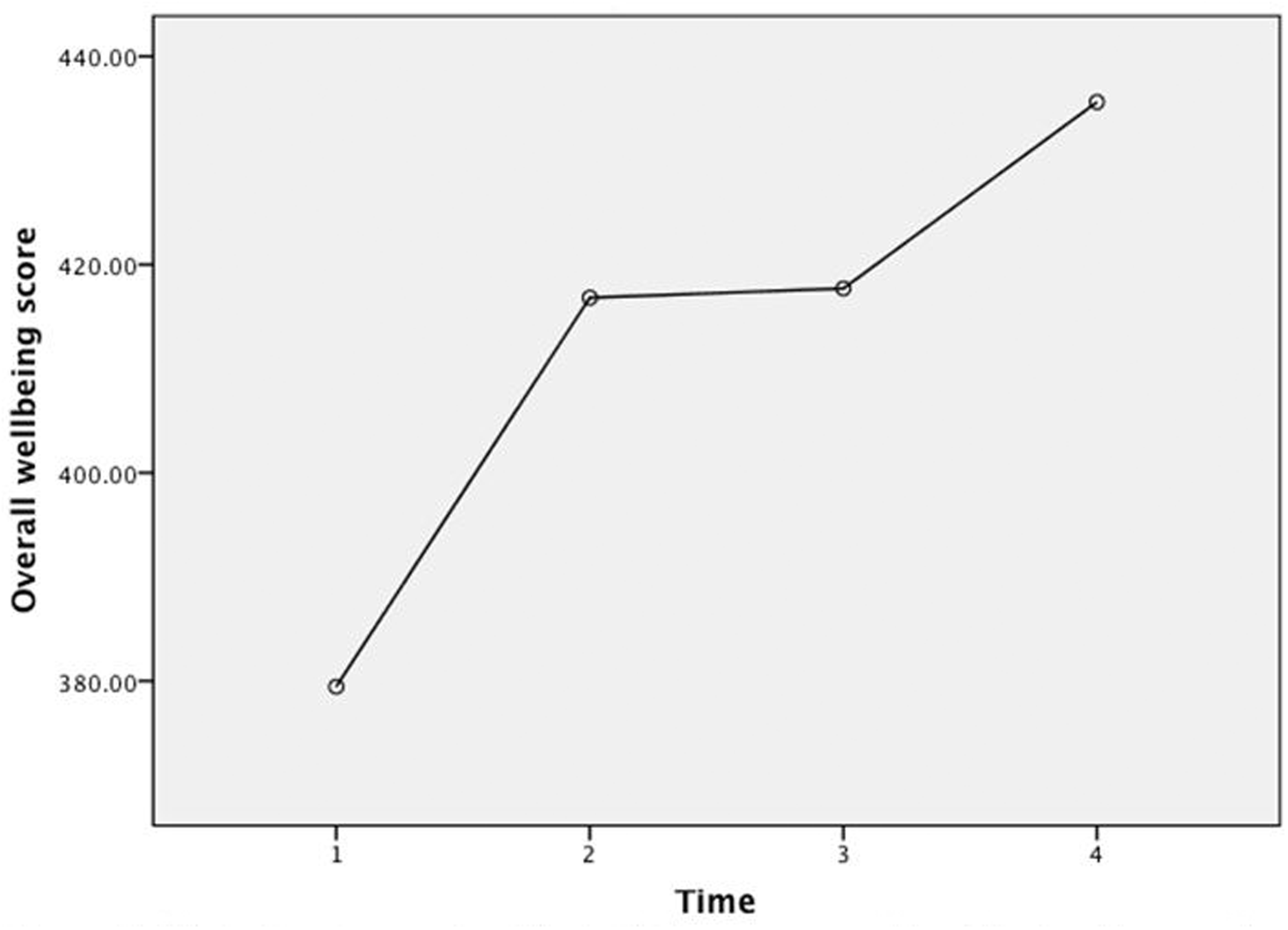
Caregivers
A mixed-design ANOVA with time (time 1, 2, 3, and 4) as a within-subjects factor and order as a between-subjects factor revealed a significant main effect of time for caregivers (F(1.95, 54.45) = 23.46, p < .001, ηp2 = .456 (Mauchly’s test indicated that the assumption of sphericity had been violated (χ2(5) = 23.70, p < .001, therefore degrees of freedom were corrected using Greenhouse–Geisser estimates of sphericity (ɛ = .65))). There was no significant main effect of order (F(1, 28) = .945, p = .339, ηp2 = .033) and no significant interaction between time and order (F(1.95, 54.45) = .029, p = .969, ηp2 = .001). Therefore, Hypotheses 1 and 2 were supported for caregivers (Figure 4).
