
Abstract
Objectives
Despite the increasing prevalence of dementia, little is known about individuals’ attitudes towards euthanasia on patients with dementia or cognitive impairment.
Methods
Nurses (n = 1003) and representatives of the general public (n = 2796), recruited via social media and the Finnish Nurses Association, completed an electronic questionnaire in 2014.
Results
Euthanasia due to severe dementia was approved by 54.6% of nurses and 64.4% of the general public. Depending on the age of the patient, between 50.0% and 54.7% of nurses and between 58.3% and 60.9% of the general public supported euthanasia on patients with severe cognitive impairment.
Discussion
The attitudes towards euthanasia due to dementia or cognitive impairment are slightly more accepting among the general public than among nurses. Apart from religiosity, none of the background factors were found to be reliable predictors of individuals’ attitudes. Additional research is needed to describe the underlying reasons for the attitudes.
Introduction
Dementia is one of the most common degenerative conditions in developed countries. Due to the increasing age of the population, the number of this currently underdiagnosed illness is expected to double by 2050 (Chambaere, Cohen, Robijn, Bailey, & Deliens, 2015; Gastmans & De Lepeleire, 2010). International literature emphasizes the need for the improvement of end-of-life (EOL) care in patients with dementia. However, it has been argued that some older persons wish to control the circumstances of their own death, e.g. by requesting euthanasia (Chambaere et al., 2015; Tomlinson, Spector, Nurock, & Stott, 2015).
Euthanasia is one of the most controversial question about EOL. By the beginning of 2017, euthanasia has been legalized in five countries worldwide: Belgium, Canada, Columbia, Luxembourg and the Netherlands (Emanuel, Onwuteaka-Philipsen, Urwin, & Cohen, 2016; Nys, in 2017). Euthanasia has been a topic of debate in several countries (Emanuel et al., 2016), including Finland, where a citizens’ initiative collected over 63,000 statements of support in 2016 (Seppänen, Viinanen, Soininvaara, & Taipale, 2016), leading to an obligation of the Finnish Parliament to take the issue into consideration (Kansalaisaloite.fi, 2016).
Pursuant to the existing legislation, euthanasia is defined in this study as ‘intentionally terminating life by another person than the person concerned, at this person’s request’ (Nys, in 2017). In Belgium, performing euthanasia on a patient with dementia is illegal based on the advanced euthanasia directive (AED), whereas it is deemed legal in the Netherlands provided that the criteria of due care are met (Gastmans & De Lepeleire, 2010; Kouwenhoven et al., 2015; Nys, 2017). In the Netherlands, the number of euthanasia cases based on dementia was 3 in 2006 (Tomlinson & Stott, 2015), while in 2015, euthanasia was performed on 109 persons with dementia and eight individuals with dementia and an additional condition, such as cancer (Regionale Toetsingcommissies Euthanasie, 2016). These figures indicate increasing prevalence of euthanasia performed on individuals with dementia, which may not be addressed by the changes in the Dutch legislation (Emanuel et al., 2016; Nys, 2017).
The amount of previous literature focusing on the attitudes towards euthanasia due to dementia or cognitive impairment is limited (Chambaere et al., 2015; Tomlinson et al., 2015). This is particularly true among nurses, who play an essential role in palliative care and the euthanasia care processes (De Bal, Gastmans, & Dierckx de Casterlè, 2008; Dierckx de Casterlé, Denier, De Bal, & Gastmans, 2010; Francke, Albers, Bilsen, de Veer, & Onwuteaka-Philipsen, 2015). The attitudes among the general public towards euthanasia due to dementia have been found to be more accepting compared with the healthcare professionals (Ryynänen, Myllykangas, Viren, & Heino, 2002; Tomlinson & Stott, 2015). In the Netherlands, the majority of the general public agreed with euthanasia due to advanced dementia based on the AED, whereas physicians regarded it as morally and legally problematic (Kouwenhoven et al., 2015). This study aims to explore the attitudes towards euthanasia performed on individuals with dementia and severe cognitive impairment as well as to describe the underlying factors of these attitudes among nurses and the general public in Finland.
