
Abstract
Background
Medical decision-making capacity is impaired in Alzheimer’s disease and mild cognitive impairment. Medical decision-making capacity depends on many different cognitive functions and varies due to situation and cognitive, social, and emotional status of the patient. Our aim was to analyze dementia patients’ capacity to estimate risks and benefits in different clinical trials and determine how cognitive decline affects their attitude toward possible participation and proxy consent.
Methods
Groups: Alzheimer’s disease (n = 20), mild cognitive impairment (n = 21) and healthy controls (n = 33). Two hypothetical clinical trials, a standardized interview and three visual analogue scales were used to investigate decisions, estimations, reasoning, and attitudes.
Results
A general positive attitude toward participation in clinical trials was shown among all groups. Both patients and controls motivated possible participation as “own-benefit” in the low-risk trial and to “help-others” in the high-risk trial. Individuals who accepted to participate in the high-risk trial scored lower in medical decision-making capacity in comparison to participants who would not have participated (p < .01). Patients in the Alzheimer’s disease but not mild cognitive impairment and healthy control groups underestimated risks and overestimated benefits in the high-risk/low-benefit trial (p < .05). A family member was most frequently chosen as possible proxy (91%).
Conclusions
Medical decisions and research consent should be interpreted with caution in patients who are already in early stages of dementia, as the patients’ acceptance to participate in high-risk trials may be due an insufficient decisional capacity and risk analysis, accelerated by a general desire to make good to society. We emphasize the use of a standardized tool to evaluate medical decisional capacity in clinical research.
Introduction
Patients’ decisional capacity may be impaired in various age-related diseases such as Alzheimer’s disease (AD) and mild cognitive impairment (MCI) (Gurrera et al., 2006; Jefferson et al., 2008; Marson et al., 1996; Okonkwo et al., 2008; Tallberg et al., 2013). A growing aging population alerts ethical challenges in dementia research and patients’ decisional capacity. Consent given by free will is central in medical law, to protect the patients against undesirable intervention. Informed consent emphasizes the importance of providing sufficient information for decisions. Healthy adults are assumed to possess consent capacity unless there are specific reasons to believe otherwise, such as suffering from mental disorders or inability to communicate. If the capacity to give informed consent is considered insufficient, proxy consent is a possible solution (Appelbaum, 2007; Panting, 2010; White & Seery, 2009). Medical decision-making capacity (MDMC) is an established term to describe the capacity to make medical decisions such as giving consent to a treatment or a clinical trial. Several previous studies have estimated MDMC in different groups with impaired cognitive function by using hypothetical medical scenarios, standardized interviews, and protocols (Marson et al., 1995; Grisso, Appelbaum, & Hill-Fotouhi, 1997; Tallberg et al., 2013). The decisional capacity is based on various cognitive standards such as expressing a choice, appreciation, reasoning, and understanding (Okonkwo et al., 2008). The capacity to give consent may vary depending on the complexity of the decision-making situation (Panting, 2010) and social and emotional status of the patient (Sugarman et al., 2007). Healthy elderly tends to participate in clinical trials because of curiosity, self-interest, and altruism (Tolmie et al., 2004). A different communication style toward research has been noted in patients with impaired cognitive function; a silent but agreeing attitude, which may risk but perhaps not correctly be interpreted as willingness to participate (Sugarman et al., 2007). The decisional capacity varies over time; patients with both very mild and mild dementia may understand information relevant for making a decision, while patients with a more progressed dementia may struggle with similar task (Buckles et al., 2003). Patients considered incapable to give consent to both low- and high-risk studies may still have preserved capacity to appoint a proxy for substitute decision (Kim et al., 2011). Attitudes toward proxy are highly dependent on the potential risk associated with the situation; a more comfortable attitude with proxy consent is noted regarding involvement in low-risk research (Ayalon, 2009; Dubois et al., 2011). Decisional capacity rests on numerous interactions between different cognitive functions and may preferable be evaluated in patients with cognitive impairment by examining various decisional abilities separately (Gurrera et al., 2014). Our aim was to investigate how cognitive decline affects the decisional reasoning and capacity to estimate risks and benefits in the context of decision-making to participate in clinical trials.