Plot showing main effect of time on overall wellbeing for caregivers with separate lines for order.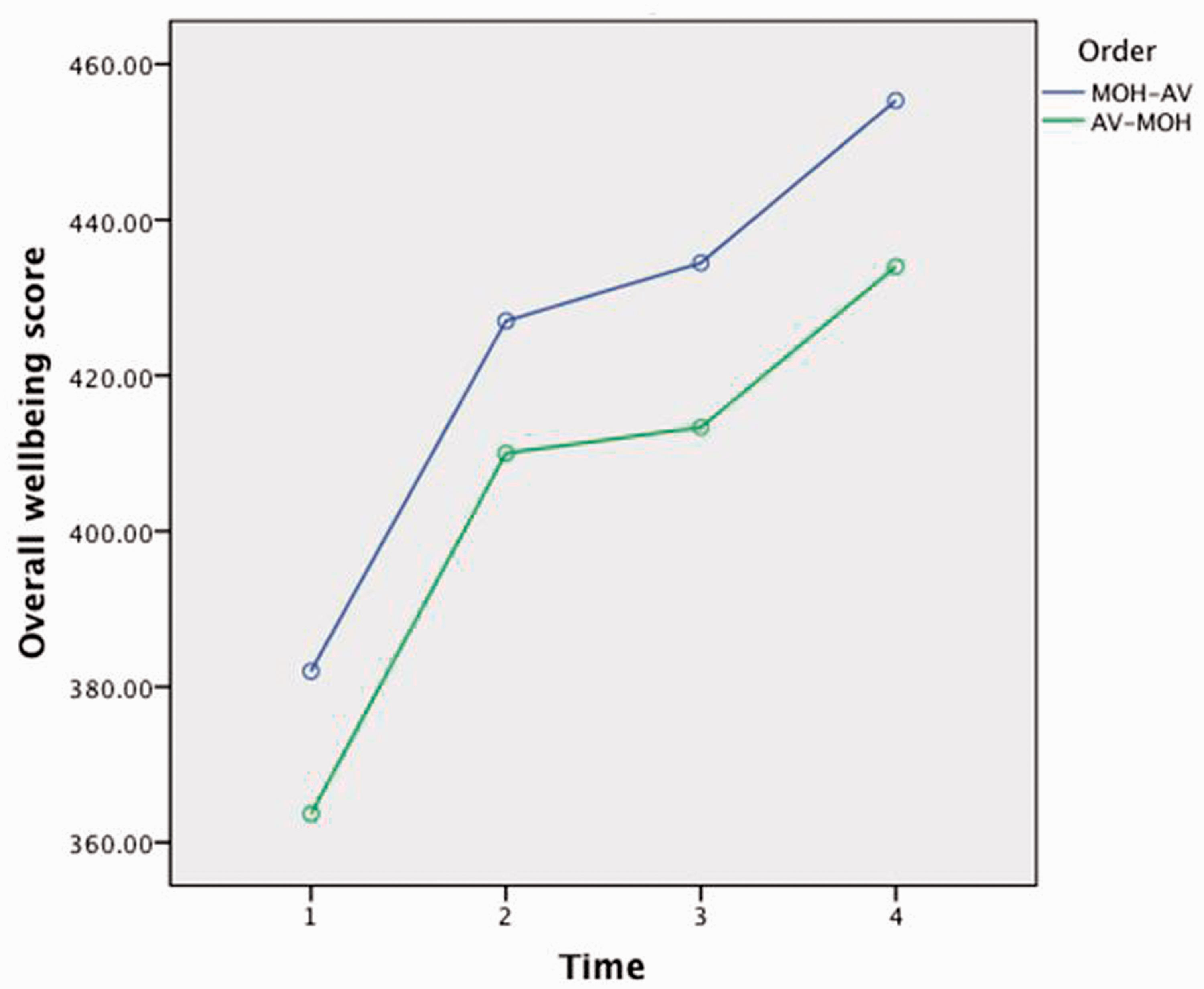
As before, collapsing scores across order but maintaining time measurements aligned allowed further exploration of the main effect of time. Paired sample t-tests indicated that overall wellbeing scores were significantly higher at time 2 (M = 418.50, SD = 58.93) than at time 1 (M = 372.83, SD = 75.51), t(29) = 4.13, p < .001, d = .75. There was no significant difference between overall wellbeing scores at time 2 (M = 418.50, SD = 58.93) and time 3 (M = 423.90, SD = 55.62), t(29) = 1.065, p = .296. Overall wellbeing scores were significantly higher at time 4 (M = 444.67, SD = 55.77) than at time 3 (M = 423.90, SD = 55.62), t(29) = 3.183, p = .003, d = .58. Hypothesis 5, that there will not be a significant increase in subjective wellbeing from a refreshment break, was supported for caregivers.