Methods
Participants
The participants of this study included nurses and representatives of the general public, who had sufficient skills in the Finnish language and were at least 18 years old. Details about the study were published on the public research blog, Facebook page and Twitter profile of the first author, and on seven discussion forums. These recruitment channels provided an opportunity to reach a large and heterogeneous population, including individuals who are hard to reach with traditional methods (Khatri et al., 2015; Otieno & Matoke, 2014). For example, over 100,000 nurses are registered in Finland, of which around half are members of the Finnish Nurses Association (Ailasmaa, 2014; The Finnish Nurses Association, 2014). It would not have been possible to reach the nurses who are not members of the Finnish Nurses Association using traditional recruitment approaches alone. The information about the study was also published in the members’ bulletin of the Finnish Nurses Association in October 2014. More detailed information about participant recruitment is provided elsewhere (Terkamo-Moisio et al., 2017; Terkamo-Moisio et al., 2016).
Data collection
Data collection was carried out over four weeks between October and November 2014 with an electronic questionnaire designed for this study. To avoid ambiguity, euthanasia was clearly defined in the questionnaire, which consisted of four components: demographic characteristics, work-related characteristics, the Centrality of Religiosity Scale (CRS) (Huber & Huber, 2012) and two different patient scenarios which have previously been used by Ryynänen et al. (2002).
Demographic characteristics included the participant’s age, gender, marital status and the most recent level of education completed. They were also asked to note whether they had children, their primary region of residence and their religious affiliation.
Only nurses were asked to submit information regarding their work-related characteristics, including their work experience, workplace, shift patterns and the most common type of patient. In addition, nurses were asked to assess their expertise in pain management and EOL care on a four-step scale (very poor – very good) as well as the frequency of their encounters with dying and dead patients (never – daily).
The CRS, presented in detail by Huber and Huber (2012), includes five dimensions of religiosity: intellect, ideology, public practice, private practice and experience based on the multidimensional model of religion by Stark and Glock (1968).
Finally, two patient scenarios (Table 1) were presented to the participants, who were asked to report their agreement with euthanasia in each case on a five-step Likert scale (strongly disagree – cannot say – strongly agree). The three variations on the age (10, 30 and 50 years) of the patient were presented for the scenario related to severe cognitive impairment (Table 1). The variations were randomly changed once per day during the data collection. Thus, only one age variable was presented to each participant.
Content of the patient scenarios.

Ethical considerations
An ethical approval was obtained prior to the data collection from the Committee on Research Ethics of the university (Approval 5/2014) to which the first author is affiliated.
Data analysis
The data analysis was conducted with SPSS 21 for Windows. No records were excluded from the data analysis. The initial nine-category variable of most recent education was recoded into six educational categories based on the International Standard Classification of Education (ISCED; Official Statistics of Finland, 2014). Moreover, the initial five-category variables measuring the acceptance of euthanasia in the patient scenarios were recoded into three categories: disagree – cannot say – agree. The aggregate of CRS was deductively computed for each participant (Huber & Huber, 2012), and, subsequently, the participants were categorized into two groups based on their religiosity. The associations between the attitudes of the participants towards euthanasia in the presented patient scenarios and the independent variables were investigated with the Chi-square test χ2 (Field, 2013). A p-value of <0.05 was considered to indicate statistical significance (Field, 2013).