Methods
The study is a part of an ethical research project initiated by the Swedish Brain Power Network (2017) (www.swedishbrainpower.se). Within the project, we constructed a Linguistic Instrument for Medical Decision-making (LIMD; Tallberg et al., 2013) with the aim to score medical decisional capacity by objective and linguistic measurements. LIMD consists of three parts: three vignettes (hypothetical clinical trials), a standardized interview and a scoring protocol. In current study, we present unpublished data both from the transcriptions of participants reasoning in the LIMD-interviews and analyses of estimated risk and benefit by VAS, which was included in the major data collection beside LIMD. The recruiting process, demographic factors, diagnosis and MDMC of the participants are described in detail in previous studies (Stormoen et al., 2014; Tallberg et al., 2013) and briefly presented below.
Participants
The study includes three groups: mild AD (n = 20), MCI (n = 21) and healthy controls (HC; n = 33). Non-significant group effects (all p > .10) for gender distribution, age, and years of education. The groups differed significantly in cognitive severity by the Mini-Mental State Examination (MMSE; p < .001) (Folstein, Folstein, & McHugh, 1975) and MDMC by the LIMD (p < .001) (Tallberg et al., 2013), see Table 1.
Demographic characteristics (gender, age and years of education), cognitive severity (MMSE) and MDMC (LIMD) in groups of subjects (AD, MCI and HC).
Note: All data are presented as mean ± standard deviation.
ns: non-significant; MMSE: Mini-Mental State Examination; LIMD: Linguistic Instrument of Medical-Decision; AD: Alzheimer’s disease; MCI: mild cognitive impairment; HC: healthy controls.
Recruiting process, inclusion and exclusion criteria
The patients (AD and MCI) were recruited from a university-based memory clinic, after being examined and diagnosed according to a standard protocol as part of the clinical routine. Patients with MMSE < 20, other primary diseases, dyslexia and/or impaired vision or hearing were excluded. HC were recruited among spouses to the patients and by advertising.
Diagnosis
The diagnosis of AD patients followed the criteria set by the National Institute of Neurological and Communications Disorders – Alzheimer’s disease and Related Disorders Association (NINCDS-ARDA) (McKhann et al., 1984). The diagnosis of MCI was made according to modified clinical criteria, which required subjective complaints and objective verification of cognitive impairment, normal global cognitive function, roughly preserved activities of daily living, and no dementia (Winblad et al., 2004).
Procedures
The participants received written information of two hypothetical clinical trials (described below), presented one at a time, in the same order for each participant. An oral interview was used to assess decisions and attitudes in each trial. The participants could keep the written information while being interviewed. The interviews (described below) were audio recorded followed by an orthographical transcription, which allowed analysis of reasoning and decision. Visual analogue scales (VAS) (described below) were used after the interview to estimate perceived personal risk (“risk”), personal benefit (“own-benefit”) and benefit for others (“other-benefit”) of each trial. One experienced clinician performed the test procedure and analysis (blinded to group).
Assessment tools administrated
Hypothetical clinical trials
The two hypothetical clinical trials (approximately one text page per trial) describe diseases and fictive trials with different degrees of possible risk and benefit. In the low-risk/high-benefit trial, the fictive participant is described as suffering from a serious progressive disease of the kidneys and is informed on the prognosis, which implies extensive dialysis with a high probability of future kidney transplantation. The fictive participant is asked to participate in a trial of a medical treatment, which might stop the disease from further progress, with a low risk of side effects. In the high-risk/low-benefit trial, the fictive participant has hypertensive blood pressure that is satisfactorily managed with standard antihypertensive medication. The fictive participant is presented with a drug trial, and if chosen to participate, will change antihypertensive medication from the presently used to a treatment that offers no additional benefit than the presently used drug, but might help other patients. The new drug is described as carrying a 1/10 risk for a number of benign side effects such as nausea, rash, but also as being associated with a small but significant risk of pulmonary edema with breathing problems and liver cancer.
Interview
Four standardized questions were used: Q1. Would you be willing to participate? Q2. Why would you be willing to participate? Q3. If you were unable to make your own decision, would it be acceptable if anyone else made the decision regarding your participation? Q4. Who would you prefer made the decision in your place?
Q1 and Q3 were asked to all participants. Q2 and Q4 are open follow-up questions, asked to participants responding “yes” to Q1 and Q2. Individual responses were categorized to facilitate a quantitative analysis and comparison between groups and/or trials.