Since no significant main effects of order were found for caregivers, results for object handling and art viewing were pooled across both orders for this analysis (Cohen, 2007) to test Hypotheses 3 and 4 for caregivers as previously done for PWD (Figure 5). Paired sample t-tests indicated that overall wellbeing scores were significantly higher post object handling (M = 430.50, SD = 59.71) than pre object handling (M = 397.67, SD = 69.13), t(29) = 3.296, p = .003, d = .51. Hypothesis 3, that there will be a significant increase in subjective wellbeing from object handling, was supported for caregivers when scores were pooled across both orders (Figure 5). Paired sample t-tests also indicated that overall wellbeing scores were significantly higher post art viewing (M = 432.67, SD = 58.04) than pre art viewing (M = 399.07, SD = 73.25), t(29) = 3.844, p = .001, d = .51. Hypothesis 4, that there will be a significant increase in subjective wellbeing from art viewing, was supported for caregivers when scores were pooled across both orders.
Plot showing main effect of time on overall wellbeing for caregivers across pooled orders.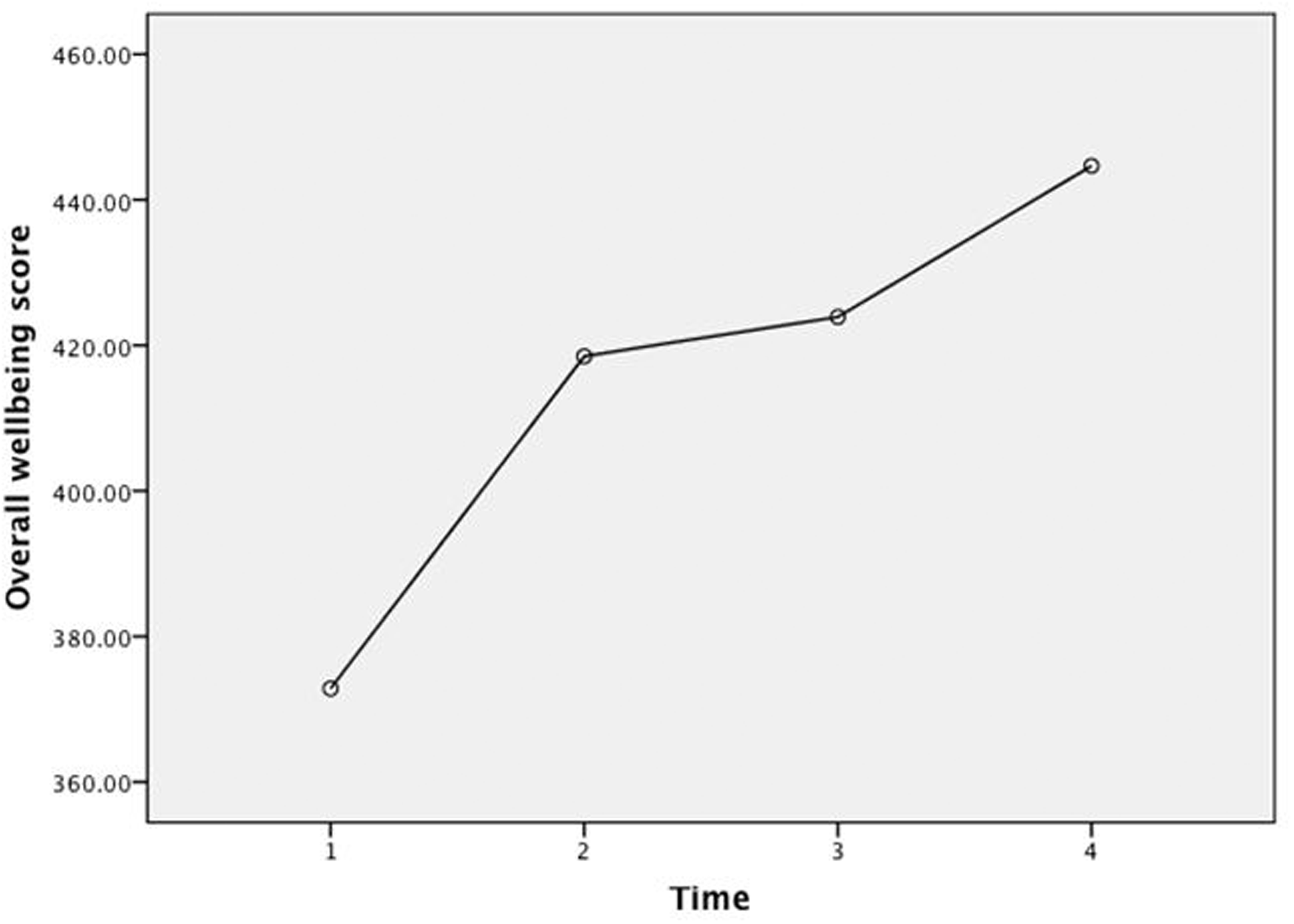
Comparison of overall wellbeing change scores
This analysis tested Hypothesis 6 that the increase in subjective wellbeing would be significantly greater from object handling than art viewing for both participant groups. Descriptive statistics (Table 4) indicated that for people with dementia, when art viewing was presented last, there was less of an increase in overall wellbeing than when object handling was presented last. However, paired sample t-tests found no significant differences between object handling and art viewing wellbeing change scores for either people with dementia or caregivers within orders 1 and 2. Therefore, Hypothesis 6 was not supported for people with dementia or caregivers.