Results
Participants
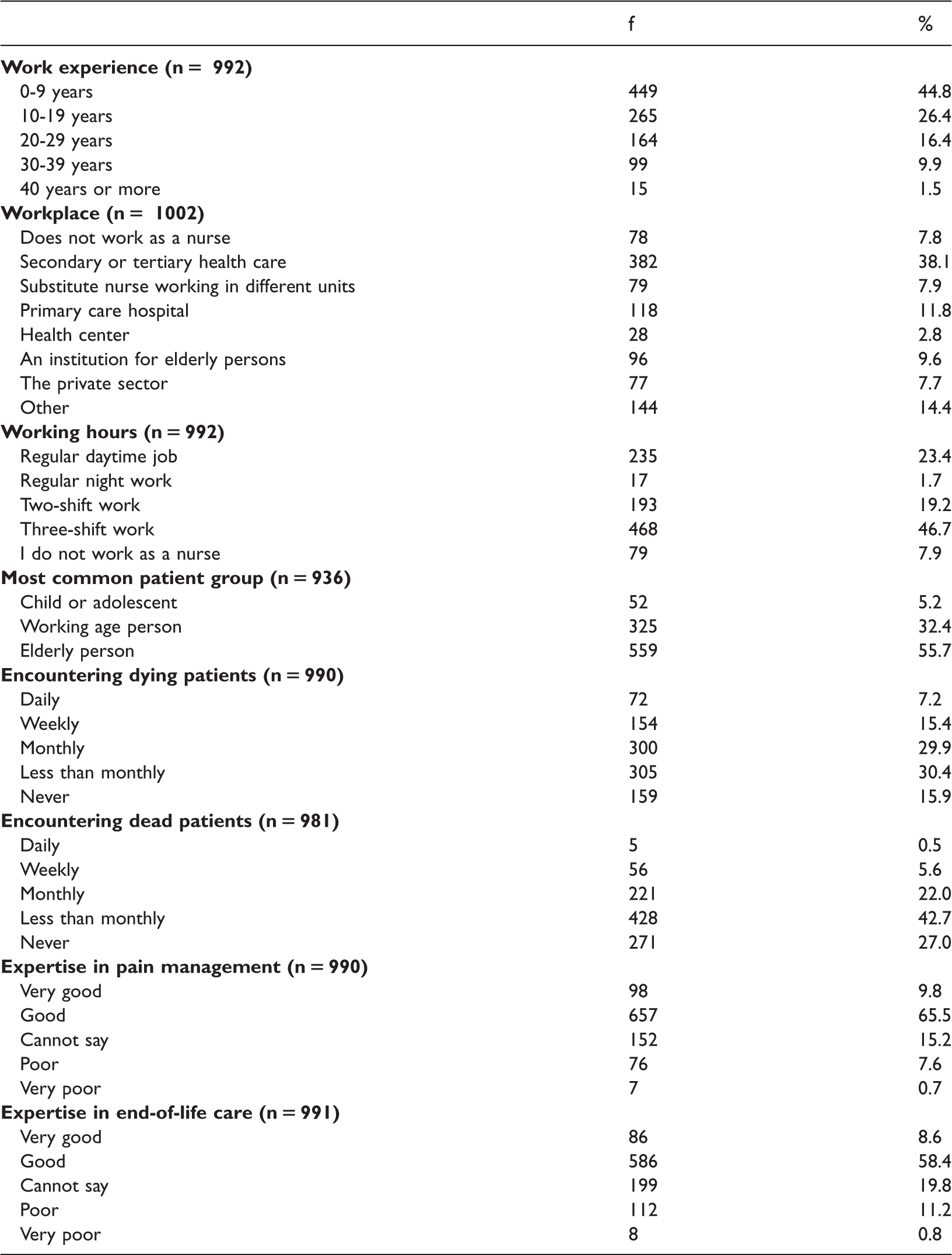
A total of 1003 nurses and 2796 representatives of the general public participated on this study. The age of the nurses ranged from 20 to 73 years (mean 39.54, SD 11.9) and the general public from 18 to 84 years (mean 39.50, SD 12.9; Table 2). Nurses’ work experience in the healthcare sector varied from 0 to 52 years (mean 13.16, SD 10.6). Most of them worked in secondary or tertiary care and encountered dying patients monthly or less frequently (Table 3). Most of the nurses assessed their expertise as good in both pain management and EOL care.