VAS
VAS (100 mm, horizontal scale, no tick marks) were used to measure subjective estimations of (1) personal risk (“risk”), (2) personal benefit (“own-benefit”), and (3) benefit for others (“other-benefit”) for each trial (0= no risk/no benefit, 100= high risk/high benefit).
Statistical analysis
Statistical analysis was performed using SPSS™ Version 22. One-way MANOVA was performed on acceptance to participate (“yes” to Q1) in the two trials as within-participants’ dependent variables and group as independent variable. Four two-way ANOVAs were performed to investigate whether groups and decisions (accepted to participate yes vs. no) had an influence on cognitive severity (MMSE) and medical decisional-making capacity (LIMD) in the two clinical trials. Two-way MANOVAs were performed on estimated risk and benefits (risk, own-benefit and other-benefit) in the two trials as within-participants’ dependent variables and groups as independent variable. These multivariate analyses were followed by one-way ANOVA on each trial and type of estimation to analyze the pattern of results regarding trial, estimate and group. Tukey’s post-hoc t-test was used to analyze pairwise group differences regarding estimates of risk, own-benefit, and others-benefit. One-way MANOVA was performed on acceptance of a proxy as decision maker (answer: “yes” to Q3) in the two trials as within-participants’ dependent variables and groups as independent variable followed by Tukey’s post-hoc t-test to analyze pairwise group differences. All results were presented as mean ± standard deviation.
Results
Acceptance to participate in the trials
A significant difference was shown between the trials regarding overall acceptance of participation (F = 44.1, df = 1/71, p < .001, ε2 = .38) demonstrating a higher acceptance to participate in the low-risk/high-benefit trial (89%) compared to the high-risk/low-benefit trial (42%). No significant difference between groups was demonstrated regarding acceptance to participate in each trial (p > .1), and no significant interaction between groups and trials was demonstrated (p > .1), indicating that AD, MCI, and HC did not differ in acceptance to participate in the two trials. Mean frequency (%) and standard error in acceptance to participate in the two trials for each group are presented in Figure 1.