Data from feedback forms
The evaluative comments overwhelmingly conveyed positive responses and enjoyment of the activities. One question asked “How did you find the session today?,” with 91% of the 66 respondents using positive adjectives such as “interesting,” “excellent,” and “uplifting,” while 6% used neutral adjectives such as “OK.” Examples of other responses included “it’s a privilege to be able to hold something so old” and the session “brought me to life.” A further question asked participants which activity they preferred with 55% (n = 36) selecting museum object handling, 36% (n = 24) art discussion, and 9% (n = 6) “both equally.”
Discussion
Summary of findings.
Findings are in line with previous research with nondementia populations, which demonstrated that brief object-handling interventions brought about significant increases in subjective wellbeing (e.g. Paddon et al., 2014). Broadly, findings are also in line with studies showing that museum art-viewing sessions elicit enjoyment and improvements in mood among people with dementia and caregivers (e.g. Rosenberg, 2009). Previous research has also indicated that the intervention site was deemed to be an important aspect to participants (Camic et al., 2014; Roberts et al., 2011). Yet, as popular as art-based interventions have become for this population, thus far there remained limited evidence to refute that psychological benefits obtained could not be attributed to group or social factors. In the present study, the refreshment break formed a social occasion and did not bring about increases in participants’ wellbeing. An alternative explanation may be that the break was of insufficient duration; making it of equal length to the other interventions would have enabled a more robust comparison; however, the present findings do not support the suggestion that any group social activity increases wellbeing. This study demonstrated the feasibility of using VAS multiple times during museum sessions with people with early to middle stage dementia. Previous research in object handling used VAS to measure wellness and happiness; therefore, the addition of subscales measuring interest, confidence, and optimism added a further dimension.
Theoretical explanations
Working memory may remain relatively intact in people in early stage Alzheimer’s (Morris, 1994). Art-viewing and object-handling activities were structured to appeal to this residual ability as they used primary sensory functions and required focus only on what was happening in the present moment. The facilitator’s questions elicited “in the moment” observations with the aim that people with dementia were not placed at a disadvantage, as factual knowledge was not emphasized. However, it was noticed that participants, including people with dementia, frequently asked questions that indicated they wished to acquire facts about the objects and paintings. This may imply that acquisition of semantic knowledge is more important to this population than previously thought and is analogous with findings suggesting that the arts can be used to support new learning in people with dementia (Eekelaar et al., 2012).
Isserow (2008) posited that wellbeing benefits in art-based interventions may at least partly be attributed to the triangular element of the experience, whereby attention jointly directed at an art object by the person with dementia–caregiver dyad forms a shared experience, promoting enjoyment from the shared interactions that follow. Object handling adds a tactile element to viewing and discussion and in turn may elaborate and intensify these aspects of the shared social experience (Thomson, Ander, Menon, Lanceley, & Chatterjee, 2012) in the group or dyad. For both caregivers and people with dementia, both art viewing and object handling appeared to enhance wellbeing, lending support to existing guidelines for psychosocial interventions in dementia care that recommend a more elaborate kinesthetic and multisensory experience (Spector, Woods, & Orrell, 2008). Museum object handling differs from therapies using reminiscence objects, as the artifacts are usually novel and rare. Some authors have suggested that the process of encountering novel stimuli can increase cognitive processing in people with dementia, especially in a context with cocurrent social interaction, positing that this may lead to new neuronal connections being formed (Spector et al., 2008). Ander et al. (2012) found that participants frequently expressed a sense of privilege in being able to touch museum artifacts and wonder at the historical significance of the objects during handling sessions, and suggested these may be key determinants implicated in increasing subjective wellbeing. A sense of privilege may have been particularly potent for this group, given that stigma and social exclusion are often associated with dementia (Graham et al., 2003).