Characteristics of the participants.
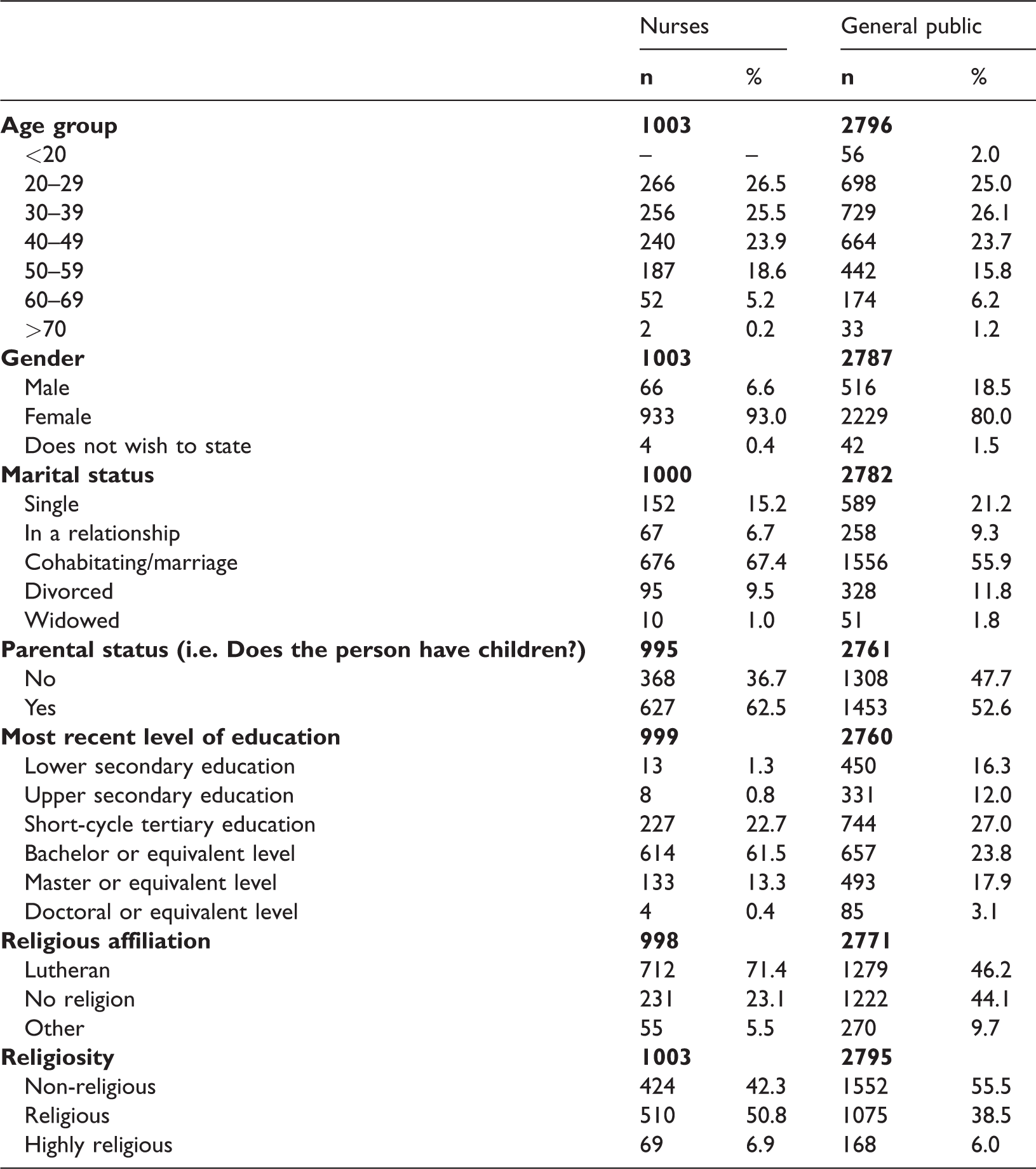
The number of responses varies due to missing data.