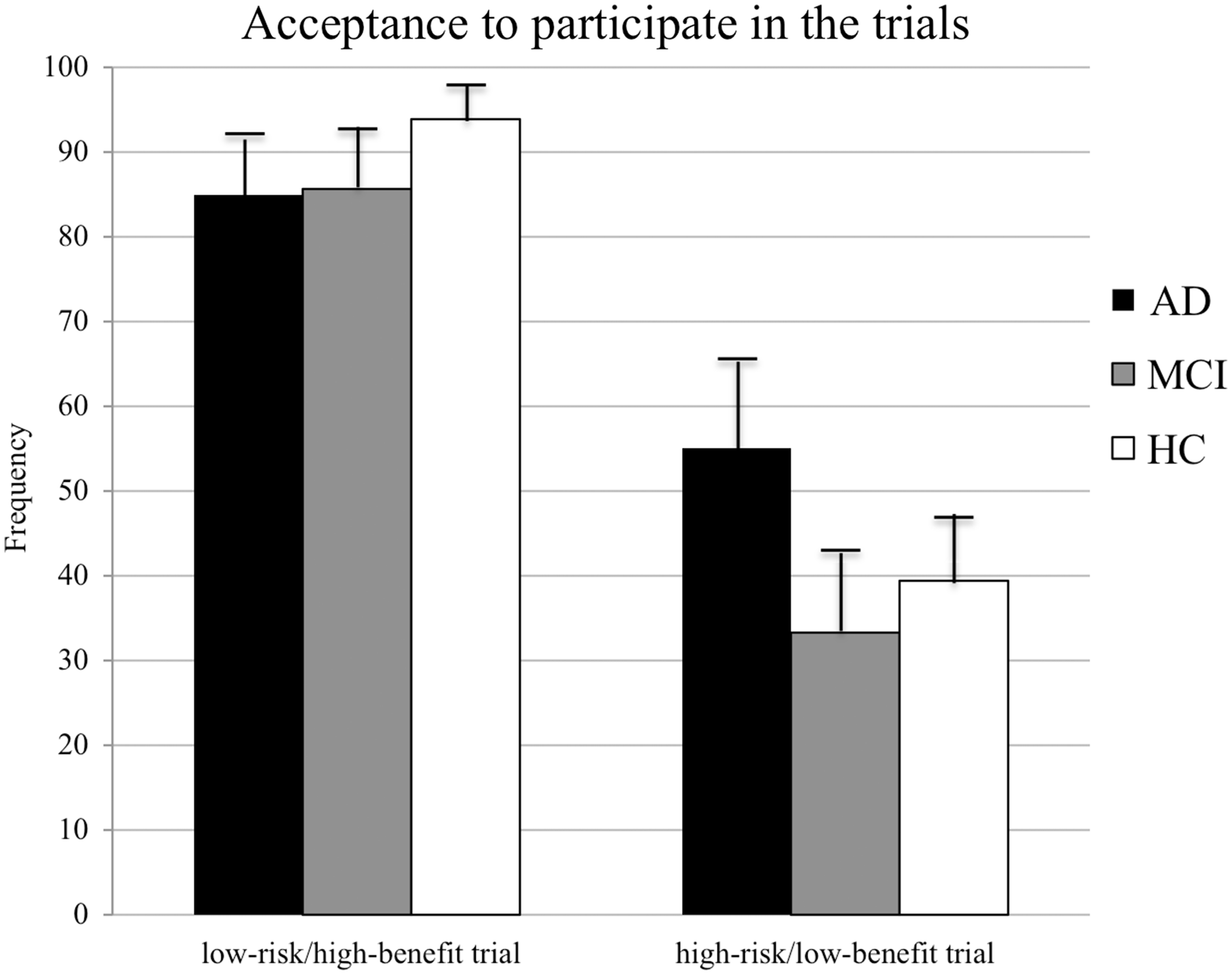
Mean frequency (%) and standard error in acceptance to participate in the two trials (low-risk/high-benefit and high-risk/low-benefit) in groups of subjects (AD, MCI and HC).
Significant differences in medical decisional-making capacity (MDMC by LIMD score) were obtained between groups of participants who accepted to participate in the low-risk/high-benefit (F = 6.60, df = 1/73, p < .01, ε2 = .09) and in the high-risk/low-benefit (F = 3.86, df = 1/73, p < .01, ε2 = .05). Participants who accepted to participate in the low-risk/high-benefit (n = 66) had higher LIMD score (18 ± 8) than participants who did not accept to participate (n = 8; LIMD score 10 ± 9). Participants who accepted to participate in the high-risk/low-benefit trial (n = 31) had lower LIMD score (14 ± 8) in comparison to participants’ who did not accept to participate (n = 43, LIMD score 18 ± 8).
No difference in cognitive severity (MMSE) was shown between groups of participants who were willing or not to participate in each trial (p > .1).
Reasons to participate in the trials
Five categories of reasons to participate in the trials were identified among the individual responses to Q2 (Why would you be willing to participate): “own-benefit”, “help others”, “own benefit and help others”, “support research and make good” and “other reasons” (such as curiosity or difficulties to define). The result showed that “own-benefit” was the primary reason in the low-risk/high-benefit trial (mean frequency across groups: 37%), while “help others” was the primary reason in the high-risk/low-benefit trial (mean frequency across groups: 47%). The different reasons among groups to participate in the trials are presented in Figure 2.