Limitations
Participants were recruited from postdiagnostic support groups making it not possible to generalize to all people with dementia and caregivers, as people do not attend these groups for a range of reasons. It is also not known whether participants who volunteered did so due to an existing interest in art. Most people with dementia in the study were male and most caregivers were female; this gender imbalance formed a potential confounding variable that needs to be considered in planning future research. The design of the present study required a measure of subjective wellbeing suitable for repeated administration. Due to their brevity, the dimensions captured by the VAS were limited in scope and comprehensiveness. The meaningfulness of the results were also dependent on the extent to which participants were able to understand the concepts represented by the VAS (Wewers & Lowe, 1990), although only a few people with dementia appeared to have limited difficulty with this which appeared to resolve after further explanation. In addition, it is acknowledged that the nonsignificance of the main effect of order in ANOVAs may have been due to an insufficient number of participants to achieve power (82 participants were required for the between-subjects factor), therefore findings should be considered in light of this.
Practice implications
The results lend support to healthcare professionals encouraging people with dementia and caregivers to make use of museum activities such as object handling and viewing art after being recently diagnosed. Museum activities should also be considered through the progression of dementia, including use in day care and residential care settings through museum outreach programs or the development of “mini-museums” within care homes (Camic & Kimmel, 2015). Using material objects and art works also offers cocurating opportunities for people with dementia and caregivers working together with museum/art gallery staff to develop in-house museum tours and traveling exhibitions to care homes. The intervention provided an implicit message that meaningful activities can continue after diagnosis in line with a rehabilitation-based approach to dementia care (Clare et al., 2000). Several caregivers commented on the appeal of a group suitable for their needs that was situated in a nonmedical institution, supporting previous ideas of the value of offering therapeutic interventions not associated with illness in nonstigmatizing community settings (Ander et al., 2012). Healthcare and museum professionals could consider formalizing links in order to offer health-related psychosocial interventions within such stimulating and engaging settings (Camic & Chatterjee, 2013).
Future research
To further explore the benefits of this type of intervention, multiple museum sessions over a longer period of time are recommended. Adding measures to assess cognitive domains alongside wellbeing, as has been done in singing research (Särkämö et al., 2014), would broaden our understanding of the impact. Using museum sessions as a community-based, non-clinical intervention to support dyad relationships (Camic et al., 2014) is also worth investigating in order to further determine their psychosocial value for dementia care. A three-armed randomized controlled trial to compare object handling, art viewing, and a treatment-as-usual group would provide more robust evidence for the efficacy of these activities. Further research would also benefit from observational methods such as using video recording to code aspects of physical engagement with objects alongside VAS measures. Zeilig et al. (2014) has recommended that research is further broadened to include people with moderate–severe dementia and results of the present study warrant further investigation into art viewing and object handling as potentially helpful interventions for this population.
Conclusions
This study compared two art-based activities, object handling and art viewing, and a social activity in the form of a refreshment break, that took place within a museum setting. It is the first study of its kind to quantitatively demonstrate that art viewing and museum object handling both showed statistically significant increases in subjective wellbeing as compared to a nonart social event for people with dementia and their caregivers, further delineating the value of the museum activities as a psychosocial intervention. Collaboration between healthcare providers and museum or arts professionals provides an example of harnessing existing community resources to promote psychosocial wellbeing outside of traditional medical settings. Best practice guidelines for psychosocial interventions in dementia care now recommend engagement in arts-related activities and sensory stimulation (Guss et al., 2014), although the evidence for museum-based interventions remains a small but growing area of research. Since social and cognitive stimulation are commonly cited as needs for people with dementia (Cohen-Mansfield, 2005), it seems a highly appropriate time to extend the research base to evidence what the arts can contribute to meeting these needs. In this study, we have demonstrated that art activities in a museum can be accessed and enjoyed by people with dementia and their caregivers, and that such activities provide a beneficial impact on subjective wellbeing in a way that refreshments and conversation do not.
Footnotes
Acknowledgements
The authors would like to thank the people who participated in this project for generously volunteering their time and providing feedback about their experiences of the interventions. We would also like to thank the award winning Beaney House of Art and Knowledge in Canterbury, Kent, UK for being such welcoming hosts of the project and offering their expertise, time, and long-term commitment to community-oriented research. Special thanks to Kent and Medway National Health Service Partnership Trust for their knowledge about dementia care and help with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.