Nurses’ work-related characteristics.
Attitudes towards euthanasia due to dementia and cognitive impairment
Euthanasia on a patient with severe dementia was accepted by 54.6% of the nurses and 64.4% of the general public (Table 4). Furthermore, around half of the nurses agreed with euthanasia on a patient with severe cognitive impairment, whereas the acceptance among the general public was slightly higher. Statistically significant difference was found between the attitudes of nurses and the general public towards euthanasia in both scenarios (Table 4).
Attitudes towards euthanasia on patients with severe dementia and severe cognitive impairment.
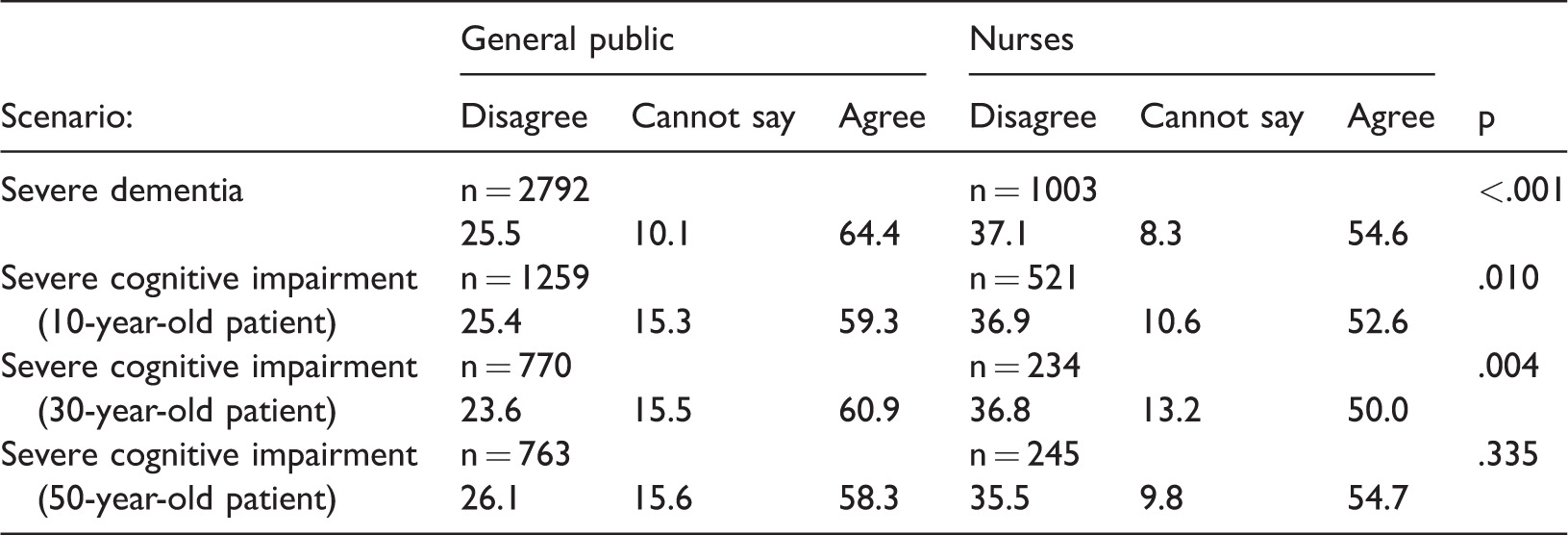
Note. p-value indicates the statistical significance of agreement between the general public and nurses.