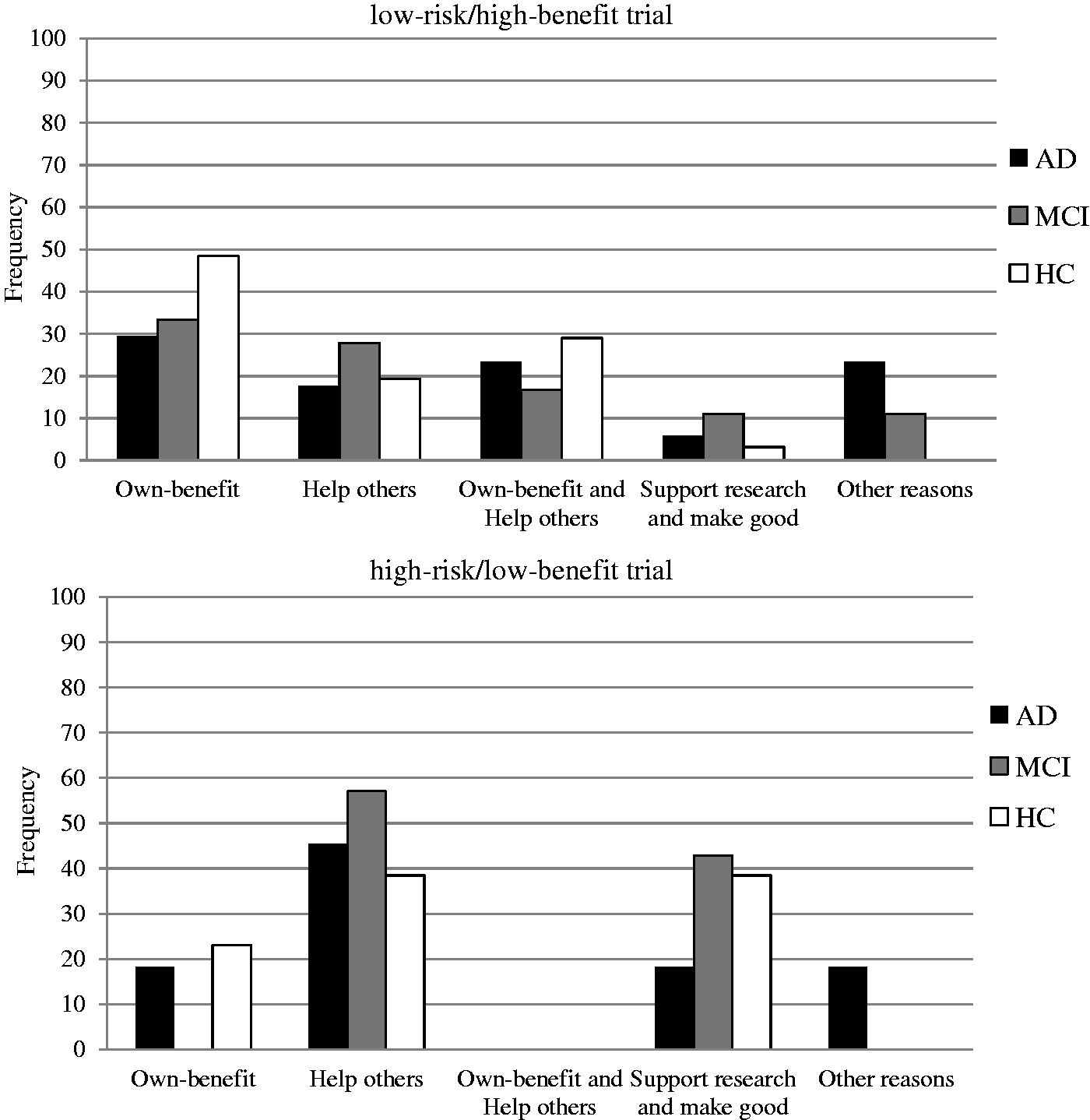
Frequency (%) of different reasons to participate in the two trials (low-risk/high-benefit and high-risk/low-benefit) in groups of subjects (AD, MCI and HC).
Estimations of risk and benefits in the trials
Estimations of risk, own-benefit, other-benefit were measured by VAS (0 = no risk/benefit; 100 = high risk/benefit). Estimations of risk and benefits among groups are presented in Figure 3.