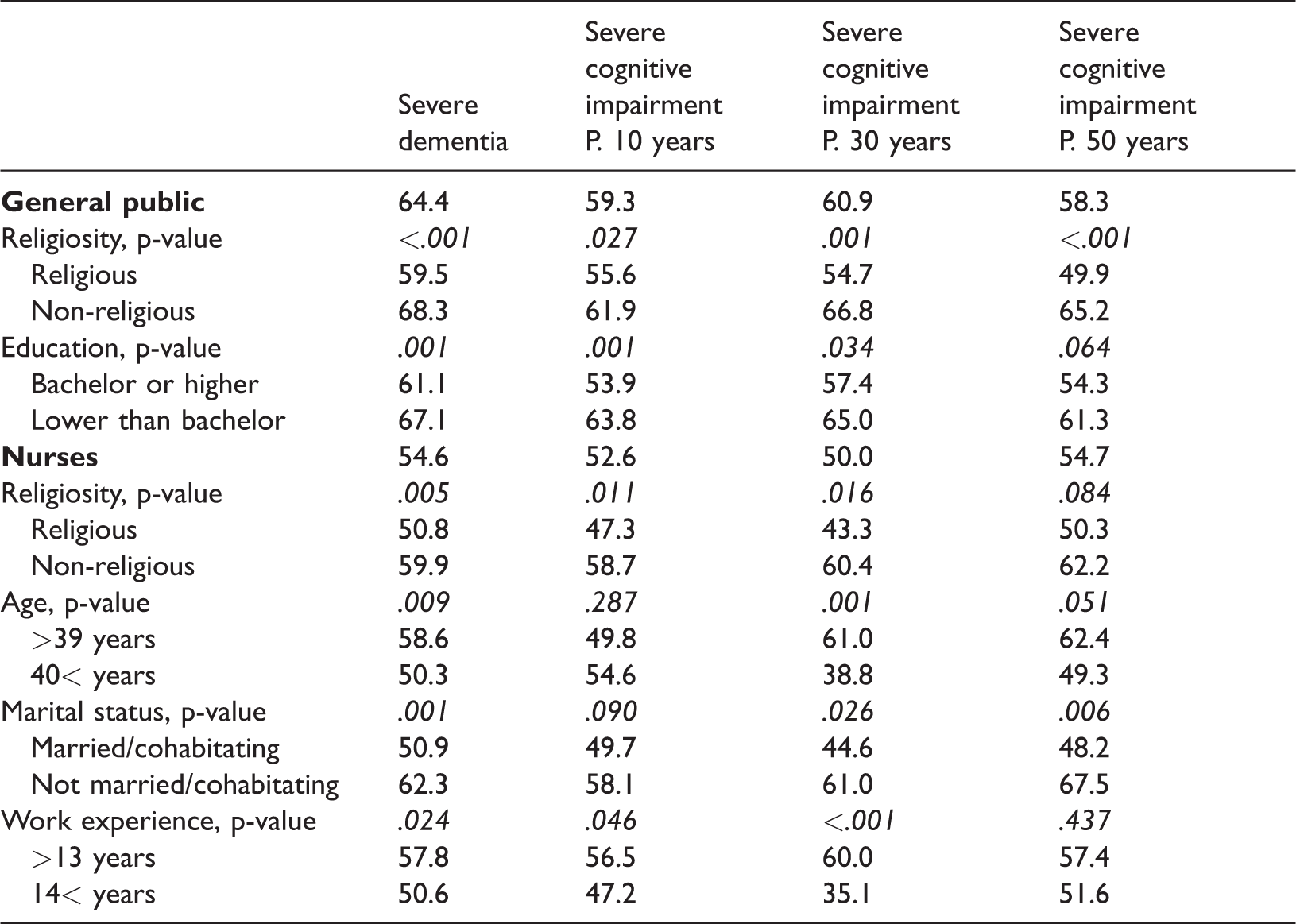
In both groups, religiosity was associated with the participant’s acceptance of euthanasia (Table 5), indicating lower acceptance compared with the non-religious participants. In addition, higher level of education indicated more rejecting attitudes towards euthanasia among the general public, but not among the nurses (Table 5). Among the nurses, more work experience in healthcare settings indicated a less permissible attitude in all of the presented scenarios, with an exception concerning a 50-year-old patient with cognitive impairment (Table 5). Moreover, among nurses, younger age indicated greater acceptance of euthanasia due to dementia and severe cognitive impairment in a scenario with a 30-year-old patient, whereas there was no statistically significant association between age and attitudes among the general public. Nurses who were married or cohabitating were less likely to accept euthanasia due to severe dementia and cognitive impairment in 30- and 50-year-old patients (Table 5). Among the general public, being married or cohabitating indicated greater rejection of euthanasia on a 10-year-old patient with metal deficiency (p=.028) but not in other patient scenarios. No statistically significant association was found between the attitudes and gender or parental status in either group. Similarly, there was no statistically significant association between nurses’ attitudes towards euthanasia and their workplace, working hours, expertise in pain management/EOL care, the frequency of encountering dying/dead patients or other patients for whom they provide care.
Acceptance (%) of euthanasia according to the associated factors.
Discussion
Our results provide new knowledge about the attitudes of nurses and the general public towards euthanasia due to severe dementia and cognitive impairment and thus contribute to the ongoing discussion on the topic. In general, around one half of the nurses and over half of the general public accepted euthanasia on a patient with severe dementia and cognitive impairment in the current study. This finding is in line with The Netherlands, where one-third of physicians as well as most nurses (58%) and the general public (77%) would agree with euthanasia in case of severe dementia (Kouwenhoven et al., 2013). However, our results are contradictory with findings from Cyprus, where the majority of the general public opposed euthanasia due to incurable illness and/or dementia (Televantos, Talias, Charalambous, & Soteriades, 2013). The latter findings were associated with deep religious beliefs and cultural traditions, whereas Finland is regarded as a secularized country with an individualistic culture (Cohen et al., 2006; Televantos et al., 2013). This explanation is supported by the results of the present study, in which religiosity was an important predictor of one’s attitudes towards euthanasia in line with previous findings in this regard (Bolt, Snijdewind, Willems, van der Heide, & Onwuteaka-Philipsen, 2015; Ryynänen et al., 2002; Televantos et al., 2013; Tomlinson & Stott, 2015). However, religiosity is a concrete predictor only once it has been divided into multiple, separately assessed dimensions, such as in the present study (Terkamo-Moisio et al., 2016).
In our results, nurses were less supportive towards euthanasia than the general public, which confirms previous findings in this regard (Kouwenhoven et al., 2013; Ryynänen et al., 2002; Tomlinson & Stott, 2015). This may be attributed to the higher level of knowledge about healthcare that nurses have based on their profession. The association between nurses’ work experience and their acceptance of euthanasia may be considered to support this explanation.
Comparison of our results with a previous study from the same cultural context with identical patient scenarios (Ryynänen et al., 2002) indicates that acceptance has increased in both groups during the past decade. The study of Ryynänen at al. (2002) revealed that 48% of the general public accepted euthanasia based on severe dementia and 42% due to severe cognitive impairment in Finland. Among the nurses, the acceptance rates were 23% and 22%, respectively. Most physicians (92%) opposed euthanasia in both cases (Ryynänen et al., 2002), Due to the differences in recruitment and assessment of the studies, this is a tentative suggestion. However, society’s shift towards a more liberal culture may influence individuals’ attitudes towards euthanasia (Cohen et al., 2006).
Somewhat surprisingly, the age of the patient in the vignettes depicting severe cognitive impairment did not influence participants’ euthanasia-related attitudes, which highlights the need for further research concerning the underlying rationale people may have.