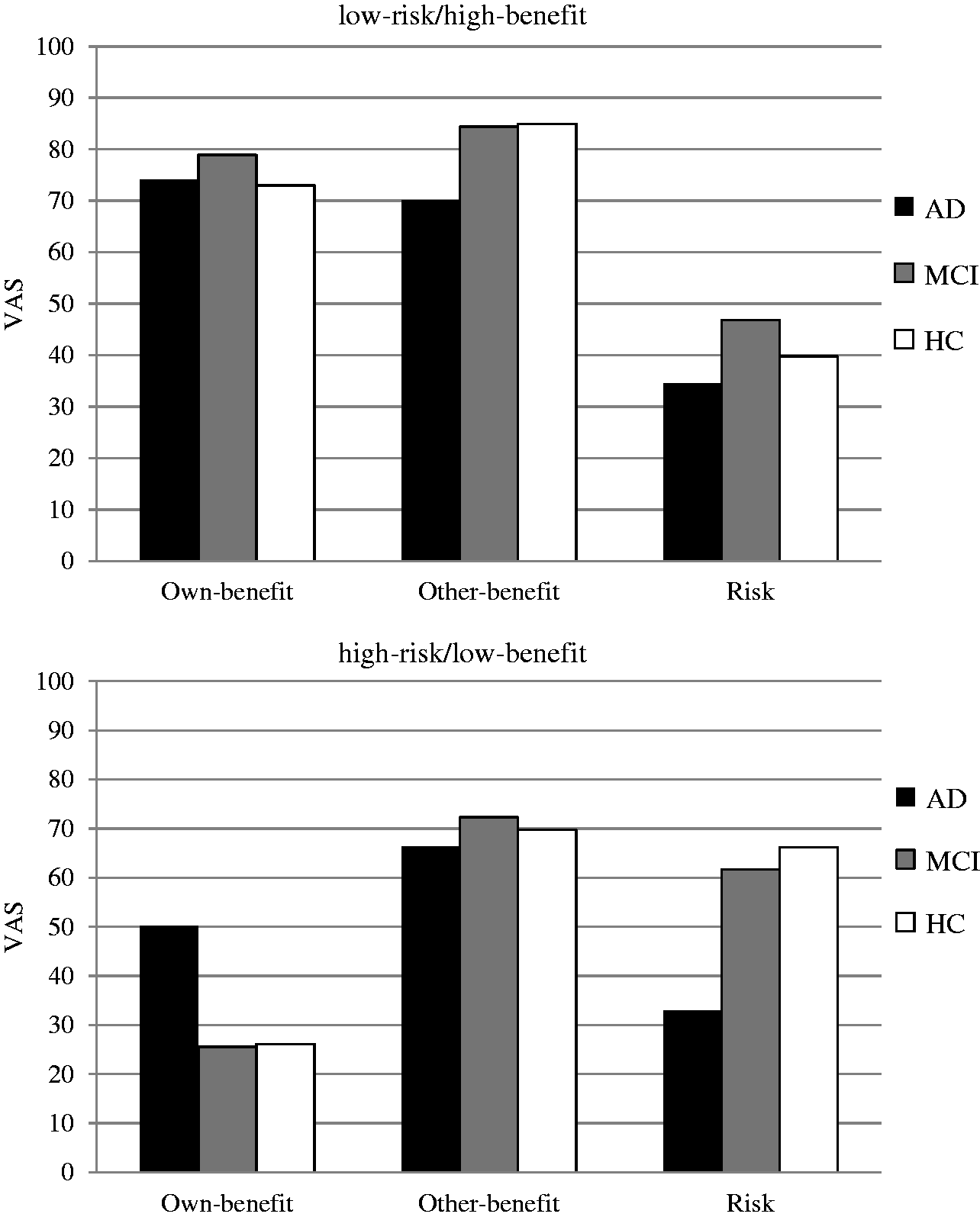
Mean value of VAS (0 = no risk/benefit; 100 = high risk/benefit) of estimated risk and benefits (own-benefit, other-benefit and risk) regarding participation in the two trials (low-risk/high-benefit and high-risk/low-benefit) in groups of subjects (AD, MCI and HC).
There was a significant difference between the two trials across groups (F = 43.5, df = 1/71, p < .001, ε2 = .38) and between types of estimations across groups (F = 52.4, df = 2/70, p < .001, ε2 = .60). The interaction between trial and estimation (F = 40.3, df = 2/70, p < .001, ε2 = .54) and between type of estimation and group was significant across trials (F = 4.42, df = 4/142, p < .01, ε2 = .11) as well as the three-way interaction concerning trial, type of estimation and group (F = 3.26, df = 4/142, p < .05, ε2 = .08), which indicated that groups made different estimations in the two trials.
In the low-risk/high-benefit trial, significant group differences were obtained on mean VAS score for other-benefit (F = 5.38, df = 2/71, p < .01). In the high-risk/low-benefit trial, significant group differences were obtained on mean VAS score for own-benefit (F = 5.05, df = 2/71, p < .01) and risk (F = 8.96, df = 2/71, p < .001).
AD patients estimated risk and benefit significantly differently in comparison to both MCI and HC in the two trials. In the low-risk/high-benefit trial, AD patients estimated the other-benefit lower than MCI and HC (p < .05; AD (70) vs. MCI (84) and HC (85)). In the high-risk/low-benefit trial, AD patients estimated the own-benefit higher than MCI and HC (p < .05; AD (50) vs. MCI (26) and HC (26) and the risk lower than MCI and HC (p’s < .05; AD (33) vs. MCI (62) and HC (66)). No significant group differences were obtained between MCI and HC regarding estimations of benefits and risk in the two trials (all p’s > .1).
Attitudes toward proxy in the trials
A significant difference was shown regarding an overall acceptance to proxy between the trials (F = 20.2, df = 1/58 p < .001, ε2 = .26), demonstrating a higher acceptance of proxy in the low-risk/high-benefit trial (72%) compared to the high-risk/low-benefit trial (38%). The interaction between groups and trials was significant (F = 6.35, df = 2/58; p < .01; ε2 = .18). A significant group difference was shown in acceptance to proxy (F = 4.66, df = 2/58; p < .05; ε2 = .14). AD patients were more willing to accept proxy in the high-risk/low-benefit trial than HC (p < .001; AD (60%) vs. HC (22%)). No group difference was shown regarding acceptance of proxy in the low-risk/high-benefit trial (p > .1). AD patients showed an overall positive attitude to proxy and no difference in acceptance to proxy between the two trials (t < 1, df = 13; p > .1), while acceptance to proxy differed between trials in both MCI (t = 2.92; df = 17; p < .01) and HC (t = 5.56; df = 28; p < .001).
Three categories of proxy were identified among the individual responses to Q4 (Who would you prefer made the decision in your place): “family member” (spouse, child, or sibling), “physician” and “family member in consultant with physician”. Results showed that “a family member” was overall the most frequently chosen proxy (91%) in all groups.
Discussion
The result revealed a positive attitude in all groups toward participation in the trials as approximately 90% of all participants expressed that they would have participated in the low-risk/high-benefit trial, and approximately 40% would have participated also in the high-risk/low-benefit trial (which was written to exaggerate side effects beyond what would be accepted by an ethical committee for this type of treatment). Although no significant difference was shown between groups in willingness to participate in the two trials, those who were willing to participate in this high-risk trial had impaired medical decision-making capacity as shown by the significant difference in LIMD-score. Interestingly, the MMSE-scores were not significantly different, illustrating the fact that the association between general cognitive function and medical decision-making capacity is weak in early stages of dementia. Further on, AD showed an impaired estimation of risk and benefits (by VAS) compared to both MCI and HC, which suggests a possible parallel between MDMC and risk analysis ability. The notable high acceptance to participate in the high-risk/low-benefit trial should also be discussed in terms of patients’ interest to make good, despite highly implied risk and low benefit. The result showed five main reasons why groups were willing to participate in the two trials: “own-benefit”, “help others”, “own benefit and help others”, “support research and make good,” and “other reasons”. It is known from previous research that common reasons to participate in trials among elderly are own-benefit and a general desire to make good (Tolmie et al., 2004), which is in coherence with present results. However, the present study contributed with new data as it included different groups of elderlies (AD, MCI, and HC), and also two different fictive trials with varied implied risk and benefit. The results indicate a general accordance between groups regarding reasoning to participate but reveal a difference in how to reason between the two trials. The primary reason to participate in the low-risk/high-benefit trial was “own-benefit” in comparison to “help others” in the high-risk/low-benefit trial. Another possible interpretation why AD showed such high acceptance of participation in the high-risk trial is that they suffer from a deadly disease and thus are more willing to take more risks than MCI or HC. The estimation of risk and benefit in the trials differed significantly between groups in both trials. In the high-risk/low-benefit trial, patients with AD perceived the risk as lower and the own-benefit as higher compared to both MCI and HC. The result shows that reduced cognitive functions characteristic of mild AD – but not MCI – have a significant impact on the patients’ ability to estimate risk and benefit. But perhaps might also here the knowledge of having a deadly disease impact the estimation of possible risk and benefit? In the context of informed consent to participation in research, our results show that even in mild dementia, patients will often not possess the capacity to consent to participation through a procedure we should consider to be truly “informed..