In both scenarios presented in our study, the patients were unable to express a euthanasia request due to their health condition and no details on their AED were given in the scenarios. Therefore, the scenarios did not exactly comply with the existing euthanasia legislation, although the responses reflected the respondents’ acceptance of euthanasia (Nys, 2017). Deliberate termination of life without the patient’s explicit request is an illegal act in Belgium and the Netherlands. However, it has been argued that his procedure nevertheless takes place in both countries on the grounds of shortening a patient’s agony or alleviating the burden of his or her relatives (Cohen-Almagor, 2015, 2016). Quality of life is perceived differently by every individual, which makes it difficult to determine it for someone other than the person himself/herself. Thus, the possibility that relatives project their personal concerns onto a family member with dementia can be considered as a risk for a problematic euthanasia (Gastmans & De Lepeleire, 2010), an idea that is further highlighted by the experiences of some caregivers based on which dementia is worse for those close to the patient than to the patient himself/herself (Tomlinson et al., 2015). Moreover, defining the right moment for performing euthanasia has been perceived challenging. In the early stages of dementia, the patient has the capacity to make a euthanasia request, but terminating a patient’s life at this point is seen as premature, as his or her quality of life can still be preserved for an undefined period of time (Bolt et al., 2015; Cohen-Almagor, 2016; Gastmans & De Lepeleire, 2010; Kouwenhoven et al., 2015). At the advanced stage of dementia, patients are no longer able to express their views or current priorities, which might have been changed over time, even in cases where an AED is available (Bolt et al., 2015; Cohen-Almagor, 2016; Gastmans & De Lepeleire, 2010).
Further explanation to the increasing acceptance of euthanasia, especially in case of dementia, may be found in the individualistic values of Western societies that emphasize the respect for autonomy and the dignity of an individual, which is (incorrectly) seen as part of one’s intellectual capacity (Cohen-Almagor, 2016; Gastmans & De Lepeleire, 2010). Thus, the positive attitudes towards euthanasia due to dementia and cognitive impairment apparent in our results might reflect the fear of loss of dignity or becoming a burden to others. However, additional research is needed in this regard.
Furthermore, it has been noted that euthanasia should be granted for individuals with advanced dementia out of respect for autonomy (Gastmans & De Lepeleire, 2010; Kouwenhoven et al., 2015). However, in the advanced stage of dementia, or in case of severe cognitive impairment, individuals often have no recollection of their autonomous self (Cohen-Almagor, 2016). Thus, respecting their humanity and dignity ought to be in the focus of the provided care (Cohen-Almagor, 2016; Gastmans & De Lepeleire, 2010).
The current results demonstrate that little is still known about the underlying rationale of individuals’ attitudes towards euthanasia in case of dementia and cognitive impairment. The increasing prevalence of dementia emphasizes the need for additional research in this area. Based on previous literature and the current results, we consider the improvement of palliative care, in particular for dementia, as crucial for ensuring that the positive attitudes towards euthanasia are not based on the respondents’ fear of an undignified end of life.
Limitations
Even though out results are based on a large and heterogeneous dataset, this study has some limitations. Those concerning the recruitment of participants and data collection have been discussed in detail in previous papers (Terkamo-Moisio et al., 2017; Terkamo-Moisio et al., 2016). The way in which the patients presented their euthanasia request was not described in the scenarios, which may be considered as a limitation. However, we did not want to change the form of the original formulations to ensure the comparability of the results. It has been argued that vignettes may not exactly reflect the reality (Evans et al., 2015). In this study, the presented vignettes were considered to provide an appropriate means for determining the influence of a number of factors on individuals’ attitudes. The undisputed gender bias among the general public limits the generalization of the results in this group. However, the gender of the participants was not statistically significantly associated with their attitudes in our results, which makes this limitation less severe. By contrast, a comparison of the sample of nurses with a previous randomized sample (Ryynänen et al., 2002) revealed no differences in the gender distribution or mean age of the nurses, which strengthens the generalizability of our results concerning the nurses.
Conclusion
Attitudes towards euthanasia on patients with severe dementia or cognitive impairment were more accepting among the general public than nurses. Aside from religiosity as a predictor of euthanasia-related attitudes, little is known about the underlying rationale. The increasing prevalence of dementia in the aging population highlights the significance of additional research and development of the palliative care, especially in the context of this patient group.
Footnotes
Acknowledgements
We would like to express our gratitude to all of the participants in this study, without whom this article would not exist.