When capacity to consent is considered insufficient, proxy consent is a possible solution in most countries (Appelbaum, 2007; Panting, 2010; White & Seery, 2009). Appointing a possible proxy should preferably be discussed with patient before the MDMC may be in doubt. However, previous study showed that patients with AD who were not considered capable to give informed consent, still had preserved capacity to appoint a proxy (Kim et al., 2011). This stresses the importance of investigating attitudes toward proxy also in patients with AD, but the implications will inevitably depend on the national legislation on this subject. Our result of attitudes toward possible proxy in the two trials showed an overall higher acceptance of proxy in the low-risk/high-benefit-trial, a result coherent with previous findings (Ayalon, 2009; Dubois et al., 2011). However, acceptance to proxy differed in the high-risk trial, where AD showed a higher acceptance to proxy. The difference between groups in acceptance to proxy may be explained by reduced capacity in AD patients to recognize the implied high risk or that they somehow perceived that this trial was different and that a proxy was needed? No difference between groups was noted in acceptance of proxy in the low-risk trial. A family member was the primary choice ( > 90%) of proxy in all groups, which indicates that both healthy elderly and dementia patients value family support when discussing possible proxy consent. However, this finding may hardly be generalizable in clinical practice as relationship fluctuates and must be evaluated individually.
To objectively investigate different aspects of patients participating in clinical trials is a difficult task. There are some potential problems associated with a study like this. First, in a study with many statistical analyses, it always a risk of type II error, which has to be considered when results are interpreted. Second, the use of hypothetical trials could be questioned, as it requires a reasonably advanced level of thinking. Still, to imagine possible risk and benefit in real research context requires a similar capacity of abstract thinking. Previous studies have showed that hypothetical scenarios enhance understanding on decisions in medical settings (Fung, Lam, & Lui, 2010). Third, there could also be a potential bias to investigate participants’ willingness to participate in the two hypothetical trials, as all participants showed a probable positive interested in research by participating in present study. However, this does not reduce the credibility of result concerning comparison of acceptance between groups, estimations of risk and benefits, and attitudes toward proxy. The participants are recruited from three groups with varied cognitive function (AD, MCI, and HC) and presumptive different capacity to analyze given information, which supports the aim of present study: To investigate how cognitive decline affects the decisional reasoning and capacity to estimate risks and benefits. Still, it must also be noted that agreeing to undertake this particular study was considered most harmless and thereby well approved although MDMC of the participants varied. Finally, the capacity to give consent may vary over time, due to cognitive progression, daily status and complexity of information, which could have affected the results. However, we tried to minimize bias of possible change in daily status or cognitive progression by having the test procedure including both trials at one occasion per patient. The texts of the two trials were written with a similar complexity of basic language and similar length of information.
Practical implications: To avoid non-desired consequences for dementia patients due to poor decisional capacity, we emphasize the use of a clinical tool to estimate patients’ medical decisional capacity as a practical implication to guide physicians working with dementia patients. Second, to protect patients’ autonomy without compromising safety and medical treatment, we suggest practical standards of how to engage dementia patients in different medical decisions before their decisional capacity is crucially doubtful, such as standardized questionnaire regarding patient's decisions and attitudes to clinical trials and proxy.
Conclusion
Medical decisions and research consent should be interpreted with caution in patients who are already in early stages of dementia, as the patients’ acceptance to participate in high-risk trials may be due an insufficient decisional capacity and risk analysis, accelerated by a general desire to make good to society. We emphasize the use of a standardized tool to evaluate medical decisional capacity in clinical research.
Footnotes
Ethics
The Regional Ethics Committee in Stockholm approved the study. All subjects were well informed of the study and informed consent was obtained from all subjects. Since our results show that many patients with mild AD cannot evaluate risks properly, the informed consent we used for the participants in this study can be questioned. However, we strongly believe that the patients were not exposed to any physical or mental risks due to their participation. We confirm that identifiers of all persons studied have been removed or disguised so the subjects described are not identifiable and cannot be identified through the details of the story.
Authors’ contributions
S. Stormoen designed the study, was test leader, and responsible for the data collection, analyzed the results and wrote the paper. I.M. Tallberg participated in the design of the study, contributed with linguistic methodology and supervised the project from the data collection up to the writing of the manuscript. O. Almkvist participated in the design of the study, contributed with expertise in the field of psychology, and supervised statistical analysis. M. Eriksdotter participated in the design of the study, underlying hypothesis, supervised inclusion of participated patients, and interpretation of the results. E. Sundström participated in the design of the study, underlying hypothesis, construction of the test instrument, and interpretation of the results.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.